
Abstract
Background
Arterial stiffening has emerged as an important risk factor for Alzheimer’s disease (AD) and related dementias. Carotid-femoral pulse wave velocity has been proposed as a non-invasive and reproducible method to assess arterial stiffness. However, the association of pulse wave velocity with performance across multiple cognitive domains as well as interactions with in vivo AD biomarkers and apolipoprotein E (APOE) genotype has received limited study.
Method
We studied 193 older adult volunteers (167 with normal cognition and 26 with mild cognitive impairment) who underwent comprehensive medical and neuropsychological evaluation at the University of California, San Diego Alzheimer’s Disease Research Center. Cerebrospinal fluid (CSF) biomarkers were available on 123 participants (63%). Linear models examined whether pulse wave velocity significantly interacted with APOE ε4 status and CSF AD biomarker positivity (based on the ratio of total tau over beta-amyloid [tau/Aβ42]) on memory, language, executive functioning, attention, and visuospatial abilities.
Results
After adjusting for demographic characteristics and vascular risk burden, across the entire sample, pulse wave velocity was associated with poorer executive functioning but not the performance in the other cognitive domains. When the modifying effects of AD genetic risk and CSF AD biomarkers were considered, pulse wave velocity interacted with APOE genotype and CSF tau/Aβ ratio such that a stronger association between elevated pulse wave velocity and poorer memory performance was found among those positive for CSF and genetic AD markers. There were no significant interaction effects for non-memory cognitive domains.
Conclusion
The findings suggest that pulse wave velocity, a non-invasive method to assess arterial wall properties, may be a useful marker of risk for cognitive decline, particularly among individuals who are APOE ε4 carriers or CSF AD biomarke0r-positive.
Similar content being viewed by others
Introduction
Risk factors for cerebrovascular disease can also increase the risk of developing Alzheimer’s disease (AD) and are potentially modifiable to prevent or delay cognitive impairment [1, 2]. Arterial stiffness underlies the effect of blood pressure on the brain and has emerged as an important non-traditional vascular risk factor [3, 4]. Arterial stiffening occurs with aging and is exacerbated by conditions such as hypertension and diabetes [5]. Pulse wave velocity (PWV) is a non-invasive and reproducible method to assess arterial stiffness [6] that has been linked to increased cerebral small vessel disease evidenced by white matter hyperintensities on magnetic resonance imaging (MRI) and to β-amyloid (Aβ) accumulation associated with AD [1]. Indeed, increased PWV (i.e., greater arterial stiffness) has been proposed as a possible mechanism linking hypertension to both cerebral small vessel disease and Aβ accumulation [1]. Increased PWV may damage the microcirculation due to elevated flow pulsatility [7, 8] and interfere with Aβ clearance by impairing perivascular drainage [9].
Higher PWV has been shown to be associated with poorer cognitive performance (particularly episodic memory and executive functioning) [7, 10] in normally aging samples, mild cognitive impairment (MCI) [11], and cognitive decline over time [12, 13]; however, findings have been inconsistent with some studies reporting the loss of this effect after adjustment for other cardiovascular risk factors [14]. The association between higher PWV and poorer cognition may be particularly salient in carriers of the apolipoprotein E (APOE) ε4 allele [15], the strongest genetic risk factor for late-onset, sporadic AD [16, 17]. APOE ε4 promotes blood-brain barrier (BBB) breakdown [18] and facilitates Aβ accumulation in the brain parenchyma and blood vessel walls [19]. Notably, APOE ε4-mediated neurovascular defects appear to occur prior to neuronal dysfunction and degeneration [18], suggesting that APOE ε4 carriers may be more vulnerable than non-carriers to cerebrovascular dysfunction stemming from adverse vascular changes such as increased PWV [15].
Prior neuroimaging and neuropathological investigations suggest that the co-occurrence of cerebrovascular disease and AD-related changes lowers the threshold at which pathology is expressed as cognitive impairment [20, 21]. These findings suggest that measures of arterial stiffening and in vivo measures of cerebrospinal fluid (CSF) tau and Aβ may interact to reduce cognitive performance in older adults prior to the development of dementia. To test this possibility, we examined the relationships among PWV, genetic and CSF AD risk factors (APOE ε4 genotype, CSF Aβ42, and tau), and cognition in a well-characterized sample of older adults free of clinical dementia and stroke. We hypothesized that higher PWV would be associated with poorer episodic memory and executive functioning, especially in individuals at elevated risk of developing AD (i.e., APOE ε4 carriers or CSF tau/Aβ+).
Materials and methods
Standard protocol approvals and participant consents
Participants for this cross-sectional study were selected from the ongoing longitudinal study of the University of California, San Diego (UCSD) Shiley-Marcos Alzheimer’s Disease Research Center (ADRC) and ADRC-affiliated research studies. The research protocols were reviewed and approved by the human subject’s review boards at UCSD and/or the VA San Diego Healthcare System. Informed consent was obtained from all participants.
Participants
Participants were 193 older adults without dementia who had completed clinical, neurological, and neuropsychological evaluations under the ongoing ADRC research study protocol [22, 23]. Non-demented participants are recruited to the ADRC from the community through community outreach events and word-of-mouth and from local practitioners who refer patients with possible memory deficits. The inclusion criteria for the present study included available PWV and neuropsychological test data and no current major physical/medical health problems. The exclusion criteria included a history of major stroke, neurologic disorder, major psychiatric illness, substance abuse, or learning disability. Overall, the participants had a mean age of 74.9 ± 5.9 (mean ± standard deviation) years and a mean of 16.7 ± 2.4 years of formal education, and 53% were women and 10% were Hispanic. Based on the results of the ADRC evaluations, 167 participants were classified as cognitively normal (CN) and 26 as MCI by consensus of a multidisciplinary team that included two senior neurologists and a neuropsychologist. Forty percent of the participants had at least one copy of the APOE ε4 allele. This included 64/167 (38%) CN participants and 14/26 (54%) MCI participants. CSF was available for 123 participants (64.7% of the sample; 103 CN, 20 MCI). The use of anticoagulant medication was a contraindication for lumbar puncture (see Table 1 for participant characteristics across the entire sample; see supplemental tables comparing the characteristics of APOE ε4+ versus APOE ε4− participants (Supplemental Table 1) and tau/Aβ42+ versus tau/Aβ42− participants (Supplemental Table 2)). Notably, there were no significant group differences between APOE ε4+ and APOE ε4− participants or between tau/Aβ42+ and tau/Aβ42− participants, in terms of PWV.
Neuropsychological evaluation
The comprehensive neuropsychological test battery included measures of global cognitive function (Dementia Rating Scale, Mini Mental State Examination (MMSE), Clinical Dementia Rating (CDR)), memory (Wechsler Memory Scale-Revised (WMS-R) Visual Reproduction and Logical Memory, California Verbal List Learning Test (CVLT)), language (Multilingual Naming Test (MiNT), letter fluency (FAS), category fluency (animals, fruits, vegetables), Pyramids and Palm Trees), executive functions and attention (Modified Wisconsin Card Sorting Test, Color-Word Interference Test (CWIT), Trail Making Test Parts A and B, Wechsler Adult Scale of Intelligence-Revised (WAIS-R) Digit Symbol Substitution Test, WMS-R Digit Span), and visuospatial abilities (Wechsler Intelligence Scale for Children-Revised (WISC-R) Block Design Test, WMS-R Visual Reproduction copy).
Cognitive domain scores were generated through principal component analysis (PCA) with varimax rotation of all cognitive test scores (excluding global measures CDR, MMSE, and DRS) using previously described methods [24]. Prior to the PCA, a small percentage of missing scores for each test (< 5% for all tests, except for up to 10% for CWIT and visual reproduction copy) was imputed using a partial means matching approach based on demographics, diagnostic classification, and scores on global cognitive measures and the other cognitive tests. The PCA resulted in five components which were conceptually labeled “memory,” “executive functioning,” “language,” “visuospatial abilities,” and “attention” based on the tests with the highest loadings in each component (Table 2). A cognitive domain score was generated for each component based on the loadings for that component. Test scores from a pool of 146 “robust” normal controls (i.e., diagnosed as normal on their first ADRC evaluation and remained normal for the duration of their participation in the longitudinal study) were submitted to the same component loadings to generate “normal” cognitive domain scores that were used as reference values to “normalize” (i.e., convert cognitive domain scores to z-scores) the scores of the current study participants. The robust normal control participants were selected from the overall ADRC sample in a separate process not associated with the current study; however, 90 of the 146 (62%) robust normal control participants were included in the present study.
Vascular risk assessment: Framingham Stroke Risk Profile (FSRP)
Estimated 10-year stroke risk (as a percentage) was derived using the revised Framingham Stroke Risk Profile (FSRP) [25] which was calculated using exponential equations with sex-specific baseline survival rates and sex-specific beta coefficients for the following risk factors: age, systolic blood pressure, diabetes mellitus, history of cardiovascular disease, atrial fibrillation, cigarette smoking, and use of antihypertensive medications. Systolic blood pressure was the average of three blood pressure readings. Diabetes was defined as self-reported diabetes, use of an anti-diabetic therapy, or casual blood glucose ≥ 200 mg/dL. History of cardiovascular disease (coronary artery disease [myocardial infarction, angina pectoris, coronary insufficiency], intermittent claudication, or cardiac failure) and atrial fibrillation were determined by clinical interview, physical exam, and review of outside medical care records and laboratory studies. Current smoking (yes/no) was based on self-report. The use of antihypertensive medications was ascertained through medication review. Height and weight were recorded, and body mass index (BMI) was calculated with the following formula: weight in kilograms/height in meters squared.
Pulse wave velocity
Aortic-femoral PWV was measured with the SphygmoCor XCEL device (AtCor Medical, Sydney, NSW, Australia) using well-validated procedures [26, 27] performed by trained operators. All measurements were collected with the participant in the supine position after 10 min of rest. Femoral pulse was measured using a blood pressure cuff around the upper thigh. Carotid pulse was simultaneously measured with a tonometer manually applied at the neck. On average, three PWV measurements were recorded, and the mean value was used in statistical analyses.
Biomarker acquisition and analysis
Participants received a research lumbar puncture with standardized procedures, preanalytical preparation of CSF, and storage of CSF as previously described [28] and in accordance with the recommended best practices [29]. In brief, CSF (15–25 mL) was collected by routine lumbar puncture early in the morning after overnight fasting. Samples were processed, aliquoted into 500 μL fractions in polypropylene microtubes, snap-frozen, and stored at − 80 °C until assayed. Lumbar punctures were generally conducted within 1 year of the PWV measurements for the vast majority of the participants, although we included CSF data collected within 3 years of the baseline visit given research showing the stability of CSF biomarkers over several years [30].
CSF AD biomarkers examined were beta-amyloid (Aβ42), total tau (Tau), and the ratio of tau over beta-amyloid (tau/Aβ42). A small portion of cases (n = 18) had biomarkers analyzed in the facilities of ADx (Ghent, Belgium) using ELISA assays developed by ADx and commercialized by EUROIMMUN AG (Lubeck, Germany). The remaining cases’ samples (n = 106) were analyzed locally at UCSD using the automated Lumipulse platform using assays developed with established monoclonal antibodies (Fujirebio Inc.) [31]. Weighted Deming regression of a set of 113 CSF samples analyzed on both platforms demonstrated high correlation (Pearson’s R of .87 for Aβ42 and .95 for Tau), so the resulting equations were used to transform ADx values into native Lumipulse space for analyses. A cutpoint for biomarker positivity in Lumipulse space was derived from CSF samples from a larger cohort of 462 unique participants at the UCSD ADRC (ranging from cognitively normal to severely demented). The ratio of tau/Aβ42 was used as it appears to provide the best subdivision of individuals without dementia into those with and without pre-clinical AD [32]. A 2-component mixture model was fit to the bimodal distribution of the log-transformed tau/Aβ42 ratio using the mixtools [33] package version 1.2.0 for R, and the cutpoint of tau/Aβ42 > 0.52 was chosen as the value at which an individual was equally likely to belong to either component of the bimodal distribution [34]. This cutpoint is highly consistent with a published cutpoint (tau/Aβ42 > 0.54) for AD biomarker positivity using the Lumipulse assays, derived against clinical read of amyloid PET scans and validated in multiple cohorts [31].
Statistical analysis
Demographics and clinical characteristics between those with and without CSF were compared by Student’s t-test and chi-squared tests as appropriate. Relationships between PWV and performance in each cognitive domain were analyzed with separate linear models adjusted for age, sex, education, and FSRP. These analyses were then repeated with APOE genotype or CSF AD biomarker status (+/-) added to explore the interaction of PWV and AD risk markers (APOE ε4+; tau/Aβ42+) on cognition (while adjusting for age, sex, education, and FSRP).
Additional post hoc analyses were performed to determine whether significant results were retained in models including the individual FSRP components in place of the overall FSRP. That is, in cases where there were significant results, we reran the primary analyses described above but in place of overall FSRP instead adjusted for systolic blood pressure, history of diabetes, cardiovascular disease and/or atrial fibrillation, current smoking, and use of antihypertensive medication. We also reran these analyses with the individual FSRP components listed above while adjusting for two more vascular risk factors: BMI and history of transient ischemic attack (TIA).
Results
Associations of PWV with participant characteristics
Across the cohort, there was a significant increase in PWV with increasing age in both men and women (p < 0.001), with no evidence of an interaction between sex and age (p = .89). Overall, men had higher PWV than women (p < 0.001) (Fig. 1A). There was no significant association between PWV and APOE ε4 status (Fig. 1B), nor between PWV and the level of CSF Tau or Aβ42, or the tau/Aβ42 ratio (Fig. 1C).

PWV is associated with age and sex but does not differ by APOE ε4 or AD CSF biomarker status. A PWV is shown as a function of age for male and female participants. Regression lines fit separately by sex show nearly identical slopes, with men showing consistently higher PWV across the age range. B Boxplot of PWV as a function of APOE genotype shows no difference between those with an APOE ε4 allele (ε2ε4, ε3ε4, ε4ε4) and those without (ε2ε2, ε2ε3, ε3ε3). C PWV is plotted as a function of AD biomarker level (tau/Aβ ratio). A regression line shows no association. The dashed vertical line represents the biomarker positivity threshold (> 0.52)
Associations of PWV with cognitive test performance
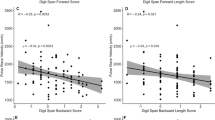
Performance on each of the cognitive domain scores is presented as a function of PWV in Fig. 2A. After adjusting for age, sex, education, and FSRP, PWV was significantly negatively associated with the executive domain score (β = −0.09 ± 0.04, p = .03), but not with the memory (β = −0.03 ± 0.04, p = .43), language (β = 0.06 ± 0.04, p = .07), attention (β = 0.03 ± 0.04, p = .42), or visuospatial abilities (β = 0.04 ± 0.05, p = .31) domain scores (Fig. 2A).

PWV predicts executive function beyond age and sex and interacts with APOE genotype and AD CSF biomarkers to predict memory performance. A Cognitive domain z-scores are shown as a function of PWV. Regression models adjusted for age, sex, education, and FSRP (excluding age points) demonstrate a significant main effect of PWV on executive function (p = 0.03). B The same cases were classified based on APOE genotype as APOE ε4+ (ε2ε4, ε3ε4, ε4ε4) or APOE ε4 − (ε2ε2, ε2ε3, ε3ε3). In regression models examining the interaction of PWV and APOE genotype, a significant interaction (p = 0.01) suggested that PWV was more predictive of memory scores in those that were APOE ε4+. C In a subset of patients with CSF biomarkers, individuals were classified into AD-like and non-AD profiles based on the tau/Aβ1–42 ratio. In regression models examining the interaction of PWV and CSF AD biomarker status, a significant interaction (p = 0.02) suggests that PWV was similarly more predictive of memory z-scores in those that were AD-like in their profile
Interaction of APOE genotype with PWV on cognitive test performance
Performance on each of the cognitive domain scores is presented as a function of PWV separately for APOE ε4+ and ε4− participants in Fig. 2B. After adjusting for age, sex, education, and FSRP, there was a significant interaction between PWV and APOE genotype on the memory domain score (interaction p = .01) reflecting a larger decrease in performance with increasing PWV for the ε4+ participants than for the ε4− participants. There was no interaction between PWV and APOE genotype for the executive functioning (p = .73), language (p = .86), attention (p = .13), or visuospatial abilities (p = .21) domain scores (Fig. 2B).
Interaction of AD biomarkers with PWV on cognitive test performance
Performance on each of the cognitive domain scores is presented as a function of PWV separately for AD biomarker+ and AD biomarker− participants (defined by the tau/Aβ42 ratio cutoff) in Fig. 2C. After adjusting for age, sex, education, and FSRP, there was a significant interaction between PWV and AD biomarker positivity on the memory domain score (interaction p = .01) reflecting a larger decrease in performance with increasing PWV for the AD biomarker+ participants than for the AD biomarker− participants. There was no interaction between PWV and AD biomarker positivity for the executive functioning (p = .69), language (p = .97), attention (p = .23), or visuospatial abilities (p = .83) domain scores (Fig. 2C).
When additional post hoc analyses including individual vascular risk factors in place of overall FSRP score were performed, the results remained similar. That is, the significant main effect of the pulse wave velocity on executive function, and the significant interactions of pulse wave velocity and both APOE ε4 status and CSF AD biomarker status on memory, remained significant (see Supplemental Tables 3, 4, and 5 for detailed results).
Discussion
We found that increased arterial stiffness measured through carotid-femoral PWV is associated with poorer performance on tests of executive functioning and memory in a well-characterized sample of older adults free of clinical dementia or stroke. The relationship between PWV and executive functioning was independent of the degree of AD risk as determined by APOE genotype or CSF AD biomarkers. In contrast, the relationship between elevated PWV and reduced memory performance was only present in at-risk participants by virtue of the APOE ε4 genotype or an above threshold CSF tau/Aβ ratio. Notably, the observed relationships between PWV and cognition were apparent even after adjusting for important demographic factors and overall cardiovascular risk estimated by the FSRP.
Arterial stiffening increases with advancing age, particularly when cardiovascular disease risk factors are present [35]. This increase in arterial stiffening results in higher PWV and pressure pulsatility, a reduction of the normal protective gradient of increasing stiffness moving from aorta to periphery, transmission of potentially harmful pulsatile energy, and reactive changes to microvascular function and structure that may compromise blood flow [8]. High-flow organs such as the brain may be particularly vulnerable to these secondary changes to the microcirculation and reduced perfusion [8]. Consistent with this possibility, we found that elevated PWV, a reflection of increased arterial stiffness, was associated with poorer executive function regardless of the degree of AD risk. Executive functioning has been repeatedly shown to decline in the context of normal aging [36], and indeed, “normal” cognitive aging has been conceptualized as a selective vulnerability in frontal-subcortical executive processes [37, 38]. Our results suggest that arterial stiffening may contribute to this age-related decline (see [39]). Interestingly, however, we observed a relationship between PWV and executive functioning even after adjusting for age. This suggests that elevated PWV may relate to executive decline over and beyond normal, expected age-related changes [39], and this finding is consistent with prior evidence demonstrating that vascular damage preferentially affects frontally mediated executive abilities [40, 41].
Our finding that elevated PWV interacts with APOE genotype and CSF tau/Aβ42 ratio to influence memory function is consistent with previous research suggesting that high pulse pressure and vascular risk factors may interact with genetic risk for AD and markers of AD-related pathology to confer an increased risk of cognitive decline [39, 42, 43]. For example, a previous study found that APOE ε4 carriers demonstrated poorer cognitive performance than non-carriers among participants with higher aortic PWV [15]. The authors proposed that APOE ε4 carriers may be more vulnerable to vascular changes given a loss or reduction of normal protective mechanisms that may be compromised due to existing neurovascular dysfunction and increasing neuropathology. It is possible that there is a threshold effect such that the adverse impact of higher PWV on cognition in at-risk adults may emerge at PWV values that are not detrimental to cognition in older adults with low risk of AD [15].
Our results are also consistent with previous research that has shown reduced regional cerebral blood flow and increased regional cerebrovascular resistance in older adults with elevated vascular risk and in those with MCI and AD [44,45,46]. These cerebrovascular changes were observed in the subcortical, frontal, and medial temporal regions, and they were linked to poorer cognitive abilities. Impaired cerebrovascular regulation and cerebral hypoperfusion may be most harmful in these brain regions because they are among the most metabolically active, are supplied by terminal arteries, and thereby are susceptible to the effects of small vessel disease, and may be affected by Aβ-mediated vasoconstriction [15, 46]. Our finding of associations between elevated PWV and reduced memory performance in those with AD risk (i.e., APOE e4+ or AD CSF biomarker+) dovetail with this prior work and may reflect the vulnerability of the frontal and hippocampal regions to vascular dysfunction and accumulating ischemic insults [47, 48].
The present results contribute to a growing body of research that suggests vascular vulnerabilities interact with AD pathophysiology to increase the risk of neurodegeneration [39, 43] and cognitive decline [39, 42]. We and others have previously shown that elevated vascular risk burden influences the clinical expression of AD [21] whereby the overlap of cerebrovascular disease and Aβ deposition in the brain lowers the threshold at which an individual with accumulating neuropathology develops cognitive impairment [21, 49]. The two-hit hypothesis of AD proposed by Zlokovic states that vascular disease may contribute to AD pathophysiology through blood-brain barrier breakdown resulting in the leakage of neurotoxic molecules into the tissue and/or through chronic hypoperfusion [2]. It also has been suggested that cerebrovascular abnormalities may impair Aβ clearance via impairment of perivascular drainage [9, 50] and may also directly lead to neurodegeneration independent of cerebral amyloidosis [4]. Indeed, greater arterial stiffening has been associated with the presence of multiple forms of neuropathology including white matter disease, cerebral microbleeds, and tau and Aβ deposition [1, 4]. Given that vascular risk factors such as arterial stiffening are potentially modifiable, their association with cognition suggests that in some cases, cognitive impairment and dementia may be prevented and/or delayed [51]. Targeting arterial stiffening and other vascular risk factors through lifestyle and/or pharmacological interventions may be a promising way to facilitate brain health in aging.
Although PWV has been associated with white matter hyperintensity volume (WMH) [1], studies suggests that WMH only partially mediates the effect of hypertension on cognitive performance [52]. A recent study, for example, showed that microvascular dysfunction measured as a composite of MRI WMH volume and biomarkers of microvascular disease (e.g., plasma soluble intercellular adhesion molecule-1 [sICAM-1] and soluble vascular adhesion molecule-1 [sVCAM-1]) explained only 16.2% of the effect of aortic stiffness on cognitive function [53]. Studies examining WMH volume and other vascular risk factors such as diabetes also have not found an imaging metric that fully explains the association between the risk factor and cognitive performance [54, 55]. Taken together, these studies highlight the importance of examining vascular risk factors in and of themselves rather than only the downstream end-organ damage they may cause [55].
The strengths of this study include the use of a well-validated carotid-femoral PWV measurement to assess arterial stiffening, administration of a comprehensive neuropsychological test battery that allowed empirical derivation of cognitive domain scores, and examination of CSF tau and Aβ biomarkers to detect AD pathology in non-demented older adults. In addition, we adjusted for important demographic and vascular risk factor variables that influence cognition including age, sex, and aggregate vascular risk (as well as the individual FSRP components, BMI, and history of TIA in post hoc analyses), and our findings remained statistically significant suggesting PWV is an independent contributor to cognitive performance.
Limitations
Our study is limited in generalizability given the cohort is a relatively homogeneous sample of older adults who were predominantly White and well-educated with relatively good vascular health. Indeed, the prevalence of FSRP components of cardiovascular disease (14%) and diabetes (6%) in our sample were lower than in the general population over age 65 (24 to 37% for cardiovascular disease and 22 to 23% for diabetes) [56]. It is likely that associations between PWV and cognitive abilities would have been stronger in a sample with a greater vascular risk burden, and these associations should be explored in people with more prominent risk factors in future studies. Nonetheless, our findings suggest that even relatively mild vascular dysfunction may contribute to poorer cognitive function in individuals with elevated AD risk. In addition, the percentage of APOE ε4+ cognitively normal participants in our cohort (38%) is higher than reported in some previously published studies. AD case-control studies combining data from several research groups reported that among Caucasian individuals, approximately 14% of cognitively normal controls were APOE ε4 carriers [57, 58] (although allele frequencies are known to vary based on factors such as sex, ethnicity, and geography [59, 60]). However, the percentage of APOE ε4+ cognitively normal participants in our cohort is very similar to those reported in other AD cohort studies (e.g., Uniform Data Set of the Alzheimer’s Disease Centers [UDS] program and Australian Imaging, Biomarkers and Lifestyle Flagship Study of Ageing [AIBL]) [61]. Notably, there is bias in recruitment for our study and other AD cohort studies that results in enrichment for APOE ε4 carriers, and this limits the generalizability of our findings to the general population [61]. We also do not have available FLAIR WMH data for our cohort, which will be critical to include in future studies to better characterize the presence and extent of vascular disease in our participants. Future longitudinal studies are necessary to determine if APOE genotype and AD biomarkers influence the trajectories of PWV and its relationship to cognitive decline as well as to explore some of the potential mechanisms underlying these relationships.
Conclusions
The findings of the current study showed that elevated PWV is associated with poorer cognitive performance in older adults, particularly on memory tasks, in those who are at risk for AD. These findings suggest that PWV, a non-invasive method to assess arterial stiffness, should be explored as a potential marker of risk for cognitive decline in older adults. PWV appears to have added predictive value beyond the FSRP and individual FSRP variables, including blood pressure. While previous studies suggest that PWV correlates strongly with fluid-attenuated inversion recovery (FLAIR) MRI WMH measures [1], PWV is much easier and less expensive to acquire than MRI and can be measured and tracked in a clinician’s primary care office. In addition, there are very few contraindications of PWV assessment, whereas many older adults have contraindications to MRI (e.g., pacemakers, metal implants, claustrophobia). Our results also provide a rationale for attempts to improve central vascular function and decrease cerebral pulsatility as an intervention to reduce dementia risk by preventing or slowing the accumulation of AD and vascular neuropathology across the aging spectrum [1, 39].
Availability of data and materials
Anonymized datasets analyzed in the current study are available to qualified investigators on reasonable request.
Abbreviations
- AD:
-
Alzheimer’s disease
- APOE:
-
Apolipoprotein E
- CSF:
-
Cerebrospinal fluid
- Aβ:
-
Beta-amyloid
- PWV:
-
Pulse wave velocity
- MCI:
-
Mild cognitive impairment
- BBB:
-
Blood-brain barrier
- UCSD:
-
University of California, San Diego
- ADRC:
-
Alzheimer’s Disease Research Center
- CN:
-
Cognitively normal
- MMSE:
-
Mini-Mental State Examination
- CDR:
-
Clinical Dementia Rating
- WMS-R:
-
Wechsler Memory Scale-Revised
- CVLT:
-
California Verbal List Learning Test
- MiNT:
-
Multilingual Naming Test
- CWIT:
-
Color-Word Interference Test
- WAIS-R:
-
Wechsler Adult Scale of Intelligence-Revised
- WISC-R:
-
Wechsler Intelligence Scale for Children-Revised
- PCA:
-
Principal component analysis
- FSRP:
-
Framingham Stroke Risk Profile
- BMI:
-
Body mass index
- TIA:
-
Transient ischemic attack
References
Hughes TM, Wagenknecht LE, Craft S, et al. Arterial stiffness and dementia pathology: Atherosclerosis Risk in Communities (ARIC)-PET Study. Neurology. 2018;90:e1248–56. 2018/03/20. https://doi.org/10.1212/wnl.0000000000005259.
Zlokovic BV. Neurovascular pathways to neurodegeneration in Alzheimer’s disease and other disorders. Nat Rev Neurosci. 2011;12:723–38. 2011/11/04. https://doi.org/10.1038/nrn3114.
Hughes TM, Craft S, Lopez OL. Review of ‘the potential role of arterial stiffness in the pathogenesis of Alzheimer’s disease’. Neurodegener Dis Manag. 2015;5:121–35. 2015/04/22. https://doi.org/10.2217/nmt.14.53.
Nation DA, Edmonds EC, Bangen KJ, et al. Pulse pressure in relation to tau-mediated neurodegeneration, cerebral amyloidosis, and progression to dementia in very old adults. JAMA Neurol. 2015;72:546–53. 2015/03/31. https://doi.org/10.1001/jamaneurol.2014.4477.
Cockcroft JR, Webb DJ, Wilkinson IB. Arterial stiffness, hypertension and diabetes mellitus. J Hum Hypertens. 2000;14:377–80. 2000/07/06. https://doi.org/10.1038/sj.jhh.1001023.
Rabkin SW. Arterial stiffness: detection and consequences in cognitive impairment and dementia of the elderly. J Alzheimers Di. 2012;32:541–9. 2012/08/14. https://doi.org/10.3233/jad-2012-120757.
Mitchell GF, van Buchem MA, Sigurdsson S, et al. Arterial stiffness, pressure and flow pulsatility and brain structure and function: the Age, Gene/Environment Susceptibility--Reykjavik Study. Brain. 2011;134:3398–407. 2011/11/15. https://doi.org/10.1093/brain/awr253.
Mitchell GF. Effects of central arterial aging on the structure and function of the peripheral vasculature: implications for end-organ damage. J Appl Physiol (Bethesda, MD: 1985). 2008;105:1652–60. 2008/09/06. https://doi.org/10.1152/japplphysiol.90549.2008.
Weller RO, Boche D, Nicoll JA. Microvasculature changes and cerebral amyloid angiopathy in Alzheimer’s disease and their potential impact on therapy. Acta Neuropathol. 2009;118:87–102. 2009/02/24. https://doi.org/10.1007/s00401-009-0498-z.
Zhong W, Cruickshanks KJ, Schubert CR, et al. Pulse wave velocity and cognitive function in older adults. Alzheimer Dis Assoc Disord. 2014;28:44–9. 2013/05/02. https://doi.org/10.1097/WAD.0b013e3182949f06.
Meyer ML, Palta P, Tanaka H, et al. Association of central arterial stiffness and pressure pulsatility with mild cognitive impairment and dementia: the Atherosclerosis Risk in Communities Study-Neurocognitive Study (ARIC-NCS). J Alzheimers Dis. 2017;57:195–204. 2017/02/23. https://doi.org/10.3233/jad-161041.
Watson NL, Sutton-Tyrrell K, Rosano C, et al. Arterial stiffness and cognitive decline in well-functioning older adults. J Gerontol A Biol Sci Med Sci. 2011;66:1336–42. 2011/07/20. https://doi.org/10.1093/gerona/glr119.
Waldstein SR, Rice SC, Thayer JF, et al. Pulse pressure and pulse wave velocity are related to cognitive decline in the Baltimore Longitudinal Study of Aging. Hypertension. 2008;51:99–104. 2007/11/21. https://doi.org/10.1161/hypertensionaha.107.093674.
Poels MM, van Oijen M, Mattace-Raso FU, et al. Arterial stiffness, cognitive decline, and risk of dementia: the Rotterdam Study. Stroke. 2007;38:888–92. 2007/02/03. https://doi.org/10.1161/01.Str.0000257998.33768.87.
Cambronero FE, Liu D, Neal JE, et al. APOE genotype modifies the association between central arterial stiffening and cognition in older adults. Neurobiol Aging. 2018;67:120–7. 2018/04/16. https://doi.org/10.1016/j.neurobiolaging.2018.02.009.
Corder EH, Saunders AM, Strittmatter WJ, et al. Gene dose of apolipoprotein E type 4 allele and the risk of Alzheimer’s disease in late onset families. Science. 1993;261:921–3 1993/08/13.
Saunders NB, Zollinger WD, Rao VB. A rapid and sensitive PCR strategy employed for amplification and sequencing of porA from a single colony-forming unit of Neisseria meningitidis. Gene. 1993;137:153–62 1993/12/31.
Bell RD, Winkler EA, Singh I, et al. Apolipoprotein E controls cerebrovascular integrity via cyclophilin A. Nature. 2012;485:512–6. 2012/05/25. https://doi.org/10.1038/nature11087.
Castellano JM, Kim J, Stewart FR, et al. Human apoE isoforms differentially regulate brain amyloid-β peptide clearance. Sci Transl Med. 2011;3:89ra57. 2011/07/01. https://doi.org/10.1126/scitranslmed.3002156.
Provenzano FA, Muraskin J, Tosto G, et al. White matter hyperintensities and cerebral amyloidosis: necessary and sufficient for clinical expression of Alzheimer disease? JAMA Neurol. 2013;70:455–61. 2013/02/20. https://doi.org/10.1001/jamaneurol.2013.1321.
Bangen KJ, Nation DA, Delano-Wood L, et al. Aggregate effects of vascular risk factors on cerebrovascular changes in autopsy-confirmed Alzheimer’s disease. Alzheimers Dement J Alzheimers Assoc. 2015;11:394–403.e391. 2014/07/16. https://doi.org/10.1016/j.jalz.2013.12.025.
Galasko D, Hansen LA, Katzman R, et al. Clinical-neuropathological correlations in Alzheimer’s disease and related dementias. Arch Neurol. 1994;51:888–95. 1994/09/01. https://doi.org/10.1001/archneur.1994.00540210060013.
Salmon DP, Butters N. Neuropsychological assessment of dementia in the elderly. In: Katzman R, Rowe JW, editors. Principles of Geriatric Neurology. Philadelphia: F.A. Davis; 1992. p. 144–63.
Smirnov DS, Galasko D, Edland SD, et al. Cognitive decline profiles differ in Parkinson disease dementia and dementia with Lewy bodies. Neurology. 2020;94:e2076–87. 2020/04/26. https://doi.org/10.1212/wnl.0000000000009434.
Dufouil C, Beiser A, McLure LA, et al. Revised Framingham Stroke Risk Profile to Reflect Temporal Trends. Circulation. 2017;135:1145–59. 2017/02/06. https://doi.org/10.1161/circulationaha.115.021275.
Laurent S, Cockcroft J, Van Bortel L, et al. Expert consensus document on arterial stiffness: methodological issues and clinical applications. Eur Heart J. 2006;27:2588–605. 2006/09/27. https://doi.org/10.1093/eurheartj/ehl254.
Hwang MH, Yoo JK, Kim HK, et al. Validity and reliability of aortic pulse wave velocity and augmentation index determined by the new cuff-based SphygmoCor Xcel. J Hum Hypertens. 2014;28:475–81. 2014/01/17. https://doi.org/10.1038/jhh.2013.144.
Xiao MF, Xu D, Craig MT, et al. NPTX2 and cognitive dysfunction in Alzheimer’s disease. Elife. 2017;6 2017/04/26. https://doi.org/10.7554/eLife.23798.
Vanderstichele H, Bibl M, Engelborghs S, et al. Standardization of preanalytical aspects of cerebrospinal fluid biomarker testing for Alzheimer’s disease diagnosis: a consensus paper from the Alzheimer’s Biomarkers Standardization Initiative. Alzheimers Dement J Alzheimers Assoc. 2012;8:65–73. 2011/11/04. https://doi.org/10.1016/j.jalz.2011.07.004.
Lleó A, Alcolea D, Martínez-Lage P, et al. Longitudinal cerebrospinal fluid biomarker trajectories along the Alzheimer’s disease continuum in the BIOMARKAPD study. Alzheimers Dement J Alzheimers Assoc. 2019;15:742–53. 2019/04/11. https://doi.org/10.1016/j.jalz.2019.01.015.
Kaplow J, Vandijck M, Gray J, et al. Concordance of Lumipulse cerebrospinal fluid t-tau/Aβ42 ratio with amyloid PET status. Alzheimers Dement J Alzheimers Assoc. 2020;16:144–52. 2020/01/09. https://doi.org/10.1002/alz.12000.
Van Harten AC, Wiste HJ, Weigand SD, et al. CSF biomarkers in Olmsted County: evidence of 2 subclasses and associations with demographics. Neurology. 2020;95:e256–67. 2020/06/28. https://doi.org/10.1212/wnl.0000000000009874.
Benaglia T, Chauveau D, Hunter DR, et al. mixtools: an R package for analyzing mixture models. J Stat Softw. 2009;32:29. 2009-10-14. https://doi.org/10.18637/jss.v032.i06.
Bartlett JW, Frost C, Mattsson N, et al. Determining cut-points for Alzheimer’s disease biomarkers: statistical issues, methods and challenges. Biomark Med. 2012;6:391–400. 2012/08/25. https://doi.org/10.2217/bmm.12.49.
Mitchell GF, Guo CY, Benjamin EJ, et al. Cross-sectional correlates of increased aortic stiffness in the community: the Framingham Heart Study. Circulation. 2007;115:2628–36. 2007/05/09. https://doi.org/10.1161/circulationaha.106.667733.
Hultsch DF, Hertzog C, Small BJ, et al. Short-term longitudinal change in cognitive performance in later life. Psychol Aging. 1992;7:571–84. 1992/12/01. https://doi.org/10.1037//0882-7974.7.4.571.
Daigneault S, Braun CM. Working memory and the self-ordered pointing task: further evidence of early prefrontal decline in normal aging. J Clin Exp Neuropsychol. 1993;15:881–95. 1993/11/01. https://doi.org/10.1080/01688639308402605.
McPherson S, Koltai D. A practical guide to geriatric neuropsychology. New York: Oxford University Press; 2018.
Nation DA, Preis SR, Beiser A, et al. Pulse pressure is associated with early brain atrophy and cognitive decline: modifying effects of APOE-epsilon4. Alzheimer Dis Assoc Disord. 2016;30:210–5. 2016/08/25. https://doi.org/10.1097/wad.0000000000000127.
Lamar M, Price CC, Giovannetti T, et al. The dysexecutive syndrome associated with ischaemic vascular disease and related subcortical neuropathology: a Boston process approach. Behav Neurol. 2010;22:53–62. 2009/01/01. https://doi.org/10.3233/ben-2009-0237.
Libon DJ, Drabick DA, Giovannetti T, et al. Neuropsychological syndromes associated with Alzheimer’s/vascular dementia: a latent class analysis. J Alzheimers Dis. 2014;42:999–1014. 2014/07/16. https://doi.org/10.3233/jad-132147.
Bangen KJ, Beiser A, Delano-Wood L, et al. APOE genotype modifies the relationship between midlife vascular risk factors and later cognitive decline. J Stroke Cerebrovasc Dis. 2013;22:1361–9. 2013/04/23. https://doi.org/10.1016/j.jstrokecerebrovasdis.2013.03.013.
Bangen KJ, Himali JJ, Beiser AS, et al. Interaction between midlife blood glucose and APOE genotype predicts later Alzheimer’s disease pathology. J Alzheimers Dis. 2016;53:1553–62. 2016/07/10. https://doi.org/10.3233/JAD-160163.
Bangen KJ, Werhane ML, Weigand AJ, et al. Reduced regional cerebral blood flow relates to poorer cognition in older adults with type 2 diabetes. Front Aging Neurosci. 2018;10. Original Research. https://doi.org/10.3389/fnagi.2018.00270.
Clark LR, Nation DA, Wierenga CE, et al. Elevated cerebrovascular resistance index is associated with cognitive dysfunction in the very-old. Alzheimers Res Ther. 2015;7:3. 2015/01/01. https://doi.org/10.1186/s13195-014-0080-3.
Nation DA, Wierenga CE, Clark LR, et al. Cortical and subcortical cerebrovascular resistance index in mild cognitive impairment and Alzheimer’s disease. J Alzheimers Dis. 2013;36:689–98. 2013/05/15. https://doi.org/10.3233/jad-130086.
Raz N, Rodrigue KM, Acker JD. Hypertension and the brain: vulnerability of the prefrontal regions and executive functions. Behav Neurosci. 2003;117:1169–80. 2003/12/17. https://doi.org/10.1037/0735-7044.117.6.1169.
Zarow C, Vinters HV, Ellis WG, et al. Correlates of hippocampal neuron number in Alzheimer’s disease and ischemic vascular dementia. Ann Neurol. 2005;57:896–903. 2005/06/02. https://doi.org/10.1002/ana.20503.
Arvanitakis Z, Capuano AW, Leurgans SE, et al. Relation of cerebral vessel disease to Alzheimer’s disease dementia and cognitive function in elderly people: a cross-sectional study. Lancet Neurol. 2016;15:934–43. 2016/06/18. https://doi.org/10.1016/s1474-4422(16)30029-1.
Weller RO, Subash M, Preston SD, et al. Perivascular drainage of amyloid-beta peptides from the brain and its failure in cerebral amyloid angiopathy and Alzheimer’s disease. Brain Pathol. 2008;18:253–66. 2008/03/28. https://doi.org/10.1111/j.1750-3639.2008.00133.x.
Gottesman RF, Albert MS, Alonso A, et al. Associations between midlife vascular risk factors and 25-year incident dementia in the Atherosclerosis Risk in Communities (ARIC) cohort. JAMA Neurol. 2017;74:1246–54. 2017/08/08. https://doi.org/10.1001/jamaneurol.2017.1658.
Hajjar I, Quach L, Yang F, et al. Hypertension, white matter hyperintensities, and concurrent impairments in mobility, cognition, and mood: the Cardiovascular Health Study. Circulation. 2011;123:858–65. 2011/02/16. https://doi.org/10.1161/circulationaha.110.978114.
Rensma SP, Stehouwer CDA, Van Boxtel MPJ, et al. Associations of arterial stiffness with cognitive performance, and the role of microvascular dysfunction: the Maastricht Study. Hypertension. 2020;75:1607–14. 2020/04/11. https://doi.org/10.1161/hypertensionaha.119.14307.
Callisaya ML, Beare R, Moran C, et al. Type 2 diabetes mellitus, brain atrophy and cognitive decline in older people: a longitudinal study. Diabetologia. 2019;62:448–58. 2018/12/14. https://doi.org/10.1007/s00125-018-4778-9.
Zlokovic BV, Gottesman RF, Bernstein KE, et al. Vascular contributions to cognitive impairment and dementia (VCID): a report from the 2018 National Heart, Lung, and Blood Institute and National Institute of Neurological Disorders and Stroke Workshop. Alzheimers Dement J Alzheimers Assoc. 2020;16:1714–33. 2020/10/09. https://doi.org/10.1002/alz.12157.
Villarroel MA, Blackwell DL, Jen A. Tables of summary health statistics for U.S. adults: 2018 National Health Interview Survey. National Center for Health Statistics; 2019. Available from: http://www.cdc.gov/nchs/nhis/SHS/tables.htm.
Farrer LA, Cupples LA, Haines JL, et al. Effects of age, sex, and ethnicity on the association between apolipoprotein E genotype and Alzheimer disease. A meta-analysis. APOE and Alzheimer Disease Meta Analysis Consortium. JAMA. 1997;278:1349–56 1997/10/29.
Bang OY, Kwak YT, Joo IS, et al. Important link between dementia subtype and apolipoprotein E: a meta-analysis. Yonsei Med J. 2003;44:401–13. 2003/07/02. https://doi.org/10.3349/ymj.2003.44.3.401.
Zannis VI, Kardassis D, Zanni EE. Genetic mutations affecting human lipoproteins, their receptors, and their enzymes. Ad Hum Genet. 1993;21:145–319. 1993/01/01. https://doi.org/10.1007/978-1-4615-3010-7_3.
Eisenberg DT, Kuzawa CW, Hayes MG. Worldwide allele frequencies of the human apolipoprotein E gene: climate, local adaptations, and evolutionary history. Am J Phys Anthropol. 2010;143:100–11. 2010/08/25. https://doi.org/10.1002/ajpa.21298.
Heffernan AL, Chidgey C, Peng P, et al. The neurobiology and age-related prevalence of the ε4 allele of apolipoprotein E in Alzheimer’s disease cohorts. J Mol Neurosci. 2016;60:316–24. 2016/08/09. https://doi.org/10.1007/s12031-016-0804-x.
Acknowledgements
The authors would like to thank the dedicated UCSD ADRC study coordinators and staff members who contributed to the collection of the pulse wave velocity data.
Funding
This work was supported by the US Department of Veterans Affairs Clinical Sciences Research and Development Service (Merit Award 1I01CX001842 to K.J.B., Merit Award 1I01CX000565 to C.E.W.), NIA/NIH grants (NIH P30 AG062429 to D.G. and D.P.S.; R01 AG063782 to K.J.B.; R01 AG049810 and R01 AG054049 to M.W.B.), and the Alzheimer’s Association (AARG-18-566254 to K.J.B).
Author information
Authors and Affiliations
Contributions
K.J.B., D.S.S., D.P.S., and D.G. designed the study. K.J.B. and D.S.S. analyzed the data. D.S.S. made the figures. K.J.B., D.S.S., L.D-W., C.E.W., M.W.D., D.P.S., and D.G. drafted and revised the paper. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All procedures were approved by the Institutional Review Boards at UCSD. Written informed consent was obtained from every research participant according to the Declaration of Helsinki and the Belmont Report.
Consent for publication
Not applicable.
Competing interests
D. Galasko serves as an editor for Alzheimer’s Research and Therapy; is a consultant for Biogen, Inc., Fujirebio, Inc., and Amprion, Inc.; and serves on a Data Safety Monitoring Board for Cognition Therapeutics. D.P. Salmon serves as a paid consultant for Takeda Pharmaceuticals, Inc.; Aptinyx, Inc.; and Biogen, Inc. M. Bondi receives royalties from Oxford University Press. Other authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Table S1.
Participant Demographics and Clinical Characteristics by APOE ε4 Status. Table S2. Participant Demographics and Clinical Characteristics by AD CSF Biomarker Status. Table S3. Post-hoc Exploration of Influence of Individual Vascular Risk Variables in Place of Overall Framingham Stroke Risk Profile: Results of Models Examining Main Effect of PWV on Executive Function. Table S4. Post-hoc Exploration of Influence of Individual Vascular Risk Variables in Place of Overall Framingham Stroke Risk Profile: Results of Models Examining Interaction of PWV and APOE ε4 Status on Memory. Table S5. Post-hoc Exploration of Influence of Individual Vascular Risk Variables in Place of Overall Framingham Stroke Risk Profile: Results of Models Examining Interaction of PWV and CSF AD Biomarker Status on Memory.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Bangen, K.J., Smirnov, D.S., Delano-Wood, L. et al. Arterial stiffening acts synergistically with APOE genotype and AD biomarker status to influence memory in older adults without dementia. Alz Res Therapy 13, 121 (2021). https://doi.org/10.1186/s13195-021-00851-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13195-021-00851-2