
Abstract
Background
Both Alzheimer’s disease (AD) genetic risk factors and indices of cognitive reserve (CR) influence risk of cognitive decline, but it remains unclear whether they interact. This study examined whether a CR index score modifies the relationship between AD genetic risk factors and long-term cognitive trajectories in a large sample of individuals with normal cognition.
Methods
Analyses used data from the Preclinical AD Consortium, including harmonized data from 5 longitudinal cohort studies. Participants were cognitively normal at baseline (M baseline age = 64 years, 59% female) and underwent 10 years of follow-up, on average. AD genetic risk was measured by (i) apolipoprotein-E (APOE) genetic status (APOE-ε2 and APOE-ε4 vs. APOE-ε3; N = 1819) and (ii) AD polygenic risk scores (AD-PRS; N = 1175). A CR index was calculated by combining years of education and literacy scores. Longitudinal cognitive performance was measured by harmonized factor scores for global cognition, episodic memory, and executive function.
Results
In mixed-effects models, higher CR index scores were associated with better baseline cognitive performance for all cognitive outcomes. APOE-ε4 genotype and AD-PRS that included the APOE region (AD-PRSAPOE) were associated with declines in all cognitive domains, whereas AD-PRS that excluded the APOE region (AD-PRSw/oAPOE) was associated with declines in executive function and global cognition, but not memory. There were significant 3-way CR index score × APOE-ε4 × time interactions for the global (p = 0.04, effect size = 0.16) and memory scores (p = 0.01, effect size = 0.22), indicating the negative effect of APOE-ε4 genotype on global and episodic memory score change was attenuated among individuals with higher CR index scores. In contrast, levels of CR did not attenuate APOE-ε4-related declines in executive function or declines associated with higher AD-PRS. APOE-ε2 genotype was unrelated to cognition.
Conclusions
These results suggest that APOE-ε4 and non-APOE-ε4 AD polygenic risk are independently associated with global cognitive and executive function declines among individuals with normal cognition at baseline, but only APOE-ε4 is associated with declines in episodic memory. Importantly, higher levels of CR may mitigate APOE-ε4-related declines in some cognitive domains. Future research is needed to address study limitations, including generalizability due to cohort demographic characteristics.
Similar content being viewed by others

Background
In the coming decades, the prevalence and burden of Alzheimer’s disease (AD) and related dementias is projected to increase with the growth and aging of the population [1]. The lack of effective treatments for AD has led to an increased focus on potentially modifiable lifestyle factors that may mitigate dementia risk [2]. For example, variables reflecting lifetime cognitive experiences, such as more years of education, higher scores on literacy tests, and greater engagement in cognitively stimulating activities, are associated with better cognitive performance and a delayed onset of clinical symptoms of AD [3, 4]. These variables have been used as proxy measures of cognitive reserve (CR), a theoretical construct most recently defined as a property of the brain that allows for better-than-expected cognitive performance given age- and disease-related brain changes [5]. In contrast, several genetic risk factors increase the likelihood of cognitive decline and late onset AD dementia [6]. However, the extent to which CR proxy measures mitigate the relationship between genetic risk for AD and cognitive decline among individuals with normal cognition is not well understood.
The ε4 allele of the apolipoprotein-E gene (APOE-ε4) is a well-known risk factor for late onset AD dementia [7, 8], whereas the APOE ε2 allele (APOE-ε2) is associated with a reduced risk of AD dementia [9, 10]. Because other genetic factors additionally contribute to AD dementia risk, recent studies have examined polygenic risk scores for Alzheimer’s disease (AD-PRS), which combine the cumulative impact of multiple AD-associated genetic loci, as identified by genome-wide association studies (GWAS) (e.g., [6]). Like APOE, AD-PRS are also associated with increased risk of late onset AD dementia (e.g., [11,12,13,14]), though the magnitude of this risk tends to be smaller when removing the strong APOE effect from the score.
Studies examining the relationship of CR proxy measures and APOE-ε4 carrier status to longitudinal cognitive decline have been most often conducted among individuals across the clinical spectrum (i.e., including combined groups of participants who are cognitively normal and have mild cognitive impairment (MCI) or those with normal cognition, MCI, and dementia). The results of these studies are mixed, with some finding that higher levels of CR attenuate APOE-ε4-related decline in global cognition [15,16,17,18,19,20], while others did not find such associations [21,22,23,24,25]. Moreover, studies among individuals with normal cognition at baseline are more limited. One study that included older adults (M age =75.9 years) reported that more years of education attenuated APOE-ε4-related declines in a memory composite score but not declines in language or visuospatial/reasoning composite scores [26]. However, other studies among largely middle-aged cohorts [27] or with smaller sample sizes [28] have reported no interaction between CR proxy variables and APOE-ε4. Additionally, to our knowledge, no prior studies have evaluated interactions between CR proxies and APOE-ε2 in relationship to longitudinal cognitive decline, although this is an important question given prior findings suggesting greater protective effects of CR on risk of MCI symptom onset among APOE-ε2 carriers relative to APOE-ε2 noncarriers [29].
To our knowledge, only one prior study has examined whether CR proxy measures modify the impact of an AD-PRS on cognitive decline (for cross-sectional studies [30, 31]). In this study among older adults across the clinical spectrum, Shin et al. [32] found that one of several measures of cognitive activity engagement—reading books—attenuated the negative effect of an AD-PRS that included APOE on cognitive decline.
The present study addresses several issues that remain unresolved by prior literature. First, no prior studies have simultaneously examined whether CR proxy measures differentially interact with APOE-ε4 genetic status, APOE-ε2 genetic status, and AD-PRS in relationship to longitudinal cognitive trajectories. Second, few prior studies have examined these questions in individuals with normal cognition at baseline, yet this is important for identifying effective strategies for preventing or delaying future cognitive impairment. Third, most prior studies on this topic have used education as a proxy for CR. However, measures of literacy, either alone or in combination with other variables, may be more sensitive proxies for CR, given years of education does not reflect educational quality and remains largely stable after early adulthood [33]. Lastly, prior studies have often used measures of global cognition or individual test scores to measure longitudinal change. It is therefore unclear whether interactions between CR and genetic factors differ by cognitive domain. To address these gaps, this study examined whether a CR index score, combining both years of education and literacy test scores, modifies the relationship between AD genetic risk factors and longitudinal cognitive trajectories in a large sample of participants who were cognitively normal at baseline (N = 1819). We included both APOE-ε4 and APOE-ε2 genetic status and evaluated two versions of the AD-PRS—one without the APOE region and another with the APOE region. We also measured longitudinal cognitive performance with factor scores for global cognition, episodic memory, and executive function, to systematically explore the possibility of domain-specific effects.
Methods
Participants
Data for these analyses were derived from the Preclinical AD Consortium (PAC), which established large, harmonized datasets to examine questions of importance to the preclinical phase of AD that might be challenging to address with smaller sample sizes. The PAC datafiles combine data from 5 ongoing cohort studies examining the earliest phases of AD, including the Adult Children Study (ACS) [34], the Australian Imaging, Biomarker, and Lifestyle (AIBL) study [35], the Neuroimaging Substudy of the Baltimore Longitudinal Study of Aging (BLSA) [36], the Biomarkers of Cognitive Decline Among Normal Individuals (BIOCARD) study [37], and the Wisconsin Registry for Alzheimer’s Prevention (WRAP) [38]. Details about each cohort’s study design and exclusionary criteria have been described previously [35,36,37,38,39]. To be included in the PAC datafiles, each participant had to be cognitively normal at baseline and have at least one molecular biomarker (derived from cerebrospinal fluid (CSF) or positron emission tomography (PET)) collected while they were cognitively normal. The first visit at which a participant was cognitively normal and had a molecular biomarker collected was defined as the “PAC Baseline.” Molecular biomarkers were not considered in the present analyses.
Participants in all cohorts undergo longitudinal clinical and cognitive examinations, as well as medical, neurologic and psychiatric assessments and consensus diagnoses based on published criteria, e.g., the National Institute on Aging/Alzheimer’s Association criteria for MCI [40] and dementia [41]. Clinical and cognitive assessments are completed at regular intervals (e.g., every 12, 18, or 24 months) depending on each study’s design. Longitudinal neuroimaging (i.e., magnetic resonance imaging (MRI) and PET) and CSF are also collected at regular intervals (e.g., 24 months or 36 months). Clinical diagnoses were made without knowledge of biomarker measures. All participants provided written informed consent, and study protocols were approved by each site’s local institutional review board.
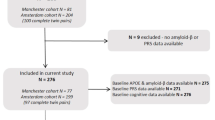
These analyses included participants who were cognitively normal at their first cognitive assessment and had both APOE genotypes and proxies for CR (i.e., years of education and scores on literacy tests: N = 1819; participants in AD-PRS analyses: N = 1175). For the purpose of this manuscript, “baseline” was defined as a participant’s first available cognitive test score (some of the sites provided data preceding the participant’s “PAC Baseline”; therefore, the first visit for a subset of participants in these analyses occurred before an individual’s “PAC Baseline”).
Cognitive assessments
Comprehensive neuropsychological batteries administered to each cohort include standardized tests spanning the cognitive domains of episodic memory, executive function, language, visuospatial processing, attention, and processing speed. In order to combine raw cognitive data across all sites, longitudinal cognitive performance was measured with previously validated harmonized cognitive factor scores for (i) global cognition, including most available tests within a cohort; (ii) episodic memory, including verbal and visual episodic memory; and (iii) executive function, including tasks such as digit span, task switching, fluency, and set shifting (for details, see [42, 43]; see Supplementary Table 1, Additional File 1 for a list of tests included in each factor score).
The cognitive factor scores were generated from the raw cognitive data using item response theory (IRT) implemented in Mplus and followed an item banking approach [44]. This method allows for tests that are common to all cohorts, as well as tests unique to one or a few cohorts, to be combined into domain-specific factor scores for each participant at each visit, thereby utilizing all available data. Briefly, generation of factor scores entailed pre-statistical harmonization to identify unique and common items across datasets [45]; statistical co-calibration using confirmatory factor analysis (CFA) models separately for each study, for each cognitive domain; and examination of model fit and the quality of the link between each study, using simulation and testing for differential item functioning by study [46]. Following pre-statistical harmonization, an item banking approach [44] was used to serially estimate graded-IRT models separately within each dataset [47]. In each model, parameters (e.g., loadings and thresholds or intercepts) of new items were retained in the item bank for use in the subsequent models. In a final standardization step, all participants were pooled to estimate a CFA in which all item parameters were fixed to their previously estimated values, resulting in factor scores for each domain, integrated across the cohorts. To facilitate comparisons across factor scores, the harmonized values were z-scored based on each participant’s “PAC Baseline.”
Cognitive reserve proxy index score
A harmonized CR index score was calculated by z-scoring and then averaging years of education and first available literacy test scores, consistent with a previously published method [48]. Literacy test scores reflected measures of verbal ability and reading, as often used in estimating crystallized intelligence. The literacy test scores were z-scored within cohort, given different assessments were administered across cohorts (ACS: Slosson Oral Reading Test [49]; AIBL: Wechsler Test of Adult Reading [50]; BIOCARD: National Adult Reading Test [51]; BLSA and WRAP: Wide Range Achievement Test 3 Letter and Word Reading [52]). The years of education variable was z-scored separately for cohorts within vs. outside the USA, given differences in educational systems.
Genetic measures
DNA was extracted from whole blood in each study. GWAS data were generated from various genotyping arrays across studies with APOE genotyping performed separately using a targeted genotyping approach (see Supplementary Table 2, Additional File 1). APOE genetic status, provided by each site, was coded with separate dichotomous indicator variables for APOE-ε2 (ε2/ε2 and ε2/3 = 1; otherwise 0), APOE-ε3 (ε3/ε3 = 1, otherwise 0), and APOE-ε4 (ε2/ε4, ε3/ε4 and ε4/ε4 = 1; otherwise 0). Individuals with ε2/ε4 alleles were included in the APOE-ε4 group given their risk for AD pathology is similar to that of ε4 carriers, rather than ε2 carriers [53].
Raw GWAS data from each site were imputed by chip using a standard pipeline that included variant filtering for genotyping efficiency (95%), minor allele frequency (> 1%), and Hardy-Weinberg equilibrium (p > 1 × 10−6). Samples were removed for low call rate (< 99%) or for a mismatch between reported and genetically confirmed sex. Given the racial and ethnic makeup of the included studies, all GWAS analyses were also restricted to those of European ancestry that was confirmed using population principal component (PC) analysis. Individuals who did not self-report as non-Hispanic White or were more than 5 SDs away from the 1000 Genomes EU reference population based on PC analysis were removed. Imputation was performed on the TOPMed Imputation Server (version 1.6.0, https://imputation.biodatacatalyst.nhlbi.nih), and variants were filtered post-imputation to include common (> 1%) biallelic single nucleotide polymorphisms (SNPs) with a high imputation quality (R 2 > 0.8) and within expected Hardy-Weinberg Equilibrium (p > 1 × 10−6). Importantly, for the purpose of the AD-PRS analysis, we restricted all GWAS datasets to overlapping variants leaving a total of 6,739,456 common variants available in all five datasets for analysis.
AD-PRS were generated using imputed GWAS data, leveraging the summary statistics provided by Kunkle et al. [6] that were regenerated for us removing PAC participants who were included in the original GWAS analysis (n = 93,220). Original summary statistics are available at https://www.niagads.org/. Prior to generating the AD-PRS, linkage disequilibrium (LD) clumping was performed in PLINK (version 1.9; [54]) using a significance threshold for index SNPs of p = 0.01, LD clumping threshold of 0.5, and a window width of 200 kb. This threshold was based on a previous publication applying and evaluating multiple thresholds when generating an AD-PRS [12]. In order to generate scores on the same scale, variants were restricted to those common across all five datasets as outlined above. Following clumping and pruning performed in the largest genomic dataset (ACS), weights from 13,172 variants available in all datasets were used for the AD-PRS calculation and 12,948 variants available in all datasets were used for AD-PRS without the APOE region. AD-PRS generation was performed with PLINK using the method published previously [12], and scores were generated with and without the APOE region (i.e., 1 MB upstream and downstream of the APOE gene). For ease of reporting, the AD-PRS with and without APOE are abbreviated AD-PRSAPOE and AD-PRSw/oAPOE, respectively.
The two AD-PRS were transformed into z-scores to simplify interpretation, using the mean and standard deviation across all five datasets. To examine the impact of relatedness on the outcomes, two sets of AD-PRS were generated: one with all participants included in the measure and the other with related individuals excluded.
Availability of data and materials
The plan is to archive the PAC datafiles at the National Archive of Computerized Data on Aging (NACDA). Investigators interested in accessing the data should contact the PAC Coordinating Center at Johns Hopkins University for details.
Statistical analyses
Pearson correlations were used to evaluate the relationship between years of education and literacy test scores, separately for each cohort. Linear regressions were used to examine the relationship between AD genetic risk factors and the CR index score.
Linear mixed-effects models including random intercepts and slopes were used to examine the relationship of AD genetic risk factors and CR index score to cognitive trajectories, with separate models run for each cognitive factor score as the outcome. All models included the following predictors: baseline age, sex, terms for genetic status (i.e., APOE or AD-PRS), the CR index score, indicators for site (to control for site differences), time, and the interaction (i.e., cross-product) of each predictor with time, including time2 for evaluating non-linear (quadratic) trajectories. To examine whether the CR index score modifies the relationship between AD genetic risk and longitudinal cognitive trajectories, the models also included the 2-way CR index score × genetic status and 3-way CR index score × genetic status × time interactions. If the 3-way interaction was not significant, reduced models excluding this term were estimated. Baseline age and the CR index score were standardized (i.e., z-scored) across all cohorts before model fitting, and time was modeled in the unit of years (since baseline). All available follow-up was included.
Two sets of models were run. In the first set, “genetic status” reflected APOE genotype, as measured by indicators for APOE-ε4 and APOE-ε2 (with APOE-ε3 as the reference group). In the second set, “genetic status” reflected the AD-PRS; these models were first run for AD-PRSw/oAPOE then for AD-PRSAPOE. Two sets of sensitivity analyses were run on the primary models. The first evaluated the relationship of the CR index score and AD genetic risk to longitudinal cognitive trajectories when individuals who progressed from normal cognition to MCI or dementia were excluded from the analyses. The second evaluated whether years of education and literacy scores made unique contributions to cognitive performance. Two additional sets of sensitivity analyses were run for the AD-PRS. The first evaluated whether the pattern of results remained unchanged when the n = 64 related individuals were excluded from the models, and within this subgroup, whether the patterns of results remained unchanged when the first five population PCs were included as covariates (for ensuring results were not driven by any unmeasured population stratification due to genetic ancestry). The second evaluated whether the relationship between the AD-PRSw/oAPOE and cognitive trajectories remained the same when terms for APOE-ε4 genetic status (i.e., APOE-ε4 and APOE-ε4 × time) were included as additional model predictors.
Effect sizes were calculated from a Cohen’s d derived from the linear mixed-effects models. To standardize each independent variable’s effect on the level or change in the cognitive outcome, effect sizes were calculated based on the standard deviation (SD) for the random intercept or SD for the random slope, respectively. SDs for random effects came from a reduced linear mixed-effects model that included only intercept and time as fixed effects and random effects.
Estimates (95% confidence intervals), p-values (with a significance level of p < 0.05), and effect sizes are reported. The mixed-effects models were run using the “lmer” function from “lmerTest” package in R (version 3.6.3) and Stata (version 17.0).
Results
Baseline characteristics of participants included in the analyses are shown in Table 1, for the APOE and AD-PRS analyses (for baseline characteristics by cohort, see Supplementary Tables 3 and 4, Additional File 1). On average, participants were late middle-aged at baseline, highly educated, approximately one-third APOE-ε4 carriers, and have undergone approximately 10 years of follow-up (maximum = 28.8 years). In each cohort, years of education was moderately correlated with literacy test scores (all r > 0.26, all p < 0.001). As shown in Fig. 1, the distributions of the harmonized AD-PRS from the five cohorts were on the same scale and aligned across datasets. While the scores were harmonized with identical weights and variants used across cohorts, we did note a difference in the observed AD-PRS across datasets (F(4, 1379) = 5.88, p < 0.001) with ACS and WRAP presenting with a slightly lower AD-PRS than the other cohorts. This difference was observed for the score with and without APOE (p < 0.01). As expected, there were no direct associations between the AD genetic risk factors (i.e., APOE-ε4, APOE-ε2, AD-PRSw/oAPOE, or AD-PRSAPOE) and the CR index score (all p > 0.34).

Distribution of harmonized AD-PRS in the PAC cohorts. Distributions shown for AD-PRSAPOE (top) and AD-PRSw/oAPOE (bottom) in each of the PAC cohorts. The dashed vertical lines indicate the mean for each cohort. Note that the dashed lines for ACS and WRAP slightly overlap (top), as do the dashed lines for AIBL and BIOCARD (bottom)
CR index score, APOE genotypes, and cognitive change
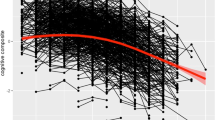
Results for the APOE analyses are shown in Table 2. Higher CR index scores were associated with better baseline cognitive performance for all cognitive factor scores (all p < 0.001), but not with rate of change in cognition over time. APOE-ε4 genotype was associated with greater rates of cognitive decline in all cognitive factor scores over time (all p < 0.001), whereas APOE-ε2 genotype was not associated with cognitive performance (see Supplementary Figure 1, Additional File 1 for spaghetti plots of participant trajectories by AD genetic risk profiles).
There were significant interactions between the CR index score and APOE-ε4 genetic status. For the global factor score, there was a significant CR index × APOE-ε4 interaction (p = 0.03), indicating that APOE-ε4 carriers with higher CR index scores had lower baseline cognitive performance, relative to APOE-ε3. Of primary interest, there were significant 3-way CR index score × APOE-ε4 × time interactions (both p ≤ 0.04) for the global and memory scores: model coefficients indicate that the negative effect of APOE-ε4 genotype on global and memory score decline was attenuated among individuals with higher CR index scores (Fig. 2).

Estimates of longitudinal cognitive change based on APOE genetic status and level of cognitive reserve. Estimated cognitive change (95% CI) shown for APOE genetic status (APOE-ε2, APOE-ε3, APOE-ε4) and high vs. low CR index scores, represented by the 25th and 75th percentiles for illustration purposes. Sample means were used in the estimation of all other covariates. Cognitive change is shown separately for global (top), memory (middle), and executive function (bottom) factor scores based on the full models, as shown in Table 2. The CR index × APOE-ε4 × time interactions were significant for the global and memory factor scores, but not for the executive function factor score
Across all models, there were significant main effects of age and sex, and age × time interactions (all p < 0.001) for all cognitive factor scores: baseline cognitive performance was lower among older participants and men, and older participants had greater rates of cognitive decline. There were also significant sex × time interactions (all p ≤ 0.04) for the executive function factor score only, indicating greater rates of decline among men compared to women.
CR index score, AD-PRS and cognitive change
Results for the AD-PRSw/oAPOE analyses are shown in Table 3. As above, higher CR index scores were associated with better baseline cognitive performance for all cognitive factor scores (all p < 0.001). Higher CR index scores were also associated with more positive rates of change in memory factor scores (p = 0.02). Higher AD-PRSw/oAPOE were associated with greater rates of decline in the global and executive function factor scores (all p ≤ 0.03), but not with memory decline (p = 0.21). However, there were no significant 3-way CR index × AD-PRSw/oAPOE × time interactions (all p > 0.23), indicating that level of CR did not attenuate the effect of the AD-PRSw/oAPOE on cognitive decline (Fig. 3). The results for AD-PRSAPOE were similar, except that the AD-PRSAPOE was associated with declines in all three cognitive factor scores (all p ≤ 0.02; Supplementary Table 5, Additional File 1). These results were essentially unchanged when cluster bootstrapping was applied (data not shown).

Estimates of longitudinal cognitive change based on AD-PRSw/oAPOE and level of cognitive reserve. Estimated cognitive change (95% CI) shown for high vs. low AD-PRSw/oAPOE and high vs. low CR index scores, represented by the 25th and 75th percentiles for illustration purposes. Sample means were used in the estimation of all other covariates. Cognitive change is shown separately for global (top), memory (middle), and executive function (bottom) factor scores based on the full models, as shown in Table 3. The AD-PRSw/oAPOE × time interactions were significant for the global and executive function factor scores, but not for the memory factor score
Sensitivity analyses
When participants who progressed from normal cognition to MCI or dementia were excluded from the models (see Supplementary Table 6, Additional File 1), the patterns of results were similar to those described above, with a few exceptions. In the APOE models (excluding n = 230 progressors), APOE-ε4 genotype was associated with greater rates decline in the memory factor score (p = 0.02), but only marginally with declines in the global and executive function factor scores (both p < 0.08). There were no interactions between the CR index score and APOE-ε4 genetic status. However, the 3-way CR index score × APOE-ε4 × time interactions remained significant for the global and memory factor scores (both p ≤ 0.04), again indicating attenuated APOE-ε4-related global and memory score declines among individuals with higher CR index scores. In the AD-PRSw/oAPOE models (excluding n = 178 progressors), there was no CR index score × time interaction for the memory factor score. Higher AD-PRSw/oAPOE were associated with greater rates of decline only in the executive function factor score (p = 0.04) and not with declines in the global or memory factor scores (both p > 0.21). As above, there were no significant 3-way CR index × AD-PRSw/oAPOE × time interactions (all p > 0.76). In the second set of sensitivity analyses, z-scored years of education and z-scored literacy scores were each significantly associated with better cognitive performance on all three factor scores, but only the years of education variable (not literacy test scores) attenuated APOE-ε4-related declines in the global and memory factor scores (Supplementary Table 7, Additional File 1).
All patterns of AD-PRS results were unchanged when n = 64 related individuals were excluded from the analyses and when covarying for population PCs (Supplementary Tables 8 and 9, Additional File 1). Additionally, the AD-PRSw/oAPOE remained significantly associated with greater rates of decline in the global and executive function factor scores when terms for APOE-ε4 genetic status were included as additional predictors (both p ≤ 0.03), whereas APOE-ε4 genetic status was independently associated with greater rates of cognitive decline in all cognitive factor scores (all p ≤ 0.005; see Table 4).
Discussion
This study examined the association between a CR index score and AD genetic risk factors in relationship to cognitive change among participants with normal cognition at baseline. There are several notable findings. First, higher CR index scores were consistently associated with better cognitive performance, whereas those at greater genetic risk for AD (based on either APOE genetic status or AD-PRS) demonstrated greater rates of cognitive decline, including among individuals who have remained cognitively normal over the course of follow-up. Second, higher levels of CR attenuated APOE-ε4-related declines in global cognition and memory. However, levels of CR did not attenuate APOE-ε4-related declines in executive function or AD-PRS-related cognitive decline. Of note, while APOE-ε4 genetic status and AD-PRSAPOE were associated with declines in all cognitive domains examined here, AD-PRSw/oAPOE was significantly associated with declines in executive function and global cognition but not episodic memory. Finally, APOE-ε2 genetic status was unrelated to cognitive performance. These results suggest that AD genetic risk factors differentially impact cognitive trajectories among individuals with normal cognition at baseline. However, the impact of APOE-ε4, in particular, may be mitigated by lifestyle factors (such as CR) that are potentially modifiable.
Interactions between level of CR and AD genetic risk
To our knowledge, no prior studies have evaluated interactions between CR proxy measures and both APOE-ε4 and AD-PRS in the same group of participants. Our results suggest that higher levels of CR differentially mitigate APOE-ε4-related vs. AD-PRS-related cognitive decline, with the protective effect of CR being specific to APOE-ε4-related declines in episodic memory (but not executive function). This may suggest that higher levels of CR (e.g., education, literacy) reduce the impact of APOE-ε4 on rates of change in episodic memory among older individuals. Given that middle-aged and older APOE-ε4 carriers, on average, have more AD-related pathology than non-carriers due to an earlier onset of amyloid accumulation [55, 56], these results suggest that individuals with higher levels of CR may be better able to tolerate early AD-related brain changes. For example, individuals with higher levels of CR may have greater brain reserve (such as greater volume, cortical thickness, or microstructural integrity [57]) or more effectively utilize alternative behavioral strategies to compensate for declining memory processes [58, 59]. The mechanisms by which this occurs, however, remain unclear and future studies are needed to determine whether CR is protective against early AD vs. non-AD processes [60,61,62], especially given that level of CR also attenuated APOE-ε4-related memory declines in the subset of individuals who have remained cognitively normal over time. Of note, the effect sizes for these interactions were small (d = 0.16 and d = 0.22 for global cognition and memory, respectively), suggesting that the degree to which CR modifies APOE-ε4-associated declines is modest.
Only three prior studies have examined interactions between CR proxy measures and APOE-ε4 genotype in relationship to longitudinal cognitive decline among individuals with normal cognition at baseline. Our results are consistent with those of Mayeux et al. [26], which reported greater APOE-ε4-related decline in an episodic memory factor score among individuals with lower levels of education, with similar effects not found for language and visuospatial/reasoning factor scores (total sample size = 563). However, other studies have reported different outcomes [27, 28]. For example, using data from WRAP, Koscik et al. [27] found only limited evidence of a relationship between APOE-ε4 and decline on individual cognitive tests among cognitively normal middle-aged participants, and this relationship was not modified by literacy scores (total sample size = 1256). Discrepancies between studies may reflect differences in cohort age and the sensitivity of the cognitive tests used (e.g., individual tests vs. cognitive composite scores), or the fact that these interactions have small effect sizes that are difficult to detect in smaller samples.
In contrast to the APOE-ε4 results, AD-PRS-related cognitive decline was not attenuated by level of CR. The one prior longitudinal study that has examined interactions between CR proxy measures and an AD-PRS on cognitive decline found only limited evidence for an interaction, as only one of eight CR proxy measures examined (reading books) was associated with reduced AD-PRSAPOE-related cognitive decline [32]. The results of that study, however, are difficult to compare to our own because participants were of mixed clinical diagnoses at baseline (i.e., not restricted to individuals with normal cognition). Because AD-PRS reflect many genetic loci with heterogenous impacts on multiple molecular and neuropathological pathways [6, 63], it may be that levels of CR have effects on a subset of AD-PRS mechanistic pathways, but not others. Additional studies are needed to further examine these questions.
AD genetic risk and cognitive decline
The AD-PRSw/oAPOE was associated with global and executive function decline, but not episodic memory decline. This association was statistically significant when APOE-ε4 genetic status was included as an additional model covariate. Additionally, in this latter set of models, APOE-ε4 was independently associated with cognitive decline in all cognitive domains examined, and with larger effect sizes than the AD-PRSw/oAPOE (see Table 4). This suggests that there may be different biological pathways that mediate AD-related cognitive decline across different cognitive domains, with some pathways having a greater impact on decline than others during the preclinical phase of AD. This likely reflects the fact that individuals at greater genetic risk (i.e., APOE-ε4 carriers; higher AD-PRS scores) have more AD pathology (e.g., [11, 64,65,66]) which at least partially underlies the relationship between these genetic risk factors and cognitive decline [63, 67, 68].
While a number of prior studies have reported greater rates of cognitive decline among cognitively normal APOE-ε4 carriers (for a review, see [60]), studies examining the relationship of AD-PRS with cognitive decline have been more limited. Analyses among non-demented and mixed diagnosis samples have reported relationships between AD-PRSw/oAPOE and both executive function and episodic memory declines [12, 67, 69], whereas studies among individuals with normal cognition have been more mixed. Consistent with our results, Tan et al. [14] found significant associations between an AD-PRSw/oAPOE and scores on several individual tests, including two attention/executive function tasks among cognitively normal individuals with AD pathology at autopsy. Additionally, a study among cognitively normal participants from AIBL found no association between an AD-PRSw/oAPOE and decline on composite scores composed largely of episodic memory tasks, although an executive function composite was not examined (Porter et al., [66]). However, Gustavson et al. [70] found only limited evidence of an association between AD-PRSw/oAPOE and cognitive decline among middle-aged cognitively normal individuals, as only one AD-PRSw/oAPOE of several examined was associated with declines in episodic memory, and none of the PRS were associated with declines in an executive function factor score. While reasons for this mixed literature are not yet clear, these findings suggest that non-APOE AD risk genes have very subtle effects on cognitive change among individuals with normal cognition. This mixed literature may also be influenced by differences in methods used for PRS calculation, including the specific loci included. Additional studies are needed to further examine this question, and the possibility of domain-specific cognitive effects.
As noted above, greater genetic risk for AD was also associated with greater rates of cognitive decline among individuals who have remained cognitively normal over the course of follow-up. Specifically, APOE-ε4 genetic status was significantly associated with declines in the episodic memory factor score, whereas the AD-PRSw/oAPOE was associated with declines in the executive function factor score. This may suggest that AD genetic risk makes notable contributions to age-related declines in these domains, though future studies are needed to evaluate how these results change when accounting for individual differences in biomarkers of AD pathology.
Level of CR and cognitive decline
In line with prior work, higher CR index scores were consistently associated with better overall cognitive performance, with less evidence of an association with change in cognition over time. This suggests that cognitive reserve confers protective effects largely by impacting level of cognitive performance across all levels of AD genetic risk (which may delay the age at which individuals reach clinically significant cognitive impairment), rather than reducing rates of cognitive decline ([71]; see also [25]). Identifying the neurobiological mechanisms of CR, and the ways by which these mechanisms modify age- and disease-related brain changes, is an important research priority.
APOE-ε2 and cognitive decline
Lastly, although the APOE-ε2 genotype is associated with reduced risk of AD dementia [8, 9], we did not find a relationship between APOE-ε2 genotype and cognitive trajectories in this sample of middle-aged and older cognitively normal individuals, either alone or in interaction with level of CR. To our knowledge, no prior studies have examined the interactions between APOE-ε2 genotype and level of CR in relationship to longitudinal cognitive trajectories. Our results differ from a prior report from the BIOCARD study, which found that higher levels of CR were more protective in APOE-ε2 carriers vs. non-carriers with respect to time to progression from normal cognition to MCI clinical symptom onset [29]. Reasons for these differing results are unclear but may be related to the outcome used (i.e., rate of change in cognition vs. time to onset of clinical symptoms). Furthermore, although prior studies have reported reduced rates of cognitive decline among APOE-ε2 carriers, findings have been mixed, particularly in younger samples (for reviews, see [10, 72]). This suggests that the direct effects of APOE-ε2 genotype on cognitive trajectories are more evident in older populations, among whom cognitive decline is more prevalent.
Limitations
This study has limitations. First, participants were primarily White, well-educated, and several cohorts were enriched for a family history of dementia due to AD. Although the family history might be beneficial for examining the relationship between AD genetic risk factors and cognitive decline, it limits the generalizability of the findings to broader populations. Additionally, there were differences in characteristics between cohorts, including baseline age and level of AD genetic risk. While this in part reflects differences in cohort design (e.g., target age range; enrichment for family history of AD dementia), we cannot rule out the possibility of survival effects in the oldest participants, given APOE-ε4 and AD-PRS effects and frequencies may vary with age (e.g., [8, 73,74,75]). Future studies are needed to evaluate whether the reported results differ between middle-aged and older adults, as well as by sex. Second, the AD-PRS models included fewer participants, and only 226/1819 participants (12%) were APOE-ε2 carriers. We therefore cannot rule out the possibility that we were underpowered to detect 3-way interactions or relationships between APOE-ε2 and cognition, despite the fact that the frequency of APOE-ε2 carriers may be slightly higher than worldwide frequency estimates [76, 77]. Similarly, we cannot rule out the possibility that some of the effects reported here are false positives. For example, we used a p < .05 significance level for all analyses to examine complex inter-relationships between these variables and because few prior studies have examined these research questions among individuals with normal cognition. However, some of the interactions had modest levels of statistical significance and small effect sizes. Third, there are limitations related to the CR index score used in this study. The CR index score was composed of variables that are closely related to general intelligence, which may at least partly underlie associations with cognitive performance. These variables are likely also closely related to other factors, such as occupational complexity, socioeconomic status, and lifetime opportunities. Additional longitudinal studies are needed to replicate these findings in more diverse cohorts with a broader range of educational attainment, using other measures of CR (such as occupational complexity and engagement in cognitively stimulating activities), and while accounting for biomarkers of age- and disease-related brain changes.
Conclusions
These findings suggest that higher levels of cognitive reserve attenuate APOE-ε4-related declines in global cognition and memory, but not APOE-ε4-related declines in executive function, or AD PRS-related cognitive decline. This raises the possibility that interventions targeting intellectual activities may disproportionately benefit APOE-ε4 carriers and supports recent recommendations on the importance of prioritizing early-life education and maintaining a cognitively active lifestyle in mid-life and later [2].
Availability of data and materials
The plan is to archive the PAC datafiles at the National Archive of Computerized Data on Aging (NACDA). Investigators interested in accessing the data should contact the PAC Coordinating Center at Johns Hopkins University for details.
Abbreviations
- ACS:
-
Adult Children Study
- AIBL:
-
Australian Imaging, Biomarker, and Lifestyle
- AD:
-
Alzheimer’s disease
- AD-PRS:
-
Alzheimer’s disease polygenic risk scores
- APOE :
-
Apolipoprotein-E (gene)
- BIOCARD:
-
Biomarkers of Cognitive Decline Among Normal Individuals
- BLSA:
-
Baltimore Longitudinal Study of Aging
- CFA:
-
Confirmatory factor analysis
- CI:
-
Confidence interval
- CR:
-
Cognitive reserve
- CSF:
-
Cerebrospinal fluid
- IRT:
-
Item response theory
- MCI:
-
Mild cognitive impairment
- MRI:
-
Magnetic resonance imaging
- NHW:
-
Non-Hispanic white
- PAC:
-
Preclinical AD Consortium
- PC:
-
Principal component
- PET:
-
Positron emission tomography
- SD:
-
Standard deviation
- WRAP:
-
Wisconsin Registry for Alzheimer’s Prevention
References
Collaborators GBDDF. Estimation of the global prevalence of dementia in 2019 and forecasted prevalence in 2050: an analysis for the Global Burden of Disease Study 2019. Lancet Public Health. 2022;7(2):e105–25.
Livingston G, Huntley J, Sommerlad A, Ames D, Ballard C, Banerjee S, et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet. 2020;396(10248):413–46.
Nelson ME, Jester DJ, Petkus AJ, Andel R. Cognitive reserve, Alzheimer’s neuropathology, and risk of dementia: a systematic review and meta-analysis. Neuropsychol Rev. 2021;31(2):233–50.
Soldan A, Pettigrew C, Albert M. Cognitive reserve from the perspective of preclinical Alzheimer disease: 2020 update. Clin Geriatr Med. 2020;36(2):247–63.
Collaboratory RR. Collaboratory on Research Definitions for Reserve and Resilience in Cognitive Aging and Dementia. 2022. Available from: http://reserveandresilience.com .
Kunkle BW, Grenier-Boley B, Sims R, Bis JC, Damotte V, Naj AC, et al. Genetic meta-analysis of diagnosed Alzheimer’s disease identifies new risk loci and implicates Abeta, tau, immunity and lipid processing. Nat Genet. 2019;51(3):414–30.
Corder EH, Saunders AM, Strittmatter WJ, Schmechel DE, Gaskell PC, Small GW, et al. Gene dose of apolipoprotein E type 4 allele and the risk of Alzheimer’s disease in late onset families. Science. 1993;261(5123):921–3.
Farrer LA, Cupples LA, Haines JL, Hyman B, Kukull WA, Mayeux R, et al. Effects of age, sex, and ethnicity on the association between apolipoprotein E genotype and Alzheimer disease. A meta-analysis. APOE and Alzheimer Disease Meta Analysis Consortium. JAMA. 1997;278(16):1349–56.
Corder EH, Saunders AM, Risch NJ, Strittmatter WJ, Schmechel DE, Gaskell PC Jr, et al. Protective effect of apolipoprotein E type 2 allele for late onset Alzheimer disease. Nat Genet. 1994;7(2):180–4.
Suri S, Heise V, Trachtenberg AJ, Mackay CE. The forgotten APOE allele: a review of the evidence and suggested mechanisms for the protective effect of APOE varepsilon2. Neurosci Biobehav Rev. 2013;37(10 Pt 2):2878–86.
Desikan RS, Fan CC, Wang Y, Schork AJ, Cabral HJ, Cupples LA, et al. Genetic assessment of age-associated Alzheimer disease risk: development and validation of a polygenic hazard score. PLoS Med. 2017;14(3): e1002258.
Mormino EC, Sperling RA, Holmes AJ, Buckner RL, De Jager PL, Smoller JW, et al. Polygenic risk of Alzheimer disease is associated with early- and late-life processes. Neurology. 2016;87(5):481–8.
Riaz M, Huq A, Ryan J, Orchard SG, Tiller J, Lockery J, et al. Effect of APOE and a polygenic risk score on incident dementia and cognitive decline in a healthy older population. Aging Cell. 2021;20(6): e13384.
Tan CH, Hyman BT, Tan JJX, Hess CP, Dillon WP, Schellenberg GD, et al. Polygenic hazard scores in preclinical Alzheimer disease. Ann Neurol. 2017;82(3):484–8.
Cook CJ, Fletcher JM. Can education rescue genetic liability for cognitive decline? Soc Sci Med. 2015;127:159–70.
Kaup AR, Nettiksimmons J, Harris TB, Sink KM, Satterfield S, Metti AL, et al. Cognitive resilience to apolipoprotein E epsilon4: contributing factors in black and white older adults. JAMA Neurol. 2015;72(3):340–8.
Makkar SR, Lipnicki DM, Crawford JD, Kochan NA, Castro-Costa E, Lima-Costa MF, et al. Education and the moderating roles of age, sex, ethnicity and apolipoprotein epsilon 4 on the risk of cognitive impairment. Arch Gerontol Geriatr. 2020;91: 104112.
Niti M, Yap KB, Kua EH, Tan CH, Ng TP. Physical, social and productive leisure activities, cognitive decline and interaction with APOE-epsilon 4 genotype in Chinese older adults. Int Psychogeriatr. 2008;20(2):237–51.
Shadlen MF, Larson EB, Wang L, Phelan EA, McCormick WC, Jolley L, et al. Education modifies the effect of apolipoprotein epsilon 4 on cognitive decline. Neurobiol Aging. 2005;26(1):17–24.
Zhang Y, Fu S, Ding D, Lutz MW, Zeng Y, Yao Y. Leisure activities, APOE epsilon4, and cognitive decline: a longitudinal cohort study. Front Aging Neurosci. 2021;13: 736201.
Kalmijn S, Feskens EJ, Launer LJ, Kromhout D. Longitudinal study of the effect of apolipoprotein e4 allele on the association between education and cognitive decline in elderly men. BMJ. 1997;314(7073):34–5.
Runge SK, Small BJ, McFall GP, Dixon RA. APOE moderates the association between lifestyle activities and cognitive performance: evidence of genetic plasticity in aging. J Int Neuropsychol Soc. 2014;20(5):478–86.
Seeman TE, Huang MH, Bretsky P, Crimmins E, Launer L, Guralnik JM. Education and APOE-e4 in longitudinal cognitive decline: MacArthur Studies of Successful Aging. J Gerontol B Psychol Sci Soc Sci. 2005;60(2):P74-83.
Van Gerven PW, Van Boxtel MP, Ausems EE, Bekers O, Jolles J. Do apolipoprotein E genotype and educational attainment predict the rate of cognitive decline in normal aging? A 12-year follow-up of the Maastricht Aging Study. Neuropsychology. 2012;26(4):459–72.
Vemuri P, Lesnick TG, Przybelski SA, Machulda M, Knopman DS, Mielke MM, et al. Association of lifetime intellectual enrichment with cognitive decline in the older population. JAMA Neurol. 2014;71(8):1017–24.
Mayeux R, Small SA, Tang M, Tycko B, Stern Y. Memory performance in healthy elderly without Alzheimer’s disease: effects of time and apolipoprotein-E. Neurobiol Aging. 2001;22(4):683–9.
Koscik RL, Norton DL, Allison SL, Jonaitis EM, Clark LR, Mueller KD, et al. Characterizing the effects of sex, APOE varepsilon4, and literacy on mid-life cognitive trajectories: application of information-theoretic model averaging and multi-model inference techniques to the Wisconsin Registry for Alzheimer’s Prevention study. J Int Neuropsychol Soc. 2019;25(2):119–33.
Woodard JL, Sugarman MA, Nielson KA, Smith JC, Seidenberg M, Durgerian S, et al. Lifestyle and genetic contributions to cognitive decline and hippocampal structure and function in healthy aging. Curr Alzheimer Res. 2012;9(4):436–46.
Pettigrew C, Soldan A, Li S, Lu Y, Wang MC, Selnes OA, et al. Relationship of cognitive reserve and APOE status to the emergence of clinical symptoms in preclinical Alzheimer’s disease. Cogn Neurosci. 2013;4(3–4):136–42.
Fletcher J, Topping M, Zheng F, Lu Q. The effects of education on cognition in older age: evidence from genotyped Siblings. Soc Sci Med. 2021;280: 114044.
Frank M, Hensel J, Baak L, Schramm S, Dragano N, Weimar C, et al. Interaction of Alzheimer’s disease-associated genetic risk with indicators of socioeconomic position on mild cognitive impairment in the Heinz Nixdorf Recall study. J Alzheimers Dis. 2021;82(4):1715–25.
Shin SH, Park S, Wright C, D’Astous VA, Kim G. The role of polygenic score and cognitive activity in cognitive functioning among older adults. Gerontologist. 2021;61(3):319–29.
Manly JJ, Schupf N, Tang MX, Stern Y. Cognitive decline and literacy among ethnically diverse elders. J Geriatr Psychiatry Neurol. 2005;18(4):213–7.
Coats M, Morris JC. Antecedent biomarkers of Alzheimer’s disease: the adult children study. J Geriatr Psychiatry Neurol. 2005;18(4):242–4.
Ellis KA, Bush AI, Darby D, De Fazio D, Foster J, Hudson P, et al. The Australian Imaging, Biomarkers and Lifestyle (AIBL) study of aging: methodology and baseline characteristics of 1112 individuals recruited for a longitudinal study of Alzheimer’s disease. Int Psychogeriatr. 2009;21(4):672–87.
Resnick SM, Goldszal AF, Davatzikos C, Golski S, Kraut MA, Metter EJ, et al. One-year age changes in MRI brain volumes in older adults. Cereb Cortex. 2000;10(5):464–72.
Albert M, Soldan A, Gottesman R, McKhann G, Sacktor N, Farrington L, et al. Cognitive changes preceding clinical symptom onset of mild cognitive impairment and relationship to ApoE genotype. Curr Alzheimer Res. 2014;11(8):773–84.
Johnson SC, Koscik RL, Jonaitis EM, Clark LR, Mueller KD, Berman SE, et al. The Wisconsin Registry for Alzheimer’s Prevention: a review of findings and current directions. Alzheimers Dement (Amst). 2018;10:130–42.
Xiong C, Roe CM, Buckles V, Fagan A, Holtzman D, Balota D, et al. Role of family history for Alzheimer biomarker abnormalities in the adult children study. Arch Neurol. 2011;68(10):1313–9.
Albert MS, DeKosky ST, Dickson D, Dubois B, Feldman HH, Fox NC, et al. The diagnosis of mild cognitive impairment due to Alzheimer’s disease: recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011;7(3):270–9.
McKhann GM, Knopman DS, Chertkow H, Hyman BT, Jack CR Jr, Kawas CH, et al. The diagnosis of dementia due to Alzheimer’s disease: recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011;7(3):263–9.
Gross AL, Jones RN, Fong TG, Tommet D, Inouye SK. Calibration and validation of an innovative approach for estimating general cognitive performance. Neuroepidemiology. 2014;42(3):144–53.
Gross AL, Hassenstab JJ, Johnson SC, Clark LR, Resnick SM, Kitner-Triolo M, et al. A classification algorithm for predicting progression from normal cognition to mild cognitive impairment across five cohorts: the preclinical AD consortium. Alzheimers Dement (Amst). 2017;8:147–55.
Vonk JMJ, Gross AL, Zammit AR, Bertola L, Avila JF, Jutten RJ, et al. Cross-national harmonization of cognitive measures across HRS HCAP (USA) and LASI-DAD (India). PLoS One. 2022;17(2): e0264166.
Briceno EM, Gross AL, Giordani BJ, Manly JJ, Gottesman RF, Elkind MSV, et al. Pre-statistical considerations for harmonization of cognitive instruments: Harmonization of ARIC, CARDIA, CHS, FHS, MESA, and NOMAS. J Alzheimers Dis. 2021;83(4):1803–13.
Gross AL, Mungas DM, Crane PK, Gibbons LE, MacKay-Brandt A, Manly JJ, et al. Effects of education and race on cognitive decline: an integrative study of generalizability versus study-specific results. Psychol Aging. 2015;30(4):863–80.
Samejima F. Graded Response Model. In: van der Linden WJH R.K, editor. Handbook of Modern Item Response Theory. 1st ed. New York: Springer; 1997.
Soldan A, Pettigrew C, Li S, Wang MC, Moghekar A, Selnes OA, et al. Relationship of cognitive reserve and cerebrospinal fluid biomarkers to the emergence of clinical symptoms in preclinical Alzheimer’s disease. Neurobiol Aging. 2013;34(12):2827–34.
Richard LN C.L. Slosson Oral Reading Test-Revised. East Aurora: Slosson Education Publications, Inc; 1990.
Holdnack HA. Wechsler Test of Adult Reading: WTAR. San Antonio, TX: The Psychological Corporation; 2001.
Nelson HE. The National Adult Reading Test (NART): Test Manual. Windsor: Nfer-Nelson; 1982.
Wilkinson GS. Wide Range Achievement Test 3. Wilmington, DE: Wide Range, Inc.; 1993.
Goldberg TE, Huey ED, Devanand DP. Association of APOE e2 genotype with Alzheimer’s and non-Alzheimer’s neurodegenerative pathologies. Nat Commun. 2020;11(1):4727.
Chang CC, Chow CC, Tellier LC, Vattikuti S, Purcell SM, Lee JJ. Second-generation PLINK: rising to the challenge of larger and richer datasets. Gigascience. 2015;4:7.
Betthauser TJ, Bilgel M, Koscik RL, Jedynak BM, An Y, Kellett KA, et al. Multi-method investigation of factors influencing amyloid onset and impairment in three cohorts. Brain. 2022;145(11):4065-79.
Pletnikova O, Kageyama Y, Rudow G, LaClair KD, Albert M, Crain BJ, et al. The spectrum of preclinical Alzheimer’s disease pathology and its modulation by ApoE genotype. Neurobiol Aging. 2018;71:72–80.
Stern Y, Arenaza-Urquijo EM, Bartres-Faz D, Belleville S, Cantilon M, Chetelat G, et al. Whitepaper: Defining and investigating cognitive reserve, brain reserve, and brain maintenance. Alzheimers Dement. 2020;16(9):1305–11.
Barulli DJ, Rakitin BC, Lemaire P, Stern Y. The influence of cognitive reserve on strategy selection in normal aging. J Int Neuropsychol Soc. 2013;19(7):841–4.
Frankenmolen NL, Fasotti L, Kessels RPC, Oosterman JM. The influence of cognitive reserve and age on the use of memory strategies. Exp Aging Res. 2018;44(2):117–34.
O’Donoghue MC, Murphy SE, Zamboni G, Nobre AC, Mackay CE. APOE genotype and cognition in healthy individuals at risk of Alzheimer’s disease: a review. Cortex. 2018;104:103–23.
Saunders AM. Apolipoprotein E and Alzheimer disease: an update on genetic and functional analyses. J Neuropathol Exp Neurol. 2000;59(9):751–8.
Yamazaki Y, Zhao N, Caulfield TR, Liu CC, Bu G. Apolipoprotein E and Alzheimer disease: pathobiology and targeting strategies. Nat Rev Neurol. 2019;15(9):501–18.
Tasaki S, Gaiteri C, Mostafavi S, De Jager PL, Bennett DA. The molecular and neuropathological consequences of genetic risk for Alzheimer’s dementia. Front Neurosci. 2018;12:699.
Bilgel M, An Y, Zhou Y, Wong DF, Prince JL, Ferrucci L, et al. Individual estimates of age at detectable amyloid onset for risk factor assessment. Alzheimers Dement. 2016;12(4):373–9.
Fouquet M, Besson FL, Gonneaud J, La Joie R, Chetelat G. Imaging brain effects of APOE4 in cognitively normal individuals across the lifespan. Neuropsychol Rev. 2014;24(3):290–9.
Porter T, Burnham SC, Milicic L, Savage G, Maruff P, Lim YY, et al. Utility of an Alzheimer’s disease risk-weighted polygenic risk score for predicting rates of cognitive decline in preclinical Alzheimer’s disease: a prospective longitudinal study. J Alzheimers Dis. 2018;66(3):1193–211.
Kumar A, Shoai M, Palmqvist S, Stomrud E, Hardy J, Mattsson-Carlgren N, et al. Genetic effects on longitudinal cognitive decline during the early stages of Alzheimer’s disease. Sci Rep. 2021;11(1):19853.
Yu L, Boyle P, Schneider JA, Segawa E, Wilson RS, Leurgans S, et al. APOE epsilon4, Alzheimer’s disease pathology, cerebrovascular disease, and cognitive change over the years prior to death. Psychol Aging. 2013;28(4):1015–23.
Marden JR, Mayeda ER, Walter S, Vivot A, Tchetgen Tchetgen EJ, Kawachi I, et al. Using an Alzheimer disease polygenic risk score to predict memory decline in Black and White Americans over 14 years of follow-up. Alzheimer Dis Assoc Disord. 2016;30(3):195–202.
Gustavson DE, Reynolds CA, Hohman TJ, Jefferson AL, Elman JA, Panizzon MS, et al. Alzheimer’s disease polygenic scores predict changes in episodic memory and executive function across 12 years in late middle age. J Int Neuropsychol Soc. 2023;29(2):136-47.
Pettigrew C, Soldan A. Defining cognitive reserve and implications for cognitive aging. Curr Neurol Neurosci Rep. 2019;19(1):1.
Li Z, Shue F, Zhao N, Shinohara M, Bu G. APOE2: protective mechanism and therapeutic implications for Alzheimer’s disease. Mol Neurodegener. 2020;15(1):63.
Bellou E, Baker E, Leonenko G, Bracher-Smith M, Daunt P, Menzies G, et al. Age-dependent effect of APOE and polygenic component on Alzheimer’s disease. Neurobiol Aging. 2020;93:69–77.
Leonenko G, Baker E, Stevenson-Hoare J, Sierksma A, Fiers M, Williams J, et al. Identifying individuals with high risk of Alzheimer’s disease using polygenic risk scores. Nat Commun. 2021;12(1):4506.
Neu SC, Pa J, Kukull W, Beekly D, Kuzma A, Gangadharan P, et al. Apolipoprotein E genotype and sex risk factors for Alzheimer disease: a meta-analysis. JAMA Neurol. 2017;74(10):1178–89.
Kim H, Devanand DP, Carlson S, Goldberg TE. Apolipoprotein E Genotype e2: Neuroprotection and its limits. Front Aging Neurosci. 2022;14: 919712.
Singh PP, Singh M, Mastana SS. APOE distribution in world populations with new data from India and the UK. Ann Hum Biol. 2006;33(3):279–308.
Acknowledgements
The authors gratefully acknowledge the participants and staff from each study for their contributions to the research program.
Funding
The Preclinical AD Consortium is supported by the National Institutes of Health (NIH), United States [grant number RF1-AG059869]. The individual studies in the consortium are funded, in part, by the following grants: U19-AG033655, P01-AG026276, RF1-AG027161, and the Australian Commonwealth Scientific Industrial Research Organization (CSIRO), as well as the NIA Intramural Program. M. Albert, C. Pettigrew, and A. Soldan are supported by NIH grant P30-AG066507. A.L. Gross was supported by NIH grants R01-AG030153 and NIA R01-AG070953. J.C. Morris is supported by NIH grants P30-AG066444, P01-AG003991, P01-AG026276, U19-AG032438, and U19-AG024904. C. Cruchaga is supported by NIH grants R01-AG044546, P01-AG003991, RF1-AG053303, RF1-AG058501, and U01-AG058922. Funding agencies were not involved in study design, data collection, data analysis, interpretation of data, or writing of the manuscript.
Author information
Authors and Affiliations
Contributions
Acquisition or interpretation of data, drafting/revising of manuscript for content, approval of submitted version, and personal accountability for their own contributions: all authors. Study concept or design: CP, AS, and MA. Statistical analyses: JN, VS, JW, TH, AG.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Study protocols for all Preclinical AD Consortium sites were approved by each site’s local institutional review board. All participants provided written informed consent. This study was conducted in accordance with the Declaration of Helsinki.
Consent for publication
Not applicable.
Competing interests
The following authors declare that they have no competing interests: C. Pettigrew, J. Nazarovs, A. Soldan, V. Singh, J. Wang, T. Hohman L. Dumitrescu, J. Libby, B. Kunkle, A.L. Gross, Q. Lu, C. Engelman, P. Maruff, S.M. Laws, J.C. Morris, J. Hassenstab, S.M. Resnick, M.H. Kitner-Triolo, and Y. An. C. L. Masters and M. Albert are advisors to Eli Lilly. C. Cruchaga receives research support from GSK and is a member of the advisory board of Vivid Genomics and Circular Genomics. S. Johnson has served as an advisor to Roche Diagnostics.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Supplementary Table 1.
Cognitive tests included in the harmonized cognitive factor scores, by cohort. Supplementary Table 2. APOE genotyping approaches used by each PAC cohort. Supplementary Table 3. Baseline participant characteristics, by cohort, for APOE analyses. Values reflect mean (SD) unless otherwise indicated. Supplementary Table 4. Baseline participant characteristics, by cohort, for AD-PRS analyses. Values reflect mean (SD) unless otherwise indicated. Supplementary Table 5. Mixed-effects model results for AD-PRSAPOE and CR in relationship to cognitive trajectories. Supplementary Table 6. Descriptive statistics by follow-up diagnosis and mixed-effects model results for AD genetic risk and CR in relationship to cognitive trajectories, excluding individuals who progressed from normal cognition to MCI or dementia. Supplementary Table 7. Mixed-effects model results for AD genetic risk and the components of the CR index score in relationship to cognitive trajectories. Supplementary Table 8. Mixed-effects model results for AD-PRSw/oAPOE and CR in relationship to cognitive trajectories, a) excluding related individuals and b) covarying for population PCs. Supplementary Table 9. Mixed-effects model results for AD-PRSAPOE and CR in relationship to cognitive trajectories, a) excluding related individuals and b) covarying for population PCs. Supplementary Figure 1. Spaghetti plots illustrating participant trajectories and estimated cognitive change by AD genetic risk profiles.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Pettigrew, C., Nazarovs, J., Soldan, A. et al. Alzheimer’s disease genetic risk and cognitive reserve in relationship to long-term cognitive trajectories among cognitively normal individuals. Alz Res Therapy 15, 66 (2023). https://doi.org/10.1186/s13195-023-01206-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13195-023-01206-9