
Abstract
Background
The epigenetic regulation of the renin–angiotensin–aldosterone system (RAAS) potentially plays a role in the pathophysiology underlying the high burden of hypertension in sub-Saharan Africans (SSA). Here we report the first epigenome-wide association study (EWAS) of plasma renin and aldosterone concentrations and the aldosterone-to-renin ratio (ARR).
Methods
Epigenome-wide DNA methylation was measured using the Illumina 450K array on whole blood samples of 68 Ghanaians. Differentially methylated positions (DMPs) were assessed for plasma renin concentration, aldosterone, and ARR using linear regression models adjusted for age, sex, body mass index, diabetes mellitus, hypertension, and technical covariates. Additionally, we extracted methylation loci previously associated with hypertension, kidney function, or that were annotated to RAAS-related genes and associated these with renin and aldosterone concentration.
Results
We identified one DMP for renin, ten DMPs for aldosterone, and one DMP associated with ARR. Top DMPs were annotated to the PTPRN2, SKIL, and KCNT1 genes, which have been reported in relation to cardiometabolic risk factors, atherosclerosis, and sodium-potassium handling. Moreover, EWAS loci previously associated with hypertension, kidney function, or RAAS-related genes were also associated with renin, aldosterone, and ARR.
Conclusion
In this first EWAS on RAAS hormones, we identified DMPs associated with renin, aldosterone, and ARR in a SSA population. These findings are a first step in understanding the role of DNA methylation in regulation of the RAAS in general and in a SSA population specifically. Replication and translational studies are needed to establish the role of these DMPs in the hypertension burden in SSA populations.
Similar content being viewed by others

Background
Sub-Saharan African (SSA) origin populations face a higher burden of hypertension compared with other ethnic groups [1], and African migrants in Europe have a much higher prevalence of hypertension than their non-migrating counterparts in Africa [2]. Salt sensitivity (SS) is one of the best studied pathophysiological mechanisms to explain the high prevalence of hypertension among SSA origin populations [3]. SS refers to an increase in blood pressure upon salt intake and relates to excessive sodium and water retention by the kidneys, and suppression of the renin-angiotensin-aldosterone system (RAAS) [4], a physiological system regulating circulating blood volume and blood pressure [5]. West African descent populations have higher prevalence of salt-sensitive hypertension [6], with a profile of suppressed renin, accompanied by an increased aldosterone-to-renin ratio [7]. SS is affected by multiple factors including genetics [8], and phenotypical aspects such as age, obesity, insulin resistance, and hypertension [9]. However, key underlying determinants and exact molecular mechanisms of SS among SSA populations still need to be elucidated. In this light, studying epigenetic modifications in relation to RAAS can be of interest. ‘Epigenetics’ refers to changes in readability and transcription of the genome, without alterations to the DNA sequence itself [10]. Epigenetic modifications, of which DNA methylation is the most widely studied epigenetic feature, are influenced by both genetic and environmental factors. Several studies have identified differentially methylated positions (DMPs) located in RAAS-related genes to be associated with hypertension [11, 12], including the AGT, AGTR1, ACE, NOS3, and SCNN1A genes [5, 13]. However, none of these studies have examined the association between epigenome-wide DNA methylation and concentration of RAAS hormones. Moreover, studies that identified RAAS-related genes were mainly conducted in European and African American populations, whereas these groups differ from SSA based populations in terms of genetics and environment. Therefore, the aim of this proof-of-principle study was to assess the association between DNA methylation and plasma renin and aldosterone concentrations, and aldosterone-to-renin ratio (ARR) in Ghanaians.
Methods
Study population and study design
For this study, baseline data of the longitudinal, multicentre Research on Obesity and Diabetes among African Migrants (RODAM) study were used. Details on the RODAM study have been published before [14] and will be briefly described here.
In the period 2012–2015, 6385 Ghanaian men and women were recruited. The participants resided in rural Ghana, urban Ghana, and in the European cities of London, Amsterdam, and Berlin. The majority of participants were of Akan ethnicity, and Ghanaians in Europe were first-generation migrants.
Of participants aged 25 years and older with complete data on physical examination and blood samples profile, 736 participants were selected for DNA methylation profiling. These participants were selected based on a case-control design, including about 300 cases with non-drug-treated diabetes, 300 controls without diabetes, and 135 controls with neither diabetes nor obesity. After excluding participants with sex discordances (n = 11), duplicates (n = 8), and those not meeting the quality control thresholds (n = 12), 713 eligible participants remained. Of these participants, those without aldosterone and renin measurements were excluded (n = 644, excluding all participants residing in London and Berlin as they were not included in aldosterone and renin analysis), as was one participant with an outlier in renin concentration (77 pg/mL), which was > 3 times the SD of the log-transformed renin concentration. This resulted in 68 participants in the current analysis, all residing in rural and urban Ghana, or Amsterdam (Additional file 1: FigureS1).
Phenotypic measurements
Data collection procedures for questionnaire and physical examination were highly standardised across the different study locations. Questionnaires were used to collect data on gender, age, level of education, and length of stay in Europe. Physical examination was performed using validated devices. Weight was measured in light clothing without shoes with a SECA 877 scale to the nearest 0.1 kg. Height was measured without shoes using a SECA 2017 portable stadiometer to the nearest 0.1 cm. Anthropometric measures were taken twice and the mean of the two measures was used in analyses. Body mass index (BMI) was calculated by dividing the weight in kilograms by the height in metres squared. After at least 5 min of rest, three blood pressure (BP) readings were taken in a sitting position, with a cuff fixed on the left arm. The mean of the second and third reading was used in the analyses. Hypertension was defined as having a BP of systolic ≥ 140 mmHg and/or diastolic ≥ 90 mmHg and/or the use of BP-lowering medication. BP-lowering medication was categorised based on Anatomical Therapeutic Chemical classification of medication that participants brought with them to the research location.
Venous blood samples were collected in the sitting position, after an overnight fast of at least ten hours. All samples were collected around the same time of the day (morning) to control for the influence of circadian rhythm. After samples collection, samples were immediately processed, aliquoted and cryopreserved, before storage in − 80˚C freezers. Samples collected in Ghana were shipped to Europe while kept frozen at − 80 ˚C. Fasting plasma glucose concentrations were measured using the hexokinase method by colorimetry, in the laboratory of the Institute of Tropical Medicine and International Health, Berlin, Germany. Diabetes mellitus was defined according to self-reported diabetes and/or fasting glucose ≥ 7.0 mmol/L. Aldosterone and renin concentration (pg/mL) were measured in heparin plasma samples, and analyses were performed at the Department of Internal Medicine of the Erasmus MC, Rotterdam, the Netherlands. All samples, including those from Ghana, were analysed in the same laboratory, to prevent inter-laboratory differences affecting the results. After thawing of the samples, renin concentration was determined by an immunoradiometric assay (Cisbio, Saclay, France) using an active site-directed radiolabelled antibody binding to renin only. The lower detection limit of this assay was 2 pg/mL. Aldosterone concentrations were measured by solid-phase radioimmunoassay (Demeditec Diagnostics, Kiel, Germany), with a lower detection limit of 12 pg/ml. Aldosterone-to-renin ratio (ARR, pg/mL/pg/mL) was calculated by dividing aldosterone by the renin concentration. The distributions of aldosterone, renin, and ARR were assessed using histograms and the Shapiro-Wilkinson test. To ensure normal distribution of the traits, aldosterone concentration was transformed using Box-Cox transformation, and renin and ARR were log-transformed. Renin, aldosterone and ARR were chosen for analysis, because of their relevance in the context of SS and salt-sensitive hypertension.
DNA methylation profiling, processing, and quality control
Previous RODAM publications have elaborated upon the DNA methylation profiling, processing, and quality control on whole blood samples [15], and this process will be summarised here. In the lab of Source BioScience, Nottingham, UK, the Zymo EZ DNAm™ kit was used for bisulfite conversion of DNA. Using the Infinium® HumanMethylation450 BeadChip, the converted DNA was amplified and hybridised, hereby quantifying DNAm levels of approximately 485,000 CpG sites. Methylation levels were measured based on the intensities of the methylated and unmethylated probes for each CpG site on the array. These intensities were expressed as methylation Beta values, which is a value between zero (unmethylated) and one (methylated). A log2 ratio of the intensities of methylated versus unmethylated probes was calculated, which is referred to as M values. Using R statistical software (version 4.2.0), quality control was performed using the MethylAid package (version 1.30.0), using default thresholds of 10.5 for methylated and unmethylated intensities, 11.75 for overall quality control, 12.75 for bisulfite conversion, 12.50 for hybridisation control, and 0.95 for detection p-value. Functional normalisation of the raw 450 K data was conducted using the minfi package (version 1.42.0). After the removal of probes annotated to the X and Y chromosomes, known to involve cross-hybridisation or to contain common single-nucleotide polymorphisms (SNPs) with a minor allele frequency of ≥ 5%, a set of 429,449 CpG sites remained for analysis [16]. Blood cell type distribution was estimated based on the method of Houseman et al. [17].
Statistical analyses
Association between renin, aldosterone, and ARR and DNA methylation
To assess differentially methylated positions (DMPs), multivariate linear regression was performed between renin concentration, aldosterone, and ARR (independent variables) and DNA methylation M values (dependent variable), using the Limma package (version 3.52.0). Methylation M values were used in statistical analysis to ensure normal distribution, whereas methylation Beta values were used to facilitate interpretation and visualisation. Models were adjusted for sex, age, BMI, diabetes mellitus, hypertension, estimated blood cell type counts (CD8 + T lymphocytes, CD4 + T lymphocytes, natural killer cells, B cells, monocytes, granulocytes), and technical covariates (hybridisation batch and array position), because of correlation with DNA methylation in the principal components analysis, as well as because of an overrepresentation of participants with diabetes and high BMI in the sample. Model fit was assessed using QQ plots, as well as the genomic inflation factor lambda. Because of improvement in model fit after bias and inflation correction using the R package bacon (version 1.24.0) [18], we applied this adjustment to all analyses (lambda with inflation correction for renin 1.046, aldosterone 0.995, ARR 1.026) (Additional file 1: FigureS2). False discovery rate (FDR) adjustment of the p-values was applied, to reduce the risk of false positive findings in multiple testing. An FDR-adjusted p-value of < 0.05 was considered epigenome-wide significant.
To identify the contribution of the top DMPs to the variance in renin and aldosterone concentration, linear regression was performed using z-standardised methylation M values of the identified DMPs as independent variable and the (untransformed) trait of interest as dependent variable. The R squared statistics from the linear regression analyses with and without covariates were used to calculate trait variance explained by each DMP. Similar methods were used to assess the explained variance in systolic and diastolic BP, with the z-standardised M values of the top DMPs associated with renin, aldosterone, and ARR as independent variables in the linear regression model, adjusted for age, sex, BMI, diabetes mellitus, blood cell distribution, and technical variates.
As several types of BP-lowering medication can interfere with the RAAS system, a sensitivity analysis excluding those on BP-lowering medication (n = 10) was performed, to assess the impact of medication use on the association.
For the top DMPs per trait, we extracted the median methylation Beta values with accompanying interquartile ranges, and stratified these per geographical location, to examine whether differences in methylation levels existed between participants residing in rural and urban Ghana, and Amsterdam. These median values were compared between the location using nonparametric the Kruskal–Wallis test. A two-sided p-value < 0.05 was considered statistically significant.
Differentially methylated regions
To assess whether DNA methylation of genomic regions, rather than on single positions, was associated with the traits of interest, the R package bumphunter (version 1.38.0) was used to assess differentially methylated regions (DMRs), using similar models as used in the DMP analysis. Methylation M value cut-offs of 0.2 was chosen for the input, which limited the analysis to 100 candidate regions and 20% difference in regression coefficient beta between candidate probes. The analysis was run with bootstrapping with 500 permutations. DMRs with more than two CpGs, and a family-wise error rate (FWER) < 0.2 were considered statistically significant. DMRs were visualised using coMET package (version 1.27.2).
Replication
We used the EWAS atlas [19] to extract all CpGs previously reported to be associated with BP, systolic blood pressure (SBP), diastolic blood pressure (DBP), and hypertension and performed a candidate DMP analysis. Additionally, we tried to replicate CpG sites significantly associated with eGFR in a large, multi-ethnic, meta-analysis of EWAS [20]. Lastly, we extracted the probes previously annotated to RAAS-related genes (ACE, AGT, REN, CYP11B2, HDS11B2, and NR3C2) [21] and performed a candidate-gene DMP analysis on these for each of our traits of interest. For these candidate-gene analyses, the same models, including adjustment for bias and inflation, were used as for the main analysis. All CpGs with an FDR-adjusted p-value of < 0.05 were considered to be statistically significant.
Biological relevance
Gene expression levels for the epigenome-wide significant DMPs were assessed using the publicly available iMethyl database, in which the DNA methylation levels of CD4 + T lymphocytes as well as gene expression levels, denoted per kilo base of transcript per million mapped fragments (FPKM), are reported for 100 apparently healthy individuals living in Japan [22].
Enrichment analysis using the Kyoto Encyclopedia of Genes and Genomes (KEGG) catalogue in package R missMethyl (version 1.30.0) was performed to gain insight into the function and biological pathways of our findings. The top 5000 CpGs with the smallest p-values per trait were used as input.
The gaphunter gfunction of the minfi package was used to examine whether the significant DMPs were potentially under the influence of genetic variation. The function was run with a threshold of 0.05, reflecting a gap of 5% in beta value, suggestive of genetic influence.
Results
Population characteristics
Table 1 shows the population characteristics. Males and females were included at nearly equal proportions, and the mean age was 52 years. The majority of the participants resided in rural and urban Ghana, and all Ghanaian migrants resided in Amsterdam. One-third of the participants had diabetes mellitus and close to 40% of the participants were classified as hypertensive. Ten participants reported taking prescribed BP-lowering medication, of which calcium channel blockers (n = 9) and angiotensin receptor blockers (n = 4) were the most used types of drugs. The median renin concentration was 7.62 pg/mL, the median aldosterone was 103.44 pg/mL, and the median ARR was 14.16 pg/mL/pg/mL.
Differentially methylated positions
Renin
We found one intergenic CpG, cg02105843, epigenome-wide significantly associated with renin concentration (Table 2, Fig. 1A). One standard deviation (SD) increase in methylation M-value of this DMP was associated with 9.08 pg/mL lower renin levels and this DMP contributed to 15% of the variance in renin concentration (Table 3). The top 5 DMPs associated with renin concentration explained 6.4% in variance in SBP and 8.0% in variance in DBP. Excluding participants on BP-lowering medication did not impact this result, and there was no difference in methylation levels for this DMP between participants residing in rural and urban Ghana or in Amsterdam.

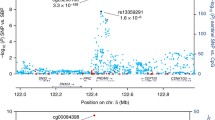
Manhattan plots for bacon adjusted p-values of the EWAS of renin A aldosterone B and aldosterone-to-renin ratio C. Dotted lines indicates epigenome-wide significant p-value
Aldosterone
Ten CpGs were associated with aldosterone concentration on an epigenome-wide level (Table 2, Fig. 1B). The DMPs with the smallest p-values were located in an intergenic region (cg06215643), in the transcription start site (TSS) of the RPL41 gene (cg03123773), and in the body of the KCNT1 gene. DMPs with the highest explained variance in aldosterone concentration were cg09869144 and cg15627834, located in the body of the MLYCD and SKIL genes, respectively, contributing to 73.58 and − 56.33 pg/mL change in aldosterone level with one SD increase in M value. The combined ten DMPs explained 46% of the variance in aldosterone concentration (Table 3), 19.6% in SBP, and 24.2% in DBP levels.
In the sensitivity analysis excluding ten participants with prescribed BP-lowering medication, four of the ten CpGs did no longer reach epigenome-wide significance. However, these four CpGs, cg17876128, cg14771658, cg18784903, and cg24500222, did show a similar direction of effect and effect size as in the main analysis including participants with BP-lowering medication. For the top DMPs, there was no significant difference in methylation levels between the geographical locations.
ARR
ARR was epigenome-wide significantly associated with methylation of intergenic CpG cg15602420 (Table 2, Fig. 1C). An increase of one SD in methylation level of this DMP was associated with 13.25 pg/mL/pg/mL lower ARR and explained 19% of the variance in this trait (Table 3). 6.2% of the variance in SBP and DBP were explained by the top 5 DMPs associated with ARR. Excluding participants with BP-lowering medication did not affect our findings. No difference in methylation level between the different locations of residence could be observed.
Differentially methylated regions
For renin, we identified two DMRs at an FWER < 0.2, annotated to the NFYA (Additional file 1: Figure S3) and the RNF39 gene (Additional file 1: Figure S4), both located on chromosome 6. One DMR, annotated to the HDL-DRB1 gene, was associated with aldosterone concentration (Additional file 1: Figure S5). No DMR was identified for the ARR. There was no overlap between the significant DMPs and DMRs.
Replication
Through the EWAS atlas we found 16 probes that had previously been associated with BP, 142 for SBP, 191 for DBP, and 151 probes for hypertension. Intergenic CpGs cg18264657 and cg11710912 annotated to the ARGLU1 gene that were previously associated with hypertension in other study populations of European and South Asian ancestry were associated with renin concentration and ARR in our Ghanaian study population (Table 4). Intergenic cg05376465, previously associated with SBP in European and South Asian ancestry population, was associated with aldosterone concentration in our study. 65 CpGs previously reported to be associated with eGFR in populations of European and African American ancestry were assessed in our Ghanaian population, of which three were associated with renin concentration and one with ARR. Intergenic CpG cg01695994, cg02059849 located in the body of PTP4A3 gene and cg22623033 annotated to the PIP5K1C gene were significantly associated with renin concentration, as was cg02059849 (PTP4A3) to ARR.
Next, we performed association analysis on a subset of 45 probes annotated to ACE, REN, CYP11B2, HSD11B2, and NR3C2 genes, which are all involved in the RAAS system. One of these CpGs, cg12841684 located in the body of the NR3C2 gene, was associated with ARR at an FDR adjusted p-value of 0.01.
Biological relevance
Generally, methylation levels as reported in the iMethyl database were similar compared to average methylation betas in our population (Additional file 1: Table S1). Additionally, for three CpGs associated with aldosterone, higher levels of methylation in the body of the SKIL and PTPRN2 gene were associated with higher gene expression, whereas higher levels of methylation in the body of the MLYCD gene were associated with lower gene expression.
In the pathway analysis using the KEGG catalogue, the top 20 pathways associated with renin, aldosterone, and ARR were involved in fatty acid metabolism, diabetes cardiomyopathy, and immunological processes (Additional file 1: Table S2). However, none of the pathways were statically significant at an FDR-adjusted p-value < 0.05.
None of the identified significant DMPs showed a gap in Beta value distribution in the gaphunter analysis, indicating no signs of genetic variation influencing methylation levels of these DMPs.
Discussion
Key findings
In this first EWAS on plasma aldosterone and renin concentrations, we identified one DMP associated with renin concentration, ten DMPs associated with aldosterone concentration, and one DMP associated with ARR in a Ghanaian population. These DMPs contributed to 15%, 46%, and 19% of the explained variance in renin, aldosterone, and ARR concentration, respectively. Additionally, DMPs associated with renin, aldosterone, and ARR explained a substantial percentage of the variance in SBP and DBP. For the genome-wide significant DMPs associated with renin and aldosterone concentration, no differences in methylation levels were observed between participants residing in rural and urban Ghana and Ghanaian migrants in Europe. Two DMRs associated with renin and one DMR associated with aldosterone concentration were identified. We found CpGs previously associated with hypertension and kidney function to be associated with concentrations of renin and aldosterone, and we found one DMP annotated to the NR3C2 gene of the RAAS system to be associated with ARR.
Discussion of the key findings
We found several DMPs associated with concentrations of aldosterone annotated to genes that have previously been reported to be related to CVD risk factors. For instance, hypermethylation in the PTPRN2 gene has been associated with metabolic syndrome in African American population [23], and hypermethylation of the SKIL gene has been associated with atherosclerosis [24]. We identified one DMP, cg21178689, annotated to the KCNT1 gene, which codes for potassium sodium-activated channel subfamily T, that, among others, regulates insulin secretion, heart rate, and smooth muscle contraction [25]. Methylation in this gene has previously been associated with BMI [26] and type 2 diabetes mellitus [27]. For renin, the significant DMP was located in an intergenic region; however, the nearby located gene PTDSS2, has previously been shown to relate to fat mass if expressed in adipose tissue [28]. DNA methylation of cg15602420, located downstream of the OTUD3 gene, was associated with ARR. Methylation in the OTUD3 gene has previously been associated with glucocorticoid exposure [29]. Additionally, the significant DMRs were annotated to genes associated with BMI [30], diabetes mellitus and coronary heart disease, and the pathway analysis suggested enrichment of pathways involved in CVD pathophysiology. These findings link hormones of the RAAS to other metabolic systems.
As this is the first EWAS on the RAAS, we could not replicate our findings nor could we replicate findings from previous studies. However, in our candidate approach, we found that several DMPs previously associated with hypertension and kidney function were also associated with concentrations of renin, aldosterone, and ARR. This suggests the potential shared regulatory mechanism. This is also supported by our findings that the top DMPs associated with plasma renin and aldosterone concentration explained a substantial percentage of variance in SBP and DBP. Remarkably, however, was that we were able to replicate only one CpG annotated to genes involved in the RAAS, namely cg12841684 annotated to the NR3C2 gene, which encodes for the mineralocorticoid receptor mediating the actions of aldosterone on salt and water balance [31]. Previous findings from animal studies have shown the impact of salt intake, hypertension, and proinflammatory cytokines on methylation and expression of the AGT and CYP11B2 gene [32]. It could therefore be that the association between DNA methylation of RAAS genes and the aldosterone and renin concentration are masked in our study, because of the complex regulation of these concentrations by other factors like salt intake, serum potassium concentrations, and sympathetic nervous system activity, or because of the small sample size of this study (i.e. false negative findings).
Hypertension is more prevalent among SSA migrants in Europe compared to their non-migrating counterparts in SSA [2], and DNA methylation has been shown to differ between migrant and non-migrant populations [33]. However, the mean methylation levels for our DMPs associated with aldosterone, renin, and ARR did not differ between participants residing in rural and urban Ghana, and Ghanaian migrants in Amsterdam (Additional file 1: Table S3). This is noteworthy, as the median levels of renin seem to be lower in Amsterdam than in urban Ghana and rural Ghana, whereas aldosterone showed an opposite trend, being highest in Amsterdam and lowest in rural Ghana. This may suggest that other factors like BMI or BP impact renin and aldosterone more directly than DNA methylation does.
Hypertension in SSA origin populations is often characterised by suppressed renin and high ARR [29]. Fitting the EWAS for suppressed versus unsuppressed renin, and for high versus low ARR, classified based on median split of both distributions, showed the same DMPs that were epigenome-wide significant in the EWAS for continuous traits (data available on request). This supports the robustness of our findings and indicates that the association between renin concentration and ARR and DNA methylation is linear.
Strengths and limitations
This is the first EWAS on hormones of the RAAS and it was conducted in a genetically homogenous populations of Ghanaians, a SSA population with a high prevalence of hypertension. Data collection was highly standardised, allowing for high-quality data and comparison of populations residing in different locations.
Our study has some limitations. Firstly, as this was an explorative study, the sample size and study design were not based on specific statistical power to detect certain effect. However, the goal of this proof-of-principle study was to lay a foundation, which can lead to further research. Secondly, we used whole blood samples to assess DNA methylation associated with aldosterone and renin concentration. DNA methylation is tissue-specific, and even though renin and aldosterone are hormones that are secreted into the blood, it is possible that DNA methylation is different in the tissues where these hormones are produced and/or act, i.e. in the kidney and adrenal glands. The DNA methylation levels for our top DMPs, however, generally showed concordance between blood, kidney, and adrenal gland tissue [34]. Thirdly, it has been shown that renin’s precursor prorenin can be activated if samples are not frozen quickly after collection, or thawed slowly before analysis [35, 36]. This cryoactivation of prorenin could result in increased renin concentration. However, as samples were frozen quickly after collection, and were thawed according to standard operating procedures, the impact of activating prorenin is likely to be minimal. Fourthly, since our study lacks genetic profiles, we were not able to exclude participants from our study with an underlying genetic defect known to be associated with changes in RAAS, such as Liddle syndrome or familial hyperaldosteronism (37). However, as these syndromes are rare, we do not expect these to have substantially impacted our findings. Additionally, results from the gaphunter analysis did not indicate potential genetic variations underlying our significant DMPs. Lastly, as this study used cross-sectional data, inference on causality should be made with caution.
Perspectives
The findings of this proof-of-principle study suggest a role of DNA methylation in the regulation of plasma renin and aldosterone concentration, with a potential link to blood pressure and other CVD risk factors. This study can serve as a starting point to further elucidate the regulation of RAAS and the pathophysiology of (salt-sensitive) hypertension, and the complex gene-environment interaction affecting these mechanisms. Specifically, future research should include larger sample size, of different ethnic origins, and preferably of longitudinal study design, in order to replicate our findings, determine ethnic-specific differences, and establish causality in relation to incidence of hypertension and CVD risk. Ultimately, this information could inform targeted interventions aiming to reduce the burden of hypertension in general, and among SSA populations specifically.
Conclusions
In this first EWAS on renin and aldosterone concentrations in general, and specifically in a SSA population, we detected several epigenome-wide significant DMPs. Our results need to be replicated in large cohorts of different ethnic origins. Additionally, translational and longitudinal studies are needed to better understand the role of DNA methylation in the regulation of hormones of RAAS, thereby disentangling the pathophysiology of salt-sensitive hypertension in SSA populations.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
References
Agyemang C, Kieft S, Snijder MB, Beune EJ, van den Born BJ, Brewster LM, et al. Hypertension control in a large multi-ethnic cohort in Amsterdam, The Netherlands: the HELIUS study. Int J Cardiol. 2015;183:180–9.
Agyemang C, Nyaaba G, Beune E, Meeks K, Owusu-Dabo E, Addo J, et al. Variations in hypertension awareness, treatment, and control among Ghanaian migrants living in Amsterdam, Berlin, London, and nonmigrant Ghanaians living in rural and urban Ghana - the RODAM study. J Hypertens. 2018;36(1):169–77.
van den Born B, Agyemang C. Ethnicity and hypertension. In: Camm A, Lüscher T, Maured G, Serruys P, editors. ESC CardioMed, 3 ed. Oxford: Oxford University Press; 2018.
Elijovich F, Weinberger MH, Anderson CA, Appel LJ, Bursztyn M, Cook NR, et al. Salt sensitivity of blood pressure: a scientific statement from the American heart association. Hypertension. 2016;68(3):e7–46.
Elgazzaz M, Lazartigues E. Epigenetic modifications of the renin-angiotensin system in cardiometabolic diseases. Clin Sci (Lond). 2021;135(1):127–42.
Richardson SI, Freedman BI, Ellison DH, Rodriguez CJ. Salt sensitivity: a review with a focus on non-Hispanic blacks and Hispanics. J Am Soc Hypertens. 2013;7(2):170–9.
Brown JM, Robinson-Cohen C, Luque-Fernandez MA, Allison MA, Baudrand R, Ix JH, et al. The spectrum of subclinical primary aldosteronism and incident hypertension: a cohort study. Ann Intern Med. 2017;167(9):630–41.
Svetkey LP, McKeown SP, Wilson AF. Heritability of salt sensitivity in black Americans. Hypertension. 1996;28(5):854–8.
Balafa O, Kalaitzidis RG. Salt sensitivity and hypertension. J Hum Hypertens. 2021;35(3):184–92.
Cavalli G, Heard E. Advances in epigenetics link genetics to the environment and disease. Nature. 2019;571(7766):489–99.
Richard MA, Huan T, Ligthart S, Gondalia R, Jhun MA, Brody JA, et al. DNA methylation analysis identifies loci for blood pressure regulation. Am J Hum Genet. 2017;101(6):888–902.
Irvin MR, Jones AC, Claas SA, Arnett DK. DNA methylation and blood pressure phenotypes: a review of the literature. Am J Hypertens. 2021;34(3):267–73.
Wang F, Demura M, Cheng Y, Zhu A, Karashima S, Yoneda T, et al. Dynamic CCAAT/enhancer binding protein-associated changes of DNA methylation in the angiotensinogen gene. Hypertension. 2014;63(2):281–8.
Agyemang C, Beune E, Meeks K, Owusu-Dabo E, Agyei-Baffour P, Aikins A, et al. Rationale and cross-sectional study design of the research on obesity and type 2 diabetes among African migrants: the RODAM study. BMJ Open. 2014;4(3): e004877.
Meeks KAC, Henneman P, Venema A, Addo J, Bahendeka S, Burr T, et al. Epigenome-wide association study in whole blood on type 2 diabetes among sub-Saharan African individuals: findings from the RODAM study. Int J Epidemiol. 2019;48(1):58–70.
Chen YA, Lemire M, Choufani S, Butcher DT, Grafodatskaya D, Zanke BW, et al. Discovery of cross-reactive probes and polymorphic CpGs in the Illumina Infinium HumanMethylation450 microarray. Epigenetics. 2013;8(2):203–9.
Houseman EA, Accomando WP, Koestler DC, Christensen BC, Marsit CJ, Nelson HH, et al. DNA methylation arrays as surrogate measures of cell mixture distribution. BMC Bioinformatics. 2012;13:86.
van Iterson M, van Zwet EW, Consortium B, Heijmans BT. Controlling bias and inflation in epigenome- and transcriptome-wide association studies using the empirical null distribution. Genome Biol. 2017;18(1):19.
Li M, Zou D, Li Z, Gao R, Sang J, Zhang Y, et al. EWAS atlas: a curated knowledgebase of epigenome-wide association studies. Nucleic Acids Res. 2019;47(D1):D983–8.
Schlosser P, Tin A, Matias-Garcia PR, Thio CHL, Joehanes R, Liu H, et al. Meta-analyses identify DNA methylation associated with kidney function and damage. Nat Commun. 2021;12(1):7174.
Nehme A, Cerutti C, Dhaouadi N, Gustin MP, Courand PY, Zibara K, et al. Atlas of tissue renin-angiotensin-aldosterone system in human: a transcriptomic meta-analysis. Sci Rep. 2015;5:10035.
Komaki S, Shiwa Y, Furukawa R, Hachiya T, Ohmomo H, Otomo R, et al. iMETHYL: an integrative database of human DNA methylation, gene expression, and genomic variation. Hum Genome Var. 2018;5:18008.
Chitrala KN, Hernandez DG, Nalls MA, Mode NA, Zonderman AB, Ezike N, et al. Race-specific alterations in DNA methylation among middle-aged African Americans and whites with metabolic syndrome. Epigenetics. 2020;15(5):462–82.
Istas G, Declerck K, Pudenz M, Szic KSV, Lendinez-Tortajada V, Leon-Latre M, et al. Identification of differentially methylated BRCA1 and CRISP2 DNA regions as blood surrogate markers for cardiovascular disease. Sci Rep. 2017;7(1):5120.
KCNT1 Gene - potassium sodium-activated channel subfamily T member 1: GeneCardsSuite, Weizmann Institute of Science; [Available from: https://www.genecards.org/cgi-bin/carddisp.pl?gene=KCNT1.
Rzehak P, Covic M, Saffery R, Reischl E, Wahl S, Grote V, et al. DNA-methylation and body composition in preschool children: epigenome-wide-analysis in the European childhood obesity project (CHOP)-Study. Sci Rep. 2017;7(1):14349.
Al Muftah WA, Al-Shafai M, Zaghlool SB, Visconti A, Tsai PC, Kumar P, et al. Epigenetic associations of type 2 diabetes and BMI in an Arab population. Clin Epigenetics. 2016;8:13.
Sharma NK, Langberg KA, Mondal AK, Das SK. Phospholipid biosynthesis genes and susceptibility to obesity: analysis of expression and polymorphisms. PLoS ONE. 2013;8(5): e65303.
Braun PR, Tanaka-Sahker M, Chan AC, Jellison SS, Klisares MJ, Hing BW, et al. Genome-wide DNA methylation investigation of glucocorticoid exposure within buccal samples. Psychiatry Clin Neurosci. 2019;73(6):323–30.
Meeks KAC, Henneman P, Venema A, Burr T, Galbete C, Danquah I, et al. An epigenome-wide association study in whole blood of measures of adiposity among Ghanaians: the RODAM study. Clin Epigenetics. 2017;9:103.
Bauersachs J, Lopez-Andres N. Mineralocorticoid receptor in cardiovascular diseases-Clinical trials and mechanistic insights. Br J Pharmacol. 2022;179(13):3119-34.
Takeda Y, Demura M, Yoneda T, Takeda Y. DNA methylation of the angiotensinogen gene, AGT, and the aldosterone synthase gene, CYP11B2 in cardiovascular diseases. Int J Mol Sci. 2021;22(9):4587.
Chilunga FP, Henneman P, Venema A, Meeks KA, Gonzalez JR, Ruiz-Arenas C, et al. DNA methylation as the link between migration and the major noncommunicable diseases: the RODAM study. Epigenomics. 2021;13(9):653–66.
Xiong Z, Yang F, Li M, Ma Y, Zhao W, Wang G, et al. EWAS open platform: integrated data, knowledge and toolkit for epigenome-wide association study. Nucleic Acids Res. 2022;50(D1):D1004–9.
Sealey JE, Moon C, Laragh JH, Alderman M. Plasma prorenin: cryoactivation and relationship to renin substrate in normal subjects. Am J Med. 1976;61(5):731–8.
Schalekamp MA, Derkx FH, Deinum J, Danser AJ. Newly developed renin and prorenin assays and the clinical evaluation of renin inhibitors. J Hypertens. 2008;26(5):928–37.
Raina R, Krishnappa V, Das A, Amin H, Radhakrishnan Y, Nair NR, et al. Overview of monogenic or mendelian forms of hypertension. Front Pediatr. 2019;7:263.
Acknowledgements
The authors are very grateful to the advisory board members for their valuable support in shaping the methods, to the research assistants, interviewers and other staff of the five research sites, who have taken part in gathering the data and, most of all, to the Ghanaian volunteers participating in this project. We gratefully acknowledge Jan van Straalen from the Academic Medical Centre for his valuable support with standardisation of the laboratory procedures and the AMC Biobank for support in biobank management and storage of collected samples.
Funding
The current work was supported by the European Commission under the Framework Programme (grant number: 278901) and European Research Council (grant number: 772244). K.A.C.M. is supported by the Intramural Research Program of the National Institutes of Health in the Center for Research on Genomics and Global Health (CRGGH). The CRGGH is supported by the National Human Genome Research Institute, the National Institute of Diabetes and Digestive and Kidney Diseases, the Center for Information Technology, and the Office of the Director at the National Institutes of Health (1ZIAHG200362). The study funder had no role in the study design, data collection, data analysis, data interpretation or writing of the report. The corresponding author had full access to all the data and the final responsibility to submit for publication.
Author information
Authors and Affiliations
Contributions
E.L.L., A.H., P.H., B.J.B., and C.A. conceived the study. C.A. and K.M. designed and carried out the recruitment and data collection. E.L.L., A.H., and P.H. were responsible for data analysis and E.L.L., A.H., P.H., B.J.B., and C.A. for the interpretation. E.L.L. wrote the article, in collaboration with A.H., supervised by P.H., B.J.B., and C.A., and in cooperation with all co-authors. All authors read and approved the final version of the article. E.L.L. had full access to all the data in the study and takes responsibility for its integrity and the data analysis. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Before the start of data collection, ethical approval was obtained from the respective ethics committees of the involved institutions in Ghana (School of Medical Sciences/Komfo Anokye Teaching Hospital Committee on Human Research, Publication & Ethical Review Board), UK (London School of Hygiene and Tropical Medicine Research Ethics Committee), the Netherlands (Institutional Review Board of the Academic Medical Center, University of Amsterdam), and Germany (Ethics Committee of Charité-Universitätsmedizin Berlin). All participants provided written informed consent before enrolment in the study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1:
Table S1 Relationship between DNA methylation of differentially methylated positions and gene expression as reported in the iMEHTYL database. Table S2 Enrichment analysis for the top 20 pathways associated with renin, aldosterone and ARR. Table S3 Median methylation beta levels of differentially methylated positions, stratified by geographical location of residence. Fig. S1. Participants inclusion flow chart. Fig. S2 QQ plots of bacon adjusted p-values for renin, aldosterone and ARR population. Fig. S3 Differentially methylated region (DMR) annotated to chromosome 6 (NFYA) associated with renin concentration. Fig. S4 Differentially methylated region (DMR) annotated to chromosome 6 (RNF39) associated with renin concentration. Fig. S5 Differentially methylated region (DMR) annotated to chromosome 6 (HLA-DRB1) associated with aldosterone concentration.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
van der Linden, E.L., Halley, A., Meeks, K.A.C. et al. An explorative epigenome-wide association study of plasma renin and aldosterone concentration in a Ghanaian population: the RODAM study. Clin Epigenet 14, 159 (2022). https://doi.org/10.1186/s13148-022-01378-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13148-022-01378-5