
Abstract
Background
Osteosarcoma arising from the bladder is extremely rare, with only 38 cases reported to our knowledge. It is often detected owing to hematuria, and is treated by surgery (for example, total cystectomy), radiation therapy, and chemotherapy; however, the prognosis is extremely poor.
Case presentation
An 83-year-old Japanese man underwent cystoscopy for postoperative follow-up of urothelial carcinoma of the bladder, which revealed a 2-cm nodular tumor on the right wall. He had a history of abdominal aortic aneurysm and hypertension, and had been smoking 15 cigarettes per day for 45 years. Seven years previously, the patient underwent transurethral resection of bladder tumor for a 5-cm tumor on the right wall of the bladder. The histopathological diagnosis was urothelial carcinoma. No recurrence had been detected since then. Transurethral resection of bladder tumor was performed, and the histopathological diagnosis was cystosarcoma. Because of his advanced age, we decided that it would be difficult to perform total cystectomy. We therefore performed a second transurethral resection of bladder tumor and found no residual tumor. At 29 months after surgery, the patient remains alive without recurrence.
Conclusion
Bladder osteosarcoma has a poor prognosis. However, our case was detected early, and treatment with transurethral resection of bladder tumor alone resulted in long-term survival without recurrence.
Similar content being viewed by others

Background
Osteosarcoma arising from the bladder is extremely rare. It is treated by total cystectomy, radiation therapy, and chemotherapy; however, the prognosis is extremely poor. In this article, we report a case of bladder osteosarcoma that was discovered asymptomatically during follow-up of urothelial carcinoma of the bladder. The patient was treated by transurethral resection of bladder tumor (TURBT) alone and achieved long-term survival without recurrence.
Case presentation
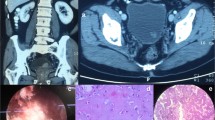
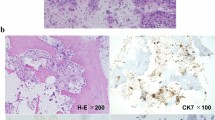
The patient was an 83-year-old Japanese man. During routine cystoscopy after TURBT, a 2-cm nodular tumor was found on the right wall (Fig. 1). He had a history of abdominal aortic aneurysm and hypertension, and had smoked 15 cigarettes per day for 45 years. In October 2012, he underwent TURBT for a 5-cm bladder cancer on the right wall. The histopathological diagnosis was urothelial carcinoma, G2, pTa. Since then, the patient had undergone regular follow-up examinations and no recurrence had been observed. This time, however, intravesical recurrence was observed; thus, the patient was examined closely. Abdominal computed tomography (CT) showed a mass with calcification in the right wall. On magnetic resonance imaging (MRI), the tumor showed a high signal intensity on diffusion-weighted imaging, with no apparent muscle layer invasion, and the vesical imaging reporting and data system (VI-RADS) score was 1 point (Fig. 2). TURBT was performed in August 2019. Microscopic examination of the resected tissue showed spindle-shaped or star-shaped cells with irregularly enlarged nuclei, some of which showed unnatural formations of osteoid and cartilage tissue (Fig. 3 A/B). Immunostaining was positive for Desmin, SMA, Vimentin, Ki-67, and p53, and negative for CD34, c-kit, AE1/AE3, and p16 (Fig. 3 C/D). Since no urothelial carcinoma component was noted and no tumor was found in the systemic bone, we diagnosed the patient with bladder osteosarcoma. We discussed the treatment plan, including total cystectomy; however, owing to his advanced age and the lack of apparent muscle layer invasion on preoperative MRI, a second TURBT procedure was performed in October 2019. Histopathological examination revealed no malignant findings. At 29 months after surgery, the patient remains alive without recurrence.

Cystoscopy showing a 2 cm nodular tumor on the right wall. The arrow points to the tumor

A Abdominal computed tomography showing a mass with calcification on the right wall. Magnetic resonance imaging also showed the tumor. B Axial section of a T2-weighted image. C The tumor showed a high signal intensity on diffusion-weighted imaging. D Coronal section of a T2-weighted image. The arrow points to the tumor

A, B Microscopic examination of the resected tissue showing spindle-shaped or star-shaped cells with irregularly enlarged nuclei, some of which show unnatural formation of osteoid and cartilage tissue. A Low-power view of hematoxylin- and eosin-stained section. B High-power view of hematoxylin- and eosin-stained section. C Expression of Ki-67 analyzed by immunostaining. The labeling index was 30%. D Expression of p53 analyzed by immunostaining, showing diffuse positive images beyond the range of Ki-67 positivity
Discussion
Osteosarcomas that arise outside of bone are called extraskeletal osteosarcomas. They account for 4% of all osteosarcomas [1]. Radiation therapy, schistosomiasis, trauma, diverticula, use of chemotherapeutic agents (for example, cyclophosphamide), and frequent urinary tract infections are considered risk factors for primary extraskeletal osteosarcoma, including bladder osteosarcoma [2]. Allan et al. described the diagnostic criteria for extraskeletal osteosarcoma, as follows: (1) the presence of a uniform morphological pattern of sarcomatous tissue that excludes the possibility of malignant mesenchymoma, (2) the production of malignant osteoid or bone by the sarcomatous tissue, and (3) the exclusion of an osseous origin [3]. Osteosarcoma arising from the bladder is even rarer, with only 38 cases reported to date [2, 4,5,6,7,8,9]. The diagnosis of osteosarcoma of the bladder requires the exclusion of sarcomatoid changes of urothelial carcinoma, urothelial carcinoma with ossification, carcinoma with pseudosarcomatoid stromal reaction, malignant fibrous histiocytoma, synovial and epithelial sarcoma, and carcinosarcoma of the bladder [10] . Sarcomatoid carcinoma is diagnosed when a malignant epithelial component is identified, even in the presence of osteoid [7]. An immunohistochemical analysis of sarcomatoid carcinoma is at least focally positive for epithelial markers, cytokeratins, and epithelial membrane antigens. The presence of epithelial tumor cells of carcinoma in nests or clusters adjacent to the sarcoma cells is another feature that supports an epithelial origin [11]. On the other hand, osteosarcoma is immunohistochemically negative for pancytokeratins 7 and 20, epithelial membrane antigens, CD34, and CD68. Vimentin and p53 are strongly expressed [7] . Won et al. summarized 31 cases of osteosarcoma of the bladder in 2011 [4] . Since then, to our knowledge, 7 cases have been reported, including our case [2, 5,6,7,8,9], and a total of 38 cases are summarized in Additional file 1. For the reports that are available in English, a history of urothelial carcinoma of the bladder and a detailed prognosis have been added. The median age of the patients is 65.5 (24–86) years; however, the patients are often younger than patients with urothelial carcinoma. Many patients experience hematuria. Ours is the only case of urothelial carcinoma of the bladder that was detected without symptoms. Seven cases had a history of urothelial carcinoma of the bladder (two cases appeared at the same time), and had received treatments such as TURBT and tumor excision. Seven patients had obvious metastasis at the time of the diagnosis, and 24 patients did not have metastasis at the time of the diagnosis. Surgery (for example, total cystectomy or tumor excision) was performed in most cases, and radiation was added in four cases. Chemotherapy was also administered in five cases, but the prognosis was very poor, and many patients developed recurrence and died within 1 year. However, radiation therapy and chemotherapy may also have a certain effect, as there are reports of cases in which the primary tumor and bone metastasis showed a complete response to radiation [12], and cases in which ifosfamide, platinum, and methotrexate resulted in tumor shrinkage [13].There were seven patients who survived for more than 1 year. However, this is the only case in which long-term survival was achieved with TURBT alone. We think that this is due to the early detection of bladder cancer during regular follow-up examinations while it remained asymptomatic. Chitiyo identified four possible causes of the development of bladder osteosarcoma: transformation of the bladder epithelium, transformation of the stroma, transfer of osteoblasts by the bloodstream, and generation of osteoblasts from immature mesenchymal tissue derived from the Wolffian body, the developmental home of the bladder triangle [14]. Five patients had a history of treatment for urothelial carcinoma of the bladder, and treatment for urothelial carcinoma of the bladder may have stimulated the development of osteosarcoma. In addition, another three patients had a history of transurethral resection of the prostate (TURP) [8, 15, 16]. Although the site of bladder osteosarcoma was far from the bladder neck in all cases, transurethral surgery itself may be a risk factor for the development of bladder osteosarcoma. In this case, osteosarcoma appeared on the right wall, which is the same site as the initial urothelial carcinoma site, suggesting that stimulation by TURBT may have caused transformation of the bladder epithelium or stroma, resulting in the development of bladder osteosarcoma.
Conclusion
We herein described a case of bladder osteosarcoma. Although osteosarcoma of the urinary bladder has an extremely poor prognosis, in the present case, in which it was detected at an early stage without subjective symptoms, treatment with TURBT alone resulted in long-term survival without recurrence.
Availability of data and materials
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.
Abbreviations
- TURBT:
-
Transurethral resection of bladder tumor
- CT:
-
Computed tomography
- MRI:
-
Magnetic resonance imaging
- VI-RADS:
-
Vesical imaging reporting and data system
References
Heng M, Gupta A, Chung PW, Healey JH, Vaynrub M, Rose PS, et al. The role of chemotherapy and radiotherapy in localized extraskeletal osteosarcoma. Eur J Cancer. 2020;125:130–41.
Mremi A, Pyuza JJ, Bartholomeo N, Andongolile AA, Yahaya JJ. Diagnosis of primary osteosarcoma of the urinary bladder in a resource-limited setting: a case report and review of the literature. J Surg Case Rep. 2020. https://doi.org/10.1093/jscr/rjaa236.
Allan CJ, Soule EH. Osteogenic sarcoma of the somatic soft tissues. Clinicopathologic study of 26 cases and review of literature. Cancer. 1971;27:1121–33.
Won KY, Lee CH, Kim YW, Park YK. Primary giant-cell-rich osteosarcoma of the urinary bladder: usefulness of osteocalcin and osteonectin immunohistochemical staining and literature review. Pathology. 2011;43:161–4.
Papandreou C, Skopelitou A, Kappes G, Daouaher H. Primary osteosarcoma of the urinary bladder treated with external radiotherapy in a patient with a history of transitional cell carcinoma: a case report. J Med Case Rep. 2010;4:70.
Grubišić I, Leniček T, Tomas D, Džombeta T, Trnski D, Tomašković I, et al. Primary osteosarcoma of bladder diverticulum mimicking intradiverticular calculus: a case report. Diagn Pathol. 2011;6:37.
Siddappa JK, Singla S, Jain A, Kumar A, Rare A. Case of primary osteosarcoma of urinary bladder. J Clin Imaging Sci. 2012;2:82. https://doi.org/10.4103/2156-7514.105145.
Abou Ghaida RR, Saoud RM, Bulbul M. Primary osteosarcoma in a bladder diverticulum. Can J Urol. 2014;21:7393–5.
Almadani N, Alsaad KO, Al-Matrafi H, Al Hadab A, Abdullah N, AlKushi A. Urinary bladder radiotherapy-related chondroblastic osteosarcoma: rare case report and review of literature. Urol Ann. 2014;6(3):247–50. https://doi.org/10.4103/0974-7796.134289.
Berenson RJ, Flynn S, Freiha FS, Kempson RL, Torti FM. Primary osteogenic sarcoma of the bladder. Case report and review of the literature. Cancer. 1986;57:350–5.
Baydar DE, Himmetoglu C, Yazici S, Kiziloz H, Ozen H. Primary osteosarcoma of the urinary bladder following cyclophosphamide therapy for systemic lupus erythematosus: a case report. J Med Case Rep. 2009;3:39.
Van Oyen PM, Bergmans G, Denyhs H, et al. Primary osteogenic sarcoma of the bladder. Acta Urol Belg. 1987;55:380–2.
Phan CN, Wilkinson M, Cohen MB, Dunn S, Carroll P. Primary osteogenic sarcoma of the urinary bladder successfully treated with combination therapy. Urology. 1994;44:771–4. https://doi.org/10.1016/S0090-4295(94)80228-9.
Chitiyo ME. Primary osteogenic sarcoma of the urinary bladder. J Pathol. 1973;111:53–6.
Carter RD, Powers JH, van Hawn CZ. Osteogenic sarcoma and transitional cell carcinoma occurring simultaneously in the urinary bladder: report of a case. J Urol. 1956;76:263–9.
Nourse MH. Primary osteogenic sarcoma of the bladder. J Urol. 1957;77:634–8.
Acknowledgements
The authors wish to thank the patient for providing permission to share his case.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
KM and KN treated the patient. KM made the histopathological diagnosis. TO and KM wrote the first draft of the manuscript. All authors contributed to the writing of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Competing interests
The authors declare no competing interests in association with the present study.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Clinical characteristics of 38 cases of bladder osteosarcoma.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Oka, T., Matsuzaki, K., Izumi, H. et al. Osteosarcoma of the bladder: a case report. J Med Case Reports 16, 118 (2022). https://doi.org/10.1186/s13256-022-03346-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13256-022-03346-2