
Abstract
Background
Toxoplasmosis is a widely distributed zoonotic disease, caused by the protozoan parasite Toxoplasma gondii. T. Infections can result in stillbirths, abortions or congenital defects during pregnancy, as well as toxoplasmic encephalitis in HIV/AIDS patients. This study aimed to determine the seroprevalence and risk factors for T. gondii infection in women seeking antenatal and medical care in the locality of Njinikom, North West of Cameroon.
Methods
We conducted a cross-sectional study from August to December 2014 consecutively enrolling 178 consenting women aged 15 to 49 years attending antenatal care or medical check-ups at the hospital. A questionnaire survey was administered to study participants and potential risk factors for Toxoplasma exposure sought. Venous blood was collected and serum from each participant analysed for T. gondii infection as evidenced by the presence of anti-T. gondii IgG and IgM antibodies detected using the indirect enzyme-linked immunosorbent assay (ELISA) technique. The proportion of anti-T. gondii antibody positivity calculated as the percentage of antibody seropositivity to T. gondii antigens. Predictors of T. gondii infection were analysed by univariate and multivariate regression and association with T. gondii seropositivity assessed. Epi-Info 3.5.4 was used for statistical analyses. A p < 0.05 was considered significant for all analyses.
Results
The seroprevalence of anti-T. gondii antibodies (IgM or IgG) were 54.5 % (97/178). Among seropositive women, 88.7 % (86/97), 30.9 % (30/97), and 19.6 % (19/97) were respectively seropositive for IgG antibody, IgM antibody and both IgM and IgG antibodies. Among the risk factors evaluated, only the consumption of raw or undercooked meat (p = 0.02) was observed to be an independent risk factor of T. gondii infection. The consumption of unwashed vegetables and fruits was significant (p = 0.01) only with simple logistic regression analysis.
Conclusions
Our findings suggest recent T. gondii exposure is high in our study population, and may constitute a significant risk factor for stillbirths, abortions or congenital defects during pregnancy in women attending antenatal care, or toxoplasmic encephalitis in those who are immunosuppressed such as in HIV/AIDS. Education and screening of HIV-positive individuals and pregnant women for T. gondii infection may be important primary prevention strategies in this population.
Similar content being viewed by others

Background
Toxoplasmosis is one of the common worldwide parasitic zoonosis, caused by the apicomplexa protozoan Toxoplasma gondii [1]. This parasite has cats as the definitive host, and warm-blooded animals as intermediate hosts [2]. T. gondii infects up to a third of the world’s population [3] and is reported to be an opportunistic parasitic infection in immune compromised hosts [4]. High prevalence of the infection has been reported among pregnant women and women of childbearing age from different parts of the world [5]. The infection occurs widely, and varies depending on social and cultural habits, geographic factors, climate, and route of transmission. It has been reported that the prevalence is higher in warm and humid areas [6].
Toxoplasma gondii is transmitted to humans through ingestion of oocysts in water, food or soil contaminated with cat’s faeces, or by eating raw or undercooked meat containing cysts [7–10], and women can transmit the infection through the placenta to their unborn foetus. Other infectious pathways are blood transfusion, and organs transplantation [11].
In the majority of immune competent subjects, the infection is asymptomatic [3, 12] and frequently results in the chronic persistence of cysts within the host tissues. The cysts normally lie dormant, probably for life [12]. But, in immune compromised states such as in HIV infections, subjects are at risk of developing acute toxoplasmosis due to reactivation of the organism if their CD4 cell count decreases below 200 cells/μL [13–15]. Moreover, in up to 10 % of HIV-infected immune compromised individuals, it causes cervical lymphadenopathy or ocular disease [16]. When the infection occurs in pregnant women, it can cause severe disease symptoms including toxoplasmic encephalitis, blindness, foetal abnormalities, abortion and even stillbirth [3, 17]. Toxoplasmosis has also been proven to be the cause of abortion and infertility in women [18].
In Cameroon, the few studies on toxoplasma have been limited to urban areas. For example, the seroprevalence of T. gondii was shown to be high among HIV/AIDS patients in the Yaoundé teaching hospital (69.9 %) [19] and pregnant women who consulted at the Department of Gynaecology in the Douala general hospital (70 %) [20]. 71.8 % prevalence was also observed among women attending antenatal care in Limbe, along the coastal region of Cameroon [21]. The study in Douala observed that the consumption of raw vegetables and untreated water were the main risk factors associated with toxoplasmosis in pregnant women [20].
The aim of this study was therefore to determine the seroprevalence of anti-T. gondii antibodies in HIV-infected and uninfected women of child-bearing age attending the antenatal clinic and medical check-ups and to identify the risk factors associated with T. gondii infection, within the rural locality of Njinikom, North West Region of Cameroon.
Methods
Study design
A cross-sectional study was carried out from August to December 2014 in St. Martin de Porres Catholic General Hospital Njinikom, North West Region of Cameroon.
Study site and population
The St. Martin de Porres Catholic General Hospital Njinikom, is a private health care institution run by the Sisters of the Franciscan Congregation whose convent is located near the hospital. The hospital was created in 1963. This hospital has an HIV treatment centre, and the majority of services rendered are in the domains of gynaecology, orthopaedics and general surgery. The hospital is situated at about 48 km from Bamenda—the regional capital of the North West Region of Cameroon. About 75 % of the women in this locality depend on agriculture for their livelihoods.
Participants in this study were volunteer women of child-bearing age (HIV-infected or uninfected) attending antenatal or medical check-ups at the hospital and who duly provided consent by signing or placing their thumbprint on the consent form. Female nurses of child-bearing age working in the hospital and other carers of patients at the Hospital were also included in this study.
Questionnaire administration and sample collection
Participants of this study were each provided with a structured questionnaire to fill. Those who could not read were assisted to fill the questionnaires by the laboratory technician or antenatal care nurse. The questionnaires contained simple closed ended questions regarding known risk factors of Toxoplasma exposure in addition to socio-demographic information.
Five millilitres of venous blood were collected into two tubes pre-labelled with an anonymised patient codes. The blood from the EDTA containing tubes was immediately tested for the presence of HIV antibodies using Determine (Alere Determine™ HIV-1/2) test strips according to manufacturer’s instructions. The CD4 cell count for women who were HIV positive was also measured. The second blood sample was allowed to clot completely before centrifugation at 3000 rpm for 15 min to obtain serum. Serum was separated from the clot into tightly screwed microfuge tubes and stored at −20 °C. These frozen sera were later tested for the presence of Toxoplasma gondii antibodies.
Serological test for T. gondii antibodies
The presence of T. gondii antibodies in the participants’ sera was determined using an indirect Enzyme-Linked Immunosorbent Assay (ELISA). This was done using the AccuDiag™ Toxo IgM and IgG ELISA Kits (The Diagnostic Automation/Cortez Diagnostics, Inc. Toxoplasma gondii [Toxo] IgM and IgG Enzyme-Linked Immunosorbent Assay [ELISA]). The Toxo IgM ELISA Kits had a specificity of 100 % and a sensitivity of 100 %, while the Toxo IgG ELISA Kits had a specificity of 100 % and a sensitivity of 95.3 %. Calibrator and controls were run with each test assay. The optical densities (OD) obtained were used to calculate the cut-off calibrator value and the Immune Status Ratio (ISR). The interpretation of results was done with respect to the ISR values. For IgM, a sample with OD ≤ 0.90 was considered negative, OD ≥ 1.10 was considered positive, and OD = 0.91–1.09 was considered indeterminate. For IgG, a sample with OD < 0.90 was considered negative, OD > 1.10 was considered positive, and OD within 0.91–1.09 was considered indeterminate.
Ethical consideration
Ethical clearance for this study was obtained from the Ethics Review and Consultancy Committee of the Cameroon Bioethics Initiative (CAMBIN) under the reference number CBI/283/ERCC/CAMBIN of August 06th, 2014. An authorisation to collect and analyse blood samples was also obtained from the St. Martin de Porres Catholic Mission Hospital Njinikom. All participants were duly informed of the study goals, procedures, potential harm and benefits, cost as well as the finality of the study. They willingly provided informed consent either by signing or placing their thumbprint on the consent form after being satisfied with responses to all questions asked the investigator. Women less than 21 years provided assent and consent from guardian was also sought for these women. Information was provided in English, French or interpreted in the local dialect by a volunteer independent of the study team. Participants’ blood samples and results were anonymised. Left over blood samples were destroyed according to hospital biosafety procedures.
Data management and statistical analysis
Data were entered into Microsoft Excel program and then transferred to Epi Info 3.5.4 statistical program. The seroprevalence of toxoplasmosis was calculated as the proportion of serologically positive anti-T. gondii samples among all samples tested at 95 % confidence interval (CI). A multivariate logistic regression model was used to investigate the association between the potential risk factors for toxoplasmosis as defined by seropositivity for Toxoplasma gondii antibodies of any kind. Variables used in the multiple regression were selected through step-wise backward elimination using a 20 % cut-off (p to remove). The strength of associations was measured using the odds ratio (OR) at 95 % CI. The Chi-square test was used for group comparisons. Statistical significance was set at 5 % and all the associations that showed a p < 0.05 were considered significant.
Results
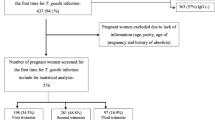
A total of 350 eligible women were approached and 178 women aged 15 to 49 years provided consent for this study. The mean age of participating women was 31.13 ± 8.12 years. The majority of the women were aged between 26 and 35 years (70/178, 39.3 %). 53.9 % (96/178) of the women were married, and 6.2 % (11/178) never went to school. Among the study participants, only 5.6 % (10/178) had cats in their homes, while 30.3 % (54/178) frequently come in contact with cats because of neighbours owning cats. A total of 59.6 % (106/178) consumed raw or undercooked meat. 5.1 % (9/178), 65.7 % (117/178), and 73.1 % (130/178) women consumed raw milk, raw unwashed vegetable or fruits, and untreated drinking water respectively. Regarding the participants residential area, 5.1 % (9/178) of the study participants lived in an urban area, while 94.9 % (169/178) lived in a rural area. Those women who lived in cemented and non-cemented floor houses were 38.2 % (68/178), and 61.8 % (110/178) respectively. Only 1.7 % (3/178) knew about toxoplasmosis (Table 1). Out of the 178 women recruited in this study, 50.6 % (90/178) were HIV-positive, 49.4 % (88/178) were HIV-negative, 50.6 % (90/178) were pregnant and 49.4 % (88/178) were not pregnant. Of the 90 HIV-positive participants only 3.3 % (3/90) had a CD4 count less than 200 cells/mm3 and 84.5 % (76/90) HIV-infected participants lived on HAART (Table 1).
Prevalence of anti-Toxoplasma antibodies in the study population
The combined seroprevalence of anti-T. gondii antibodies among the 178 women of child-bearing age in our study area was calculated to be 54.5 % (97/178). Among the seropositive women, 86 were seropositive for IgG antibodies, 30 were seropositive to IgM antibodies, and 19 were seropositive for both IgG and IgM antibodies giving a prevalence of 48.3, 16.9 and 10.7 % respectively (Table 2).
Table 2 also illustrates that the seroprevalence of antibodies to T. gondii was slightly higher in HIV-negative (55.7 %, [49/88]), than in HIV-positive (53.7 % [48/90]) participants (p > 0.05). Seroprevalence of anti-T. gondii IgG antibody was 47.8 % (43/90) in HIV-positive participants, and slightly lower than in HIV-negative participants (48.9 %, [43/88]). On the other hand, 12.2 % (11/90) of HIV-positive against 9.1 % (8/88) of HIV-negative women were seropositive to both IgG and IgM antibodies to T. gondii. Similarly, a higher seroprevalence of IgM antibody to T. gondii was found in HIV-positive (17.8 %, [16/90]), than in HIV-negative (15.9 %, [14/88]) women. A total of 55.7 % (49/88) non-pregnant women were seropositive to anti-T. gondii antibodies. This was slightly higher than the 53.3 % (48/90) pregnant women also seropositive to anti-T. gondii antibodies (Table 2).
Risk factors for Toxoplasma seropositivity
As shown in Table 3, simple logistic regression analysis with suspected variable indicated that the consumption of raw or undercooked meat (p = 0.01) and the consumption of raw unwashed vegetables and fruits (p = 0.01) were predictors of toxoplasmosis seropositivity irrespective of the antibody type. However, results of multiple logistic regression analysis of selected variables as shown in Table 4 showed that only the consumption of raw or undercooked meat (p = 0.02) was an independent predictor of toxoplasmosis seropositivity irrespective of the antibody type. No significant association was found between Toxoplasma gondii seropositivity and HIV status (p = 0.18), cat ownership (p = 0.91), contact with cats (p = 0.31) and residential area (p = 0.16).
Discussion
Toxoplasmosis is a curable but potentially fatal disease [22]. Over the years, infection with the protozoan parasite Toxoplasma gondii has been proven to be one of the most common parasitic infections of man and other warm-blooded animals [2]. In this study, we sought to investigate Toxoplasma infection, as evidenced by anti-Toxoplasma antibodies in the serum of women of child bearing age in a rural locality in Cameroon. Our findings revealed that the seroprevalence of anti-T. gondii antibodies among the women of child-bearing age in this study was 54.5 %. This prevalence was similar to that obtained among women of child-bearing age in Timis, Romania (57.6 %) [23], but far lower than that found in women of child-bearing age in Central Ethiopia (81.4 %) [24]. This lower prevalence could be attributed to a lower cat density (10/178, Table 1) and consequent oocysts shedding and a lower consumption of unpasteurised milk in our study area. The seroprevalence obtained in this study is also far lower than that obtained in other parts of Cameroon. Indeed, a prevalence of 77.1 % was observed in pregnant women in Yaoundé [25], 70 % in pregnant women in Douala [20], 69.9 % in HIV/AIDS patients in Yaoundé [19], while a prevalence of 71.8 % was observed among pregnant women in Limbe [21]. These geographic differences in prevalence rates may be explained by differences in rural/urban setting since exposure and the main sources of infection appear to be the same. This might explain differences in risk factors of Toxoplasma seropositivity as well as climatic changes. Our study population was mainly from a rural area.
The seroprevalence of anti-T. gondii IgG antibody in HIV-positive participants was 47.8 % (43/90). This was not significantly different from the 48.9 % (43/88) obtained in the HIV-negative group in this same study population (X 2 = 1.3632, p = 0.1728). This results were similar to the 42.1 % (56/133) obtained among HIV/AIDS patients in the university teaching hospital in Yaoundé [19], although the number of HIV patients in our study was smaller. Similarity in the prevalence of Toxoplasma seropositivity among HIV-infected or uninfected women in our study conforms to what has been reported by researchers in Malaysia [26], United States of America [27], and Ethiopia [28]. However, another study in Ethiopia showed a significantly higher prevalence of anti-Toxoplasma gondii antibodies (87.4 % vs 70.29 %, P = 0.003) in HIV-positive pre-antiretroviral therapy (pre-ART) individuals than in HIV-negative blood donors [10]. Indeed, in our study, up to 84.5 % (76/90) of the HIV positive study participants were on highly active antiretroviral therapy (HAART), and only three participants had CD4 counts less than 200cells/mm3 of whole blood. This indicate the benefit of HAART treatment which helps to decrease the viral load and improve CD4+ cell counts and consequently boosts the immune system of the host, with the added benefit of reducing the likelihood of reactivation of latent T. gondii infections [1, 29, 30]. We found a non-significant higher IgM antibodies in HIV positive women compared to HIV negative women, further confirming this assertion.
The seroprevalence of anti-T. gondii antibodies was higher in non-pregnant women (55.7 %, [49/88]) compared to pregnant women (53.3 %, [48/90]) irrespective of HIV status, although not significantly different. Among the 90 pregnant women enrolled in this study, 48.9 % (44/90) and 13.3 (12/90) were positive for anti-T. gondii IgG and IgM antibodies respectively. These prevalence values were significantly low compared to 71.8 and 67.6 % respectively obtain among pregnant women in the Limbe health district in the South West Region of Cameroon [21].
The consumption of raw or undercooked meat [p = 0.0184] was significant a risk factor associated with T. gondii infection in the univariate and multivariate analysis (Tables 3a and 4). In addition, consumption of unwashed vegetables or fruits was observed to be significantly associated with toxoplasma seropositivity in the univariate analysis, although it was only marginally significant in the multivariable analysis Table 4. Similar results have been observed in studies done in Mexico [31], Ethiopia [10], and Sudan [32], whereas studies done in Douala-Cameroon [20], and Thailand [33], showed a significant association between T. gondii infection and consumption of untreated water only. Although domestic cats are probably the major source of contamination [1, 34], cat ownership and contact with cats were not found to be significantly associated with T. gondii infection [9, 13]. Indeed, only 6 % of the total study population reported having cats at home. Sporulated oocysts survive in moist soil for months to years [35]. Though no significance association was found between T. gondii infection and untreated water, it is likely that oocysts might have been present in some of the untreated water sources in our study area. Poor sanitation methods with the poor quality water used to wash raw meat at abattoirs or vegetables sold in the market, might have led to their contamination with oocysts.
Our study however should be interpreted with some caution. Our sample size was small and conclusions from the present study must be measured. It is likely that we may obtain different results with increased sample size. The number of equivocal results obtained using the selected ELISA technique in some cases was high, and difficult to interpret with the absence of reference testing facilities for toxoplasmosis in or around our study area. This could affect our results by increasing or decreasing the observed prevalences. Secondly, we observed an increase in risk of seropositivity with stage in pregnancy, but we did not follow up those women who were seropositive to study delivery outcomes or health status of their children. Thirdly, we may have obtained a different result if we considered sampling only women of child bearing age at the antenatal service. However, less than 30 % of our study population was sampled among those who came for medical check-up at the hospital, making our results more likely to reflect what we desired to investigate.
Conclusions
Toxoplasma gondii infection appears to be a public health concern in Njinikom, with a global antibody seroprevalence of 54.5 % among women of child bearing age attending antenatal or outpatient medical care in our study area. In this study, recent infections were found in 16.9 % of the study population while up to 10.7 % of patients were reactivating and there was no difference between pregnant and non-pregnant or HIV negative or HIV positive women. Consumption of raw or undercooked meat and of unwashed vegetables were observed to be risk factors for T. gondii infection among women of childbearing age in the locality of Njinikom, North West Region of Cameroon. Only 1.7 % (3/178) of the study participants knew about toxoplasmosis. Education on toxoplasmosis during antenatal care or in HIV treatment centres and screening for recent Toxoplasma exposure may be strategies for primary prevention of toxoplasmosis and its devastating outcomes in pregnancy or among HIV patients.
References
Tenter AM, Heckeroth AR, Weiss LM. Toxoplasma gondii: from animals to humans. Int J Parasitol. 2000;30:1217–58.
Dubey JP. Toxoplasmosis of animals and humans. 2nd ed. Beltsville: CRC Press; 2010.
Montoya JG, Liesenfeld O. Toxoplasmosis. Lancet. 2004;363:1965–76.
Ferreira SM, Borges SA. Some aspects of protozoan infections in immune compromised patients—a review. Bio Line International System. 2002;97(4):443–57.
Pappas G, Roussos N, Falagas ME. Toxoplasmosis snapshots: global status of Toxoplasma gondii seroprevalence and implications for pregnancy and congenital toxoplasmosis. Int J Parasitol. 2009;39:1385–94.
Studeničová C, Benčaiová G, Holková R. Seroprevalence of Toxoplasma gondii antibodies in a healthy population from Slovakia. Eur J Intern Med. 2006;17:470–3.
Fayer R, Dubey JP, Lindsay DS. Zoonotic protozoa: from land to sea. Trends Parasitolol. 2004;20:531–6.
Dubey JP. Toxoplasmosis—a waterborne zoonosis. Vet Parasitol. 2004;126(1–2):57–72.
Dubey JP. The history and life cycle of Toxoplasma gondii. In: Weiss LM, Kim K, editors. Toxoplasma gondii, the model apicomplexan: perspectives and methods, 2nd edn. Waltham, MA: Elsevier; 2013. p. 1–14.
Walle F, Kebede N, Tsegaye A, Kassa T. Seroprevalence and risk factors for Toxoplasmosis in HIV infected and non-infected individuals in Bahir Dar, Northwest Ethiopia. Parasit Vectors. 2013;6:15.
CDC. Parasites—Toxoplasmosis (Toxoplasma infection). 2013. http://www.cdc.gov/parasites/toxoplasmosis/gen_info/index.html. Accessed 26 Aug 2014.
Malla N, Sengupta C, Dubey ML, Sud A, Dutta U. Antigenaemia and antibody response to Toxoplasma gondii in human immunodeficiency virus infected patients. Br J Biomed Sci. 2005;28:104–9.
Martinez E, Mago H, Rocha R, Pacheco M. Epidemiological findings and prevalence of Toxoplasma gondii antibodies in HIV-positive patients in a Venezuelan hospital. Valencia Int Conf AIDS. 2002;7–12:14.
Nissapatorn V, Lee C, Quek KF, Leong CL, Mahmud R, Abdullah KA. Toxoplasmosis in HIV/AIDS patients: a current situation, Japan. J Infect Dis. 2004;57(4):160–5.
Jayawardena S, Singh S, Burzyantseva O, Clarke H. Cerebral toxoplasmosis in adult patients with HIV infection. Clin Med J Resid Hosp Phys. 2008;44(7):17–24.
Walker M, Zunt JR. Parasitic central nervous system infections in immunocompromised hosts. Clin Infect Dis. 2005;40(7):1005–15.
Cook AJ, Gilbert RE, Buffolano W, Zufferey J, Petersen E, Jenum PA, Foulon W, Semprini AE, Dunn DT. Sources of Toxoplasma infection in pregnant women: European multicentre case-control study. European Research Network on Congenital Toxoplasmosis. BMJ. 2000;321:142–7.
Abida M, Meher R, Fatima K, Nazia K, Tamkin R, Haris MK. Toxoplasma gondii in women with bad obstetric history and infertility: a five-year study. Asian Pac J Trop Dis. 2014;4:236–9.
Assob JCN, Njunda AL, Nsagha DS, Kamga HL, Weledji PE, Che VB. Toxoplasma antibodies amongst HIV/AIDS patients attending the University Teaching Hospital Yaoundé, in Cameroon. Afr J Clin Exp Microbiol. 2011;12(3):1119–23.
Njunda AL, Assob JCN, Nsagha DS, Kamga HL, Nde PF, Yugah VC. Seroprevalence of Toxoplasma gondii infection among pregnant women in Cameroon. J Public Health Africa. 2011;2:e24.
Ndassi DV, Kamga HLF. The seroprevalence of toxoplasmosis and contributing factors among pregnant women attending antenatal consultation in the Limbe Health District, Cameroon. Afr J Integr Health. 2014;04(1):31–6.
Negash T, Tilahun G, Medhin G. Seroprevalence of Toxoplasma gondii in Nazareth town, Ethiopia. East Afr J Public Health. 2008;5:211–4.
Olariu TR, Darabus GH, Cretu O, Jurovits O, Giura E, Erdelean V, Marincu I, Iacobiciu I, Petrescu C, Koreck A. Prevalence of Toxoplasma gondii antibodies among women of childbearing age in Timis County. Lucrări Stiinłifice Medicină Veterinară. 2008;41:367–71.
Gebremedhin EZ, Abebe AH, Tessema TS, Tullu KD, Medhin G, Vitale M, Marco VD, Cox E, Dorny P. Seroepidemiology of Toxoplasma gondii infection in women of child-bearing age in central Ethiopia. BMC Infect Dis. 2013;13:101.
Ndumbe PM, Andela A, Nkemnkeng-Asong J, Watonsi E, Nyambi P. Prevalence of infections affecting the child among pregnant women in Yaounde, Cameroon. Med Microbiol Immunol. 1992;181(3):127–30.
Nissapatorn V, Kamarulzaman A, Init I, Tan LH, Rohela M, Norliza A, Chan LL, Latt HM, Anuar AK, Quek KF. Seroepidemiology of toxoplasmosis among HIV-infected patients and healthy blood donors. Med J Malaysia. 2002;57:304–10.
Falusi O, French AL, Seaberg EC, Tien PC, Watts DH, Minkoff H, Piessens E, Kovacs A, Anastos K, Cohen MH. Prevalence and predictors of Toxoplasma seropositivity in women with and at risk for human immunodeficiency virus infection. Clin Infect Dis. 2002;35:1414–7.
Shimelis T, Tebeje M, Tadesse E, Tegbaru B, Terefe A. Sero-prevalence of latent Toxoplasma gondii infection among HIV-infected and HIV-uninfected people in Addis Ababa, Ethiopia: a comparative cross-sectional study. BMC Res Notes. 2009;2:213.
Sukthana Y. Toxoplasmosis: beyond animals to humans. Trends Parasitol. 2006;22:137–42.
Khirwadkar MA, Kher JR. Study of serum immunoglobulins in normal pregnancy. Indian J Physiol Pharmacol. 1991;35(1):69–70.
Alvarado-Esquivel C, Sifuentes-Alvarez A, Narro-Duarte SG, Estrada-Martínez S, Díaz-García JH, Liesenfeld O, Martínez-García SA, Canales-Molina A. Seroepidemiology of Toxoplasma gondii infection in pregnant women in a public hospital in northern Mexico. BMC Infect Dis. 2006;6:17.
Khalil M, Kodym P, Maly M, Intisar E, Rayah I. Environmental and food habitat risk factors associated with Toxoplasma gondii Infection in rural women in Sudan. Int J Curr Microbiol Appl Sci. 2014;3(2):208–22.
Andiappan H, Nissapatorn V, Sawangjaroen N, Chemoh W, Lau YL, Kumar T, Onichandran S, Suwanrath C, Chandeying V. Toxoplasma infection in pregnant women: a current status in Songklanagarind hospital, Southern Thailand. Parasit Vectors. 2014;7:239.
Dubey JP. Oocyst shedding by cats fed isolated bradyzoites and comparison of infectivity of bradyzoites of the VEG strain Toxoplasma gondii to cat sand mice. J Parasitol. 2001;87:215–9.
Dubey JP, Beattie CP. Toxoplasmosis of animals and man. Boca Raton: CRC Press; 1988. p. 220.
Authors’ contributions
ECW, IMA and CBT conceived the study. ECW and LFS carried out sample and data collection. IMA, WAE, LFS and ECW participated in analysis of the samples, data management and statistics. ECW and IMA drafted the manuscript. All authors reviewed the manuscript the final version prior to submission. All authors read and approved the final manuscript.
Acknowledgements
We wish to thank all the participants who sacrificed their time and donated their blood for this study. We also thank particularly the Matron, Doctors, and Nurses of St. Martin De Porres Catholic Hospital Njinikom for their contributions and assistance during sample collection and analysis.
Competing interests
The authors declare that they have no competing interests.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Wam, E.C., Sama, L.F., Ali, I.M. et al. Seroprevalence of Toxoplasma gondii IgG and IgM antibodies and associated risk factors in women of child-bearing age in Njinikom, NW Cameroon. BMC Res Notes 9, 406 (2016). https://doi.org/10.1186/s13104-016-2206-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13104-016-2206-0