
Abstract
Background
82-Rubidium-Positron emission tomography myocardial perfusion imaging (Rb-PET-MPI) offers higher diagnostic performance for the detection of myocardial ischemia compared to Tc-SPECT-MPI. The aim of this economic evaluation was to perform a cost-effectiveness analysis of Rb-PET-MPI versus Tc-SPECT-MPI in patients with suspected myocardial ischemia according to pretest probabilities (PTP) of obstructive coronary artery disease based on the results of the RUBIS Trial.
Methods
Costs and effectiveness were calculated for all patients over 1 year and an incremental analysis of differences in costs and effectiveness in terms of diagnostic accuracy was performed. The uncertainty of the results was estimated using bootstrap. The analysis was conducted from the perspective of the French health care system with a time horizon of 12 months.
Results
The average cost of a Rb-PET-MPI-based strategy for the detection of myocardial ischemia was €219 lower than a SPECT-MPI-based strategy (€1192 (± 1834) vs €973 (± 1939), p < 0.01). The one-year incremental cost-effectiveness ratio was negative: − €2730 (money saved per additional accurate diagnosis) in patients presenting PTP > 15% for the Rb-PET-MPI vs. Tc-SPECT-MPI strategy. Analysis of the joint distribution of costs and outcomes found that the Rb-PET-MPI strategy had a 92% probability to be dominant (cost-saving and outcome-improving).
Conclusions
Rb-PET-MPI is cost-effective compared to Tc-SPECT-MPI for the detection of myocardial ischemia in patients with PTP > 15% of obstructive coronary artery disease.
Trial registration
RUBIS Trial registration: NCT01679886, Registered 03 September 2012, https://clinicaltrials.gov/ct2/show/NCT01679886.
Similar content being viewed by others


Introduction
Single-photon emission computed tomography myocardial perfusion imaging (SPECT-MPI) with 99m-Technetium-radiolabeled perfusion tracers (99mTc) has demonstrated its high diagnostic accuracy, prognostic value and its cost-effectiveness for the detection of myocardial ischemia [1]. Tc-SPECT-MPI has shown to be more expensive but more effective than stress echocardiography for the detection of myocardial ischemia with incremental cost-effectiveness ratios ranging from €71,930 to €168,585 per QALY gained [2]. In recent years, the diagnostic performances of Tc-SPECT-MPI benefited from technological advances but remain limited by attenuation artifacts. The diagnostic accuracy and prognostic value of CZT-SPECT derived MBF quantification is still under investigation [3, 4].
MPI with positron emission tomography with 82Rubidium (Rb-PET-MPI) provides several advantages over Tc-SPECT-MPI for the detection of myocardial ischemia. First, Rb-PET-MPI offers higher signal and a more accurate attenuation correction than Tc-SPECT-MPI. Second, the methods, accuracy and reproducibility for MBF quantification have been well validated for PET. Third, rest and stress Rb-PET-MPI can be acquired sequentially in 30 min with Rubidium-82 thanks to the short physical half-life of Rb reducing dramatically the time spent by patients in Nuclear Medicine department for MPI [5, 6]. Fourth, Rb-PET-MPI is associated with lower radiation exposure of patients than Tc-SPECT-MPI [7, 8]. Lastly, Rb-PET-MPI has consistently demonstrated its higher diagnostic performances than Tc-SPECT-MPI in different population of patients [6, 9]. In the RUBIS prospective clinical trial, our group has recently confirmed in 308 patients the higher diagnostic performance of Rb-PET-MPI vs. Tc-SPECT-MPI in a population of overweight patients and women for the detection of myocardial ischemia [8]. Rb-PET-MPI is clinically available since more than 20 years in North America and reimbursed, but clinical access was until now limited in Europe owing to the absence of clinically approved 82-Sr / 82-Rb generators and the lack of reimbursement for PET-MPI in most European countries. The aim of this study was to estimate the cost-effectiveness of Rb-PET-MPI compared to SPECT-MPI with 99mTc-Sestamibi in patients with different risks of coronary artery disease (CAD).
Material and methods
Study design
The RUBIS trial compared the diagnostic performances between Rb-PET-MPI and Tc-SPECT-MPI using CZT gamma cameras for the detection of myocardial ischemia in a population of women and overweight patients (body mass index (BMI) ≥ 25). This study was approved by the Ethics Committee of Ile-de-France VI and by the French National Agency for Medicines and Health Products (ANSM). Trial registration number NCT01679886. The method and results of RUBIS have been already published [8]. The economic analysis was carried out on three subgroups defined post hoc from the clinical analysis: low, intermediate and high pretest probabilities (PTP) of obstructive CAD, according to the ESC’s classification of PTP for obstructive CAD based on patient’s characteristics (age, sex, chest pain and dyspnea). The PTP cutoff values to classify patients are PTP < 5%, PTP between 5–15% and PTP > 15% [10]. Rb-PET-MPI and Tc-SPECT-MPI were performed successively for all patients and were compared (confirmed or rejected) to the invasive coronary angiography (ICA) with functional assessment of coronary stenosis using fractional flow reserve (FFR) measurements, which was regarded as the gold standard, for patients with abnormal examination or to the patient’s one-year clinical follow-up (ischemic events or death), in the absence of ICA. Both imaging modalities were evaluated independently from each another.
Economic evaluation
Data for the economic evaluation were prospectively collected during the trial, in accordance with the Consolidated Health Economic Evaluation Reporting Standards (CHEERS) statement [11]. The efficacy endpoint used in the economic study was the diagnostic accuracy and was obtained from data collected in the case report form (CRF). Costs and effectiveness were assessed in all patients over 1 year and an incremental cost-effectiveness ratio of cost per additional accurate diagnostic was estimated. Bootstrapping was used to quantify uncertainty on the joint distribution of costs and outcomes, and the 1000 paired estimates of mean differential costs and diagnostic accuracy in each subgroup were reported on a cost-effectiveness plane. The study perspective was the French healthcare system and the time horizon was 12 months.
Estimating resources and costs
Only direct costs were assessed in this economic study as recommended by the French National Authority for Health (HAS) [12]. Both hospital and non-hospital resources were considered.
Data for the Rb-PET-MPI procedure were collected by a bottom-up micro-costing analysis completed with data from the CRF and the local hospital claims database. Calculation methods and data sources used to estimate the cost of Rb-PET-MPI are detailed in Additional file 1: Tables S1, S2 and S3 online.
At the time of collecting data on resource utilization for the economic analysis, the radio-physicians carried out regular quality control routines for the Rubidium injectors. Since then, Rubidium injectors have been improved and these routines have automated, liberating human resource time for other activity. In the centers where the observations and resource data collection for the micro-costing were carried out, only ten patients were examined every week. For this analysis, taking into consideration the automation of the quality control and with the aim of maximizing efficiency, the base case taken in our analysis is 30 patients per week per injector which corresponds to the material being used for 50% of the working week.
A deterministic sensitivity analysis on the Rb-PET-MPI procedure cost was performed, varying firstly the lifetime of the CardioGen-82 generator and secondly the number of patients per generator. The SPECT-MPI procedure included a stress acquisition with injection of the Tc-sestamibi at stress (exercise, pharmacological stress with dipyridamole or combined stress) and a rest acquisition if necessary. The cost of SPECT-MPI has been evaluated in the past and the tariff was used as a proxy for production cost (see Additional file 1: Table S4 online). Data for the SPECT-MPI procedure were collected from the CRF. The total cost of each strategy (Rb-PET-MPI or Tc-SPECT-MPI) included the procedural cost, the additional test cost (ICA) if the procedural result was positive and follow-up admissions costs produced by CAD.
Statistical analysis
The statistical analyses were performed on all patients for each of the pre-specified subgroups (low, intermediate and high PTP of myocardial ischemia). Data are described by statistical analyses (mean, standard deviation (SD) or percentage depending on the type of variable). A comparison of baseline characteristics of participants between the three subgroups was performed using the Chi-square test or ANOVA test depending on the type of variable. Cost data of Rb-PET-MPI and SPECT-MPI were compared using Student's t-test. Mann–Whitney's nonparametric test was performed in the case of non-normal distribution. Effectiveness was compared using Fisher’s exact test. A multiple imputation of the missing data was carried out. A p value less than 0.05 was considered significant. Statistical analyses were carried out using R Software (version 3.6.4).
Results
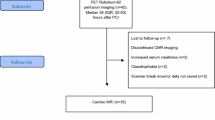
A total of 308 patients were included in the RUBIS trial, 46 in the low PTP subgroup, 132 in the intermediate PTP subgroup and 130 in the high PTP subgroup (Fig. 1). Baseline characteristics of RUBIS patients are presented in Table 1.

Flowchart of the economic evaluation
Costs
The base case is estimated from the assumption of five Rb-PET-PMI sessions scheduled per week, with an average of 6 patients per session, equivalent to 30 patients imaged per week, or to 210 patients imaged during the seven-week lifetime of the generator.
An automatic quality control (QC) of the generator was carried out before any session, eliminating time and cost of a radio-physician required for non-automatic QC. The procedural per patient cost of the Rb-PET-MPI (n = 308) was estimated to be €471 (± 0) for a volume of 30 patients per week. This cost included the costs of staff, supplies and imaging room which were, respectively, €65, €195 and €211. The average procedural cost of the SPECT-MPI was €757 (± 116).
In order to validate the positive test results, 47 (15%) ICA for Rb-PET-MPI and 31 (10%) ICA for Tc-SPECT-MPI were performed. The respective average costs per patient of ICA were, respectively, €191 (± 469) and €124 (± 381).
During the one-year follow-up, 16 patients (5.2%) were hospitalized at least once for a cardio-vascular event. The average cost of follow-up admissions was €311 (± 1718). The total one-year costs of Rb-PET-MPI and Tc-SPECT-MPI strategy were €973 (± 1939) and €1192 (± 1834), respectively p < 0.01). The one-year costs in each subgroup are presented in Table 2.
Effectiveness
Diagnostic accuracy for the two strategies in each subgroup is presented in Table 3. In patients with low PTP and intermediate PTP, the differences in diagnostic accuracy between Rb-PET-MPI and Tc-SPECT-MPI were, respectively, − 0.04 and − 0.02 (p = 0.16, p = 0.64). In patients with high PTP, the difference was 0.08 (p = 0.048).
Incremental/decremental cost-effectiveness ratio
In the low PTP and intermediate PTP groups, Rb-PET-MPI had a lower cost and a lower effectiveness than Tc-SPECT-MPI with decremental cost-effectiveness ratios of €5888 and €12,804, respectively, indicating the additional cost of Tc-SPECT-MPI over Rb-PET-MPI for each additional accurate diagnosis at a one-year horizon. In the high PTP group, the incremental cost ratio was estimated to be − €2730 per additional accurate diagnosis, that is, the use of Rb-PET-MPI rather than Tc-SPECT-MPI would lead to an average cost-saving of €2730 for each accurate diagnosis.
Sensitivity analysis
Deterministic sensitivity analysis
For six patients imaged per session and per week, with a generator lifetime of six to eight weeks, the cost of the Rb-PET-MPI procedure ranges from €449 to €498.
We evaluated the impact of the number of patients examined per session on the cost of each Rb-PET-MPI procedure (Fig. 2). The minimum number of examinations to get the Rb-PET-MPI procedure to be cost-effective was 12 per week or 105 examinations per generator over a seven-week period.

Cost of Rb-PET-MPI procedure based on the number of patients imaged per session
Probabilistic sensitivity analysis
The uncertainty on the joint distribution of costs and outcomes is presented on the cost-effectiveness plane for the three subgroups (Fig. 3).

Cost-effectiveness plane: Incremental Cost-Effectiveness Ratio of Costs per additional accurate diagnosis at 12 months in each subgroup
We observed a shift of replications from the left to the right by increasing the PTP of obstructive CAD. In the low PTP subgroup, the scatter plot of the bootstrapped ICERs showed that all the replications were located in the lower left-hand quadrant indicating that the Rb-PET-MPI strategy was unlikely to be cost-effective compared to the Tc-SPECT-MPI strategy since it is cheaper but less effective.
In the intermediate PTP subgroup, the replications were scattered on the four quadrants of the plan. So, because of this uncertainty, we cannot conclude on the cost-effectiveness of the Rb-PET-MPI.
However in the high PTP subgroup, 92% of replications were located in the lower right-hand quadrant (incrementally cost-effective), indicating that the Rb-PET-MPI strategy was both cost-saving and outcome-improving (i.e., dominant) and this strategy had a high probability of being cost-effective across the entire range of willingness-to-pay values for an additional accurate diagnosis.
Discussion
The economic evaluation of RUBIS trial estimated an average cost of €471 for the Rb-PET-MPI procedure including the costs of staff (€65), supplies (€195) and imaging room (€211) by scanning 30 patients per week or 210 patients per generator over a seven-week period. This cost was lower by €286 than the cost of SPECT-MPI with 99mTc-Sestamibi. The cost of equipment and supplies of the Rb-PET-MPI in our study was comparable to the results of a Danish costing at the Copenhagen University Hospital that estimated at €400 the cost of supplies (generator + infusion system + disposables) for 15 patients imaged per week with 82-Rubidium [5]. That is, given the fixed cost of the generator, the average cost per patient should decrease as the number of patients imaged per week increases [13]. In our study, the 82-Sr/82-Rb generator was the main cost driver representing 80% of cost of material and supplies. For example, if the number of patients scanned per week is increased to 75 (= 15 patients per day), the average cost of supplies (generator + infusion system + disposables) per patient is reduced by 48%. In addition, this new technique also saves considerable time [14]. The Tc-SPECT took typically four hours for a one-day stress/rest protocol or two separate visits of ∼ 90 min for a two-day protocol, whereas with Rb-PET-MPI 30 to 45 min for only one-day protocol were sufficient and when generator QC was automatically performed for each session.
The total costs of Rb-PET-MPI and SPECT-MPI strategies were therefore €973 (± 1939) and €1192 (± 1834), respectively (p < 0.01). With the volume of 30 patients imaged per week, Rb-PET-MPI was then 20% cheaper than the SPECT-MPI. These results are roughly similar to those found in an US paper of Merhige et al. evaluating the impact of Rb-PET versus SPECT on subsequent invasive procedures and outcomes, which demonstrated that Rb-PET had 30%, cost savings at 1 year compared with SPECT [15].
In the low PTP and intermediate PTP groups, Rb-PET-MPI had a lower cost and a lower effectiveness than Tc-SPECT-MPI with decremental cost-effectiveness ratios of €5888 and €12,804, respectively.
The one-year incremental cost-effectiveness ratio was negative: − €2730 (€2730 money saved per additional accurate diagnosis) in patients presenting a high PTP with the Rb-PET-MPI versus SPECT strategy indicating dominance (cheaper and more effective) of Rb-PET-MPI.
Analysis of the joint distribution of costs and outcomes showed a shift of replications from the left to the right by increasing the PTP of obstructive CAD (from less effective to more effective). The replications were evenly scattered on the four quadrants of the plan in the intermediate-risk group. This indicated that the two strategies tend to be similar. The probabilistic sensitivity analysis confirmed that the Rb-PET-MPI strategy had a 92% probability of being dominant (cost-saving and outcome-improving) in the high-risk group.
A study comparing the cost-effectiveness of exercise ECG, SPECT, PET and ICA of diagnosis of CAD showed that in a population with a high prevalence of CAD, PET had a lower cost per effect than other noninvasive tests because of its higher accuracy [16].
In a systematic review and meta-analysis, Rb-PET was demonstrated to have superior accuracy in comparison with Tc-SPECT when low likelihood risk patients were excluded and the difference in accuracy was more pronounced in favor of Rb-PET [6].
David et al. in a recent study found that the Rb-PET provided greater diagnostic accuracy in the detection of obstructive CAD relative to Tc-SPECT in extremely obese patients (diagnostic accuracy: Rb-PET 86.3% versus Tc-SPECT 64.9%, p = 0.02) [17].
For patients with high PTP of obstructive CAD our results support the greater accuracy of Rb-PET-MPI versus Tc-SPECT-MPI (diagnostic accuracy: Rb-PET 87% vs. Tc-SPECT 78%, p = 0.05) and confirm that Rb-PET-MPI was potentially cost-effective in detecting myocardial ischemia in patients with high PTP of obstructive CAD.
The costs of the procedures were lower in our study than in US studies previously published, with cost per scan ranging from €1000 to 2000 [15, 16]. Costs in Europe tend to be lower ranging from €260–450 for SPECT to €1000 for PET [18].
Limitations of the study
First, in the low risk subgroup, we cannot conclude on the effectiveness of Rb-PET-MPI compared to Tc-SPECT-MPI because of the small number of patients included and the absence of positive cases. Two patients were falsely classified as positive with Rb-PET which could lead to overtreatment.
Second, the cost results of this economic study only concern the French environment and are not directly applicable in other countries. Third, invasive coronary angiography and FFR were used as gold standards for the evaluation of the diagnostic performance of MPI with SPECT and PET, but offer only to assess the hemodynamic impact of epicardial coronary stenosis on hyperemic blood flow and do not provide accurate measurements of regional myocardial perfusion.
Conclusions
Rb-PET-MPI estimated cost was lower than the cost of SPECT-MPI with 99mTc-Sestamibi. The cost of Rb-PET is highly dependent on an efficient use of the materiel in terms of the number of weekly sessions and the number of patients per session.
In this study, we demonstrated that Rb-PET was cost-effective compared to Tc-SPECT for the detection of myocardial ischemia in patients with PTP > 15% of obstructive CAD.
Availability of data and materials
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- BMI:
-
Body mass index
- CHEERS:
-
Consolidated Health Economic Evaluation Reporting Standards
- CAD:
-
Coronary artery disease
- DF:
-
Diamond-Forrester
- FFR:
-
Fractional flow reserve
- HAS:
-
French National Authority for Health
- ICA:
-
Invasive coronary angiography
- ANSM:
-
National Agency for Medicines and Health Products
- PET-MPI:
-
Positron emission tomography myocardial perfusion imaging
- PTP:
-
Pretest probabilities
- QC:
-
Quality control
- SPECT-MPI:
-
Single-photon emission computed tomography myocardial perfusion imaging
- 99mTc:
-
99M-Technetium
- Rb:
-
82-Rubidium
References
Shaw LJ, Narula J. Risk assessment and predictive value of coronary artery disease testing. J Nucl Med. 2009;50(8):1296–306.
Garber AM, Solomon NA. Cost-effectiveness of alternative test strategies for the diagnosis of coronary artery disease. Ann Intern Med. 1999;130(9):719–28.
Agostini D, Roule V, Nganoa C, Roth N, Baavour R, Parienti JJ, Beygui F, Manrique A. First validation of myocardial flow reserve assessed by dynamic 99mTc-sestamibi CZT-SPECT camera: head to head comparison with 15O-water PET and fractional flow reserve in patients with suspected coronary artery disease. The WATERDAY study. Eur J Nucl Med Mol Imaging. 2018;45(7):1079–90.
Acampa W, Zampella E, Assante R, Genova A, De Simini G, Mannarino T, D’Antonio A, Gaudieri V, Nappi C, Buongiorno P, Mainolfi CG, Petretta M, Cuocolo A. Quantification of myocardial perfusion reserve by CZT-SPECT: a head to head comparison with 82Rubidium PET imaging. J Nucl Cardiol. 2021;28(6):2827–39.
Ghotbi AA, Kjaer A, Hasbak P. Review: comparison of PET rubidium-82 with conventional SPECT myocardial perfusion imaging. Clin Physiol Funct Imaging. 2014;34(3):163–70.
Mc Ardle BA, Dowsley TF, deKemp RA, Wells GA, Beanlands RS. Does rubidium-82 PET have superior accuracy to SPECT perfusion imaging for the diagnosis of obstructive coronary disease?: A systematic review and meta-analysis. J Am Coll Cardiol. 2012;60(18):1828–37.
Hunter CR, Hill J, Ziadi MC, Beanlands RS, deKemp RA. Biodistribution and radiation dosimetry of (82)Rb at rest and during peak pharmacological stress in patients referred for myocardial perfusion imaging. Eur J Nucl Med Mol Imaging. 2015;42(7):1032–42.
Hyafil F, Chequer R, Sorbets E, Estellat C, Ducrocq G, Rouzet F, Alfaiate T, Regaieg H, Abtan J, Leygnac S, Milliner M, Imbert L, Burg S, Ben Azzouna R, Potier L, Laouénan C, Quintin C, Roussel R, Hartemann A, Montalescot G, Marie PY, Steg G, Le Guludec D. Head-to-head comparison of the diagnostic performances of Rubidium-PET and SPECT with CZT camera for the detection of myocardial ischemia in a population of women and overweight individuals. J Nucl Cardiol. 2020;27(3):755–68.
Sampson UK, Dorbala S, Limaye A, Kwong R, Di Carli MF. Diagnostic accuracy of rubidium-82 myocardial perfusion imaging with hybrid positron emission tomography/computed tomography in the detection of coronary artery disease. J Am Coll Cardiol. 2007;49(10):1052–8.
Knuuti J, Wijns W, Saraste A, Capodanno D, Barbato E, Funck-Brentano C, Prescott E, Storey RF, Deaton C, Cuisset T, Agewall S, Dickstein K, Edvardsen T, Escaned J, Gersh BJ, Svitil P, Gilard M, Hasdai D, Hatala R, Mahfoud F, Masip J, Muneretto C, Valgimigli M, Achenbach S, Bax JJ, ESC Scientific Document Group. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur Heart J. 2020;41(3):407–77.
Husereau D, Drummond M, Petrou S, Carswell C, Moher D, Greenberg D, Augustovski F, Briggs AH, Mauskopf J, Loder E, ISPOR Health Economic Evaluation Publication Guidelines-CHEERS Good Reporting Practices Task Force. Consolidated Health Economic Evaluation Reporting Standards (CHEERS)—explanation and elaboration: a report of the ISPOR Health Economic Evaluation Publication Guidelines Good Reporting Practices Task Force. Value Health. 2013;16(2):231–50.
Choix méthodologiques pour l’évaluation économique à l’HAS. https://webzine.has-sante.fr/portail/upload/docs/application/pdf/2011-11/guide_methodo_vf.pdf. Accessed 12 April 2020.
Chatal JF, Rouzet F, Haddad F, Bourdeau C, Mathieu C, Le Guludec D. Story of Rubidium-82 and advantages for myocardial perfusion PET imaging. Front Med (Lausanne). 2015;2:65.
Calizzano A. Myocardial perfusion scintigraphy: state of the art and future prospects. Med Nucl. 2007;31(11):604–9.
Merhige ME, Breen WJ, Shelton V, Houston T, D’Arcy BJ, Perna AF. Impact of myocardial perfusion imaging with PET and (82)Rb on downstream invasive procedure utilization, costs, and outcomes in coronary disease management. J Nucl Med. 2007;48(7):1069–76.
Patterson RE, Eisner RL, Horowitz SF. Comparison of cost-effectiveness and utility of exercise ECG, single photon emission computed tomography, positron emission tomography, and coronary angiography for diagnosis of coronary artery disease. Circulation. 1995;91(1):54–65.
David TH, Samir H, Ronnen M, Mc Ardle BA, Ali A, Trevor S, Ellen H, Girish D, Christopher G, Robert A, Ross AD, Terrence DR, Benjamin JWC, Rob SB, Benjamin H. Clinical performance of Rb-82 myocardial perfusion PET and Tc-99m-based SPECT in patients with extreme obesity. J Nucl Cardiol. 2019;26(1):275–83.
Lorenzoni V, Bellelli S, Caselli C, Knuuti J, Underwood SR, Neglia D, Turchetti G, EVINCI Investigators. Cost-effectiveness analysis of stand-alone or combined non-invasive imaging tests for the diagnosis of stable coronary artery disease: results from the EVINCI study. Eur J Health Econ. 2019;20(9):1437–49.
Acknowledgements
Members of the RUBIS (Comparison of the Diagnostic Performances of 82Rubidium-Positron Emission Tomography and Conventional Scintigraphy With CZT Cameras for Detection of Myocardial Ischemia in a Population of Overweighed Patients and Women) Trial Group are as follows: Renata Chequer, Gregory Ducrocq, Toni Alfaiate, Hamza Regaieg, Jérémie Abtan, Sébastien Leygnac, Milan Milliner, Samuel Burg, Rana Ben Azzouna, Louis Potier, Cédric Laouénan, Caroline Quintin, Ronan Roussel, Gabriel Steg, Dominique Le Guludec (Bichat University Hospital, Paris, France); Emmanuel Sorbets (Avicenne University Hospital, Bobigny, France); Laetitia Imbert, Pierre-Yves Marie (Brambois University Hospital, Vandœuvre-Lès-Nancy, France); Agnès Hartemann, Gilles Montalescot (Pitié-Salpétriêre University Hospital, Paris, France).
Funding
This research was funded by a grant from the French Ministry of Health (Programme Hospitalier de Recherche Clinique 2011 AOM11066).
Author information
Authors and Affiliations
Consortia
Contributions
FH and IDZ were involved in conceptualization; JB, CE, FH and IDZ helped in methodology; MM and JB contributed to investigation; MM was involved in analysis and writing original draft preparation; JB, MD, CE, FR, IDZ and FH helped in writing review and editing, FH and IDZ contributed to supervision. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. All patients provided signed informed consent; the full description of the study design has been registered on clinicaltrials.gov (NCT01679886; https://clinicaltrials.gov/ct2/show/NCT01679886). The French Institutional Review Board approved the study protocol (IRB number: 2012-A00552-41).
Consent for publication
Not applicable.
Competing interests
Fabien Hyafil is Consultant for Naogen, Curium Pharma, Blue Earth Diagnostics, Novo Nordisk and shareholder of Naogen. The other authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1. Table S1.
Calculation method, data sources and valuation used to calculate the cost of Rb-PET-MPI (procedural and follow-up costs). Table S2. Hourly cost of human resources of Rb-PET-MPI intervention. Table S3. Unit cost of supplies and drugs used on Rb-PET-MPI procedure. Table S4. Resources used in Tc-SPECT-MPI procedure
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Mimouni, M., Bulsei, J., Darlington, M. et al. Cost-effectiveness of 82-Rubidium PET myocardial perfusion imaging for the diagnosis of myocardial ischemia depending on the prevalence of coronary artery disease. EJNMMI Res 13, 9 (2023). https://doi.org/10.1186/s13550-023-00954-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13550-023-00954-x