
Abstract
Objective
Hypnosis can be an effective treatment for many conditions, and there have been attempts to develop instrumental approaches to continuously monitor hypnotic state level (“depth”). However, there is no method that addresses the individual variability of electrophysiological hypnotic correlates. We explore the possibility of using an EEG-based passive brain-computer interface (pBCI) for real-time, individualised estimation of the hypnosis deepening process.
Results
The wakefulness and deep hypnosis intervals were manually defined and labelled in 27 electroencephalographic (EEG) recordings obtained from eight outpatients after hypnosis sessions. Spectral analysis showed that EEG correlates of deep hypnosis were relatively stable in each patient throughout the treatment but varied between patients. Data from each first session was used to train classification models to continuously assess deep hypnosis probability in subsequent sessions. Models trained using four frequency bands (1.5–45, 1.5–8, 1.5–14, and 4–15 Hz) showed accuracy mostly exceeding 85% in a 10-fold cross-validation. Real-time classification accuracy was also acceptable, so at least one of the four bands yielded results exceeding 74% in any session. The best results averaged across all sessions were obtained using 1.5–14 and 4–15 Hz, with an accuracy of 82%. The revealed issues are also discussed.
Similar content being viewed by others

Introduction
Hypnosis can be an effective treatment for numerous disorders [1,2,3]. The hypnotic response may depend on factors such as hypnotisability, the hypnotic state, expectations [4,5,6], motivation, the therapeutic relationship, etc. [7]. Hypnotisability is a personal trait that greatly affects treatment outcomes [8,9,10,11,12,13]. Nevertheless, hypnosis is currently defined as a state of consciousness [14], and this study is focused solely on the hypnotic state. Hypnotic “depth” has been a contentious issue, but it is still used in contemporary research to describe the hypnotic state quantitatively [5, 15,16,17,18,19,20,21,22], alongside the related concepts of “deep hypnosis” [6, 18, 19, 23,24,25,26,27,28,29,30,31] and “deepening” [16, 32,33,34,35,36,37,38,39]. Multiple studies indicate that sufficient depth is beneficial in some cases, e.g., in non-pharmacological analgesia [24, 25, 40], general hypnotic anaesthesia [26, 30, 33], etc. Greater depth could result in subjects’ feeling more influenced by hypnotic procedures, leading to better compliance [41, 42]. Depth self-ratings can correlate with hypnotisability scores [19].
Probably, a hypnotic state gradually evolves during a session and tends to fluctuate [43]. The possible usefulness of a more accurate estimation of subtle depth alterations, unable to be seen visually, led researchers to the idea of a “hypnometer” [40], a device for real-time hypnotic depth measures to help a practitioner decide whether to continue with deepening or to begin therapeutic suggestions. Heart rate variability (HRV) [40] and an EEG-based parameter, the bispectral index (BIS), were considered the bases for such measures. BIS is a promising method [36, 44]; however, its calculation algorithm is designed primarily for pharmacological anaesthesia rather than hypnotherapy. Moreover, although hypnosis is characterised by some common EEG correlates [18, 31, 36, 44,45,46,47,48,49,50,51,52,53,54,55,56,57], differences between subjects are also observed. Perhaps an approach that addresses individual variability could have benefits.
Passive brain-computer interfaces (pBCI) are used to assess mental states such as fatigue, concentration, etc. [58, 59]. We hypothesise that machine learning might be used to recognise and continuously quantify EEG correlates of hypnosis specific to a person. We aim to explore this possibility by designing a prototype system using an EEG-based pBCI to real-time monitor hypnosis deepening and conducting its initial feasibility test.
Materials and methods
Participants
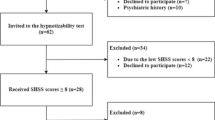
Nine outpatients (six women, mean age: 38.33 ± 10.61 years) underwent up to seven hypnosis sessions. Inclusion criteria: age 18–65 years; consent for participation. Patients had previously reported experiencing deep hypnosis, described as a lack of self-awareness, external awareness, and memories for the deepest period of a session. Thus, probably all included participants could be classified as “dissociators” [60,61,62], “amnesia-prone” [63], or “dissociative” subtype individuals [64]. This is common, yet not the only type to experience hypnosis [4, 5, 15, 65]. Assumed neural correlates of such phenomena were shown in several studies [29, 66]. Exclusion criteria: cognitive decline, epilepsy, psychosis, and no episode of feeling deeply hypnotised during the first session. See “Supplements A(1)” for the participants’ summary.
Hardware and software equipment
The BCI system included equipment for synchronised EEG and video recording and also software: WinEEG 2.130.101 [67], EEGLab 2019.0 [68], and OpenVibe 2.2.0 [69]. See “Supplements A(2)” for details.
A brief description of a hypnotic session
In each patient, after installing the electrodes and equipment for EEG and video recording, a baseline EEG was recorded for 3–5 min with eyes closed. Hypnosis was then induced and deepened by the counting method. After therapeutic suggestions, a patient was awakened. Feedback was then collected.
The principle of the proposed approach
We used the passive type of BCI [58, 59, 70] and supervised learning [71, 72]. A recording from the first session with each patient was used as a calibration file to train a classifier. We first manually identified and then labelled the EEG intervals corresponding to two opposite states of an implied neurophysiological continuum: wakefulness (which matched the baseline registration periods) and the deepest states. The timing of the deepest states was identified with two criteria that had to be present simultaneously:
-
a)
The physical signs recommended to verify sufficient depth [23, 24, 26]: substantial changes in breathing, relaxation of facial muscles, etc.
-
b)
The patients’ post-session feedback on the hypnotherapist’s counting range during which they felt most deeply hypnotised (see “Supplements A(3)” for this procedure’s details).
The file with two sets of labels was then used to train a classifier to continuously recognise (“predict”) these two opposite states in subsequent sessions with interdependent probability. Assuming that deepening is a continuous transition from wakefulness to the deepest hypnotic state, we hypothesise that the continual real-time measurement of the probability of a deep hypnosis during a session could tentatively, to some extent, operate as a quantitative reflection of the deepening process.
Analysis and processing of obtained recordings
The collected data were processed in four ways.
-
a)
Using WinEEG to compare the averaged power spectra of the identified deep hypnosis and the waking periods (5–10 min each) in each EEG, we obtained an overview of each patient’s assumed deep hypnosis patterns (which rhythms at which locations tend to alter while deeply hypnotised). We also assessed their putative stability throughout the treatment, qualitatively comparing them over different patient sessions. This analysis was conducted in parallel with all the others.
-
b)
During supervised learning, we trained prediction models, and those derived from the first sessions were then used in the following sessions for real-time classification. The Common Spatial Pattern (CSP) [73,74,75,76] method was employed for signal spatial filtering, and Linear Discriminant Analysis (LDA) was a classification method. We tested four frequency bands: 1.5–45 Hz; 1.5–8 Hz; 1.5–14 Hz; and 4–15 Hz, to determine which could yield the models with the most classification accuracy, as assessed by the 10-fold cross-validation test. To get the cross-validation results for all sessions, the training procedure should be performed in each session as we did in the first (calibration) one. Thus, each second and subsequent session produced the “auxiliary” models. See “Supplements A(3)” for details.
-
c)
Using models derived from the first sessions for real-time state predictions in subsequent sessions yielded a Probability Value parameter, varying between 0 and 1, displayed as a moving curve, which informed the hypnotherapist of the probability of a deep hypnotic state occurring. We called this curve the Predictive curve. “Supplements A(4)” describe details.
-
d)
Each second and subsequent session was labelled by a specialist not privy to their predictive outcomes, and a percentage of correctly predicted states for different epochs was calculated to additionally test the accuracy [77]. The above-mentioned “auxiliary” models from these sessions were applied to classify the same data on which these models had been trained to plot a curve that reflected depth dynamics in a session most accurately—the Native curve. The Native and Predictive curves of the same sessions were then visually compared. For details, see “Supplements A(5)”.
Results and their discussion
Patient T reported no periods of deep hypnosis in the first session and was excluded from the analysis. Due to the artefacts, the recording from session #5 of Patient E was also excluded. Thus, the total number of EEGs from the remaining eight participants was 27.
Results of the qualitative assessment of the estimated patterns of deep hypnosis in patients and their stability throughout the treatment
Figure 1 demonstrates examples of topographic maps representing these results for three patients.

Comparison of power spectra between periods of deep hypnosis and wakefulness
This is an example of topographic maps displaying the differences in the averaged power spectra between deep hypnosis and the waking periods of EEG (“deep hypnosis” minus “wakefulness”) for three patients. Sessions for display are arbitrarily selected. Thus, the maps demonstrate the alterations in the power of different rhythms for different localizations while achieving deep hypnosis. Power changes are displayed in colour according to the graduation of a nearby colour scale (in uV²). The bands used are: Delta (1.5-4 Hz), Theta (4–8 Hz), Alpha (8–12 Hz), Sensory-motor or Low beta (12–15 Hz), Beta1 (15–18 Hz), Beta2 (18–25 Hz) and Gamma (25–45 Hz)
As seen, the electrophysiological changes tend to be generally similar in different sessions of a particular patient, which suggests that a classifier would correctly recognise the target patterns in the following sessions. Correlates common to the patients are seen, e.g., a slow-wave activity increase, which is consistent with the literature [18, 31, 45,46,47,48,49,50,51,52,53,54,55,56,57]. Several differences between individuals are also shown; therefore, an individualised approach to quantifying hypnosis appeared to be preferable. These points suggest that machine learning may potentially apply to hypnosis. However, the qualitative analysis is approximate, and further statistical assessment may be useful.
“Supplements B” contain all the maps for all 27 sessions for all patients and the details on electrophysiological changes revealed.
Results of the 10-fold cross-validation test of classification accuracy
Table 1(A) shows that the accuracy exceeded 85% in the majority of cases. Results of 100% were possibly due to the optimistic calculation outcomes of the software [78] or the over-fitting phenomenon [79], which are undesirable and should be addressed further.
Results of real-time visual testing of the method (in the second and subsequent sessions)
As an example of such results, Fig. 2(A) shows Patient A’s Predictive curve from his seventh session.

Examples of the Predictive (A) and Native (B) curves. The horizontal axis is a time scale (s), and the vertical axis is a Probability Value scale (from 0 to 1). (A) The Predictive curve graph was played back using data from the seventh session of Patient A. In this example, the classification model was trained using the 1.5–14 Hz range. The curve was smoothed by the Moving epoch average (Immediate) function. The number of 4-s epochs with an overlap of 0.5 s used for averaging was 50. This curve was obtained by feeding the real-time patient’s EEG during the seventh session to the model trained on data from the first session and represents the changing probability of a deep hypnotic state over the session. “Supplements C” contain a detailed case-related analysis of how it could potentially describe session dynamics. (B) The Native curve of the seventh session with Patient A. The band and the smoothing features are the same as in the Predictive curve. This curve was obtained after this (seventh) session by training a model (auxiliary) on data from the same session and then feeding this EEG recording to this model. Thus, this curve, which could only be constructed after the session was over, reflects the changes in the probability of deep hypnosis with very high accuracy
“Supplements C” contain the Predictive curves for each patient. In general, post-session patients’ reports revealed an approximate match between the time when a curve was consistently above 0.7 (approximately, depending on smoothing settings) and a period of unawareness. The high-amplitude wave-like motion was associated with alternating awareness, fractional memories, etc. Thus, this could potentially confirm instrumentally the literature reports of hypnotic depth variations during a session [43]. “Supplements C” contain a detailed analytical description using the individual case.
Results of the classification accuracy evaluation based on the data from the second and subsequent sessions
Table 1(B) shows these results. As seen, the accuracy was high in many cases. Some poor results were due to either myographic artefacts or drift [80]. For a detailed analysis of the case-related findings, see “Supplements D”. In each session, at least one band yielded an accuracy exceeding 74%. Also, as seen, each patient had their “preferred” band for which the model was most accurate, e.g., for Patient A, it was 1.5–14 Hz; for Patients G and S, 1.5–8 Hz, etc., which might correspond with the literature observing variation in findings on electrophysiological correlates of hypnosis [31].
The accuracy averaged across all these sessions was highest when using bands 1.5–14 and 4–15 Hz. This is also in line with studies that reported the most changes in alpha and theta activity [18, 31, 36, 51, 54, 55].
Results of a visual comparison of the Predictive and Native curves
Figure 2(B) shows the Native curve of Patient A’s seventh session. The configurations of curves (A) and (B) largely coincide, giving us additional confirmation that the model can reflect the real picture relatively accurately. “Supplements C” contain the pairs of the Predictive and Native curves for each patient for the second and following sessions.
This study extends the idea of a “hypnometer” [40] but focuses on direct monitoring of brain activity rather than peripheral measurements. BIS for this purpose is promising [36, 44]; however, we suggest that a new approach, which addresses individual correlates of neural activity, may have benefits. It could be used to optimise therapy by controlling depth more precisely when sufficient depth can be helpful [24,25,26, 30, 32, 33, 40,41,42,43, 81].
The designed system is a trial version only and requires further substantial improvements, using both the results and issues we revealed. However, we suppose it could initially demonstrate that pBCI applies to hypnosis.
Limitations
-
Small sample size, the heterogeneous number of sessions, and the artefacts in some recordings.
-
Involvement only of those patients who described their deepest experiences as a lack of awareness and self-awareness. Although these phenomena are common for hypnotic experiences [4, 5, 15, 29, 65, 66], they are probably only characteristics of “dissociators” [60,61,62] or “amnesia-prone” individuals [63]. Perhaps the “fantasizers” [60,61,62] or “fantasy-prone” individuals [63] occurred outside of our focus, and further research should include this group.
-
We did not measure the participants’ hypnotisability. Trait effects are considered to have a different basis [4,5,6,7, 9], and the research of the interaction of state and trait is a serious task that we believe deserves a separate investigation.
-
A single rater was used to label each given recording.
-
Using the measurement of the continuously changing deep hypnosis probability as a tentative reflection of the deepening process is a hypothetical idea in the early stages of testing. The qualitative analysis conducted could partly underpin the information from a Predictive curve, but it is not comprehensive. Further studies, utilising the classification of intermediate levels of hypnosis, are needed.
-
The qualitative analysis of estimated hypnotic patterns is approximate, and further studies can incorporate statistical assessment to strengthen these findings as well as quantify differences in accuracies across subjects and bands and identify similarities between the Native and Predictive curves.
-
Our system is a prototype only, and the signal processing techniques used are not comprehensive, being the initial option. Further research is necessary to test other feature extraction approaches and classification methods [74, 82].
Data Availability
All data generated or analysed during this study are included in this published article and its supplementary information files.
Abbreviations
- EEG:
-
Electroencephalography
- BCI:
-
Brain-computer Interface
- pBCI:
-
Passive Brain-computer Interface
- HRV:
-
Heart Rate Variability
- BIS:
-
Bispectral Index
- CSP:
-
Common Spatial Pattern
- LDA:
-
Linear Discriminant Analysis
References
Elkins G. Clinical hypnosis in health care and treatment. Int J Clin Exp Hypn. 2022;70(1):1–3.
Häuser W, Hagl M, Schmierer A, Hansen E. The efficacy, safety and applications of medical hypnosis: a systematic review of meta-analyses. Dtsch Arztebl Int. 2016;113(17):289–96.
Kirsch I, Montgomery G, Sapirstein G. Hypnosis as an adjunct to cognitive-behavioral psychotherapy: a meta-analysis. J Consult Clin Psychol. 1995;63(2):214–20.
Pekala RJ, Kumar VK, Maurer R, Elliott-Carter N, Moon E, Mullen K. Suggestibility, expectancy, trance state effects, and hypnotic depth: I. Implications for understanding hypnotism. Am J Clin Hypn. 2010;52(4):275–90.
Pekala RJ, Baglio F, Cabinio M, Lipari S, Baglio G, Mendozzi L, et al. Hypnotism as a function of trance state effects, expectancy, and suggestibility: an italian replication. Int J Clin Exp Hypn. 2017;65(2):210–40.
Cardeña E, Terhune DB. The roles of response expectancies, baseline experiences, and hypnotizability in spontaneous hypnotic experiences. Int J Clin Exp Hypn. 2019;67(1):1–27.
Peter B. Hypnosis. In: Wright JD, editor. International encyclopedia of the social and behavioral sciences. 2nd ed. Elsevier Inc.; 2015. pp. 458–64.
Elkins G, Hypnotizability. Emerging perspectives and research. Int J Clin Exp Hypn. 2021;69(1):1–6.
Landry M, Lifshitz M, Raz A. Brain correlates of hypnosis: a systematic review and meta-analytic exploration. Neurosci Biobehav Rev. 2017;81(Pt A):75–98.
Lynn SJ, Shindler K. The role of hypnotizability assessment in treatment. Am J Clin Hypn. 2002;44(3–4):185–97.
Montgomery GH, Schnur JB, David D. The impact of hypnotic suggestibility in clinical care settings. Int J Clin Exp Hypn. 2011;59(3):294–309.
Santarcangelo EL, Carli G. Individual traits and pain treatment: the case of hypnotizability. Front Neurosci. 2021;15:683045.
Thompson T, Terhune DB, Oram C, Sharangparni J, Rouf R, Solmi M, et al. The effectiveness of hypnosis for pain relief: a systematic review and meta-analysis of 85 controlled experimental trials. Neurosci Biobehav Rev. 2019;99:298–310.
Elkins G, Barabasz AF, Council JR, Spiegel D. Advancing research and practice: the revised APA Division 30 definition of hypnosis. Int J Clin Exp Hypn. 2015;63(1):1–9.
Cardeña E, Lindström L, Åström A, Zimbardo PG. Dispositional self-consciousness and hypnotizability. Int J Clin Exp Hypn. 2022;70(1):16–27.
Darmayanti N, Ekawati D, Erlina W. Language aspects in hypnosis dental therapy: pragmatic and stylistic studies. Int J Lang Linguist. 2018;5(2):84–94.
Deeley Q, Oakley DA, Toone B, Giampietro V, Brammer MJ, Williams SCR, et al. Modulating the default mode network using hypnosis. Int J Clin Exp Hypn. 2012;60(2):206–28.
Halsband U, Wolf TG. Current neuroscientific research database findings of brain activity changes after hypnosis. Am J Clin Hypn. 2021;63(4):372–88.
Lush P, Moga G, McLatchie N, Dienes Z. The Sussex-Waterloo Scale of Hypnotizability (SWASH): measuring capacity for altering conscious experience. Neurosci Conscious. 2018;2018(1). niy006.
Perri RL, Perrotta D, Rossani F, Pekala RJ. Boosting the hypnotic experience. Inhibition of the dorsolateral prefrontal cortex alters hypnotizability and sense of agency. A randomized, double-blind and sham-controlled tDCS study. Behav Brain Res. 2022;425:113833.
Perri RL, Di Filippo G. Alteration of hypnotic experience following transcranial electrical stimulation of the left prefrontal cortex. Int J Clin Health Psychol. 2023;23(2):100346.
Tukaev R. The integrative theory of hypnosis in the light of clinical hypnotherapy. In: Mordeniz C, editor. Hypnotherapy and hypnosis. IntechOpen; 2020. https://doi.org/10.5772/intechopen.92761.
Casiglia E, Finatti F, Tikhonoff V, Stabile MR, Mitolo M, Gasparotti F, et al. Granone’s plastic monoideism demonstrated by functional magnetic resonance imaging (fMRI). Psychology. 2019;10(04):434–48.
Casiglia E, Finatti F, Tikhonoff V, Stabile MR, Mitolo M, Albertini F, et al. Mechanisms of hypnotic analgesia explaned by functional magnetic resonance (fMRI). Int J Clin Exp Hypn. 2020;68(1):1–15.
Casiglia E, Finatti F, Gasparotti F, Stabile MR, Mitolo M, Albertini F, et al. Functional magnetic resonance imaging demonstrates that hypnosis is conscious and voluntary. Psychology. 2018;09(07):1571–81.
Casiglia E, Tikhonoff V, Albertini F, Lapenta AM, Gasparotti F, Finatti F, et al. The mysterious hypnotic analgesia: experimental evidences. Psychology. 2018;09(08):1935–56.
De Benedittis G. Neurophysiology and neuropsychology of hypnosis: recent advances and future perspectives: part 2. Am J Clin Hypn. 2021;64(1):1–3.
Facco E, Bacci C, Casiglia E, Zanette G. Preserved critical ability and free will in deep hypnosis during oral surgery. Am J Clin Hypn. 2021;63(3):229–41.
Jiang H, White MP, Greicius MD, Waelde LC, Spiegel D. Brain activity and functional connectivity associated with hypnosis. Cereb Cortex. 2017;27(8):4083–93.
Pilia E, Sirigu D, Mereu R, Zamboni F, Pusceddu E. A clinical operative sequence for hypnosis implementation to general anesthesia during major surgery for orthotopic liver transplantation. Ann Med Surg (Lond). 2022;80:104345.
Wolf TG, Faerber KA, Rummel C, Halsband U, Campus G. Functional changes in brain activity using hypnosis: a systematic review. Brain Sci. 2022;12(1):108.
Barabasz A, Barabasz M. Hypnotic phenomena and deepening techniques. In: Elkins G, editor. Handbook of medical and psychological hypnosis. New York, NY: Springer Publishing Company; 2016. pp. 69–76.
Barabasz A, Barabasz M. Induction technique: beyond simple response to suggestion. Am J Clin Hypn. 2016;59(2):204–13.
Bricco G, Boglione M, Moncalvo C, Bossa S, Coppolino A, Valeri L, et al. P355 the hypnotic communication use in cardiology setting. Eur Heart J Suppl. 2022;24(SupplementC):uac012342.
Casiglia E, Tikhonoff V, Giordano N, Regaldo G, Facco E, Marchetti P, et al. Relaxation versus fractionation as hypnotic deepening: do they differ in physiological changes? Int J Clin and Exp Hypn. 2012;60(3):338–55.
Dunham CM, Burger AJ, Hileman BM, Chance EA, Hutchinson AE. Bispectral index alterations and associations with autonomic changes during hypnosis in trauma center researchers: formative evaluation study. JMIR Form Res. 2021;5(5):e24044.
Lynn SJ, Kirsch I. Essentials of clinical hypnosis: an evidence-based approach. Washington: American Psychological Association; 2006.
Mazini Filho M, Savoia R, Brandão Pinto de Castro J, Moreira O, Venturini G, Curty V, et al. Effects of hypnotic induction on muscular strength in men with experience in resistance training. J Exerc Physiol Online. 2018;21(1):52–61.
Montgomery GH, Green JP, Erblich J, Force J, Schnur JB. Common paraverbal errors during hypnosis intervention training. Am J Clin Hypn. 2021;63(3):252–68.
Diamond SG, Davis OC, Howe RD. Heart-rate variability as a quantitative measure of hypnotic depth. Int J of Clin and Exp Hypn. 2007;56(1):1–18.
Pekala RJ, Kumar VK, Maurer R, Elliott-Carter NC, Moon E. How deeply hypnotized did I get? Predicting self-reported hypnotic depth from a phenomenological assessment instrument. Int J of Clin and Exp Hypn. 2006;54(3):316–39.
Pekala RJ, Maurer R, Kumar VK, Elliott NC, Masten E, Moon E, et al. Self-hypnosis relapse prevention training with chronic drug/alcohol users: effects on self-esteem, affect, and relapse. Am J Clin Hypn. 2004;46(4):281–97.
Watkins JG, Barabasz A. Advanced hypnotherapy. Routledge; 2008.
Almeida-Marques FX, Sánchez-Blanco J, Cano-García FJ. Hypnosis is more effective than clinical interviews. Int J Clin Exp Hypn. 2018;66(1):3–18.
De Benedittis G. Neural mechanisms of hypnosis and meditation-induced analgesia: a narrative review. Int J Clin Exp Hypn. 2021;69(3):363–82.
Jensen M, Battalio S, Chan J, Edwards K, Day M, Sherlin L, et al. Use of neurofeedback and mindfulness to enhance response to hypnosis treatment in individuals with multiple sclerosis: results from a pilot randomized clinical trial. Int J Clin Exp Hypn. 2018;66(3):231–64.
Cordi MJ, Schlarb AA, Rasch B. Deepening sleep by hypnotic suggestion. Sleep. 2014;37(6):1143–52.
Pekala RJ, Creegan K. States of consciousness, the qEEG, and noetic snapshots of the brain/mind interface: a case study of hypnosis and sidhi meditation. OBM Integr Complem Med. 2020;5(2):1–35.
De Pascalis V, Santarcangelo EL. Hypnotizability-related asymmetries: a review. Symmetry (Basel). 2020;12(6):1015.
De Pascalis V, Ray WJ, Tranquillo I, D’Amico D. EEG activity and heart rate during recall of emotional events in hypnosis: relationships with hypnotizability and suggestibility. Int J Psychophysiol. 1998;29(3):255–75.
Deivanayagi S, Manivannan M, Fernandez P. Spectral analysis of EEG signals during hypnosis. Int J Syst Cybern Inf. 2007;4:75–80.
Freeman R, Barabasz A, Barabasz M, Warner D. Hypnosis and distraction differ in their effects on cold pressor pain. Am J Clin Hypn. 2000;43(2):137–48.
Jamieson GA, Burgess AP. Hypnotic induction is followed by state-like changes in the organization of EEG functional connectivity in the theta and beta frequency bands in high-hypnotically susceptible individuals. Front Hum Neurosci. 2014;8:528.
Jensen M, Adachi T, Hakimian S. Brain oscillations, hypnosis, and hypnotizability. Am J Clin Hypn. 2015;57(3):230–53.
Kropotov JD, Quantitative. EEG, event-related potentials and neurotherapy. Academic Press; 2009.
Paoletti P, Dotan Ben-Soussan T, Glicksohn J. Inner navigation and theta activity: from movement to cognition and hypnosis according to the sphere model of consciousness. In: Mordeniz C, editor. Hypnotherapy and hypnosis. IntechOpen; 2020. https://doi.org/10.5772/intechopen.92755.
Vaitl D, Birbaumer N, Gruzelier J, Jamieson GA, Kotchoubey B, Kübler A, et al. Psychobiology of altered states of consciousness. Psychol Bull. 2005;131(1):98–127.
Krol LR, Andreessen LM, Zander TO. Passive brain-computer interfaces: a perspective on increased interactivity. In: Nam CS, Nijholt A, Lotte F, editors. Brain-computer interfaces handbook: technological and theoretical advances. Boca Raton, FL, USA: CRC Press; 2018. pp. 69–86.
Zander TO, Andreessen LM, Berg A, Bleuel M, Pawlitzki J, Zawallich L, et al. Evaluation of a dry EEG system for application of passive brain-computer interfaces in autonomous driving. Front Hum Neurosci. 2017;11:78.
Barrett D. Hypnosis and empathy: a complex relationship. Am J Clin Hypn. 2016;58(3):238–50.
Barrett D. Fantasizers and dissociaters: two types of high hypnotizables, two different imagery styles. In: Kunzendorf RG, Spanos NP, Wallace B, editors. Hypnosis and imagination. 1st ed. Routledge; 1996. pp. 123–35.
Barrett D. Fantasizers and dissociaters: data on two distinct subgroups of deep trance subjects. Psychol Rep. 1992;71(3):1011–4.
Barber TX. A deeper understanding of hypnosis: its secrets, its nature, its essence. Am J Clin Hypn. 2000;42(3–4):208–72.
Finn MTM, McKernan LC. Styles of experiencing hypnosis: a replication and extension study. Int J Clin Exp Hypn. 2020;68(3):289–305.
Cardeña E. The phenomenology of deep hypnosis: quiescent and physically active. Int J Clin Exp Hypn. 2005;53(1):37–59.
McGeown WJ, Mazzoni G, Vannucci M, Venneri A. Structural and functional correlates of hypnotic depth and suggestibility. Psychiatry Res Neuroimaging. 2015;231(2):151–9.
WinEEG User Manual. https://manualzz.com/doc/7137615/wineeg-user-manual---bio-medical-instruments--inc.#p1. Accessed 10 May 2023.
Delorme A, Makeig S. EEGLAB: an open source toolbox for analysis of single-trial EEG dynamics including independent component analysis. J Neurosci Methods. 2004;134(1):9–21.
Renard Y, Lotte F, Gibert G, Congedo M, Maby E, Delannoy V, et al. OpenViBE: an open-source software platform to design, test, and use brain–computer interfaces in real and virtual environments. Presence (Camb). 2010;19:35–53.
Roy RN, Bonnet S, Charbonnier S, Campagne A. Mental fatigue and working memory load estimation: interaction and implications for EEG-based passive BCI. Annu Int Conf IEEE Eng Med Biol Soc. 2013;2013:6607–10.
Kostenko A, Rauffet P, Coppin G. Supervised classification of operator functional state based on physiological data: application to drones swarm piloting. Front Psychol. 2022;12:770000.
Liu Q, Wu Y. Supervised learning. In: Seel NM, editor. Encyclopedia of the sciences of learning. Boston, MA: Springer US; 2012. pp. 3243–5.
Aydemir Ö. Common spatial pattern-based feature extraction from the best time segment of BCI data. Turk J Elec Eng Comp Sci. 2016;24(5):3976–86.
Bird JJ, Buckingham CD, Ekárt A, Faria DR. Mental emotional sentiment classification with an EEG-based brain-machine interface. 2019. http://jordanjamesbird.com/publications/Mental-Emotional-Sentiment-Classification-with-an-EEG-based-Brain-machine-Interface.pdf. Accessed 5 May 2023.
Blankertz B, Tomioka R, Lemm S, Kawanabe M, Muller K. Optimizing spatial filters for robust EEG single-trial analysis. IEEE Signal Process Mag. 2008;25(1):41–56.
Ramoser H, Muller-Gerking J, Pfurtscheller G. Optimal spatial filtering of single trial EEG during imagined hand movement. IEEE Trans Rehabil Eng. 2000;8(4):441–6.
Kohavi R, Provost F. Glossary of terms. Special issue of applications of machine learning and the knowledge discovery process. Mach Learn. 1998;30(2/3):271–4.
How to cross-validate better. http://openvibe.inria.fr/tutorial-how-to-cross-validate-better/. Accessed 11 May 2023.
Santos MS, Soares JP, Abreu PH, Araújo H, Santos J. Cross-validation for imbalanced datasets: avoiding overoptimistic and overfitting approaches [Research Frontier]. IEEE Comput Intell Mag. 2018;13(4):59–76.
van Driel J, Olivers CNL, Fahrenfort JJ. High-pass filtering artifacts in multivariate classification of neural time series data. J Neurosci Methods. 2021;352:109080.
Barabasz A, Watkins JG. Hypnotherapeutic techniques. Routledge; 2005.
Bird JJ, Manso LJ, Ribeiro EP, Ekart A, Faria DR. A study on mental state classification using EEG-based brain-machine interface. http://jordanjamesbird.com/publications/A-Study-on-Mental-State-Classification-using-EEG-based-Brain-Machine-Interface.pdf. Accessed 5 May 2023.
Acknowledgements
We would like to thank the patients who participated in the study. We also thank Gelera U. Utemisheva, Svetlana V. Khetrik, Valentin A. Kuznetsov, Tatiana E. Zhukova, and Michael P. for organisational assistance.
Funding
The work has not been funded by any organization.
Author information
Authors and Affiliations
Contributions
N.V.O conceived the study. N.V.O and I.E.S conducted the data collection and processing. N.V.O, P.L.N.N, T.G.S, and I.A.M analysed the data and led the writing of the manuscript. P.L.N.N supervised the study and reviewed the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
This study was performed in accordance with the principles of the Declaration of Helsinki. Ethical approval was obtained from the Ethical Committee of the Association of Experts in the Field of Clinical Hypnosis (AEFCH, Saint Petersburg). Written informed consent was obtained from all participants.
Consent for publication
Not applicable.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Obukhov, N.V., Naish, P.L., Solnyshkina, I.E. et al. Real-time assessment of hypnotic depth, using an EEG-based brain-computer interface: a preliminary study. BMC Res Notes 16, 288 (2023). https://doi.org/10.1186/s13104-023-06553-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13104-023-06553-2