
Abstract
Background
A complete blood count (CBC) analysis is one of the most common conventional blood tests that physicians frequently prescribe.
The objective
of this study was to determine the reference intervals (RIs) of CBC parameters in the population of healthy adults living in the western Sudan region.
Methods
A cross-sectional study of healthy people residing in the western area of Sudan was carried out. We assessed the CBC RIs in samples taken from 153 individuals using an automated haematology analyser (Sysmex KX-21) and a modified Box–Cox transformation procedure to transform the data into a Gaussian distribution after eliminating outliers using the Dixon method. IBM SPSS Statistics version 25 was used to analyse the data, and t tests were employed to examine variations in the mean CBC parameters according to sex and age. P was considered significant at ≤ 0.05.
Results
Beyond all the other measured values, the only CBC parameters that significantly differed between the sexes were haemoglobin (HGB) and white blood cell (WBC) counts. Women were found to experience more WBC counts than men did. However, they have less HGB RIs.The male participants in our study exhibited lower WBC count RIs, a significantly lower limit, and a greater upper limit of platelet RIs than did the individuals from other nations.
Conclusions
Compared with males, females had higher platelet and WBC counts and lower HGB.
Similar content being viewed by others


Introduction
A complete blood count (CBC) is an essential tool for the diagnosis and treatment of hematologic illnesses as well as for the general assessment of an individual’s health [1]. However, recent research has shown that there are notable variations in hematological reference values between various populations, underscoring the significance of creating reference intervals (RIs) unique to each ethnic group [2, 3]. Inappropriate RIs can result in incorrect patient care and misclassification; hence, RIs that take geography, race, and ethnicity into consideration are essential for screening, diagnosing, treating, and monitoring hematological disorders [4].To guarantee correct evaluations, the International Federation of Clinical Chemistry (IFCC) and the Clinical and Laboratory Standards Institute (CLSI) advise laboratories to develop their own RIs [5,6,7].
An essential measure of immunological response and inflammation is the white blood cell (WBC) count. Age, sex, and ethnicity are a few variables that may have an impact on variations in WBC count [8, 9]. For instance, African Americans typically have higher WBC counts than Caucasian people [10]. It is important to take these differences into account when assessing WBC counts in various groups.
Factors, including ethnicity, smoking status, and altitude, can all have an impact on variations in red blood cell (RBC) counts [11, 12]. People who live at high elevations, for instance, might have increased RBC counts because of the body’s adaptation to low oxygen levels [12]. Similarly, research has revealed that people of African heritage typically have greater RBC counts than people from other groups [13].A number of variables, including age, sex, altitude, and ethnicity, might affect haemoglobin (HGB) levels [14]. For instance, research indicates that because of the body’s adaptation to low oxygen levels, individuals who live at high elevations typically have lower haemoglobin levels [15]. Furthermore, differences in haemoglobin levels have been noted among several ethnic groups [16,17,18,19,20,21,22,23,24].
Age, sex, and ethnicity are a few variables that may have an impact on platelet count [25]. For instance, research indicates that men often have larger platelet counts than women [25]. Furthermore, differences in platelet counts have been noted between several ethnic groups [16,17,18,19,20,21,22,23,24].
The variation in the size of red blood cells was measured by determining the red cell distribution width (RDW). Research has indicated that older people typically have greater RDWs than younger people [26]. Furthermore, differences in RDW have been noted among several ethnic groups [16,17,18,19,20,21,22,23,24].
Since each population is unique and several factors can influence normal physiological values, it is imperative to obtain reference values from the local population before applying them in a clinical setting [27]. In Sudan, where blood cell reference values have not yet been established, it is common to rely on values from developed countries. Therefore, this study aimed to determine the reference intervals for CBC parameters in a healthy adult population residing in western Sudan, focusing on the specific variations observed within this population.
Methods
Study design, duration and setting
A cross-sectional descriptive study of healthy adults residing in Al Fashir city, the capital of the western Sudan region (which includes Darfur and Kordofan), was carried out in September and October 2019. At the time of the most recent census, the region’s estimated population was 14.448.738. Its area is 869.325 km² (337.352 miles²).
Study population and eligibility criteria
Study participants were chosen on the basis of their clinical history, physical examination, and CLSI-IFCC inclusion and exclusion criteria [5]. The inclusion criteria for individuals were as follows: male or female between the ages of 18 and 64, inhabited by western Sudan for at least six months, and seronegative for hepatitis B and C viruses. The exclusion criterion included having any medical condition, such as high blood pressure, anaemia, or Cardio Vascular Diseases (CVD). Drug treatment, alcohol use, heavy smoking, chronic illnesses such as diabetes mellitus (DM), and blood donation within the previous three months were additional exclusion criteria. People who had recently undergone surgery were also excluded.
Sample size and technique
To establish reference intervals using the percentile method, the IFCC-CLSI recommends a sample size of 120 samples for each stratum [5]. For robust and parametric methods, the recommended sample size is at least 40 samples per category. In this study, we used a parametric method to establish RIs among 153 subjects.
Data collection and study procedure
Each of the chosen participants completed a questionnaire with detailed personal information, medical history, level of physical activity, food, and smoking status. To analyse 18 complete blood count (CBC) parameters (white blood cell (WBC), red blood cell (RBC), platelet (PLT), haemoglobin (HGB), haematocrit (HCT), mean corpuscular voulume (MCV), mean corpuscular haemoglobin (MCH), mean corpuscular haemoglobin concentration (MCHC), red cell distribution width count and percentage (RDW), platelet distribution width (PDW), mean platelet volume (MPV), leukocyte differential absolute counts (abs) and percentages (%) of neutrophils (Neu), lymphocytes (Lym) and mixed (monocyte (Mon), eosinophil (Eos), basophil (Bas)) cells (mxd)), a sample of 2–3 ml of venous blood was drawn and placed into vacutainer tubes containing ethylenediaminetetraacetic acid (EDTA) anticoagulant. The time frame for collecting the samples was 8:00 a.m. to 11 a.m. Following the blood and anticoagulant mixture, the test vials were properly labelled. After that, the samples were placed in an ice box, brought to the laboratory, and processed for two hours. A Sysmex KX-21 automated haematology analyser at Alfashir Police Hospital Laboratory was used to analyse the blood.
Quality control
Precautions for IFCC-CLSI sample analysis were taken into account. Every day, the analyser was calibrated using industry standards. 10% of the samples were reanalyzed in the reference laboratory as part of an external quality control measure.
Data analysis
SPSS version 25, or the Statistical Package for the Social Sciences, was used to conduct the statistical analysis. The data distribution was assessed using the Shapiro‒Wilk and Kolmogorov‒Smirnov tests. A modified Box–Cox transformation formula was used to convert the data into a Gaussian distribution so that reference intervals could be calculated using a parametric approach. Using the Dixon method, the participants were examined for outliers. The data included the mean, standard deviation, and reference intervals (mean ± 1.96*SD), which represent the central 95% lower (LL) and upper limits (UL) under the transformed scale. The LL and UL at the original scale are then obtained by reversing the limits. In addition, the obtained reference intervals were contrasted with values from other African nations. Student’s t test was used to assess the relationships between the participants’ age and sex and blood parameters. A P value ≤ 0.05 was considered to indicate statistical significance.
Results
The purpose of the study was to determine the reference values for complete blood counts in adults in western Sudan who were in good health.
The participants’ characteristics
In all, 172 participants in the 18–64 age range participated in the study. Nineteen patients were eliminated owing to diabetes mellitus (3), hypertension (5), high BMI (3), or outliers (8), resulting in a final sample size of 153. There were 56 (36.7%) males and 97 (63.3%) females in total, with a mean age of 23.5 years.
Determination of reference intervals
Reference intervals (means ± 1.96*SD) were obtained for each of the eighteen complete blood count parameters through the parametric approach. Table 1. Of the complete blood count parameters measured, only WBC and HGB counts significantly differed between the sexes. Table 2. Age was not a significant (p value ˃ 0.05) source of variation for any of the measured CBC parameters.
The reference intervals determined in this study were also contrasted with those reported in related studies conducted in Kenya (18) and Eritrea (19) using parametric methods and nonparametric methods, respectively. Table 3.
Discussion
The complete blood count (CBC) test is essential for diagnosing a wide range of illnesses and assessing overall health. The outcomes were influenced by a number of factors, such as geography and sex. The purpose of this study was to ascertain CBC reference intervals for the population of western Sudan region to determine the standards for laboratory results. The study’s findings highlight the fact that the RIs discovered in one community should not be extrapolated to other communities.
According to our research, the RIs for several RBC parameters, such as RBC count, HCT, MCV, MCH, MCHC, and RDW, did not differ according to sex. However, males had a greater HGB than females did. This result is consistent with earlier research conducted in African nations [20, 21]. A poor diet; frequent childbirth; monthly blood loss in women; and the effects of androgen, oestrogens, and testosterone on RBC synthesis are thought to be the main causes of these sex differences [14, 18, 23, 28]. Furthermore, a World Health Organization (WHO) report [29] states that a woman over the age of 15 is considered anaemic if her HGB is less than 12 g/dl. Therefore, given that we report a lower limit (10.4 g/dl) for HGB reference intervals in our study, a certain percentage of women are anemic.
There was a noticeable difference in the RI of the total WBC count between males and females. These results are consistent with research conducted in Turkey [30]. This contradicts the results of a study conducted in the Central African Republic [31]. Although there was considerable sex variation in the WBC count, the WBC differential (LYM, NEUT, and MXD) counts and percentages of males and females did not exhibit any discernible sex variation. These results are consistent with those of other studies conducted in the Central African Republic and Turkey [30, 31]. In addition, our results imply that, in comparison to those of the Eritrean study, the male WBC count reference intervals were lower [19].
Additionally, there was no statistically significant difference in platelet count or platelet indices (PDW or MPV) between the sexes according to our study. These findings are consistent with those of other research carried out in Ghana and Kenya [24, 32]. According to our research, the PLT reference intervals in males had a greater upper limit and a significantly lower limit. This finding is in contrast to research conducted in Kenya and Eritrea [18, 19]. Although our investigation of reduced platelet count is in line with findings from other countries [28, 32], the reason for this difference has yet to be determined.
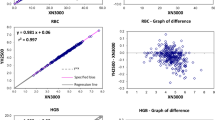
The parametric method is more dependable than the nonparametric method at driving precise and narrower reference intervals because it includes a step for excluding values outside of the mean, can successfully transform data into a normal distribution shape by using a modified Box–Cox transformation formula, and provides a fairly consistent optimal power value for the Gaussian transformation parameter by parameter [27]. These facts are established unequivocally by comparing the reference intervals generated by the two techniques in the Kenyan study [18].
Conclusion
The HGB and WBC counts were significantly different according to sex, with women having lower HGB and higher WBC count RIs than men. Compared to that in previous studies, the lower limit of the platelet count RIs in males was significantly lower.
Strengths and limitations
To the best of our knowledge, this is the first study to create CBC RIs for adults living in western Sudan; the created RIs might be useful for diagnostic laboratories in the area. Additionally, RIs obtained using the parametric methods are more accurate than those derived using other methods. However, there was a drawback to our research. The recruitment of samples and the dominance of particular tribes in the area may introduce selection bias, which could restrict the ability to generalize the findings.
Data availability
The corresponding author can provide the datasets used and analysed for this study upon reasonable request.
References
Agnello L, Giglio RV, Bivona G, Scazzone C, Gambino CM, Iacona A, Ciaccio AM, Lo Sasso B, Ciaccio M. The value of a complete blood Count (CBC) for Sepsis diagnosis and prognosis. Diagnostics. 2021;11(10):1881. https://doi.org/10.3390/diagnostics11101881.
Parameaswari ARS, Shanthi PJ, Revathy B, Parijatham C. The reference intervals for the haematological parameters in healthy adult population of Chennai, southern India. J Clin Diagn Res. 2012;6(10):1675–80. https://doi.org/10.7860/JCDR/2012/4882.2630. Epub 2012 Oct 6. PMID: 23373026; PMCID: PMC3552202.
Saad Bakrim et al. Establishment of the hematology reference intervals in a healthy population of adults in the Northwest of Morocco (Tangier-Tetouan region). Pan African Medical Journal 2018;29:169. https://doi.org/10.11604/pamj.2018.29.169.13042.
Yesim Ozarda K, Sikaris T, Streichert J, on behalf of IFCC Committee on Reference intervals and Decision Limits (C-RIDL). Distinguishing reference intervals and clinical decision limits– A review by the IFCC Committee on Reference Intervals and decision limits. Crit Rev Clin Lab Sci. 2018;55(6):420–31. https://doi.org/10.1080/10408363.2018.1482256.
CLSI. Defining, establishing, and verifying reference intervals in the clinical laboratory; approved Guideline– Third Edition. CLSI EPC28-A3c. Wayne (PA): Clinical and Laboratory Standards Institute; 2010.
CLSI. Method procedure comparison and bias estimation using patient samples, approved guideline, 3rd ed. Wayne (PA): CLSI, 2013. CLSI document EP09-A3.
Ozarda Y, Higgins V, Adeli K. Verification of reference intervals in routine clinical laboratories: practical challenges and recommendations. Clin Chem Lab Med (CCLM). 2019;57(1):30–7. https://doi.org/10.1515/cclm-2018-0059.
Bain BJ. Ethnic and sex differences in the total and differential white cell count and platelet count. J Clin Pathol. 1996;49(8):664–6. https://doi.org/10.1136/jcp.49.8.664. PMID: 8881919; PMCID: PMC500612.
Eun HN, Suyoung K, Seon C, Hanik C. Complete blood count reference intervals and patterns of changes across Pediatric, Adult and Geriatric ages in Korea. Annals Lab Med. 2018;38(6):503–11.
Lim E, Miyamura J, Chen JJ. Racial/Ethnic-Specific reference intervals for Common Laboratory tests: a comparison among asians, blacks, hispanics, and White. Hawaii J Med Public Health. 2015;74(9):302–10. PMID: 26468426; PMCID: PMC4578165.
Ahmed IA, Mohammed MA, Hassan HM, Ali IA. Relationship between tobacco smoking and hematological indices among Sudanese smokers. J Health Popul Nutr. 2024;43(1):5. https://doi.org/10.1186/s41043-023-00493-0. PMID: 38178235; PMCID: PMC10765807.
Husain Y, Alkhaldy ZA, Awan, Ahmed A, Abouzaid, Hossameldin M, Elbahaey, Saeed M, Al Amoudi, Shehata F, Shehata, Muhammad Saboor. Effect of Altitude on Hemoglobin and Red Blood cell indices in adults in different regions of Saudi Arabia. Int J Gen Med. 2022;15:3559–65. https://doi.org/10.2147/IJGM.S358139.
Beutler E, West C. Hematologic differences between African-Americans and whites: the roles of iron deficiency and alpha-thalassemia on hemoglobin levels and mean corpuscular volume. Blood. 2005;106(2):740-5. doi: 10.1182/blood-2005-02-0713. Epub 2005 Mar 24. PMID: 15790781; PMCID: PMC1895180.
Sala C, Ciullo M, Lanzara C, Nutile T, Bione S, Massacane R. Variations of hemoglobin levels in normal Italian populations from genetic isolates. Haematologica. 2008;93:1372–75.
Storz JF. Hemoglobin-oxygen affinity in high-altitude vertebrates: is there evidence for an adaptive trend? J Exp Biol. 2016;219(Pt 20):3190–203. https://doi.org/10.1242/jeb.127134. PMID: 27802149; PMCID: PMC5091379.
Roshan TM, Rosline H, Ahmed SA, Rapiaah M, Zaidah AW, Khattak MN. Hematological reference values of healthy Malaysian population. Int J Lab Hematol. 2009;31:505–12.
Kamal M, Awad AA, Bashir AA, Osman MA, Malek AA, Alborai, et al. Refrence value s of hemoglobin and red cells indices in Sudanese in Khartoum State. Internatio J Healt Sci Res. 2019;9(1):214.
Omuse G, Maina D, Mwangi J, Wambua C, Radia K, Kanyua A et al. Complete blood count reference intervals from a healthy adult urban population in Kenya. PLoS ONE 2018; 13(6): e0198444. https://doi.org/10.1371/journal.pone.0198444.
Siraj, et al. Establishment of hematological reference intervals for healthy adults in Asmara. BMC Res Notes. 2018;11:55. https://doi.org/10.1186/s13104-018-3142-y.
Yalew A, Terefe B, Alem M, Enawgaw B. Hematological reference intervals determination in adults at Gondar university hospital, Northwest Ethiopia. BMC Res Notes. 2016;9:483. https://doi.org/10.1186/s13104-016-2288-8.
Isa AH, Hassan A, Garba Y, Ijei IP. Reference ranges of some haematological parameters in healthy northern Nigerian adults. Jos J Med. 2012;6:10–5.
Xinzhong WU, Min Z, Baishen PJ, Mingting PL, Wang X, et al. Complete blood count reference intevals for healthy Han Chinese adults. PLoS ONE. 2015;10(3):e0119669.
Saathoff E, Schneider P, Kleinfeldt V, Geis S, Haule D. Laboratory reference values for healthy adults from Southern Tanzania. Trop Med Int Healt. 2008;13:612–25.
Dosoo DK, Kayan K, Adu-Gyasi D, Kwara E, Ocran J, et al. Haematological and biochemical reference values for healthy adults in the middle belt of Ghana. PLoS ONE. 2012;7(4):e36308. https://doi.org/10.1371/journal.
De Gaetano G, Bonaccio M, Cerletti C. How different are blood platelets from women or men, and young or elderly people? Haematologica. 2023;108(6):1473–5. https://doi.org/10.3324/haematol.2022.282131. PMID: 36384253; PMCID: PMC10230435.
Pilling LC, Atkins JL, Duff MO, Beaumont RN, Jones SE, Tyrrell J, Kuo CL, Ruth KS, Tuke MA, Yaghootkar H, Wood AR, Murray A, Weedon MN, Harries LW, Kuchel GA, Ferrucci L, Frayling TM, Melzer D. Red blood cell distribution width: genetic evidence for aging pathways in 116,666 volunteers. PLoS ONE. 2017;12(9):e0185083. https://doi.org/10.1371/journal.pone.0185083. PMID: 28957414; PMCID: PMC5619771.
Ichihara K, Ozarda Y, Barth JH, Klee G, Qiu L, Erasmus R, et al. A global multicenter study on reference values: 1. Assessment of methods for derivation and comparison of reference intervals. Clin Chim Acta. 2017;467:70–82. PMID: 27666761.
Usman K, Syed ZA, Rao AA. Reference range values of haematological parameters in healthy Pakistani adults. Pak J Physiol. 2007;3:19–22.
WHO. Haemoglobin concentrations for the diagnosis of anaemia and assessment of severity. https://www.who.int/publications/i/item/WHO-NMH-NHD-MNM-11.1
Kaya H, Kiki Ý, Akarsu E, Gündoðdu M, Tekin BS, Ýnand T. Hematological values of healthy adult population living at moderate altitude 1869 m, Erzurum, Turkey. Turk J Haematol. 2000;17(3):123–8.
Didier M, Marie JM, Mesmin BT, et al. Immunohaematological reference ranges for adults from the Central African Republic. Clin Diagn Lab Immunol. 2003;10:443–5.
Kibaya RS, Bautista CT, Sawe FK, Shafer DN, Sateren WB, Scott PT, et al. Reference ranges for the clinical laboratory derived from a rural population in Kericho, Kenya. PLoS ONE. 2008;3(10):e3327.
Acknowledgements
Many thanks to everyone who took part in this study and provided blood samples.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
MI, IA, MA obtained the ethical approval. MI, IA, MA, KM, EH OA conceived of the study and participated in the design. MI, IA, MI, IA, MA, KM, EH OA have made substantial contributions.MA, KM, MI, IA analyzed the data, draft and edit the manuscript. MI, IA, MA, KM recruited participants, collected samples, and performed laboratory experiments. EH, OA review the scientific content and supervise the work at all stages. MI, IA, MA, KM, EH OA read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The National Ribat University’s Ethics Committee granted this study ethical approval. Following an explanation of the study’s purpose, each participant provided written informed consent.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Mustafa, M.I., Ali, I.A., Mohammed, M.A. et al. Reference intervals of complete blood count parameters in the adult western Sudanese population. BMC Res Notes 17, 99 (2024). https://doi.org/10.1186/s13104-024-06754-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13104-024-06754-3