
Abstract
Background
To develop and validate an MRI texture-based machine learning model for the noninvasive assessment of renal function.
Methods
A retrospective study of 174 diabetic patients (training cohort, n = 123; validation cohort, n = 51) who underwent renal MRI scans was included. They were assigned to normal function (n = 71), mild or moderate impairment (n = 69), and severe impairment groups (n = 34) according to renal function. Four methods of kidney segmentation on T2-weighted images (T2WI) were compared, including regions of interest covering all coronal slices (All-K), the largest coronal slices (LC-K), and subregions of the largest coronal slices (TLCO-K and PIZZA-K). The speeded-up robust features (SURF) and support vector machine (SVM) algorithms were used for texture feature extraction and model construction, respectively. Receiver operating characteristic (ROC) curve analysis was used to evaluate the diagnostic performance of models.
Results
The models based on LC-K and All-K achieved the nonsignificantly highest accuracy in the classification of renal function (all p values > 0.05). The optimal model yielded high performance in classifying the normal function, mild or moderate impairment, and severe impairment, with an area under the curve of 0.938 (95% confidence interval [CI] 0.935–0.940), 0.919 (95%CI 0.916–0.922), and 0.959 (95%CI 0.956–0.962) in the training cohorts, respectively, as well as 0.802 (95%CI 0.800–0.807), 0.852 (95%CI 0.846–0.857), and 0.863 (95%CI 0.857–0.887) in the validation cohorts, respectively.
Conclusion
We developed and internally validated an MRI-based machine-learning model that can accurately evaluate renal function. Once externally validated, this model has the potential to facilitate the monitoring of patients with impaired renal function.
Key points
-
1.
Texture analysis based on coronal T2-weighted MR images could evaluate the renal function in patients with diabetes.
-
2.
The All-K and LC-K outperformed other segmentation methods in the evaluation of renal function impairment.
-
3.
The segmentation methods could affect the results of renal function evaluation and the integrity of the coronal slices was crucial for renal imaging texture analysis.
Similar content being viewed by others


Background
Chronic kidney disease (CKD) is a global health and economic burden and a raising cause of global deaths [1]. Diabetes and hypertension are the two main causes of CKD and subsequent end-stage kidney disease [2]. Early detection of renal function impairment is of great importance for promptly potent treatment strategies and eventually preventing renal dysfunction deterioration [3]. Chronic hypoxia and fibrosis are a vicious circle leading to renal functional and structural damages [4]. In clinical settings, it is meaningful to develop accurate and reliable biomarkers for detecting early renal function impairment and monitoring the disease progression.
Functional magnetic resonance imaging (fMRI) has been used to evaluate renal oxygenation and fibrosis [5,6,7]. Blood oxygenation level-dependent (BOLD) and arterial spin labeling (ASL) MRI has been performed to assess renal oxygenation changes as the renal function declined [8, 9]. Diffusion tensor imaging (DTI) and intravoxel incoherent motion diffusion-weighted imaging (IVIM-DWI) are semiquantitative methods to assess the fibrotic process during the chronic renal dysfunction [10, 11]. The fMRI techniques allow for quantifying and visualizing the renal function impairment on images; however, they suffer from low interobserver reproducibility and additional time and cost. Thus, fMRI is still not routinely used to evaluate the renal function.
With the advances in image analysis techniques in recent years, we can extract invisible textural features from MR images, which provides meaningful information to reflect the tissue heterogeneity [12, 13]. The degree of fibrosis was correlated with the imaging textures extracted from computed tomography and MRI on liver cirrhosis [14, 15]. Similarly, imaging textures of kidneys are potential biomarkers to reflect fibrosis and determine the estimated glomerular filtration rate (eGFR) and CKD status [16]. On MRI, the abundant features were indicative of renal function changes. The T2-weighted images (T2WI) are a commonly used sequence that can demonstrate the structures, cellular edema, fibrils and other underlying pathophysiology of some diseases [17, 18]. Texture analyses on T2WI have been used to evaluate the early renal function of the transplanted kidney and diabetic nephropathy, respectively [18, 19]. Therefore, the texture analysis on T2WI is able to reflect the pathological status of kidneys. However, the ROIs were variable in previous renal studies, which affect the process of model construction and performance [16, 18,19,20,21]. Thus, we aimed to investigate the value of texture analysis on T2WI in evaluating renal function and standardize the renal ROI segmentation method.
Methods
Subjects
This observational cohort study was approved by the institutional review board of our hospital. Written informed consent was obtained from each participant for renal MRI. Consecutive patients with hypertension and diabetes between October 2013 and November 2019 were recruited prospectively for renal MRI examination, and as the technique of imaging processing method developed, we retrospectively reviewed and secondary analyzed their images. The serum creatinine was obtained before and after one week of the date of MRI examination and eGFR was calculated by CKD Epidemiology Collaboration (CKD-EPI) 2009 (formula in Additional file 1). Patients with CKD1 (eGFR ≥ 90 mL/min/1.73 m2) are regarded as normal renal function, CKD2 and CKD3 (30 mL/min/1.73 m2 ≥ eGFR < 90 mL/min/1.73 m2) as mild or moderate renal function impairment, and CKD4 and CKD5 (eGFR < 30 mL/min/1.73 m2) as severe renal function impairment. The exclusion criteria were as follows: (1) coronal T2WI with severe artifacts; (2) patients with polycystic kidney diseases or acute renal injury; (3) patients who were using medications that can affect the creatinine level (e.g., cimetidine, trimethoprim, or cefotaxime); and (4) patients with poor control of hypertension. Finally, a total of 174 patients were enrolled for analysis. The patients were randomly assigned to the training cohort (n = 123) and the validation cohort (n = 51).
MRI acquisition and preprocessing
All patients underwent MR examination at 3.0 T (Discovery MR 750, GE Healthcare, Milwaukee, WI, USA). The acquisition parameters were as follows: axial T1WI: repetition time (TR) = 6.2 (ms), echo time (TE) = 2.8 (ms), field of view (FOV) = 100 (mm2), matrix = 512 × 512, slice thickness = 4 mm, flip angle = 20°, bandwidth = 162.773 Hz/pixel; Coronal T2WI: TR = 1984 (ms), TE = 70 (ms), FOV = 100 (mm2), matrix = 512 × 512, slice thickness = 4.0 mm, flip angle = 90°, bandwidth = 325.508 Hz/pixel. Due to the differences between patients, the intensity range of T2WI was normalized to 0–255 by mean–variance normalization to reduce the influence on texture analysis.
MR kidney image segmentation
The bilateral kidneys were manually segmented on coronal T2WI using ITK-SNAP software (version 3.6.0, https://itk.org/) by a radiologist with 5-year diagnostic experience (Z.C., reader 1). Then 30 patients were randomly selected and segmented by a radiologist with 8-year diagnostic experience (X.M., reader 2) and reader 1 again. Disagreements between 2 readers reached a consensus through a discussion with an expert on abdominal radiology. To assess the influence of segmentation methods on the results of models for renal function evaluation, we compared four different kidney segmentation methods: (1) All-K: all coronal slices of renal parenchyma were delineated on two kidneys; (2) LC-K: the largest coronal slices crossing renal hilum of bilateral renal parenchyma were outlined; (3) TLCO-K: the largest coronal slices were segmented concentrically from the outer to the inner layers into 12 equal layers; (4) PIZZA-K: the largest coronal slices were segmented like a pizza, renal hilum as the center of the circle, upper and lower poles as edges, and it was divided into 6 parts with the equal degree. The four types of segmentation are demonstrated in Fig. 1.

The four segmentation methods on the model construction for renal function evaluation. Note: All-K, all coronal slices of kidneys; LC-K, the largest coronal slices of kidneys; TLCO-K, 12 layers of the largest coronal slices of kidneys; PIZZA, 6 pieces of the largest coronal slices of kidneys
Texture extraction and model construction
The speeded up robust features (SURF) algorithm was used to detect and describe the local imaging features. Corner points were identified and 64 descriptor vectors were generated to describe each interest point. Because the corners points conducted by SURF from each ROI were different, the number of descriptor vectors was thus different. The process of SURF is described in Additional file 1. To obtain the same number of imaging features in the four segmentation methods, the bag of words (BoW) model was used to cluster similar features and describe their frequencies. The reduced imaging features by BoW were used for features selection and model construction. The reproducibility of features was evaluated by inter-/intraclass correlation coefficients (ICCs). When ICCs were more than 0.75, features were with good reproducibility. Additionally, age and gender were incorporated for their contribution to calculating eGFR. Both the imaging features and clinical characteristics entered into the support vector machine (SVM) to build a T2WI-based model for renal function evaluation. The receiver operating characteristic (ROC) curve analysis was used to evaluate the performance of SVM models, including area under the curve (AUC), sensitivity, specificity, and accuracy. We developed the models in the training cohort and validated them in the validation cohort.
Statistics
An independent samples t-test and χ2 test were used to compare the clinical characteristics of training and validation cohorts when appropriate. Sensitivity, specificity, accuracy, and AUC were used to evaluate the performance of models. Delong test was used to compare AUC values. p < 0.05 with two-sided was considered significant. All statistical analyses were implemented in 2018 Python 3.6.5 (https://www.python.org/). “NumPy” package was used to standardize the intensity range of T2WI. “OpenCV” was applied for image masking, kidney segmentation, and feature extraction. “random” package was used for random assignment of training and validation cohorts. “pengouin” package was used to calculate ICCs. “scikit-learn” package was used for SVM. The ROC curves were plotted by the “matplotlib” package.
Results
In a total of 174 patients were analyzed among 188 patients, 9 of them were excluded for motion artifacts on T2WI, and 5 of them were excluded for multiple renal cysts (occupying one-third of the renal parenchyma). Among 174 patients, 71 were categorized into the normal renal function group, 69 into the mild-moderate renal function impairment group, and 34 into the severe renal function impairment group. They were randomly assigned to the training cohort and the validation cohort (Table 1). No significant difference existed between training and validation cohorts (p > 0.05).
Reproducibility of features among four segmentations
Bilateral kidneys were outlined by reader 1 and reader 2 and ICCs were analyzed. More than 83% of features in All-K, LC-K, TLCO-K, and PIZZA-K segmentations were reproducible (ICCs > 0.75).
Performance of the four models in identifying normal renal function
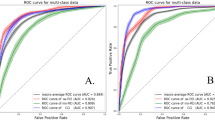
The four models based on different segmentation methods showed good performance in identifying the patients with normal renal function (Table 2 and Fig. 2a). In the training cohort, the All-K-, LC-K-, TLCO-K-, and PIZZA-K-based models yielded an AUC of 0.877 (95%CI 0.870–0.884), 0.938 (95%CI 0.935–0.940), 0.922 (95%CI 0.912–0.928), and 0.922 (95%CI 0.914–0.929), respectively, while in the validation cohort, the four models yielded an AUC of 0.866 (95%CI 0.863–0.870), 0.802 (95%CI 0.800–0.807), 0.800 (95%CI 0.785–0.816), and 0.800 (95%CI 0.784–0.958), respectively. No significant difference was found among the four models in identifying the normal renal function (All p values > 0.05).

The ROC curves of four models on normal renal function, mild or moderate and severe renal function impairment in the training and validation cohorts. Note: ROC, receiver operating characteristic; RF, renal function
Performance of the four models in identifying mild or moderate renal function impairment
The four models based on different segmentation methods showed good performance in identifying the patients with mild or moderate renal function impairment (Table 3 and Fig. 2b). In the training cohort, the All-K-, LC-K-, TLCO-K-, and PIZZA-K-based models achieved an AUC of 0.888 (95%CI 0.881–0.895), 0.919 (95%CI 0.916–0.922), 0.926 (95%CI 0.919–0.932), and 0.867 (95%CI 0.860–0.874), respectively, while in the validation cohort, the four models achieved an AUC of 0.820 (95%CI 0.817–0.823), 0.852 (95%CI 0.846–0.857), 0.705 (95%CI 0.691–0.720), and 0.705 (95%CI 0.690–0.721), respectively. No significant difference was observed among the four models in identifying the mild or moderate renal function impairment (All p values > 0.05).
Performance of the four models in identifying severe renal function impairment
The All-K- and LC-K-based models showed excellent performance in identifying severe renal function impairment (Table 4 and Fig. 2c). The All-K-based model obtained an AUC of 0.974 (95%CI 0.967–0.982) and 0.938 (95%CI 0.934–0.941) in the training and validation cohorts, respectively. The LC-K-based model demonstrated an AUC of 0.959 (95%CI 0.956–0.962) and 0.863 (95%CI 0.857–0.887) in the training and validation cohorts, respectively. However, the performance of TLCO-K- and PIZZA-K-based models showed a big gap in the two cohorts, suggesting potential model overfitting. The TLCO-K-based model obtained an AUC of 0.970 (95%CI 0.964–0.977) in the training cohort whereas 0.314 (95%CI 0.201–0. 426) in the validation cohort. The PIZZA-K-based model obtained an AUC of 0.994 (95%CI 0.986–1.00) in the training cohort and 0.688 (95%CI 0.673–0.704) in the validation cohort. The All-K-based model showed significantly better performance than TLCO-K- and PIZZA-K-based models in the validation cohort (p = 0.009 and 0.009, respectively).
Discussion
This current study demonstrated the good performance of texture-based MRI models in the evaluation of renal function impairment. The four machine learning models were similar in identifying normal renal function (AUC ≥ 0.800 in the validation cohorts). Interestingly, All-K- and LC-K-based models were more stable and reliable than TLCO-K- and PIZZA-K-based models when assessing impaired renal function.
T2WI is a routine and stable sequence and decreased signal intensity represents more fibrocollagenous stroma within the tissue. As fibrosis is the result of renal ischemia and inflammation, the degree of fibrosis reflects the status of renal function [22]. Subtle renal fibrosis is not identifiable with naked eyes based on T2WI, but the length of kidneys decreases as renal function deteriorates [23]. These subtle changes are transferred into the changes of a great number of texture features. Texture analysis on T2WI has been investigated in classifying the stages of liver cirrhosis [24]. But as for hemosiderin sedation and fibrosis in liver cirrhosis, hypointense hemosiderin on T2WI masks the fibrotic changes and lead to poor performance in further research [25]. However, renal fibrosis is mainly characterized by glomerulosclerosis, tubulointerstitial fibrosis, and tubular atrophy but a certain of hemosiderin deposition. Therefore, renal fibrosis results in more significant change of signal intensity on T2WI than hemosiderin deposition. On the other hand, the DWI, DTI, and IVIM were generated by changing scanning parameters based on T2WI, which has made the underlying fibrosis visible and measurable. Therefore, renal texture analysis on T2WI has provided an alternative method for evaluating the degree of renal fibrosis and detecting early renal function impairment.
ROI segmentation is an essential step in texture analysis and subsequent model construction. The models based on 4 segmentations have achieved good performance in training and validation cohorts when identifying normal renal function. And it has revealed that normal renal structure changed too little to yield difference among the whole kidneys, the largest coronal slices, or subregional segmentations of the largest coronal slices on texture analysis. However, subtle structures changed as renal function declined. The All-K- and LC-K-based models outperformed the TLCO-K- and PIZZA-K-based models in assessing the mild or moderate and severe renal function impairment. It may infer that the integrity of coronal slices is significant to reflect the renal texture changes during the chronic process of renal dysfunction. Meanwhile, the All-K consisted of LC-K and other coronal slices, but the All-K-based model did not significantly better than the LC-K-based model. This may be due to feature redundancy from too many coronal ROI sections in All-K. Feature redundancy referred to the strong correlations between texture features among slices. Thus, the imaging textures from LC-K were representative of the corresponding kidney. Our finding was in accordance with previous fMRI studies which measured the values on the coronal slices [26, 27]. Both All-K and LC-K were feasible segmentation methods for establishing a robust and effective model to evaluate renal function.
Renal function was determined by the glomerular mainly in the cortex and renal tubules in the medulla. The remarkable pathological changes of advanced renal dysfunction blurred the boundary between the renal cortex and medulla. The cortico-medullary areas were related to renal oxygenation, eGFR and the progression of chronic kidney diseases [28, 29], yet their textures were under-investigated in TLCO-K and PIZZA-K segmentations. The performance of the PIZZA-K-based model was better than the TLCO-K-based model in identifying severe renal function impairment. It might reveal that the integrity of cortico-medullary areas on texture analysis was important in evaluating renal function. Meanwhile, the abundant texture features from layers or pieces led to overfitting in the training cohort when identifying the severe renal function impairment. The overfitting suggested the TLCO-K- and PIZZA-K-based models were rather complicated and their generalization ability was poor. The indifferent results referred that the separation of texture analysis of renal cortex or medulla or segmental renal areas was inappropriate in the evaluation of impaired renal function. Although the imaging models built by the subregional ROI analysis within the lesion outperformed the ones from the primary whole lesion on tumor studies for the abundant heterogeneity [30,31,32], the subregional ROI texture analysis may not show good performance in non-tumoral diseases. Our study has proven that texture analysis models based on the integral largest coronal slices or the whole organs for chronic kidney diseases showed a satisfying performance.
This study has some limitations. First, the sample size was relatively small. MRI examination is not a routine examination for patients with chronic renal function impairment. We categorized patients into 3 renal function groups on evaluation of MRI-texture-based models for the uneven distribution of eGFR. Second, we only investigated the four ROI segmentations on coronal slices of T2WI. The predictive value of various segmentations on axial slices remains unknown, which needs further study. However, the largest coronal slices contained more information than the largest axial slices, and the former has been commonly used in fMRI studies. Thirdly, our study was based on T2WI only, the predictive value of other MRI or fMRI sequences was not discussed. T2WI as a routine sequence makes it more convenient to obtain. Moreover, the models constructed from T2WI were easy-to-use in other institutions compared to the extra fMRI.
In conclusion, we developed and validated a texture-based MRI model to evaluate renal function, which offers an alternative tool to detect renal impairment. Furthermore, texture analysis on MRI should be on the integral coronal slices or the whole coronal slices of the kidney, which would develop more robust models than the subregional segmentations-based models for assessing the different status of renal function. The stable segmentations on renal MRI texture analysis will promote future studies of other nephropathies and predict the risk of renal function decline of CKD.
Availability of data and materials
The datasets generated and/or analyzed during the current study are not publicly available due to the ongoing further studies but are available from the corresponding author on reasonable request.
Abbreviations
- All-K:
-
All coronal slices
- ASL:
-
Arterial spin labeling
- BOLD:
-
Blood oxygenation level-dependent
- CKD:
-
Chronic kidney diseases
- DTI:
-
Diffusion tensor imaging
- DWI:
-
Diffusion-weighted imaging
- eGFR:
-
Estimated glomerular filtration rate
- IVIM:
-
Intravoxel incoherent motion
- LC-K:
-
The largest coronal slice
- PIZZA-K:
-
Six pieces segmentation of the largest coronal slice
- ROI:
-
Region of interest
- SURF:
-
Speeded up robust features
- T2WI:
-
T2-weighted images
- TLCO-K:
-
Twelve concentric objective segmentation of the largest coronal slice
References
Collaboration GBDCKD (2020) Global, regional, and national burden of chronic kidney disease, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 395:709–733. https://doi.org/10.1016/S0140-6736(20)30045-3
Webster AC, Nagler EV, Morton RL, Masson P (2017) Chronic kidney disease. Lancet 389:1238–1252. https://doi.org/10.1016/S0140-6736(16)32064-5
Gigante A, Proietti M, Petrillo E, Mannucci PM, Nobili A, Muscaritoli M (2021) Renal function, cardiovascular diseases, appropriateness of drug prescription and outcomes in hospitalized older patients. Drugs Aging 38:1097–1105. https://doi.org/10.1007/s40266-021-00903-0
Kawakami T, Mimura I, Shoji K, Tanaka T, Nangaku M (2014) Hypoxia and fibrosis in chronic kidney disease: crossing at pericytes. Kidney Int Suppl 4:107–112. https://doi.org/10.1038/kisup.2014.20
Eckerbom P, Hansell P, Cox E et al (2019) Multiparametric assessment of renal physiology in healthy volunteers using noninvasive magnetic resonance imaging. Am J Physiol Renal Physiol 316:F693–F702. https://doi.org/10.1152/ajprenal.00486.2018
Mao W, Zhou J, Zeng M et al (2018) Intravoxel incoherent motion diffusion-weighted imaging for the assessment of renal fibrosis of chronic kidney disease: a preliminary study. Magn Reson Imaging 47:118–124. https://doi.org/10.1016/j.mri.2017.12.010
Inoue T, Kozawa E, Okada H et al (2011) Noninvasive evaluation of kidney hypoxia and fibrosis using magnetic resonance imaging. J Am Soc Nephrol 22:1429–1434. https://doi.org/10.1681/ASN.2010111143
Khatir DS, Pedersen M, Jespersen B, Buus NH (2015) Evaluation of renal blood flow and oxygenation in CKD using magnetic resonance imaging. Am J Kidney Dis 66:402–411. https://doi.org/10.1053/j.ajkd.2014.11.022
Mora-Gutierrez JM, Garcia-Fernandez N, Slon Roblero MF et al (2017) Arterial spin labeling MRI is able to detect early hemodynamic changes in diabetic nephropathy. J Magn Reson Imaging 46:1810–1817. https://doi.org/10.1002/jmri.25717
Wang YC, Feng Y, Lu CQ, Ju S (2018) Renal fat fraction and diffusion tensor imaging in patients with early-stage diabetic nephropathy. Eur Radiol 28:3326–3334. https://doi.org/10.1007/s00330-017-5298-6
Zhang H, Wang P, Shi D et al (2022) Capability of intravoxel incoherent motion and diffusion tensor imaging to detect early kidney injury in type 2 diabetes. Eur Radiol. https://doi.org/10.1007/s00330-021-08415-6
Lambin P, Rios-Velazquez E, Leijenaar R et al (2012) Radiomics: extracting more information from medical images using advanced feature analysis. Eur J Cancer 48:441–446. https://doi.org/10.1016/j.ejca.2011.11.036
Gillies RJ, Kinahan PE, Hricak H (2016) Radiomics: images are more than pictures, they are data. Radiology 278:563–577. https://doi.org/10.1148/radiol.2015151169
Lubner MG, Pickhardt PJ (2018) Multidetector computed tomography for retrospective, noninvasive staging of liver fibrosis. Gastroenterol Clin North Am 47:569–584. https://doi.org/10.1016/j.gtc.2018.04.012
Zhang X, Gao X, Liu BJ et al (2015) Effective staging of fibrosis by the selected texture features of liver: which one is better, CT or MR imaging? Comput Med Imaging Graph 46(Pt 2):227–236. https://doi.org/10.1016/j.compmedimag.2015.09.003
Kuo CC, Chang CM, Liu KT et al (2019) Automation of the kidney function prediction and classification through ultrasound-based kidney imaging using deep learning. NPJ Digit Med 2:29. https://doi.org/10.1038/s41746-019-0104-2
Huang S, Shi K, Zhang Y et al (2022) Texture analysis of T2-weighted cardiovascular magnetic resonance imaging to discriminate between cardiac amyloidosis and hypertrophic cardiomyopathy. BMC Cardiovasc Disord 22:235. https://doi.org/10.1186/s12872-022-02671-0
Yu B, Huang C, Fan X et al (2022) Application of MR imaging features in differentiation of renal changes in patients with stage III type 2 diabetic nephropathy and normal subjects. Front Endocrinol (Lausanne) 13:846407. https://doi.org/10.3389/fendo.2022.846407
Grzywińska M, Jankowska M, Banach-Ambroziak E, Szurowska E, Dębska-Ślizień A (2020) Computation of the texture features on T2-weighted images as a novel method to assess the function of the transplanted kidney: primary research. Transplant Proc 52:2062–2066. https://doi.org/10.1016/j.transproceed.2020.02.084
Ding J, Xing Z, Jiang Z et al (2019) Evaluation of renal dysfunction using texture analysis based on DWI, BOLD, and susceptibility-weighted imaging. Eur Radiol 29:2293–2301. https://doi.org/10.1007/s00330-018-5911-3
Deng Y, Yang BR, Luo JW, Du GX, Luo LP (2020) DTI-based radiomics signature for the detection of early diabetic kidney damage. Abdom Radiol (NY) 45:2526–2531. https://doi.org/10.1007/s00261-020-02576-6
Berchtold L, Friedli I, Crowe LA et al (2020) Validation of the corticomedullary difference in magnetic resonance imaging-derived apparent diffusion coefficient for kidney fibrosis detection: a cross-sectional study. Nephrol Dial Transplant 35:937–945. https://doi.org/10.1093/ndt/gfy389
Lin HY, Lee YL, Lin KD et al (2017) Association of renal elasticity and renal function progression in patients with chronic kidney disease evaluated by real-time ultrasound elastography. Sci Rep 7:43303. https://doi.org/10.1038/srep43303
Chunmei X, Mei H, Yan Z, Haiying W (2019) Diagnostic method of liver cirrhosis based on MR image texture feature extraction and classification algorithm. J Med Syst 44:11. https://doi.org/10.1007/s10916-019-1508-x
Schawkat K, Ciritsis A, von Ulmenstein S et al (2020) Diagnostic accuracy of texture analysis and machine learning for quantification of liver fibrosis in MRI: correlation with MR elastography and histopathology. Eur Radiol 30:4675–4685. https://doi.org/10.1007/s00330-020-06831-8
Niles DJ, Artz NS, Djamali A, Sadowski EA, Grist TM, Fain SB (2016) Longitudinal assessment of renal perfusion and oxygenation in transplant donor-recipient pairs using arterial spin labeling and blood oxygen level-dependent magnetic resonance imaging. Invest Radiol 51:113–120. https://doi.org/10.1097/RLI.0000000000000210
Sigmund EE, Vivier PH, Sui D et al (2012) Intravoxel incoherent motion and diffusion-tensor imaging in renal tissue under hydration and furosemide flow challenges. Radiology 263:758–769. https://doi.org/10.1148/radiol.12111327
Milani B, Ansaloni A, Sousa-Guimaraes S et al (2017) Reduction of cortical oxygenation in chronic kidney disease: evidence obtained with a new analysis method of blood oxygenation level-dependent magnetic resonance imaging. Nephrol Dial Transplant Off Publ Eur Dial Transpl Assoc Eur Renal Assoc 32:2097–2105. https://doi.org/10.1093/ndt/gfw362
Pruijm M, Milani B, Pivin E et al (2018) Reduced cortical oxygenation predicts a progressive decline of renal function in patients with chronic kidney disease. Kidney Int 93:932–940. https://doi.org/10.1016/j.kint.2017.10.020
Chaddad A, Daniel P, Desrosiers C, Toews M, Abdulkarim B (2019) Novel radiomic features based on joint intensity matrices for predicting glioblastoma patient survival time. IEEE J Biomed Health Inform 23:795–804. https://doi.org/10.1109/JBHI.2018.2825027
Xie C, Yang P, Zhang X et al (2019) Sub-region based radiomics analysis for survival prediction in oesophageal tumours treated by definitive concurrent chemoradiotherapy. EBioMedicine 44:289–297. https://doi.org/10.1016/j.ebiom.2019.05.023
Xu H, Lv W, Feng H et al (2020) Subregional radiomics analysis of PET/CT imaging with intratumor partitioning: application to prognosis for nasopharyngeal carcinoma. Mol Imaging Biol 22:1414–1426. https://doi.org/10.1007/s11307-019-01439-x
Acknowledgements
This work is supported by the National Natural Science Foundation of China (81871323, 81801665, 81901709); the Natural Science Foundation of Guangdong Province (2018B030311024, 2019A1515011918).
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
XM, WC, SZ, and BZ conceptualized and designed the study and methodology. XM wrote the main manuscript. WC and BZ performed the imaging texture analysis and main statistical analysis. SZ reviewed and edited the manuscript. LZ, XW, and YC collected the imaging and clinical data. SC, ZC, XM and YG delineated the region of interests. QC, ZJ, and ML reorganized the results. LC, JY, and ZX contributed to data visualization and figures production. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Our study was approved by the ethics committee of the First Affiliated Hospital of Jinan University.
Consent for publication
Consent to publish was obtained from all participants.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Supplementary materials.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Mo, X., Chen, W., Chen, S. et al. MRI texture-based machine learning models for the evaluation of renal function on different segmentations: a proof-of-concept study. Insights Imaging 14, 28 (2023). https://doi.org/10.1186/s13244-023-01370-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13244-023-01370-4