
Abstract
Background
Sinonasal teratocarcinosarcoma is a rare and aggressive malignancy with histological features of both carcinosarcoma and teratoma. The optimal management of this malignancy is unclear, with most patients being managed by a combination of surgery and radiotherapy.
Case presentation
We describe an 83-year-old white woman with sinonasal teratocarcinosarcoma of her left nasal cavity treated with surgical debulking initially with radiological evidence of residual disease which was treated with radiotherapy (60 Gy in 30 fractions). A follow-up examination at 2 years showed no evidence of recurrence.
Conclusions
In cases of sinonasal teratocarcinosarcoma with residual disease post-surgery, radiotherapy alone can be an effective option.
Similar content being viewed by others

Background
Sinonasal teratocarcinosarcoma (SNTCS) is an extremely rare malignant neoplasm of uncertain histogenesis [1]. It is highly malignant and locally aggressive, with a high recurrence rate. Almost all cases are found in adults with a significant male predominance [2]. Histopathological findings of this tumor comprise a complex malignant neoplasm that has combined features of teratoma and carcinosarcoma. Phenotypically, these tumors are composed of benign neural elements and various malignant epithelial and mesenchymal components [3]. The clinical features and treatment of patients with these tumors, therefore, remains to be addressed [4]. Here we present a case of SNTCS in an 83-year-old woman treated with debulking surgery and postoperative intensity-modulated radiation therapy (IMRT). There is no evidence of recurrence or complications at 2-year follow-up. This case highlights that radiotherapy alone can be effective post-surgery, and that IMRT is a promising modality in the treatment of SNTCS.
Case presentation
An 83-year-old white woman presented to her general practitioner initially with 1 month of nasal obstruction, intermittent epistaxis, and anosmia. This is on the background of atrial fibrillation, hypertension, and osteoarthritis. Her regular medications were apixaban, digoxin, amlodipine/valsartan, frusemide, metoprolol, and paracetamol with no known drug allergies. She lived with her son, mobilized independently with a walking stick, and was independent with all activities of daily living (ADLs) with an Eastern Cooperative Oncology Group (ECOG) score of one. She did not smoke tobacco and drank three to four standard units of alcohol per day.
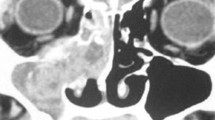
On examination, her vital signs were within normal range and the rest of the physical and neurological examinations were normal. Her blood pressure was within normal range at 120/70 mmHg. A nasal speculum examination found a large tissue growth in her left nasal cavity and a subsequent computed tomography (CT) scan revealed a large soft tissue mass opacifying the left maxillary, ethmoidal, frontal, and sphenoid sinuses – there was no intracranial extension (Fig. 1). Laboratory findings including a full blood count, renal function, and liver function were unremarkable. She was referred to the Ear, Nose, and Throat surgical team and underwent a debulking surgery.

Computed tomography scan revealing a large soft tissue mass opacifying the left maxillary, ethmoidal, frontal, and sphenoid sinuses
On frozen section the provisional diagnosis was a poorly differentiated squamous cell carcinoma on the basis of what was thought to be evidence of squamous differentiation in amongst a population of poorly differentiated cells. Only after processing and examination of the whole lesion was it appreciated that the tumor had both mature and immature components from more than one germ cell line.
A postoperative positron emission tomography (PET) scan revealed some ongoing soft tissue thickening in her left nasal cavity and her maxillary, ethmoid, and frontal sinuses with no evidence of distal fluorodeoxyglucose (FDG)-avid disease (Fig. 2). She received postoperative IMRT 60 Gy in 30 fractions to her sinuses. The treatment technique was a seven-field step-and-shoot IMRT plan with 80 control points. This was prescribed to a dose of 60 Gy. The difficulty in planning this was the close proximity of critical structures including brainstem and optic chiasm; the dose to the planning target volume (PTV) near these structures was reduced to 54 Gy in order to maintain tolerable dose constraints to these adjacent organs at risk. This resulted in a significant resolution of the tumor with no evidence of FDG-avid disease in her left maxillary sinus or nasal region on a repeat PET scan 6 months post-completion of radiotherapy (Fig. 3). We have followed her up closely at 3 monthly intervals and she had no evidence of local recurrence on nasal endoscopic examination at her 2-year follow-up.

Positron emission tomography scan after debulking surgery showing ongoing soft tissue thickening in the left nasal cavity and the maxillary, ethmoid, and frontal sinuses

Positron emission tomography scan post-completion of radiotherapy showing no fluorodeoxyglucose-avid disease
Discussion
SNTCS is a highly aggressive and rare malignant tumor with epithelial, mesenchymal, and neuroepithelial origins. The term was first used by Heffner and Hyams based on a case series with 20 patients with SNTCS [3]. This is a rare tumor with less than 100 cases being reported in the medical literature [5]. It is found mostly in adults with only a handful of pediatric cases being reported, and has a male predilection [6]. It is most commonly found in the nasal cavity, with involvement of the ethmoid sinus in approximately half of the patients and the maxillary sinus in approximately one-quarter of patients [7]. Intracranial extension is fairly common given the aggressive nature of the tumor [8].
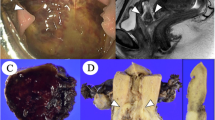
Only after formal examination of the whole specimen was it recognized both histologically and on immunohistochemistry that the tumor was a heterogeneous mixture of components from all three germ cell layers at varying degrees of differentiation. These included both mature benign glandular and stromal components (Fig. 4) along with immature malignant glandular and stromal components (Fig. 5). Parts of the undifferentiated component showed either CD-99 or synaptophysin positivity. This combination of features is considered to give rise to the diagnosis of a sinonasal teratocarcinosarcoma (malignant teratoma). It can then be seen that inadequate sampling can lead to frequent misdiagnosis particularly due to the rare nature of the tumor [9].

Mature benign glandular and stromal components of tumor

Immature malignant glandular and stromal components of tumor
On clinical examination, patients often present with nasal obstruction and epistaxis; however, they can also present with anosmia, headache, visual changes, and neurological symptoms [6].
The prognosis in SNTCS remains unclear, however, it is an aggressive tumor and recurrence and metastasis are common, with a recent systematic review of 71 cases quoting figures of approximately one-quarter having recurrence and 10% having metastasis [7]. Local invasion with intracranial extension can also occur. In Heffner and Hyams’ review of 20 cases, 12 died within 3 years with an average survival of 1.7 years [3]. However, in the eight cases that survived beyond 3 years there was no further recurrence or metastasis.
The optimal approach to treatment remains unclear in this condition due to the lack of large-scale studies given the rarity of the disease. A systematic review by Misra et al. consisting of 86 patients showed that the most common treatment modality was surgical resection followed by radiation therapy, with 51 cases out of 86 utilizing this approach [7]. The average dose of radiotherapy used was 55 Gy, and two case reports by Tokunaga et al. and Peng et al. have utilized IMRT with good effect, with no recurrence at 2 and 3.5 years respectively [10, 11]. Our case supports the use of IMRT given the excellent outcome in our patient with minimal side effects 2 years post-radiotherapy.
The role of adjuvant chemotherapy remains unclear; there is some suggestion that adjuvant chemotherapy can lead to better survival outcomes. Misra et al. reported an 88.8% survival rate at follow-up after an average of 32 months for those who received adjuvant chemotherapy in addition to surgery and radiation, as compared to 56.5% at 45 months for those who received surgery and radiation only [7, 12]. However, given the small number of cases that have utilized this approach a larger case series will lead to a better understanding of the efficacy of adjuvant chemotherapy for SNTCS.
Conclusions
This case demonstrates that radiotherapy alone can be an effective and well-tolerated treatment modality in patients with SNTCS who have residual disease post-surgery. Further larger scale studies should be conducted to clarify if there is a role for adjuvant chemotherapy.
Abbreviations
- ADLs:
-
Activities of daily living
- CT:
-
Computed tomography
- ECOG:
-
Eastern Cooperative Oncology Group
- FDG:
-
Fluorodeoxyglucose
- IMRT:
-
Intensity-modulated radiation therapy
- PET:
-
Positron emission tomography
- PTV:
-
Planning target volume
- SNTCS:
-
Sinonasal teratocarcinosarcoma
References
Redondo ME, Rey LA, Reguera PV, Bolanos RC. Sinonasal teratocarcinosarcoma. Acta Otorrinolaringol Esp. 1990;42(5):363–7.
Barnes L, Eveson J, Reichart P, Sidransky D. World Health Organisation Classification of Tumours: Pathology and genetics of head and neck tumours: International Agency for Research on Cancer. 2005.
Heffner DK, Hyams VJ. Teratocarcinosarcoma (malignant teratoma?) of the nasal cavity and paranasal sinuses: a clinicopathologic study of 20 cases. Cancer. 1984;53(10):2140–54.
Fernandez P, Cardesa A, Alos L, Pinto J, Traserra J. Sinonasal teratocarcinosarcoma: an unusual neoplasm. Pathol Res Pract. 1995;191(2):166–71.
Su Y-Y, Friedman M, Huang C-C, Wilson M, Lin H-C. Sinonasal teratocarcinosarcoma. Am J Otolaryngol. 2010;31(4):300–3.
Agrawal N, Chintagumpala M, Hicks J, Eldin K, Paulino AC. Sinonasal teratocarcinosarcoma in an adolescent male. J Pediatr Hematol Oncol. 2012;34(7):e304–7.
Misra P, Husain Q, Svider PF, Sanghvi S, Liu JK, Eloy JA. Management of sinonasal teratocarcinosarcoma: a systematic review. Am J Otolaryngol. 2014;35(1):5–11.
Shorter C, Nourbakhsh A, Dean M, Thomas-Ogunniyi J, Lian TS, Guthikonda B. Intracerebral metastasis of a sinonasal teratocarcinosarcoma: a case report. Skull Base. 2010;20(05):393–6.
Terasaka S, Medary MB, Whiting DM, Fukushima T, Espejo EJ, Nathan G. Prolonged survival in a patient with sinonasal teratocarcinosarcoma with cranial extension: case report. J Neurosurg. 1998;88(4):753–6.
Peng G, Ke Y, Wang T, Feng Y, Li Y, Wu G. Intensity-modulated radiotherapy for sinonasal teratocarcinosarcoma. J Huazhong Univ Sci Technolog Med Sci. 2011;31:857–60.
Tokunaga T, Sunaga H, Kimura Y, Tsuda G, Fujieda S. A case of sinonasal teratocarcinosarcoma treated with surgery and post-operative intensity-modulated radiotherapy (IMRT). Auris Nasus Larynx. 2012;39(6):641–5.
Budrukkar A, Agarwal J, Kane S, Siddha M, Laskar SG, Pai P, et al. Management and clinical outcome of sinonasal teratocarcinosarcoma: single institution experience. J Laryngol Otol. 2010;124(07):739–43.
Acknowledgements
We would like to acknowledge Lynne Dove for her assistance with the manuscript.
Funding
We have no sources of funding to declare.
Availability of data and materials
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.
Authors’ contributions
YCF drafted the manuscript. VM carried out the immunohistochemistry. NN performed the initial debulking surgery and had ongoing follow-ups with the patient. LH participated in the radiotherapy planning. RA participated in the radiotherapy planning and drafting the manuscript. All authors read and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Ethics approval and consent to participate
Not applicable.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Foong, Y.C., Murdolo, V., Naiman, N. et al. Sinonasal teratocarcinosarcoma: a case report. J Med Case Reports 11, 167 (2017). https://doi.org/10.1186/s13256-017-1327-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13256-017-1327-y