
Abstract
Background
The novel long noncoding RNA MEF2C-AS1 has been identified to play suppressor roles during tumorigenesis. DNA methylation has a regulatory effect on gene expression in cancer initiation and progression. However, the methylation status of MEF2C-AS1 and its role in colorectal cancer (CRC) development remain unclear.
Methods
The expression and methylation levels of MEF2C-AS1 were systematically analyzed among 31 cancers with available qualified data in GEPIA and UCSC Xena databases. Then, the MEF2C-AS1 methylation status was firstly examined among 12 CRCs by Illumina Infinium MethylationEPIC BeadChip in in-house step 1 and further quantified among 48 CRCs by the MassARRAY method in in-house step 2. Subsequently, its methylation and expression levels were quantified among 81 non-advanced adenomas (NAAs), 81 advanced adenomas (AAs), and 286 CRCs using the MassARRAY method, and among 34 NAAs, 45 AAs, and 75 CRCs by qRT-PCR, in in-house step 3, respectively. The effect of MEF2C-AS1 methylation on CRC survival was analyzed by the Kaplan–Meier method. Additionally, in vitro cell proliferation, migration and invasion assays, and bioinformatics analysis were performed to explore the role of MEF2C-AS1 in colorectal carcinogenesis.
Results
Lower expression and higher methylation of MEF2C-AS1 were found in CRC by online databases. In the comparisons of lesion tissues with adjacent normal tissues, MEF2C-AS1 hypermethylation of each individual site and mean level was found among CRC patients in in-house step 1 and step 2, more meaningfully, among NAA patients, AA patients, and CRC patients at all stages during colorectal carcinogenesis in in-house step 3 (all p < 0.05). Further comparisons demonstrated significant differences between CRC and NAA (p = 0.025), AA and NAA (p = 0.020). Moreover, MEF2C-AS1 hypermethylation was associated with poorer disease-specific survival of CRC patients (p = 0.044). In addition, hypermethylation and lower expression of MEF2C-AS1 were verified in RKO cells, and the MEF2C-AS1 overexpression significantly suppressed RKO cell proliferation, migration, and invasion.
Conclusions
The findings reveal that MEF2C-AS1 hypermethylation might be an early driven event during colorectal carcinogenesis. It might serve as a promising prognostic biomarker for CRC survival. Our study also indicates the potential tumor-suppressing role of MEF2C-AS1 in CRC.
Similar content being viewed by others


Background
Colorectal cancer (CRC) is the third most commonly diagnosed malignancy and the second leading cause of cancer death worldwide [1]. Most sporadic CRCs are recognized to develop from colorectal adenomas following the adenoma–carcinoma sequence [2]. In the complex multi-step process of colorectal carcinogenesis and progression, environmental factors, genetic factors, and epigenetic factors play important roles in composing a regulatory network involving many molecules [3,4,5].
Long noncoding RNAs (lncRNAs) are defined as transcripts of more than 200 nucleotides that are not translated into proteins except for functional small peptides [6]. Nowadays, these transcripts are involved in various diseases related to biological behaviors such as cell proliferation, differentiation, and migration [7,8,9], and their aberrant expression is significantly associated with the initiation and development of cancers [10]. For instance, an oncogenic lncRNA BLACAT1 was reported in osteosarcoma (OS) [11], pancreatic cancer (PC) [12], breast cancer (BC) [13], and CRC [14]. The elevated expression of BLACAT1 was detected in lesion tissues and was associated with poor prognosis of patients with cervical squamous cell carcinoma (CSCC) [15] and CRC [14]. Until now, plenty of functional lncRNAs have been characterized and they might regulate target mRNAs expression through the competitive endogenous RNA (ceRNA) mechanism mediated by miRNAs [16]. Nevertheless, the potential molecules participating in the specific regulatory network need to be further explored.
Aberrant DNA methylation, expressed as the hypermethylation or hypomethylation of cytosine–guanine dinucleotide (CpG), has been proved to be one of the most important factors in regulating gene expression at the pretranscriptional level in human cancers [17, 18]. Specifically, tumor suppressor genes could be inhibited by their promoter hypermethylation and could be reactivated after demethylation; on the contrary, oncogenes might be activated by its hypomethylation [19,20,21,22,23]. For instance, hypermethylation and downregulation of lncRNA LINC00472 were identified in CRC tissues as compared with adjacent normal tissues, and its hypermethylation might serve as a potential CRC diagnostic biomarker [24]. Recently, studies have revealed that methylation alteration could be detected at the early stages of colorectal carcinogenesis [25, 26]. Fan J et al. [26] found that aberrant hypermethylation of ADHFE1 promoter had maintained throughout the low-grade adenoma and high-grade adenoma which were associated with colorectal adenoma development. However, the number of lncRNAs that have been reported to show aberrant methylation status during carcinogenesis was still limited.
A novel lncRNA gene MEF2C antisense RNA 1 (MEF2C-AS1), located at 5q14.3, has been identified to be downregulated and to play tumor suppressor roles in diffuse gastric cancer (DGC), cervical cancer (CC), and BC by inhibiting cell proliferation and aggressive tumor phenotypes [27,28,29]. However, the role of MEF2C-AS1 in CRC development has not been investigated. Hence, this study aimed to clarify the MEF2C-AS1 methylation status and its functional role during colorectal carcinogenesis. Firstly, we systematically analyzed MEF2C-AS1 methylation and expression levels by online databases. Then, we validated the findings in our CRCs, and further among our additional non-advanced adenomas (NAAs), advanced adenomas (AAs), and CRCs to assess the MEF2C-AS1 methylation status and expression changes at all stages of colorectal carcinogenesis. Furthermore, we examined the effect of MEF2C-AS1 methylation on disease-specific survival (DSS) of CRC patients. Lastly, in vitro assays and bioinformatics analysis were performed to confirm the influence of MEF2C-AS1 methylation on its expression and explore the role of MEF2C-AS1 in colorectal carcinogenesis.
Results
The expression and DNA methylation status of MEF2C-AS1 in various cancers by online databases
MEF2C-AS1 expression levels were compared between lesion tissues and normal tissues among 31 cancers with available RNA sequencing (RNA-Seq) data in the GEPIA database. Its expression levels were found to be significantly higher in lymphoid neoplasm diffuse large B cell lymphoma (DLBC), significantly lower in bladder urothelial carcinoma (BLCA), breast invasive carcinoma (BRCA), cervical squamous cell carcinoma and endocervical adenocarcinoma (CESC), ovarian serous cystadenocarcinoma (OV), testicular germ cell tumors (TGCT), uterine corpus endometrial carcinoma (UCEC), uterine carcinosarcoma (UCS), colon adenocarcinoma (COAD), and rectum adenocarcinoma (READ), but not significantly different in remaining 21 cancers, in the comparisons of lesion tissues and corresponding normal tissues (Fig. 1, Additional file 1: Fig. S1). To explore the relationship of MEF2C-AS1 expression with its methylation, methylation levels were further compared between lesion tissues and normal tissues among 31 cancers if there were qualified methylation data from the UCSC Xena database. Among 10 cancers with differential MEF2C-AS1 expression, higher methylation levels were found in lesion tissues of BLCA, BRCA, CESC, UCEC, COAD, and READ with available data (Fig. 2) compared with normal tissues, and comparisons of the remaining 21 cancers are presented in Additional file 1: Fig. S2. It is suggested that MEF2C-AS1 might be downregulated and hypermethylated in CRC, which was further confirmed in the following study in consideration of sample availability.

Differential MEF2C-AS1 expression between lesion tissues and normal tissues among 10 cancers in the GEPIA database. Every dot represents the expression level for a tissue sample. Box plot in red or gray represents the distribution of expression level. Expression level is presented in log2(TPM + 1) scale. TPM: transcripts per million. *p < 0.05

MEF2C-AS1 hypermethylation among 10 cancers with differential expression in the UCSC Xena database. Violin plot in blue or orange represents the distribution of methylation level. *p < 0.05
Primary comparison of MEF2C-AS1 methylation status in in-house colorectal cancers
To clarify the methylation status of MEF2C-AS1 in our samples, we quantified its promoter methylation levels among 12 CRC patients in in-house step 1 using Illumina MethylationEPIC BeadChip (850 K array). Specifically, the methylation levels of all 6 individual sites were found to be significantly higher in lesion tissues than those in adjacent normal tissues, and a similar difference was also observed in the comparison of their mean levels (Table 1, all p < 0.01).
Further validation of MEF2C-AS1 hypermethylation in in-house colorectal cancers
The methylation status of MEF2C-AS1 was reconfirmed among our additional 48 CRC patients in in-house step 2. By the MassARRAY method, methylation levels of 18 CpG sites were successfully detected and were then included in the subsequent analysis. As shown in Fig. 3a, all individual CpG sites were observed to be significantly hypermethylated in lesion tissues compared with adjacent normal tissues (all p < 0.001). The mean level of MEF2C-AS1 methylation of lesion tissues was 0.25, which was remarkably higher than 0.04 of adjacent normal tissues (Fig. 3b, p < 0.001). MEF2C-AS1 hypermethylation frequently happened in 91.67% (44/48) of CRC patients (Fig. 3c).

MEF2C-AS1 hypermethylation among CRC patients in in-house step 2. a Methylation level of each individual CpG site. b Mean methylation level of all individual CpG sites. c Percentage of patients with hypermethylation or hypomethylation status. ***p < 0.001
Elucidation of MEF2C-AS1 hypermethylation in in-house patients at all stages of colorectal carcinogenesis
In in-house step 3, we ulteriorly quantified MEF2C-AS1 methylation levels among 81 NAA, 81 AA, and 286 CRC patients by the MassARRAY method to elucidate its methylation status at all stages of colorectal carcinogenesis. In total, methylation levels were successfully measured for both lesion tissues and adjacent normal tissues in 80 NAAs, 79 AAs, and 283 CRCs. As expected, higher MEF2C-AS1 methylation levels of individual CpG sites and mean levels were observed in lesion tissues of NAA (Fig. 4a, all p < 0.05), AA (Fig. 4b, all p < 0.001), and CRC (Fig. 4c, all p < 0.001) as compared with adjacent normal tissues, respectively. Compared with their adjacent normal tissues, the percentage of higher MEF2C-AS1 methylation increased from 76.25% (61/80) of NAAs, to 84.81% (67/79) of AAs, and to 89.05% (252/283) of CRCs (Fig. 4).

MEF2C-AS1 hypermethylation among patients at all stages during colorectal carcinogenesis in in-house step 3. a NAA patients. b AA patients. c CRC patients. Line chart presents the methylation level of each individual CpG site. The distribution of the mean methylation level of all individual CpG sites is shown in the scatter plot. Pie chart presents the percentage of patients with hypermethylation or hypomethylation status. AA, advanced adenoma; CRC, colorectal cancer; NAA, non-advanced adenoma. ***p < 0.001
Further comparisons of methylation in lesion tissues among patients are presented in Table 2. Interestingly, in most individual sites, significant differences were found between CRC and NAA, AA and NAA, but not between CRC and AA. The mean levels of MEF2C-AS1 methylation in NAA, AA, and CRC tissues were 0.19, 0.28, and 0.25, respectively. Similarly, there were significant differences in comparisons of CRC with NAA (p = 0.025), AA with NAA (p = 0.020), but not in CRC with AA (p = 1.000).
Confirmation of low MEF2C-AS1 expression in in-house patients at all stages of colorectal carcinogenesis
To confirm the potential influence of MEF2C-AS1 methylation on its expression, expression levels, detected by quantitative reverse transcription-polymerase chain reaction (qRT-PCR), were then compared between lesion tissues and adjacent normal tissues among 34 NAAs, 45 AAs, and 75 CRCs in in-house step 3. Significantly lower MEF2C-AS1 expression was found in the comparisons of lesion tissues versus adjacent normal tissues of NAA patients (Fig. 5a, p = 0.002), AA patients (Fig. 5b, p < 0.001), and CRC patients (Fig. 5c, p < 0.001). However, additional comparisons of expression levels between lesion tissues showed significant lower expression as CRC compared with NAA (p < 0.001), but not as CRC compared with AA (p = 0.122), AA compared with NAA (p = 0.085).

MEF2C-AS1 expression among patients at all stages during colorectal carcinogenesis in in-house step 3. a NAA patients. b AA patients. c CRC patients. Each scatter in blue or red represents the expression level for a tissue sample. AA, advanced adenoma; CRC, colorectal cancer; NAA, non-advanced adenoma
Effect of MEF2C-AS1 methylation on disease-specific survival of colorectal cancer patients
Moreover, survival analysis was performed for CRC patients to examine the prognostic effect of the methylation. Among 285 CRC patients who successfully detected methylation status, 49 patients died of CRC during a median of 3.8 years of follow-up. The mean level of MEF2C-AS1 methylation was negatively associated with DSS of CRC patients, indicating that patients with higher methylation had poorer survival than those with lower methylation (Fig. 6a, log-rank p = 0.044). In stratified and subgroup analyses, significant associations between MEF2C-AS1 hypermethylation and poor DSS were observed in patients who were less than 60 years, female, and patients with rectum cancer or high differentiation cancer, and the associations were similar in patients with different stages (Fig. 6b–f).

Survival analysis on CRC patients in in-house step 3. Kaplan–Meier method and log-rank test were used to compare DSS between CRC patients with high methylation and those with low methylation. a All CRC patients. Stratified and subgroup analyses were performed between the groups stratified by b age, c gender, d tumor location, e TNM stage, and f differentiation. CRC, colorectal cancer; DSS, disease-specific survival
Influence of MEF2C-AS1 methylation on its expression in colorectal cancer cells
Based on the above findings of MEF2C-AS1 methylation and expression in tissues, we further evaluated whether the expression of MEF2C-AS1 was regulated by its aberrant promoter methylation in vitro. As shown in Fig. 7a, the decreased expression of MEF2C-AS1 was found in all three CRC cell lines, HT29, RKO, and SW480, compared with normal colonic cell line FHC (all p < 0.05). After demethylation treatment with different concentrations of 5-aza-2'-deoxycytidine (5-Aza-dC) to the CRC cell line with moderate MEF2C-AS1 downregulation, RKO cell line, its expression was significantly rescued in the 15 and 20 µM groups compared with the 0 µM group, and the effect showed a dose-dependent manner (Fig. 7b, all p < 0.05).

MEF2C-AS1 expression levels in different cell lines and its functional role in cell proliferation, migration, and invasion in CRC cells. a The difference of MEF2C-AS1 expression between normal colonic cell line and CRC cell lines. b MEF2C-AS1 expression in RKO cells treated with different concentrations of demethylation agent 5-Aza-dC. c Transfection efficiency of MEF2C-AS1 overexpression plasmid in RKO cells. The cells in the control group are treated with empty vectors. d Cell viability assay. e Wound healing assay. f Transwell migration assay. g Transwell invasion assay. 5-Aza-dC, 5-aza-2’-deoxycytidine; CRC, colorectal cancer. ***p < 0.001, **p < 0.01, *p < 0.05, ns p > 0.05
Function of MEF2C-AS1 on colorectal cancer cell proliferation, migration, and invasion
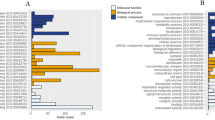
To determine the potential role of MEF2C-AS1 in CRC, we performed several assays in RKO cells. Compared to cells transfected with an empty pLV3 vector, MEF2C-AS1 expression levels significantly increased in cells transfected with a pLV3-MEF2C-AS1 plasmid (Fig. 7c). And cell proliferation was significantly inhibited in cells with MEF2C-AS1 overexpression (Fig. 7d). Wound healing and transwell assays showed that MEF2C-AS1 overexpression significantly reduced cell migration and invasion capacities (Fig. 7e–g) (all p < 0.05). To further explore the potential regulatory pathway, the putative target miRNAs and mRNAs of MEF2C-AS1 were predicted by bioinformatics analysis using public databases. The comprehensive bioinformatics analysis showed that low expression of MEF2C-AS1 in CRC might lead to downregulation of 10 target mRNAs including KCNB1, CFL2, FAM129A, CLIP4, CYBRD1, SLC16A9, TMEM100, BVES, TRPM6, and ZEB1 through upregulating 3 miRNAs, hsa-miR-17-5p, hsa-miR-24-3p, and hsa-miR-429 (Additional file 1: Table S1).
Discussion
Aberrant DNA methylation of functional lncRNAs has been widely reported in carcinogenesis and progression of CRC; however, the methylation status of MEF2C-AS1 and its role remains unclear. In this study, we performed a comprehensive analysis of MEF2C-AS1 methylation status and its expression changes in comparisons of lesion tissues and normal tissues among patients during colorectal carcinogenesis. Firstly, we found high methylation and low expression of MEF2C-AS1 in CRC tissues by online public databases. Then, the MEF2C-AS1 hypermethylation and downregulation were found among our patients at all stages of colorectal carcinogenesis as early as in NAAs, and significant differences in methylation levels in lesion tissues were found between AAs and NAAs, CRCs and NAAs. Moreover, patients with MEF2C-AS1 hypermethylation were found to be more likely to suffer CRC-specific death. Lastly, we confirmed the reduction of MEF2C-AS1 expression caused by its promoter hypermethylation and also found that its overexpression could suppress proliferation, migration, and invasion in CRC cells.
It is noteworthy that promoter methylation plays an important regulatory role in gene expression [30,31,32]. Although previous studies have reported that MEF2C-AS1 was downregulated in DGC [27] and CC [28] lesion tissues, and BC [29] cells, the current study is the first that systematically described the MEF2C-AS1 methylation status and its influence on expression. Hypermethylation and lower expression were found in 6 cancers including BLCA, BRCA, CESC, UCEC, COAD, and READ. However, for the other 4 cancers including DLBC, OV, TGCT, and UCS, though lower expression levels were found in the comparisons of lesion tissues versus normal tissues, its methylation change and correlation between methylation and expression could not be examined due to the unavailability of methylation data of normal tissues. Further exploration might be performed in future studies.
Promoter hypermethylation is identified to play an important role during tumorigenesis through silencing the gene expression of tumor suppressor genes [33, 34]. Based on a genome-wide screening performed by Li Y et al., aberrant hypermethylation of α-internexin gene promoter was identified in both colon adenoma and cancer, and the findings were validated in biospecimens of 30 normal colons, 37 adenomas, and 30 colon cancers using quantitative methylation-specific PCR, and the silenced α-internexin expression by epigenetic alteration was confirmed in CRC cells [35]. Using 450 K data and RNA-Seq expression data in public databases, we found the higher methylation and lower expression of MEF2C-AS1 in the comparisons of colon and rectum adenocarcinoma lesion tissues versus normal tissues. Then, the study was extended to our in-house samples, and we further validated the hypermethylation of MEF2C-AS1 promoter in CRC and its precursor lesions step-by-step, followed by corresponding downregulation of MEF2C-AS1. Additional demethylation assay verified the regulatory role of promoter hypermethylation of MEF2C-AS1 on its expression in vitro. Taken together, our results demonstrated that MEF2C-AS1 hypermethylation might be an early driven event during colorectal carcinogenesis.
Colorectal adenoma could be divided into NAA and AA according to the histology clinically, and AA has more advanced features than NAA. The detection and treatment of AA were important for the early prevention of CRC [36]. At present, there are few studies revealing the differences between AA and NAA at the epigenetic level. Our identification that the hypermethylation of MEF2C-AS1 occurred in colorectal lesions at all stages of colorectal carcinogenesis provided the potential application possibility for this methylation marker in early cancer detection. Furthermore, significant differences in methylation of lesion tissues were found between AAs and NAAs, CRCs and NAAs, but not between CRCs and AAs, indicating the inheritance and development of epigenetic alteration from NAA, to AA, and to CRC. Meanwhile, differences in expression levels were found in the comparison of CRCs and NAAs. Collectively, our findings provide epigenetic evidence for the potential of being an effective biomarker which might be applied in early diagnosis and treatment practice to detect advanced neoplasia including AA and CRC.
The prognostic significance of hypermethylated lncRNA genes has been well proved in various human cancers. For instance, promoter hypermethylation of the lncRNA PLUT was significantly associated with shorter relapse-free survival of lung adenocarcinoma [37], and hypermethylated ZNF667-AS1 was correlated with ESCC patients’ survival [38]. In our study, a reverse association was found between hypermethylation of MEF2C-AS1 and DSS in CRC patients, revealing the value in developing predictive prognostic models integrating molecular biomarkers with age, TNM stage, or other clinical characteristics [39]. Mechanically, the impact of MEF2C-AS1 methylation on DSS might be explained by its posttranscriptional regulatory role through a competing endogenous RNA network or cis-activating transcription of near coding genes [40, 41]. In general, our findings suggest the potential that MEF2C-AS1 hypermethylation might act as a predictor of CRC prognosis.
The tumor suppressor role of MEF2C-AS1 expression in cancer initiation and progression has been reported in several cancers. Briefly, knock-down of MEF2C-AS1 promoted aggressive tumor behaviors by reducing the protein levels of FAT3, NTN1, and LYVE1 which were related to proliferation and invasion in GC cell lines [27]. Wang X et al. [28] have found that MEF2C-AS1 played a suppressor role in CC via suppressing miR-592 by targeting RSPO1. Similarly, MEF2C-AS1 was reported to inhibit proliferation, migration, and invasion of BC cells by targeting miR-3646 downregulation which might be related to the inhibition of CDK1 and MMP-2 protein expression [29]. In our study, we observed that MEF2C-AS1 overexpression significantly inhibited cell proliferation, migration, and invasion of RKO cells, revealing its potential tumor-suppressing role in colorectal carcinogenesis. Further comprehensive bioinformatics analysis revealed that 3 miRNAs were upregulated by MEF2C-AS1 downregulation, resulting in the downregulation of 10 mRNAs in CRC. Among them, hsa-miR-429 has been proved to act as an important oncogenic miRNA and be involved in the regulation of several cellular processes contributing to the progression and metastasis of CRC via targeting SOX2 [42]. The underlying mechanism of whether MEF2C-AS1 suppresses cell proliferation, migration, and invasion through the ceRNA regulatory pathway needs future exploration.
Our study has several advantages. The consistency of our results and those from online databases could summarize the stability and repeatability of MEF2C-AS1 hypermethylation status in CRC. Comprehensive analysis of MEF2C-AS1 methylation status along with expression changes in patients at all stages of colorectal carcinogenesis presents a great value in the CRC etiology at the epigenetic level. This study also has a few limitations. Firstly, the number of patients with colorectal adenoma was limited in the confirmation step. Secondly, samples used for methylation assessment were local tissues in this study. Evidence among other samples like blood and stool might further provide supplementary confirmation for our results. Lastly, the underlying molecular mechanism of hypermethylated MEF2C-AS1 during CRC development was not fully elucidated, and in vivo and in vitro experiments are necessary for further study.
Conclusions
In summary, this is the first study to explore the methylation status of MEF2C-AS1 and its expression in patients at all stages during colorectal carcinogenesis, revealing promoter hypermethylation and low expression in lesion tissues when compared with adjacent normal tissues. The findings reveal that hypermethylation of MEF2C-AS1 promoter might be an early driven event increasing sequentially in the process of malignant transformation from non-advanced adenoma, to advanced adenoma, and to carcinoma. It is suggested that MEF2C-AS1 hypermethylation might serve as a promising prognostic biomarker for CRC survival. Moreover, our study also confirms the tumor-suppressing role of MEF2C-AS1 in colorectal carcinogenesis.
Materials and methods
Study design
Figure 8 shows the overall flowchart of this study. Firstly, we systematically analyzed the MEF2C-AS1 expression and methylation status among 31 cancer types using available data based on the GEPIA and UCSC Xena databases. Then, three independent steps were conducted in our in-house samples. In in-house step 1, the methylation status of MEF2C-AS1 promoter was primarily compared between lesion tissues and adjacent normal tissues using 850 K array scan data from 12 CRCs. In in-house step 2, the MEF2C-AS1 methylation status was further measured among additional 48 CRCs using the MassARRAY method to technically validate the above array-based findings. In in-house step 3, to clarify the methylation status and corresponding expression changes of MEF2C-AS1 among patients at all stages during colorectal carcinogenesis, its methylation levels were further elucidated in a larger sample including additional 81 NAAs, 81 AAs, and 286 CRCs also using the MassARRAY method, and its expression levels were confirmed among 34 NAAs, 45 AAs, and 75 CRCs using qRT-PCR. Furthermore, survival analysis was performed in 286 CRCs by the Kaplan–Meier method. In addition, a demethylation assay was used to assess the influence of MEF2C-AS1 methylation on its expression in CRC cells. And cell proliferation, wound healing and transwell assays in vitro and bioinformatics analysis were performed to evaluate the functional role of MEF2C-AS1 in colorectal carcinogenesis.

Overall flowchart of the current study. AA, advanced adenoma; CRC, colorectal cancer; NAA, non-advanced adenoma; qRT-PCR, quantitative reverse transcription-polymerase chain reaction
Patients and samples
The basic characteristics of our own patients are presented in Table 3. CRC patients were collected from Shaoxing People's Hospital between January 2015 and July 2018. Patients with colorectal adenoma have been enrolled from a large-scale population-based screening program for early detection and treatment of colorectal cancer in Jiashan County, Zhejiang Province, China [43]. All patients were ethnic Han Chinese from Zhejiang Province and pathologically confirmed, with no familial adenomatous polyposis (FAP), no previous history of CRC, and none had received any preoperative anticancer treatment. All CRC patients were histologically confirmed with adenocarcinoma. For colorectal adenoma, AA is defined as adenoma ≥ 10 mm in diameter, and/or with high-grade dysplasia or villous or tubulovillous histology, and NAA is defined as adenoma < 10 mm without advanced histology according to guidelines [44]. For each patient, both lesion tissue and adjacent normal tissue at a distance of at least 5 cm away were taken simultaneously through surgery or colonoscopy. Information on characteristics including age, gender, tumor location, TNM stage [45], and pathological differentiation was also obtained. Patients who participated in the study signed informed consents, and the study was approved by the Medical Ethics Committee of Zhejiang University School of Medicine.
Cell culture and treatment
The normal colonic epithelial cell line FHC was cultured in DMEM/F12 medium, and the CRC cell lines HT29, RKO, and SW480 were also cultured in DMEM medium. All the mediums were supplemented with 1% antibiotics and 10% fetal bovine serum (FBS). All cells were cultured in a thermostatic incubator with 5% CO2 at 37 °C. For the demethylation assay, the CRC cells (5 × 105/well) were treated with different concentrations (0, 10, 15, 20 µM) of demethylation agent 5-Aza-dC (AdooQ Bioscience, USA) for 24 h. The MEF2C-AS1 expression levels in different cell lines were measured by qRT-PCR.
Online database
GEPIA (http://gepia.cancer-pku.cn/) [46] is a newly developed interactive web server for analyzing the RNA-Seq expression data of 9,736 tumor and 8,587 normal samples of 33 cancer types from the TCGA and the Genotype-Tissue Expression (GTEx) projects. The expression data of MEF2C-AS1 were presented on the scale of log2(TPM + 1).
DNA methylation data of 33 cancers, measured experimentally using the Illumina Infinium HumanMethylation450 BeadChip (450 K array), were downloaded from the UCSC Xena database (https://xena.ucsc.edu/) [47]. DNA methylation values, described as beta values (β), are continuous variables between 0 and 1, representing the ratio of the intensity of the methylated bead type to the combined locus intensity. Four CpG sites (cg04694437, cg10571951, cg12621171, and cg18109838) were identified in MEF2C-AS1 promoter, and their mean level was considered as its methylation.
Genome-wide DNA extraction and bisulfite conversion
Genomic DNA was extracted from fresh-frozen tissue samples using the DNA Tissue Kit (TianLong Biotech, Xi’an, China), and the concentration and purity of DNA were measured using NanoDrop 2000 spectrophotometer (Thermo Scientific, Wilmington, DE, USA) following the manufacturer’s instructions. The EZ Methylation Gold Kit (Zymo Research, Irvine, CA, USA) was used to conduct bisulfite treatment on genomic DNA (500 ng).
DNA methylation assessment
MEF2C-AS1 methylation status of 12 pairs of lesion tissues and adjacent normal tissues of CRC patients were assessed using 850 K array as previously described [48]. Six CpG sites (cg04694437, cg08966485, cg15297153, cg10571951, cg12621171, and cg18109838) in the MEF2C-AS1 promoter were identified according to the annotation mapped against the human reference version GRCh37/hg19. The mean level of six CpG sites was considered as the methylation level of MEF2C-AS1.
The validation of MEF2C-AS1 methylation was performed on the Sequenom MassARRAY platform (Sequenom, San Diego, CA, USA). The primers (forward: 5’-aggaagagagAGTAGGAGGTAGGTTTTGGGTTTTT-3’; reverse: 5’-cagtaatacgactcactatagggagaaggctCCCTCTTACTCTCCCAAATTTACA-3’) were designed using EpiDesigner (http://epidesigner.com). The tested sequence (chr5:88,185,329–88,185,810, GRCh37/hg19) contained 26 CpG sites, and sites outside of the mass spectrometry analytical window were filtered out of the methylation measurement (Additional file 1: Fig. S3). The MassARRAY Compact MALDI-TOF system (Sequenom, BioMiao Biological Technology, Beijing, China) was used to collect the mass spectra, and the methylation proportions were generated by EpiTYPER software (Sequenom, San Diego, CA). Methylation level was expressed as beta value (β), which was the ratio of methylated intensity to the sum of methylated intensity and unmethylated intensity with a range from 0 (completely unmethylated) to 1 (completely methylated). Samples and CpG sites with > 10% missing values were eliminated in the subsequent analysis. The mean level of all individual CpG sites was considered as the MEF2C-AS1 methylation level.
RNA isolation and qRT-PCR
Total RNA was extracted using TRIzol reagent (Invitrogen, Carlsbad, CA, USA) following the manufacturer’s instructions. The cDNA was synthesized from 1 µg of total RNA using Moloney Murine Leukemia Virus reverse transcriptase (Takara, Otsu, Shiga, Japan). The qRT-PCR was performed on LightCycler-480 system (Roche, Mannheim, Germany) with SYBR Green protocol. β-actin was used as an internal control. Relative expression levels were calculated by 2−ΔΔCT or 2−ΔCT method. The primer sequences were as follows: 5’-GTGGCCGAGGACTTTGATTG-3’ (forward) and 5’-CCTGTAACAACGCATCTCATATT-3’ (reverse) for β-actin, and 5’-GCTCCTAGGTATGGGTGGGA-3’ (forward) and 5’-TTTGTTGTGTGGTGCGACAG-3’ (reverse) for MEF2C-AS1.
Cell transfection
The pLV3 vector and pLV3-MEF2C-AS1 plasmid were constructed by Shanghai Hewu Biotechnology Co., Ltd. (Shanghai, China). The cells were cultured overnight and transfected by these two plasmids with the Lipofectamine™ 2000 Transfection Reagent (Invitrogen, USA) following the manufacturer’s protocol. The MEF2C-AS1 expression was measured by qRT-PCR 24 h later.
Cell proliferation assay
The direct cell count method was used to examine cell proliferation. Briefly, 1.2 × 105 cells/well were seeded in 12-well plates, and cells were transfected with control (pLV3 vector) or pLV3-MEF2C-AS1 plasmids after 24 h, respectively. Cells were collected at 24 h and 48 h after transfection and counted using a CytoSMART Exact FL Cell Counter (CytoSMART Technologies, Netherlands).
Wound healing and transwell assays
The transfected RKO cells (pLV3 vector and pLV3-MEF2C-AS1 plasmid) were seeded in 6-well plates. A wound healing assay was used to assess the cell migration. The wound margins were photographed at 0 h and 24 h after scratching the cells with a 200 µl sterile pipette tip. Cell migration and invasion assays were performed using 8-µm transwell chambers (BIOFIL, China). For migration assay, the cells (2 × 105/well) were plated in serum-free medium onto the upper chamber and a 500 µl medium containing 30% FBS was added to the lower chamber. After incubation for 72 h, the cells were fixed with 4% paraformaldehyde and stained with 0.1% crystal violet. The migrated cells on the lower surface were photographed under an inverted microscope (Olympus CKX53, Japan) and counted. For invasion assay (3 × 105 cells/well), the upper chamber was precoated with Matrigel (Corning, USA), and all other processes were the same.
Target miRNA and mRNA prediction
The differentially expressed miRNAs and mRNAs were analyzed using data from the TCGA and UCSC Xena databases. The miRNAs targeted by MEF2C-AS1 were predicted using the miRcode database (http://www.mircode.org/) [49], and then the target mRNAs regulated by miRNAs were predicted by the combinative analysis using the miRDB (http://mirdb.org/) [50], miRTarBase (https://mirtarbase.cuhk.edu.cn/) [51], and TargetScan (http://www.targetscan.org/) databases [52].
Statistical analysis
The continuous variable was expressed as the mean ± standard deviation (SD), and the categorical variable was expressed as the frequency. Paired Student’s t test and Wilcoxon test were used to compare the differences between paired groups. The Kruskal–Wallis test and one-way analysis of variance (ANOVA) followed by the post hoc Dunn’s and Dunnett’s tests were used to compare the differences among multiple groups. Survival time was calculated from the date of diagnosis to the death date or the end date of uniform follow-up. CRC patients were further divided into groups of high and low methylation using maxstat statistics in the R package “survminer”. The Kaplan–Meier method and log-rank test were used to compare the DSS of CRC patients in different groups. All statistical analyses were performed in R software (version 3.6.1). A two-tailed p value less than 0.05 was considered statistically significant.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable requests. RNA-Seq expression data and 450 K array methylation data for 33 cancers could be obtained from the GEPIA (http://gepia.cancer-pku.cn/), UCSC Xena (https://xena.ucsc.edu/), and TCGA (https://portal.gdc.cancer.gov/) databases, respectively. Prediction of target miRNAs and mRNAs was performed by the miRcode (http://www.mircode.org/), miRDB (http://mirdb.org/), miRTarBase (https://mirtarbase.cuhk.edu.cn/), and TargetScan (http://www.targetscan.org/) databases.
Abbreviations
- 450 K array:
-
Illumina HumanMethylation450 BeadChip
- 5-Aza-dC:
-
5-Aza-2’-deoxycytidine
- 850 K array:
-
Illumina MethylationEPIC BeadChip
- AA:
-
Advanced adenoma
- ANOVA:
-
Analysis of variance
- BC:
-
Breast cancer
- CC:
-
Cervical cancer
- ceRNA:
-
Competitive endogenous RNA
- CpG:
-
Cytosine–guanine dinucleotide
- CRC:
-
Colorectal cancer
- CSCC:
-
Cervical squamous cell carcinoma
- DGC:
-
Diffuse gastric cancer
- DSS:
-
Disease-specific survival
- ESCC:
-
Esophageal squamous cell carcinoma
- FAP:
-
Familial adenomatous polyposis
- FBS:
-
Fetal bovine serum
- GTEx:
-
Genotype-Tissue Expression
- lncRNA:
-
Long noncoding RNA
- MEF2C-AS1:
-
MEF2C antisense RNA 1
- NAA:
-
Non-advanced adenoma
- OS:
-
Osteosarcoma
- PC:
-
Pancreatic cancer
- qRT-PCR:
-
Quantitative reverse transcription-polymerase chain reaction
- RNA-Seq:
-
RNA sequencing
- SD:
-
Standard deviation
- TCGA:
-
The Cancer Genome Atlas
- TPM:
-
Transcripts per million
References
Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–49.
Hill MJ, Morson BC, Bussey HJ. Aetiology of adenoma–carcinoma sequence in large bowel. Lancet. 1978;1(8058):245–7.
Brenner H, Kloor M, Pox CP. Colorectal cancer. Lancet. 2014;383(9927):1490–502.
Lichtenstein P, Holm NV, Verkasalo PK, Iliadou A, Kaprio J, Koskenvuo M, et al. Environmental and heritable factors in the causation of cancer–analyses of cohorts of twins from Sweden, Denmark, and Finland. N Engl J Med. 2000;343(2):78–85.
Gu M, Huang Q, Bao C, Li Y, Li X, Ye D, et al. Attributable causes of colorectal cancer in China. BMC Cancer. 2018;18(1):38.
Kopp F, Mendell JT. Functional classification and experimental dissection of long noncoding RNAs. Cell. 2018;172(3):393–407.
Liao K, Xu J, Yang W, You X, Zhong Q, Wang X. The research progress of lncRNA involved in the regulation of inflammatory diseases. Mol Immunol. 2018;101:182–8.
Schmitz SU, Grote P, Herrmann BG. Mechanisms of long noncoding RNA function in development and disease. Cell Mol Life Sci. 2016;73(13):2491–509.
Uchida S, Dimmeler S. Long noncoding RNAs in cardiovascular diseases. Circ Res. 2015;116(4):737–50.
Ge Q, Jia D, Cen D, Qi Y, Shi C, Li J, et al. Micropeptide ASAP encoded by LINC00467 promotes colorectal cancer progression by directly modulating ATP synthase activity. J Clin Invest. 2021;131:e152911.
Dong Z, Wang Y. LncRNA BLACAT1 accelerates the proliferation and migration of osteosarcoma cells through regulating STAT3. Pathol Res Pract. 2019;215(3):571–9.
Zhou X, Gao W, Hua H, Ji Z. LncRNA-BLACAT1 facilitates proliferation, migration and aerobic glycolysis of pancreatic cancer cells by repressing CDKN1C via EZH2-induced H3K27me3. Front Oncol. 2020;10: 539805.
Hu X, Liu Y, Du Y, Cheng T, Xia W. Long non-coding RNA BLACAT1 promotes breast cancer cell proliferation and metastasis by miR-150-5p/CCR2. Cell Biosci. 2019;9:14.
Su J, Zhang E, Han L, Yin D, Liu Z, He X, et al. Long noncoding RNA BLACAT1 indicates a poor prognosis of colorectal cancer and affects cell proliferation by epigenetically silencing of p15. Cell Death Dis. 2017;8(3):e2665.
Cheng H, Tian J, Wang C, Ren L, Wang N. LncRNA BLACAT1 is upregulated in cervical squamous cell carcinoma (CSCC) and predicts poor survival. Reprod Sci. 2020;27(2):585–91.
Geng T, Heyward CA, Chen X, Zheng M, Yang Y, Reseland JE. Comprehensive analysis identifies ameloblastin-related competitive endogenous RNA as a prognostic biomarker for Testicular Germ Cell Tumour. Cancers (Basel). 2022;14(8):1870.
Zhang J, Huang K. Pan-cancer analysis of frequent DNA co-methylation patterns reveals consistent epigenetic landscape changes in multiple cancers. BMC Genomics. 2017;18(Suppl 1):1045.
Dawson MA, Kouzarides T. Cancer epigenetics: from mechanism to therapy. Cell. 2012;150(1):12–27.
Choi JA, Kwon H, Cho H, Chung JY, Hewitt SM, Kim JH. ALDH1A2 is a candidate tumor suppressor gene in ovarian cancer. Cancers (Basel). 2019;11(10):1553.
Olsson M, Beck S, Kogner P, Martinsson T, Carén H. Genome-wide methylation profiling identifies novel methylated genes in neuroblastoma tumors. Epigenetics. 2016;11(1):74–84.
Zheng Y, Huang Q, Ding Z, Liu T, Xue C, Sang X, et al. Genome-wide DNA methylation analysis identifies candidate epigenetic markers and drivers of hepatocellular carcinoma. Brief Bioinform. 2018;19(1):101–8.
Kim Y, Wen X, Jeong S, Cho NY, Kim WH, Kang GH. Combinatory low methylation statuses of SAT-α and L1 are associated with shortened survival time in patients with advanced gastric cancer. Gastric Cancer. 2019;22(1):37–47.
Uhan S, Zidar N, Tomažič A, Hauptman N. Hypermethylated promoters of genes and as potential novel diagnostic biomarkers in colorectal cancer. Epigenomics. 2020;12(19):1677–88.
Chen L, Zhang W, Li DY, Wang X, Tao Y, Zhang Y, et al. Regulatory network analysis of LINC00472, a long noncoding RNA downregulated by DNA hypermethylation in colorectal cancer. Clin Genet. 2018;93(6):1189–98.
Fiedler D, Hirsch D, El Hajj N, Yang HH, Hu Y, Sticht C, et al. Genome-wide DNA methylation analysis of colorectal adenomas with and without recurrence reveals an association between cytosine-phosphate-guanine methylation and histological subtypes. Genes Chromosom Cancer. 2019;58(11):783–97.
Fan J, Li J, Guo S, Tao C, Zhang H, Wang W, et al. Genome-wide DNA methylation profiles of low- and high-grade adenoma reveals potential biomarkers for early detection of colorectal carcinoma. Clin Epigenetics. 2020;12(1):56.
Luo T, Zhao J, Lu Z, Bi J, Pang T, Cui H, et al. Characterization of long non-coding RNAs and MEF2C-AS1 identified as a novel biomarker in diffuse gastric cancer. Transl Oncol. 2018;11(5):1080–9.
Wang X, Zhang C, Gong M, Jiang C. A novel identified long non-coding RNA, lncRNA MEF2C-AS1, inhibits cervical cancer via regulation of miR-592/RSPO1. Front Mol Biosci. 2021;8: 687113.
Yin W, Yang F, Guo J, Yan M. LncRNA MEF2C-AS1 inhibits the proliferation, migration and invasion of breast cancer cells by down-regulating the expression of miR-3646. Chin J Biomed Eng. 2019;25(6):678–84.
Panagopoulou M, Drosouni A, Fanidis D, Karaglani M, Balgkouranidou I, Xenidis N, et al. ENPP2 promoter methylation correlates with decreased gene expression in breast cancer: implementation as a liquid biopsy biomarker. Int J Mol Sci. 2022;23(7):3717.
Kodama T, Oki K, Otagaki Y, Baba R, Okada A, Itcho K, et al. Association of DNA methylation with steroidogenic enzymes in Cushing’s adenoma. Endocr Relat Cancer. 2022;29(8):495–502.
Zhou J, Zhao Y, Leng J, Gu Y, Xu Z, Ma J, et al. DNA methylation-mediated differential expression of DLX4 isoforms has opposing roles in leukemogenesis. Cell Mol Biol Lett. 2022;27(1):59.
Ranjan N, Pandey V, Panigrahi MK, Klumpp L, Naumann U, Babu PP. The tumor suppressor MTUS1/ATIP1 modulates tumor promotion in Glioma association with epigenetics and DNA repair. Cancers (Basel). 2021;13(6):1245.
Pan J, Tan Y, Wang F, Hou N, Xiang Y, Zhang J, et al. Aberrant expression and DNA methylation of lipid metabolism genes in PCOS: a new insight into its pathogenesis. Clin Epigenetics. 2018;10:6.
Li Y, Bai L, Yu H, Cai D, Wang X, Huang B, et al. Epigenetic inactivation of α-internexin accelerates microtubule polymerization in colorectal cancer. Cancer Res. 2020;80(23):5203–15.
He X, Hang D, Wu K, Nayor J, Drew DA, Giovannucci EL, et al. Long-term risk of colorectal cancer after removal of conventional adenomas and serrated polyps. Gastroenterology. 2020;158(4):852-61.e4.
Kim-Wanner SZ, Assenov Y, Nair MB, Weichenhan D, Benner A, Becker N, et al. Genome-wide DNA methylation profiling in early stage I lung adenocarcinoma reveals predictive aberrant methylation in the promoter region of the long noncoding RNA PLUT: an exploratory study. J Thorac Oncol. 2020;15(8):1338–50.
Dong Z, Li S, Wu X, Niu Y, Liang X, Yang L, et al. Aberrant hypermethylation-mediated downregulation of antisense lncRNA ZNF667-AS1 and its sense gene ZNF667 correlate with progression and prognosis of esophageal squamous cell carcinoma. Cell Death Dis. 2019;10(12):930.
Wang X, Wang D, Liu J, Feng M, Wu X. A novel CpG-methylation-based nomogram predicts survival in colorectal cancer. Epigenetics. 2020;15(11):1213–27.
Bhan A, Soleimani M, Mandal SS. Long noncoding RNA and cancer: a new paradigm. Cancer Res. 2017;77(15):3965–81.
Xu M, Xu X, Pan B, Chen X, Lin K, Zeng K, et al. LncRNA SATB2-AS1 inhibits tumor metastasis and affects the tumor immune cell microenvironment in colorectal cancer by regulating SATB2. Mol Cancer. 2019;18(1):135.
Li J, Du L, Yang Y, Wang C, Liu H, Wang L, et al. MiR-429 is an independent prognostic factor in colorectal cancer and exerts its anti-apoptotic function by targeting SOX2. Cancer Lett. 2013;329(1):84–90.
Ye D, Huang Q, Li Q, Jiang X, Mamat M, Tang M, et al. Comparative evaluation of preliminary screening methods for colorectal cancer in a mass program. Dig Dis Sci. 2017;62(9):2532–41.
Rex DK, Boland CR, Dominitz JA, Giardiello FM, Johnson DA, Kaltenbach T, et al. Colorectal cancer screening: recommendations for physicians and patients from the U.S. multi-society task force on colorectal cancer. Gastroenterology. 2017;153(1):307–23.
Edge SB, Compton CC. The American joint committee on cancer the 7th edition of the AJCC cancer staging manual and the future of TNM. Ann Surg Oncol. 2010;17(6):1471–4.
Tang Z, Li C, Kang B, Gao G, Li C, Zhang Z. GEPIA: a web server for cancer and normal gene expression profiling and interactive analyses. Nucleic Acids Res. 2017;45(W1):W98-102.
Goldman MJ, Craft B, Hastie M, Repečka K, McDade F, Kamath A, et al. Visualizing and interpreting cancer genomics data via the Xena platform. Nat Biotechnol. 2020;38(6):675–8.
Gu S, Lin S, Ye D, Qian S, Jiang D, Zhang X, et al. Genome-wide methylation profiling identified novel differentially hypermethylated biomarker MPPED2 in colorectal cancer. Clin Epigenetics. 2019;11(1):41.
Jeggari A, Marks DS, Larsson E. miRcode: a map of putative microRNA target sites in the long non-coding transcriptome. Bioinformatics. 2012;28(15):2062–3.
Chen Y, Wang X. miRDB: an online database for prediction of functional microRNA targets. Nucleic Acids Res. 2020;48(D1):D127–31.
Huang HY, Lin YC, Li J, Huang KY, Shrestha S, Hong HC, et al. miRTarBase 2020: updates to the experimentally validated microRNA-target interaction database. Nucleic Acids Res. 2020;48(D1):D148–54.
McGeary SE, Lin KS, Shi CY, Pham TM, Bisaria N, Kelley GM, et al. The biochemical basis of microRNA targeting efficacy. Science. 2019;366(6472):eaav1741.
Acknowledgements
We are grateful to the study participants who provided their samples for the study. We thank the research staff and investigators who have contributed to the data collection and sample acquisition at Shaoxing People’s Hospital and Jiashan Institute of Cancer Prevention and Treatment.
Funding
The work was supported by the National Natural Science Foundation of China (research grant: 81673262) and the National Basic Research Program of China (research grant: 2015CB554003; 973 Program).
Author information
Authors and Affiliations
Contributions
SQ, SL, MJ, and KC conceived and designed the study. XY, ZL, XF, JY, MT, and JW recruited the study participants and collected the biopsies. SQ, SL, XX, HB, and AY performed experiments in the laboratory and analyzed and interpreted the data. SL, XX, and HB performed the statistical analysis. SQ and XX drafted the manuscript with the supervision of MJ and KC. All authors read and contributed to the preparation of the final manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Patients participated in the study signed informed consents, and the study was approved by the Medical Ethics Committee of Zhejiang University School of Medicine.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1
: Fig. S1. Nonsignificant difference in MEF2C-AS1 expression between lesion tissues and normal tissues among 21 cancers by the GEPIA database. Every dot represents the expression level for a tissue sample. Box plot in red or gray represents the distribution of expression level. Expression level is presented in log2(TPM+1) scale. TPM, Transcripts Per Million. ns p > 0.05. Fig. S2. Comparisons of MEF2C-AS1 methylation between lesion tissues and normal tissues among 21 cancers by the UCSC Xena database. Violin plot in blue or orange represents the distribution of methylation level. * p < 0.05, ns p > 0.05. Fig. S3. The amplified sequence of MEF2C-AS1 was used for the methylation measurement by the MassARRAY method. CpG sites in capital letters were measured, and CpG_1 and CpG_25 correspond to cg10571951 and cg12621171, respectively. CpG sites highlighted in yellow were successfully measured, and those in gray were filtered for methylation analysis. Table S1. The putative predicted target miRNAs and mRNAs of MEF2C-AS1 in CRC.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Qian, S., Lin, S., Xu, X. et al. Hypermethylation of tumor suppressor lncRNA MEF2C-AS1 frequently happened in patients at all stages of colorectal carcinogenesis. Clin Epigenet 14, 111 (2022). https://doi.org/10.1186/s13148-022-01328-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13148-022-01328-1