
Abstract
Background
Heart disease is one of the leading causes of death in Canada. Many heart disease patients are referred for cardiac rehabilitation, a multidisciplinary outpatient program often consisting of exercise training. Cardiac rehabilitation has been proven to be a successful secondary preventative measure in reducing mortality and improving overall health in heart disease patients, and its completion is important for both sexes as there is growing evidence that women benefit as much as men, if not more, with regard to mortality. It is important to note that previous studies have shown that healthy men and women respond differently to aerobic and resistance training, possibly due to hormones, body composition, autonomic and/or cardiovascular differences. However, evaluating sex differences in the efficacy of standard cardiac rehabilitation programs has not yet been fully explored with many studies investigating clinical or anthropometric data but not physiological outcomes. This systematic review aimed to investigate physiological differences in male and female heart disease patients after cardiac rehabilitation. The inclusion criteria were purposefully broad to encompass many cardiac rehabilitation scenarios, many cardiac disease states, and various program lengths and intensities with the intention of highlighting strengths and weaknesses of the current body of literature.
Methods
To conduct a synthesis without meta-analysis, a search strategy was generated to examine the relationships between heart disease patients, a supervised exercise program, physiological outcomes, and sex differences. The review was registered (Prospero: CRD42021251614) and the following databases were searched from inception to 19 December 2023: APA PsycInfo (Ovid), CINAHL Complete (EBSCOhost), Embase (Ovid), Emcare Nursing (Ovid), Medline All (Ovid; includes PubMed non-Medline), and Web of Science Core Collection. Eighty-eight studies pertaining to fitness, metabolism, body composition, respiratory function, cardiac function and C-reactive protein underwent data extraction.
Results and conclusions
Importantly, this review suggests that men and women respond similarly to a wide-range of cardiac rehabilitation programs in most physiological variables. However, many studies discussing maximal oxygen consumption, functional capacity, six-minute walk distances, and grip strength suggest that men benefit more. Further research is required to address certain limitations, such as appropriate statistical methods and type/intensity of exercise interventions.
Similar content being viewed by others

Introduction
Heart disease (HD) is one of the leading causes of death in Canadian women with ischemic HD responsible for the vast majority at almost 14,000 deaths per year [1]. The age-standardized prevalence of ischemic HD in Canadian women is 6.3% compared to 10.0% in men [2], however, recent studies have shown that women are three times more likely to experience a major adverse cardiac event following catheterization compared to men after being diagnosed with stable angina and nonobstructive coronary artery disease (CAD) [3]. This is noteworthy considering the underrepresentation of women in clinical trials and the lack of research on sex-specific factors of cardiovascular disease in women, including prevention, diagnosis, clinical testing, treatment, and therapy [4].
Cardiac rehabilitation (CR) programs have been shown to be beneficial for both men and women with regard to mortality [5,6,7], yet significant sex differences exist in cardiovascular anatomy and physiological functioning across multiple areas of health and fitness research [8]. For example, sex-specific differences have been demonstrated when comparing men and women in terms of anatomical size, bodily composition, sympathetic or parasympathetic responses to stressors, and endocrine responses [9,10,11]. This disparity of physiological responses should be further investigated to help develop appropriate sex-specific medicine and interventions, particularly in light of evidence that men and women respond to exercise training along a different time course and to a different magnitude regarding cardiac dimensions and cardiorespiratory fitness [12]. Further, women who complete CR programs can improve mortality, however, they are less likely to be referred to CR and less likely to complete it [13,14,15]. Evidence of physiological improvements due to CR completion in women will serve to strengthen the body of evidence highlighting the benefits in women. This systematic review without meta-analysis aims to summarize pre-clinical evidence from research studies that examined the physiological responses to the completion of supervised CR exercise programs in men and women with all types of chronic HD. We aim to highlight the strengths and weaknesses of the work that has been completed to suggest improvements and future studies that need to be completed.
Methods
Data sources and search strategy
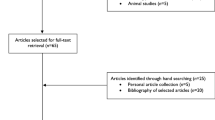
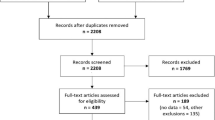
This review was conducted in accordance with the Preferred Reporting Items Systematic Reviews and Meta-Analyses [PRISMA] guidelines [16] (Fig. 1); 4884 records were retrieved from six electronic databases.

PRISMA flow diagram describing the search for relevant articles
The databases were searched from inception to 19 December 2023: APA PsycInfo (Ovid), CINAHL Complete (EBSCOhost), Embase (Ovid), Emcare Nursing (Ovid), Medline All (Ovid; includes PubMed non-Medline), and Web of Science Core Collection. The search was developed and finalized with the expertise of a librarian (MP) and utilized the PICO framework where all cardiac disease patients comprised the Population, cardiac/exercise rehabilitation was the Intervention, and gender/sex was the Comparator. To keep the results purposefully broad, no Outcome concept was added, as all physiological responses were of interest. No date or language limits were applied to the original search, but only English abstracts and articles were extracted. A hand search was conducted, but no additional articles were retrieved. The Medline search strategy is available in Supplemental Fig. 1.
Prospero and covidence registration
The review underwent Prospero registration (CRD42021251614) and was analyzed using Covidence. The review team included the primary author (JB) and four other peer reviewers for screening (TP, HJ, JD, HE). Two reviewers and the primary author would agree on a final consensus if there was a discrepancy during screening stages. Duplicates were removed, reducing the number of citations from 4884 to 2875.
Study selection and screening
Included studies focused on male and female patients with cardiac disease undergoing CR with supervised exercise. A sex difference needed to be directly investigated rather than as a covariate in the statistical model. The studies were original research studies, excluding books, abstracts, or case studies. Additionally, the methodology must have included quantitative measurements of physiological variables before and after the completion of CR. Qualitative research or research focusing on psychosocial aspects measured via questionnaires, while of great importance, were not the focus of the current investigation. A screening pilot on 25 articles was conducted to ensure consistency among reviewers.
The finalized criteria for title and abstract screening included cardiac/HD patients, an outpatient CR program which included a supervised exercise component (at-home programs with remote supervision were included), a physiological response before and after the program, and a comparison between men and women. A total of 383 articles out of 2875 titles/abstracts were included in the next stage. The full text of articles was retrieved using York University or University of Toronto Libraries. Screeners identified if there were physiological assessments at both baseline and CR completion; variables such as mortality or non-physiological variables were excluded. Sex differences were further screened at this stage. For example, many studies included both men and women and used covariate analysis for sex differences without disaggregation of the data; these studies were excluded. Lastly, any review with no original data on sex differences was also excluded. Only 88 out of the 383 progressed to the next round of screening. The JBI (Joanna Briggs Institute) quality assessment (QA) tool for cohort studies was used and modified to include an additional question regarding if empirical evidence was provided with sex difference conclusions. Two reviewers assessed the 88 papers gathered at the QA stage. No papers were eliminated based on a quality threshold.
Results
88 final articles were extracted (Table 1). Only 32 physiological variables described by ≥ 3 articles were included in Table 2 and discussed in the current review; 118 physiological variables which were described by ≤ 2 articles are listed in Supplemental Table 1. Extracted information included the title of the article, authors, population description, total number of participants, type and length of CR program, QA score, adherence rates, and statistical modelling used (Table 1). After each extraction, the papers were quantified as to whether a sex difference was or was not present per variable (Table 2). A thematic synthesis was completed after assessing all the findings and data.
The study design was characterized as one of the following: cohort study, retrospective cohort, retrospective cross-sectional, or randomized/non-randomized controlled trial. Population description presented the type of HD in the sample, with most studies investigating CAD populations. The total number of participants included the number of men and women in each population where available. Furthermore, the type of CR stated the nature of the exercise, including aerobic-only, aerobic and strength, home-based, or were not described. Typically, the articles that did not describe the exact exercise intervention were chart reviews from multiple CR programs. The length of CR specified the length of the intervention in weeks, ranging from 2 to 260 weeks. The median number of weeks of CR intervention was 12, with every intervention incorporating at least aerobic exercise (unless the intervention was unknown). The most prevalent type of CR was aerobic-only, followed by aerobic and strength exercise. The study populations generally had higher enrollment and participation rates in men compared to women, whereas adherence appeared similar between sexes.
The average QA for all articles was 11.2 ± 0.9 out of 12; 41 articles scored 12/12, 33 articles scored 11/12, 7 scored 10/12, and 7 scored 9/12. The CR completion and adherence rates were calculated and separated based on sex where available. Lastly, the type of statistics included repeated measures ANOVAs between sexes over time (i.e. “ANOVAs”; this category also included generalized linear models and generalized estimated equations analysis), t-tests over time within only one sex (i.e. “t-test”), t-tests between sexes on the change from pre- to post-CR (i.e. “t-test between deltas”), other types such as Wilcoxon signed rank test, or the statistical methods were not described. While ANCOVAs using sex only as a covariate were excluded, we retained studies that analyzed disaggregated sex data as the main variable but had other factors, such as age as a covariate.
Table 2 provides a tabular quantification of the number of articles which described each physiological variable indicating (1) a greater improvement in men, (2) only men improved, (3) greater improvement in women, (4) only women improved, (5) men and women both improved, or (6) neither men nor women improved. The variables were divided into 5 physiological groups, including fitness, metabolic measures, body composition, cardiac measures, and C-reactive protein for appropriate comparisons.
Discussion
Oxygen consumption at maximal exercise
Many studies have indicated a greater improvement in maximal oxygen consumption (VO2 max (ml/kg/min)) after CR in men compared to women [17,18,19,20,21,22,23,24,25,26], while other studies argued no sex difference in this physiological response [27,28,29,30,31,32,33,34,35,36]. Although both sets of articles have different outcomes regarding maximal oxygen consumption, the types of exercise were generally similar, including either aerobic and/or strength. Thus, the type of exercise is not a strong enough factor to predict whether men and women improve similarly. VO2max was found to only improve in men and not women in 2 additional studies [37, 38]. Kim & So utilized an extended CR program length of 36 weeks [37]. This was the longest intervention duration among articles that compared VO2max responses and could be a determining factor, as many articles stating no sex difference had interventions ranging only from 8 to 12 weeks [27, 29,30,31,32,33,34,35]. Secondly, in Willenheimer et al., only patients with heart failure (HF) were studied [38], whereas the studies concluding no sex difference looked at populations with various HDs. Thus, program length or type of HD could potentially play a role in the observation of sex differences. Interestingly, Tyni-Lenne et al. investigated patients with HF enrolled in an 8-week intervention of knee extensor exercise [39] and observed an improvement of VO2max only in women. This type of exercise is strictly experimental rather than clinical, thus it would not typically be used in isolation during a CR program. Improvements in VO2max from this exercise intervention could potentially be due to increased strength and therefore greater daily physical activity. When comparing %-predicted peak VO2, Mertens & Kavanagh found a greater improvement in men versus women after CR [40] and Kitagaki et al. found that only men improved after CR [41]; however, two studies by Trachsel et al., and Vilela et al., concluded that this percentage improves equally in both sexes [32, 33]. Mertens & Kavanagh (n = 7/20 women), Kitagaki et al. (n = 28/156 women), and Trachsel et al. (n = 19/83 women) all had small numbers of women in their investigation cohorts whereas Vilela et al. had n = 72/379. The discrepancies in this case could be due to limited sample sizes.
Functional capacity
Thirteen studies concluded that men experience a greater improvement in functional capacity (metabolic equivalents (METS)) than women post-CR [18, 26, 38, 42,43,44,45,46,47,48,49,50,51,52]. Conversely, 10 other articles observed that functional capacity improved equally in men and women after CR [30, 53,54,55,56,57,58,59,60,61,62]. When comparing the groups of studies, those that refuted a sex difference had similar CR interventions with similar duration and completion rates compared to the studies that found a sex difference. Based on the parameters collected in the scope of this review, it is undetermined what may distinguish the articles which found a sex difference from the articles which found similar responses between the sexes in functional capacity post-CR. However, as it was not in the scope of the current review, we did not extract all the information that could influence functional capacity, such as exercise intensity. This is a limitation of the current review since greater exercise intensity is associated with improved cardiorespiratory fitness and strength [63].
Six minute walk distance (6MWD)
Six studies found that men experienced a greater improvement in 6MWD after CR compared to women [39, 64,65,66,67,68]. Four other studies refuted this sex difference and reported similar improvements in 6MWD between men and women [37, 60, 69, 70]. Disease or intervention type could not predict whether there is a sex difference in 6MWD outcomes, and the two groups of articles also used similar statistics with similar adherence rates. On the contrary, 2 additional studies by Wagner et al. and Wise et al. have reported that women have a greater improvement than men in 6MWD after CR [34, 51]. Wagner et al. only investigated individuals with atrial fibrillation in a randomized controlled trial, and Wise et al. investigated patients with HF in a cohort study design. Both studies investigated an isolated HD type, which could be a determining factor as to why it was observed that women improved more than men. However, like the rest of the articles that stated no sex difference or that men improved more, these studies utilized similar training interventions with an average of 12 weeks CR, including aerobic and strength exercise.
Cardiac measures
Eight studies comparing left ventricular ejection fraction in HD patients reported equal improvements between the sexes or no improvements at all after CR [28, 32, 49, 50, 52, 71,72,73] with a single study finding that men improved to a greater degree than women (only 5 weeks of CR) [74]. While three studies investigating HR at rest showed a greater improvement in men after CR [49, 72, 75], the majority of the articles investigating HR at rest showed no sex difference or no improvement in either sex [27, 28, 30, 31, 39, 47, 50, 57, 59, 64, 71, 76,77,78,79,80]. When comparing these opposing groups of papers, there were no striking differences in terms of disease type, CR duration, adherence rates and exercise type between articles. Two further studies by Anjo et al. and Szmigielska et al. found that only men with CAD improved resting HR after 8–12 weeks of CR [52, 53] and one study by Korzeniowska-Kubacka et al. found that there was a greater improvement in women after 8 weeks of CR [81]. Anjo et al. suggested that an impaired improvement in women could have occurred since their cohort of women were significantly older.
Keteyian et al. examined HF patients and Lavie et al. examined CAD patients, yet both found that only women experienced increased maximum HR during peak exercise after CR [17, 47]. However, most studies have found no sex difference or no improvement [27, 30, 31, 47, 57, 71, 76, 79]. Every article that discussed maximal HR had purely aerobic interventions; however, no sex differences were observed in studies that had populations of multiple HD types. We suggest that the increased post-maximal HR in women observed in Keteyian et al. and Lavie et al. could be due to greater maximal effort during the stress test since maximum HR is dictated primarily by age not training. Importantly, care needs to be taken when interpreting any changes in resting, maximal, or recovery HR in cardiac disease populations considering the potential use of pharmacological agents and/or the use of pacemakers.
Kligfield et al. looked at differences in heart rate variability in HD patients and concluded that there was a greater improvement in heart rate recovery (HRR) after CR in men compared to women [46]; however, four other studies found that both men and women improve equally. The major difference between Kligfield et al. and those that observed equal improvements could be due to their unspecified statistical methods. Indeed, the studies by Anjo et al., Araya-Ramirez et al., MacMillan et al., and Soleimani et al. utilized either ANOVAs or t-tests and did not support this conclusion; instead, they expressed that men and women experienced similar changes in HRR post-CR [30, 53, 64, 76]. The vast discrepancies in statistical analysis observed throughout this systematic review (without meta-analysis) were striking. We suggest that every research group investigating sex differences in CR programs should consult a biostatistician to determine appropriate analyses.
Rate pressure product (RPP) is the product of systolic blood pressure and heart rate and is an index of myocardial oxygen consumption. At rest, while Stojanovic et al. found that only men improved their RPP, both Szmigielska et al. and Ades et al. found that either both sexes improved equally or that there was no improvement at all [52, 82, 83]. During a peak exercise test, both Cannistra et al. and Szmigielska et al. found that men improved RPP [52, 56] whereas 5 other studies found either equal improvements or no improvement at all [47, 77, 79, 82, 83]. The bulk of evidence therefore suggests that men and women do not improve or improve RPP equally after completion of CR.
Other fitness variables
Men and women responded similarly to CR in terms of absolute energy expenditure [25, 75, 84]. The remaining fitness variables included respiratory exchange ratio (RER), peak workload/lean body mass, exercise time, and grip strength. RER was found to improve more in women than men in Rengo et al., though studies by Ades et al., Trachsel et al., and Vilela et al. found equal improvements or no difference in improvement between men and women [22, 27, 32, 33]. Interestingly, in Rengo et al., the CR intervention included high-intensity interval training compared to the other studies that followed a typical continuous aerobic-only or aerobic and strength-based CR. Peak workload (normalized to lean body mass) during an exercise test was discussed and compared in studies by Trachsel et al., Kodis et al., Szmigielska et al. and Tyni-Lenne et al. [18, 32, 39, 52]. Most indicated no sex difference in peak workload improvement; however, Kodis et al. found a greater improvement in men compared to women. In the study by Kodis et al., only patients with CABG were studied, and they utilized a 24-week CR program, which is longer compared to the other 8–12 week interventions. Therefore, these findings suggest that sex differences may not become evident until a longer CR program is completed.
When comparing exercise time, Wagner et al. and Safdar et al. found that women with atrial fibrillation or CABG surgery, respectively, experienced a greater improvement than men, or only women improved [6, 34]. However, the bulk of studies found that men and women with multiple types of HD had similar improvements in exercise time and included a variety of aerobic, strength and home-based programs [33, 54, 56, 57, 71, 82, 85]. Thus, sex differences in the improvement in exercise time could potentially be dependent on the type of cardiac disease investigated. Importantly, grip strength was measured in four studies [6, 20, 22, 37], and men experienced a greater improvement than women in Mroszczyk-McDonald et al. and Rengo et al., while Kim & So and Safdar et al. found only an improvement in men. Therefore, the consensus reached is that men experienced a significantly greater improvement in handgrip after CR as compared to women.
Cholesterol and triglycerides
Weinberger et al. concluded that HDL cholesterol levels improved more in men compared to women after CR [86]. However, the type of exercise prescribed during CR intervention was not specified in this study. Similarly, studies by Gupta et al. and Sadeghi et al. expressed that only men improved in HDL levels after CR [48, 68]. On the contrary, studies by Savage et al., Casey et al., Heald et al. and Terada et al. found that women had a greater improvement in HDL levels compared to men [23, 26, 78, 87]. Furthermore, a 5-year long cohort study by Warner et al. stated that only women improve their HDL levels after a CR intervention [88]. Women may have begun these latter studies with less favourable body composition, allowing them to manifest a greater HDL benefit [89]. Despite these conflicting observations on sex-related HDL improvement, the general consensus stated by most articles was that men and women appear to either improve equally in HDL levels after CR or see no improvement [24, 25, 29, 36, 37, 41, 42, 45, 47, 50, 52, 53, 59, 71, 75, 87, 90, 91].
Most of the articles in this review discussing LDL cholesterol, LDL: HDL, and total cholesterol: HDL concluded that no sex differences, or no improvements, in the response to CR were found [23,24,25,26, 29, 36, 37, 41, 42, 45, 47, 48, 50, 52, 53, 59, 68, 71, 72, 75, 78, 87, 88, 91]. However, interestingly 2 recent studies from Jafri et al. and Proenca et al. found that men improve LDL to a greater degree than women after CR [92, 93]. These were very large retrospective cohort studies of 15,613 and 881 cardiac patients, respectively. While the majority of studies found that no sex differences were evident in the improvement of total cholesterol after CR [23, 24, 26, 29, 36, 37, 47, 48, 50, 52, 53, 58, 59, 68, 71, 75, 88, 90, 91], El Missiri et al., Casey et al., Ghasghaei et al., and Jafri et al. all concluded that men experienced a greater improvement in total cholesterol levels compared to women [45, 72, 87, 92]. Adherence to the CR program could have played a role since the studies by Casey et al., El Missiri et al., and Jafri et al. found that women had lower completion/adherence rates compared to men; however, adherence was not discussed in the study by Ghashghaei et al. Participants with higher adherence are likely to experience greater benefit of CR participation. On the other hand, poor adherence or non-compliance with the prescribed regimen could impede progress.
Studies by El Missiri et al., Turk-Adawi et al., and Jafri et al. stated that there was a greater reduction in triglyceride levels in men compared to women after CR [72, 91, 92] and Szmigielska et al. similarly found that only men improved triglycerides after CR [52]. The remainder of the reviewed studies indicate equal improvements or no sex differences [23,24,25,26, 29, 36, 37, 42, 47, 48, 50, 53, 58, 59, 71, 75, 78, 87, 88, 91]. As each group of studies included a range of CR duration and a mix of aerobic and strength training it is unclear why a few studies found that women do not improve their triglycerides as much as men except perhaps for the very large sample sizes in Jafri et al. and Turk-Adawi et al. (> 10,000) This finding could further indicate that in order to observe sex differences in certain variables large populations must be studied.
Systolic and diastolic blood pressure
Multiple references found that men and women improve equally (or do not improve) systolic blood pressure after CR [24,25,26,27, 32, 36, 37, 47, 50, 52, 57, 59, 62, 64, 77,78,79, 87, 89, 92, 94]. However, O’Farrell et al. and Turk-Adawi et al. observed a greater reduction in systolic blood pressure in women compared to men after 12 weeks of CR [75, 91], Wahlstrom et al. observed that only women reduced systolic blood pressure after 12 weeks of CR [80], and Mittag et al. observed a greater improvement in men after 52 weeks of CR [90]. Similarly, the majority of the research leaned towards no sex difference (or no improvement) in diastolic blood pressure response to CR [24, 26, 36, 37, 50, 52, 57, 59, 62, 64, 75, 77,78,79,80, 87, 89, 91, 94]. However, two studies by El Missiri et al., and Trachsel et al., stated that women improved their diastolic blood pressure more than men after CR [32, 72]. The outlier studies do not appear to be distinguished from the rest regarding CR duration, HD type, or other extracted variables; thus, it is difficult to identify the factor(s) driving these sex differences. However, the overwhelming majority of studies have indicated that after CR, blood pressure either improves equally between the sexes or no improvement in either sex is observed.
Glucose & glycated hemoglobin
Most reviewed studies found that plasma glucose either did not improve after CR or that there were equal improvements in both sexes [24, 25, 29, 71, 75, 78]. However, a few studies did observe sex differences. Anjo et al. found that glucose measures improved more in women after completion of CR [53], yet women expressed worse glucose levels at baseline, thus eliciting a greater improvement after CR. Ghashghaei et al. and Szmigielska et al. observed that only men improved plasma glucose after CR [45, 52]. All of these outlier studies used t-test analyses and were perhaps statistically underpowered. Similar to the changes in plasma glucose, changes in glycated hemoglobin showed similar improvements (or no change) in men and women after CR [36, 41, 53, 89, 91], yet Jafri et al. recently found that men had a greater improvement in their large retrospective study [92].
Body composition
Most studies have indicated that body composition measures (i.e. weight, waist circumference, BMI, body fat %, total fat mass) either improved equally between the sexes or did not improve at all after CR [6, 20, 22,23,24,25, 29, 31, 36, 37, 42, 47, 50, 52, 53, 58, 59, 64, 68, 72, 75, 87, 89, 91, 92, 95]. There were a few exceptions where Braga et al. and Sarrafzadegan et al. observed more improvement in waist circumference and BMI in women compared to men [50, 96], Heald et al. and Szmigielska et al. observed an improvement of BMI only in men [26, 52], and Terada et al., Ghashghaei et al. and Brochu et al. observed that there were greater improvements of body weight, body fat %, total fat mass, and waist circumference in men compared to women [29, 36, 78]. Brochu et al. hypothesized that their observations of greater improvements in men could stem from their observation that the women in their cohort were generally less fit than men [29]. Therefore, baseline fitness and physical activity levels could play a role in any observed sex differences.
C-reactive protein
Thorin-Trescases et al. found that the levels of C-reactive protein (CRP; an inflammatory marker) were reduced in men after CR but not in women [24]. Three other studies, however, determined that no sex difference was found in CRP levels after CR [71, 97, 98]. Thorin-Trescases et al. investigated patients specifically with acute coronary syndrome, whereas the studies by Goldhammer et al., Sheikhian et al., and Caulin-Glaser et al. all investigated patients with CAD. Therefore, the sex differences observed by Thorin-Trescases et al. could be due to the type of HD investigated.
Limitations
The current review has broadly described sex differences in the physiological responses to a wide range of CR programs. We did not limit the search with regards to physiological response, program length, program intensity, or cardiac disease type with the purpose of searching for trends that currently exist in the literature. A more targeted approach could have enhanced the precision of the findings, enabling a more comprehensive understanding of select research topics. However, limiting our search parameters to programs at least 12 weeks long would have reduced the number of studies to 46/88; further limiting our search within that group to those that investigated isolated cardiac conditions would have reduced our search to 17 articles for CAD (encompassing myocardial infarction, CABG, PCI), 5 articles for heart failure, and 2 articles for atrial fibrillation. We acknowledge that program length, intensity and cardiac disease type can all influence the physiological responses to cardiac rehabilitation; however, this review was necessary to determine the most appropriate direction to take for subsequent investigations and to highlight strengths and weaknesses in the current body of literature.
Sex differences that may be present after completion of a short CR program may not be evident with longer programs, or vice-versa. Indeed, CR programs longer than the typical 12 weeks have been shown to elicit further improvements [99]. Similarly, we did not extract data on daily physical activity which could play an important role in the physiological response to CR if it changed over the course of the program. A recent umbrella review found that in CR participants, physical activity increased and sedentary behavior decreased compared to with usual care [100]. Furthermore, some of the articles in the current review that proposed a physiological sex difference used populations with only HF or only atrial fibrillation, as compared to a combination of patients with CABG, CAD, history of MI, and/or angina. As all these conditions have different pathophysiology, it is certainly plausible that different HD populations would respond differently to CR or exercise. Another limitation could be that most HD patients are middle-aged and older and are likely to have passed menopause and progressed through andropause. Thus, the effects of sex hormones have been minimized, making men and women potentially less distinct in their responses to exercise training. Lastly, psychosocial factors were beyond the scope of this review but could also impede the improvement of physiological responses after CR by influencing such factors as program adherence (included in this review). Psychosocial factors that can affect adherence include patient motivation, understanding and awareness of the benefits, social support, and access to resources. These factors are particularly important to consider when investigating sex differences, as it has been shown that men and women have differing limitations to CR enrollment and adherence [101]. Though the psychosocial factors of adherence were not explored in this review, it is imperative to note that optimizing adherence can substantially enhance the success of cardiac rehabilitation programs and ultimately improve patient outcomes and impact comparisons.
The results of this systematic review were not quantitatively pooled in a meta-analysis due to the breadth of inclusion criteria. Therefore, sensitivity analyses and statistical power could not be assessed. Future reviews and analyses should build on the findings of this review by narrowing the inclusion criteria to draw more specific conclusions. An essential factor that could play a role in the outcomes observed is the type of statistical analysis conducted in each study. In this review, repeated measures ANOVAs, t-tests, and t-tests between deltas (i.e. change from CR) were the most frequently used statistics. In the ideal case of comparing the differences between the two sexes at two different time points, repeated measures ANOVAs should be conducted on disaggregated data to obtain the most accurate conclusions. Unfortunately, most of the studies in this current review used t-tests over time within each sex, preventing valid sex comparisons. Thus, due to the possibility that t-tests may reflect an inaccuracy of the results, many of our assessments where only one sex responded to CR may have been better interpreted as a greater response in one sex should the appropriate statistics have been conducted. We recommend that investigators consult statistical experts to ensure accurate conclusions when comparing sexes.
Conclusions
Based on the findings of this systematic review without meta-analysis, men and women with HD respond similarly to CR. However, many articles have found larger improvements in men compared to women with regard to maximal oxygen consumption, functional capacity, 6MWD and grip strength. Reasons for such findings could be physiologically attributed to larger muscle mass in men compared to women. Though many other responses to CR have weakly suggested a sex difference, our work highlights that limitations such as low recruitment of women, statistics used, intervention type, type of HD population, adherence rates, and program length could dampen the ability to discern sex differences after CR. More research is required on CR effectiveness that includes larger cohorts of women and proper statistical analysis. It is important to note that our findings show that women benefit as much as men in most physiological measures highlighting that women should be prescribed CR as a standard therapy following a cardiac diagnosis.
Data availability
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.
References
Norris CM, Yip CYY, Nerenberg KA, Clavel MA, Pacheco C, Foulds HJA, Hardy M, Gonsalves CA, Jaffer S, Parry M et al. State of the science in women’s cardiovascular disease: a Canadian perspective on the influence of sex and gender. J Am Heart Association. 2020;9(4).
Pacheco C, Mullen KA, Coutinho T, Jaffer S, Parry M, Van Spall HGC, Clavel MA, Edwards JD, Sedlak T, Norris CM, et al. The Canadian women’s Heart Health Alliance Atlas on the epidemiology, diagnosis, and management of cardiovascular disease in women - Chap. 5: sex- and gender-unique manifestations of Cardiovascular Disease. CJC Open. 2022;4(3):243–62.
Sedlak TL, Lee M, Izadnegahdar M, Merz CNB, Gao M, Humphries KH. Sex differences in clinical outcomes in patients with stable angina and no obstructive coronary artery disease. Am Heart J. 2013;166(1):38–44.
Gulati M. Improving the cardiovascular health of women in the nation: moving beyond the bikini boundaries. Circulation. 2017;135(6):495–8.
Beauchamp A, Worcester M, Ng A, Murphy B, Tatoulis J, Grigg L, Newman R, Goble A. Attendance at cardiac rehabilitation is associated with lower all-cause mortality after 14 years of follow-up. Heart. 2013;99(9):620–5.
Safdar B, Mori M, Nowroozpoor A, Geirsson A, D’Onofrio G, Mangi AA. Clinical profile and sex-specific recovery with cardiac rehabilitation after coronary artery bypass grafting surgery. Clin Ther. 2022;44(6):846–58.
Eijsvogels TMH, Maessen MFH, Bakker EA, Meindersma EP, van Gorp N, Pijnenburg N, Thompson PD, Hopman MTE. Association of cardiac rehabilitation with all-cause mortality among patients with cardiovascular disease in the Netherlands. JAMA Netw Open. 2020;3(7):e2011686.
Kolar F, Ostadal B. Sex differences in cardiovascular function. Acta Physiol. 2013;207(4):584–7.
Rossy LA, Thayer JF. Fitness and gender-related differences in heart period variability. Psychosom Med. 1998;60(6):773–81.
Salton CJ, Chuang ML, O’Donnell CJ, Kupka MJ, Larson MG, Kissinger KV, Edelman RR, Levy D, Manning WJ. Gender differences and normal left ventricular anatomy in an adult population free of hypertension. J Am Coll Cardiol. 2002;39(6):1055–60.
Vitale C, Fini M, Speziale G, Chierchia S. Gender differences in the cardiovascular effects of sex hormones. Clin Pharmacol. 2010:11.
Howden EJ, Perhonen M, Peshock RM, Zhang R, Arbab-Zadeh A, Adams-Huet B, Levine BD. Females have a blunted cardiovascular response to one year of intensive supervised endurance training. J Appl Physiol (1985). 2015;119(1):37–46.
Colbert JD, Martin BJ, Haykowsky MJ, Hauer TL, Austford LD, Arena RA, Knudtson ML, Meldrum DA, Aggarwal SG, Stone JA. Cardiac rehabilitation referral, attendance and mortality in women. Eur J Prev Cardiol. 2015;22(8):979–86.
Samayoa L, Grace SL, Gravely S, Scott LB, Marzolini S, Colella TJ. Sex differences in cardiac rehabilitation enrollment: a meta-analysis. Can J Cardiol. 2014;30(7):793–800.
Colella TJ, Gravely S, Marzolini S, Grace SL, Francis JA, Oh P, Scott LB. Sex bias in referral of women to outpatient cardiac rehabilitation? A meta-analysis. Eur J Prev Cardiol. 2015;22(4):423–41.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71.
Keteyian SJ, Duscha BD, Brawner CA, Green HJ, Marks CR, Schachat FH, Annex BH, Kraus WE. Differential effects of exercise training in men and women with chronic heart failure. Am Heart J. 2003;145(5):912–8.
Kodis J, Smith KM, Arthur HM, Daniels C, Suskin N, McKelvie RS. Changes in exercise capacity and lipids after clinic versus home-based aerobic training in coronary artery bypass graft surgery patients. J Cardpulm Rehabil. 2001;21(1):31–6.
Lee LS, Tsai MC, Oh PI, Brooks D. The effectiveness of progressive aerobic interval training in cardiac rehabilitation. Med Sci Sports Exerc. 2018;50(5):881–8.
Mroszczyk-McDonald A, Savage PD, Ades PA. Handgrip strength in cardiac rehabilitation: normative values, interaction with physical function, and response to training. J Cardiopulm Rehabil Prev. 2007;27(5):298–302.
Nguyen CH, Thomas SG, Marzolini S. Factors associated with change in cardiovascular fitness for patients with peripheral and coronary artery disease in cardiac rehabilitation. J Cardiopulm Rehabil Prev. 2021;41(4):230–6.
Rengo JL, Khadanga S, Savage PD, Ades PA. Response to exercise training during cardiac rehabilitation differs by sex. J Cardiopulm Rehabilitation Prev. 2020;40(5):319–24.
Savage PD, Brochu M, Ades PA. Gender alters the high-density lipoprotein cholesterol response to cardiac rehabilitation. J Cardpulm Rehabil. 2004;24(4):248–54. quiz 255.
Thorin-Trescases N, Hayami D, Yu C, Luo X, Nguyen A, Larouche JF, Lalonge J, Henri C, Arsenault A, Gayda M, et al. Exercise lowers plasma angiopoietin-like 2 in men with post-acute coronary syndrome. PLoS ONE [Electronic Resource]. 2016;11(10):e0164598.
Shultz B, Kamphoff C, Dalleck L. Relative energy expenditure may prove beneficial when prescribing exercise to phase II cardiac rehabilitation patients. J Exerc Physiol Online. 2010;13(5):1–8.
Heald FA, Marzolini S, Colella TJF, Oh P, Nijhawan R, Grace SL. Women’s outcomes following mixed-sex, women-only, and home-based cardiac rehabilitation participation and comparison by sex. BMC Womens Health. 2021;21(1):413.
Ades PA, Waldmann ML, Polk DM, Coflesky JT. Referral patterns and exercise response in the rehabilitation of female coronary patients aged greater than or equal to 62 years. Am J Cardiol. 1992;69(17):1422–5.
Antunes-Correa LM, Melo RC, Nobre TS, Ueno LM, Franco FG, Braga AM, Rondon MU, Brum PC, Barretto AC, Middlekauff HR, et al. Impact of gender on benefits of exercise training on sympathetic nerve activity and muscle blood flow in heart failure. Eur J Heart Fail. 2010;12(1):58–65.
Brochu M, Poehlman ET, Savage P, Fragnoli-Munn K, Ross S, Ades PA. Modest effects of exercise training alone on coronary risk factors and body composition in coronary patients. J Cardpulm Rehabil. 2000;20(3):180–8.
MacMillan JS, Davis LL, Durham CF, Matteson ES. Exercise and heart rate recovery. Heart Lung. 2006;35(6):383–90.
Temfemo A, Chlif M, Mandengue SH, Lelard T, Choquet D, Ahmaidi S. Is there a beneficial effect difference between age, gender, and different cardiac pathology groups of exercise training at ventilatory threshold in cardiac patients? Cardiol J. 2011;18(6):632–8.
Trachsel LD, Boidin M, Henri C, Fortier A, Lalonge J, Juneau M, Nigam A, Gayda M. Women and men with coronary heart disease respond similarly to different aerobic exercise training modalities: a pooled analysis of prospective randomized trials. Appl Physiol Nutr Metabolism = Physiologie Appliquee Nutr et Metab. 2020;23:23.
Vilela EM, Ladeiras-Lopes R, Joao A, Braga J, Torres S, Ribeiro J, Primo J, Fontes-Carvalho R, Campos L, Miranda F, et al. Differential impact of a cardiac rehabilitation program in functional parameters according to patient gender. Am J Cardiovasc Dis. 2020;10(4):367–75.
Wagner MK, Zwisler ADO, Risom SS, Svendsen JH, Christensen AV, Berg SK. Sex differences in health status and rehabilitation outcomes in patients with atrial fibrillation treated with ablation: results from the CopenHeartRFA trial. Eur J Cardiovasc Nurs. 2018;17(2):123–35.
Piña IL, Bittner V, Clare RM, Swank A, Kao A, Safford R, Nigam A, Barnard D, Walsh MN, Ellis SJ, et al. Effects of exercise training on outcomes in women with heart failure. JACC: Heart Fail. 2014;2(2):180–6.
Vidal-Almela S, Way KL, Terada T, Tulloch HE, Keast ML, Pipe AL, Chirico D, Reed JL. Sex differences in physical and mental health following high-intensity interval training in adults with cardiovascular disease who completed cardiac rehabilitation. Appl Physiol Nutr Metab. 2021:1–9.
Kim YH, So W-Y. Gender differences in home-based cardiac rehabilitation of post-percutaneous coronary intervention patients. Aging Clin Experimental Res. 2019;31(2):249–55.
Willenheimer R, Erhardt L, Cline C, Rydberg E, Israelsson B. Exercise training in heart failure improves quality of life and exercise capacity. Eur Heart J. 1998;19(5):774–81.
Tyni-Lenne R, Gordon A, Europe E, Jansson E, Sylven C. Exercise-based rehabilitation improves skeletal muscle capacity, exercise tolerance, and quality of life in both women and men with chronic heart failure. J Card Fail. 1998;4(1):9–17.
Mertens DJ, Kavanagh T. Exercise training for patients with chronic atrial fibrillation. J Cardpulm Rehabil. 1996;16(3):193–6.
Kitagaki K, Ono R, Konishi H, Nakanishi M, Miura H, Aoki T, Noguchi T. Sex-related differences in exercise capacity trends and determinants after cardiac rehabilitation in patients with acute myocardial infarction. Phys Ther Res. 2022;25(3):106–12.
Caulin-Glaser T, Maciejewski PK, Snow R, LaLonde M, Mazure C. Depressive symptoms and sex affect completion rates and clinical outcomes in cardiac rehabilitation. Prev Cardiol. 2007;10(1):15–21.
Chai A, McCormick A, Jacobson A, Kligfield P. Effects of cardiac rehabilitation on the exercise performance of men and women in the fourth through the ninth decades. Cardiovasc Reviews Rep. 1999;20(9):476–80.
Gee MA, Viera AJ, Miller PF, Tolleson-Rinehart S. Functional capacity in men and women following cardiac rehabilitation. J Cardiopulm Rehabilitation Prev. 2014;34(4):255–62.
Ghashghaei FE, Sadeghi M, Rabiei K, Roohafza H, Sarrafzadegan N. Gender differences in risk factors of obese patients after cardiac rehabilitation program. Iran J Nurs Midwifery Res. 2012;17(5):381–5.
Kligfield P, McCormick A, Chai A, Jacobson A, Feuerstadt P, Hao SC. Effect of age and gender on heart rate recovery after submaximal exercise during cardiac rehabilitation in patients with angina pectoris, recent acute myocardial infarction, or coronary bypass surgery. Am J Cardiol. 2003;92(5):600–3.
Lavie CJ, Milani RV. Effects of cardiac rehabilitation and exercise training on exercise capacity, coronary risk factors, behavioral characteristics, and quality of life in women. Am J Cardiol. 1995;75(5):340–3.
Sadeghi M, Ghashghaei FE, Rabiei K, Roohafza H, Afshar H. Is there any difference between non-obese male and female in response to cardiac rehabilitation programs? J Res Med Sci. 2012;17(8):787–91.
Saeidi M, Mostafavi S, Heidari H, Masoudi S. Effects of a comprehensive cardiac rehabilitation program on quality of life in patients with coronary artery disease. Arya Atherosclerosis. 2013;9(3):179–85.
Sarrafzadegan N, Rabiei K, Kabir A, Sadeghi M, Khosravi A, Asgari S, Taghipour HR, Roohafza H. Gender differences in risk factors and outcomes after cardiac rehabilitation. Acta Cardiol. 2008;63(6):763–70.
Wise FM, Patrick JM. Cardiac rehabilitation outcomes in women with chronic heart failure: mood, fitness, and exercise safety. J Cardiopulm Rehabilitation Prev. 2012;32(2):78–84.
Szmigielska K, Jegier A. Clinical outcomes of cardiac rehabilitation in women with coronary artery disease-differences in comparison with men. J Pers Med. 2022;12(4).
Anjo D, Santos M, Rodrigues P, Brochado B, Sousa MJ, Barreira A, Viamonte S, Fernandes P, Reis AH, Gomes JL, et al. The benefits of cardiac rehabilitation in coronary heart disease: a gender issue? Rev Port Cardiol. 2014;33(2):79–87.
Balady GJ, Jette D, Scheer J, Downing J. Changes in exercise capacity following cardiac rehabilitation in patients stratified according to age and gender. Results of the Massachusetts Association of Cardiovascular and Pulmonary Rehabilitation Multicenter Database. J Cardpulm Rehabil. 1996;16(1):38–46.
Branco C, Viamonte S, Matos C, Magalhães S, Cunha I, Barreira A, Fernandes P, Torres S. Predictors of changes in functional capacity on a cardiac rehabilitation program. Revista Portuguesa De Cardiologia (English Edition). 2016;35(4):215–24.
Cannistra LB, Balady GJ, Omalley CJ, Weiner DA, Ryan TJ. Comparison of the clinical profile and outcome of women and men in cardiac rehabilitation. Am J Cardiol. 1992;69(16):1274–9.
Korzeniowska-Kubacka I, Bilinska M, Dobraszkiewicz-Wasilewska B, Piotrowicz R. Hybrid model of cardiac rehabilitation in men and women after myocardial infarction. Cardiol J. 2015;22(2):212–8.
McConnell TR, Laubach ICA, Szmedra L. Age and gender related trends in body composition, and lipids, exercise capacity during cardiac rehabilitation. Am J Geriatric Cardiol. 1997;6(4):37–45.
Pischke CR, Weidner G, Elliott-Eller M, Scherwitz L, Merritt-Worden TA, Marlin R, Lipsenthal L, Finkel R, Saunders D, McCormac P, et al. Comparison of coronary risk factors and quality of life in coronary artery disease patients with versus without diabetes mellitus. Am J Cardiol. 2006;97(9):1267–73.
Rejeski WJ, Foy CG, Brawley LR, Brubaker PH, Focht BC, Norris IJL, Smith ML. Older adults in cardiac rehabilitation: a new strategy for enhancing physical function. Med Sci Sports Exerc. 2002;34(11):1705–13.
Brawner CA, Pack Q, Berry R, Kerrigan DJ, Ehrman JK, Keteyian SJ. Relation of a maximal exercise test to change in exercise tolerance during cardiac rehabilitation. Am J Cardiol. 2022;175:139–44.
Calvo-Lopez M, Arranz Tolos R, Marin Exposito J, Gruosso D, Andrea R, Roque M, Falces C, Yago G, Saura Araguas J, Pastor N, et al. Cardio4Health study, a cardiac telerehabilitation pilot program aimed at patients after an ischemic event: cross-sectional study. JMIR Cardio. 2023;7:e44179.
Khadanga S, Savage PD, Pecha A, Rengo J, Ades PA. Optimizing training response for women in cardiac rehabilitation: a randomized clinical trial. JAMA Cardiol. 2022;7(2):215–8.
Araya-Ramírez F, Moncada-Jiménez J, Grandjean PW, Franklin BA. Improved walk test performance and blood pressure responses in men and women completing cardiac rehabilitation: implications regarding exercise trainability. Am J Lifestyle Med. 2021:155982762199512.
Bellet RN, Francis RL, Adams L, Morris NR. Six-minute walk test distances in fast-track and traditional cardiac rehabilitation: a 3-year database review. J Cardiopulm Rehabilitation Prev. 2015;35(6):417–22.
Candelaria D, Zecchin R, Ferry C, Ladak L, Randall S, Gallagher R. Shorter wait times to cardiac rehabilitation associated with greater exercise capacity improvements: a multisite study. J Cardiopulm Rehabil Prev. 2020.
Verrill DE, Barton C, Beasley W, Lippard M, King CN. Six-minute walk performance and quality of life comparisons in North Carolina cardiac rehabilitation programs. Heart Lung. 2003;32(1):41–51.
Gupta R, Sanderson BK, Bittner V. Outcomes at one-year follow-up of women and men with coronary artery disease discharged from cardiac rehabilitation: what benefits are maintained? J Cardiopulm Rehabilitation Prev. 2007;27(1):11–8. quiz 19.
Fiorina C, Vizzardi E, Lorusso R, Maggio M, De Cicco G, Nodari S, Faggiano P, Cas LD. The 6-min walking test early after cardiac surgery. Reference values and the effects of rehabilitation programme. Eur J Cardiothorac Surg. 2007;32(5):724–9.
Freene N, McManus M, Mair T, Tan R, Davey R. Objectively measured changes in physical activity and sedentary behavior in cardiac rehabilitation: a prospective cohort study. J Cardiopulm Rehabilitation Prev. 2018;38(6):E5–8.
Goldhammer E, Ben-Sira D, Zaid G, Biniamini Y, Maor I, Lanir A, Sagiv M. Paraoxonase activity following exercise-based cardiac rehabilitation program. J Cardiopulm Rehabilitation Prev. 2007;27(3):151–4.
El Missiri AM, Awadalla HM, Almoudi MM. Gender differences among ischemic heart disease patients enrolled in a cardiac rehabilitation program. Egypt Heart J. 2020;72(1):15.
Zahedi M, Safi F. Assessment of the Heart’s left and right ventricles (EF and TAPSE) in CABG surgery patients before and after cardiac rehabilitation. Cardiovasc Hematol Disord Drug Targets. 2023;23(2):104–10.
Zahedi M, Shirmohammadi M. The effect of cardiac rehabilitation on left and right ventricular function in post primary PCI patients. Ann Med Surg (Lond). 2022;79:104093.
O’Farrell P, Murray J, Huston P, LeGrand C, Adamo K. Sex differences in cardiac rehabilitation. Can J Cardiol. 2000;16(3):319–25.
Soleimani A, Nejatian M, Hajizaynali MA, Abbasi SH, Alidoosti M, Sheikhfathollahi M, Abbasi A. Effect of gender and type 2 diabetes mellitus on heart rate recovery in patients with coronary artery disease after cardiac rehabilitation. Endokrynologia Polska. 2009;60(6):430–6.
Swank AM, Funk DC, Manire JT, Allard AL, Denny DM. Effect of resistance training and aerobic conditioning on muscular strength and submaximal fitness for individuals with chronic heart failure: influence of age and gender. J Strength Conditioning Res. 2010;24(5):1298–305.
Terada T, Chirico D, Tulloch HE, Scott K, Pipe AL, Reed JL. Sex differences in psychosocial and cardiometabolic health among patients completing cardiac rehabilitation. Appl Physiol Nutr Metabolism = Physiologie Appliquee Nutr et Metab. 2019;44(11):1237–45.
Cheragi MN, Roshan M, Dehghani VD. The effectiveness of home-based cardiac rehabilitation program on cardiovascular stress indices in men and women with myocardial infarction: a randomised controlled clinical trial. Revista Colombiana De Cardiologia. 2021;28(2):128–35.
Wahlstrom M, Medin J, Karlsson MR. Gender differences in health-related quality of life, blood pressure and heart rate among patients with paroxysmal atrial fibrillation after performing MediYoga. Int J Cardiol Heart Vasc. 2023;49:101274.
Korzeniowska-Kubacka I, Bilinska M, Piotrowska D, Stepnowska M, Piotrowicz R. The impact of exercise-only-based rehabilitation on depression and anxiety in patients after myocardial infarction. Eur J Cardiovasc Nurs. 2017;16(5):390–6.
Stojanovic MV, Stankovic A, Igrutinovic-Novkovic M, Igic J, Deljanin-Ilic I, Ilic M. Effects of cardiac rehabilitation on quality of life and exercise capacity in patients with coronary artery disease-do women benefit equally? Srp Arh Celok Lek. 2023;151(5–6):326–32.
Ades PA, Waldmann ML, Polk DM, Coflesky JT. Referral patterns and exercise response in the rehabilitation of female coronary patients aged > = 62 years. Am J Cardiol. 1992;69(17):1422–5.
Soleimani A, Abbasi A, Salarifar M, Kassaian E, Zeinali AM, Alidoosti M, Nejatian M. Effect of different sessions of cardiac rehabilitation on exercise capacity in patients with percutaneous transluminal coronary angioplasty. Eur J Phys Rehabilitation Med. 2009;45(2):171–8.
Ocallaghan WG, Teo KK, Oriordan J, Webb H, Dolphin T, Horgan JH. Comparative response of male and female patients with coronary-artery disease to exercise rehabilitation. Eur Heart J. 1984;5(8):649–51.
Weinberger AH, Mazure CM, McKee SA, Caulin-Glaser T. The association of tobacco use and gender to cardiac rehabilitation outcomes: a preliminary investigation. J Subst Use. 2014;19(1–2):171–5.
Casey A, Chang BH, Huddleston J, Virani N, Benson H, Dusek JA. A model for integrating a mind/body approach to cardiac rehabilitation: outcomes and correlators. J Cardiopulm Rehabilitation Prev. 2009;29(4):230–8. quiz 239.
Warner JG Jr., Brubaker PH, Zhu Y, Morgan TM, Ribisl PM, Miller HS, Herrington DM. Long-term (5-year) changes in HDL cholesterol in cardiac rehabilitation patients. Do sex Differences Exist? Circulation. 1995;92(4):773–7.
Terada T, Beanlands RA, Tulloch HE, Pipe AL, Chirico D, Reed JL. Aerobic interval training and moderate-to-vigorous intensity continuous training are associated with sex-specific improvements in psychological health in patients with heart disease. Eur J Prev Cardiol. 2019;26(8):888–91.
Mittag O, China C, Hoberg E, Juers E, Kolenda K, Richardt G, Maurischat C, Raspe H. Outcomes of cardiac rehabilitation with versus without a follow-up intervention rendered by telephone (Luebeck follow-up trial): overall and gender-specific effects. Int J Rehabil Res. 2006;29(4):295–302.
Turk-Adawi KI, Oldridge NB, Vitcenda MJ, Tarima SS, Grace SL. Secondary prevention recommendation attainment with cardiac rehabilitation: is there a gender disparity? Womens Health Issues. 2016;26(3):278–87.
Hussain Jafri SH, Ngamdu KS, Price D, Baloch ZQ, Cohn J, Wilcox M, Freeman AM, Ornish D, Wu WC. Intensive cardiac rehabilitation attenuates the gender gap in cardiac rehabilitation participation. Curr Probl Cardiol. 2023;48(6):101668.
Proenca T, Pinto RA, Carvalho MM, Rocha A, Dias P, Macedo F. Sex disparities and dyslipidemic control in a coronary rehabilitation program. Int J Cardiol. 2023;370:72–4.
Quindry JC, McNamara M, Oser C, Fogle C. Cardiac rehabilitation and resting blood pressure: MONTANA OUTCOMES PROJECT CARDIAC REHABILITATION REGISTRY FINDINGS. J Cardiopulm Rehabil Prev. 2022;42(2):E23–31.
Socha M, Wronecki K, Sobiech KA. Gender and age-dependent differences in body composition changes in response to cardiac rehabilitation exercise training in patients after coronary artery bypass grafting. Ann Agric Environ Med. 2017;24(3):5.
Braga M, Nascimento H, Pinto R, Araújo P, Nunes A, Rodrigues J, Araújo V, Parada-Pereira F, Maciel MJ, Rocha A. Cardiac rehabilitation in older patients: indication or limitation? Rev Port Cardiol. 2021;40(1):13–20.
Caulin-Glaser T, Falko J, Hindman L, La Londe M, Snow R. Cardiac rehabilitation is associated with an improvement in C-reactive protein levels in both men and women with cardiovascular disease. J Cardpulm Rehabil. 2005;25(6):332–6. quiz 337.
Sheikhian N, Ostovan MA, Daryanoosh F, Sharifi F. Aerobic exercise improves brain natriuretic peptide and C-Reactive protein among men and women with coronary artery disease. Int J Appl Exerc Physiol. 2018;7(4):30–40.
Morrin L, Black S, Reid R. Impact of duration in a cardiac rehabilitation program on coronary risk profile and health-related quality of life outcomes. J Cardiopulm Rehabil. 2000;20(2):115–21.
Dafny HA, Champion S, Gebremichael LG, Pearson V, Hendriks JM, Clark RA, Pinero de Plaza MA, Gulyani A, Hines S, Beleigoli A. Cardiac rehabilitation, physical activity, and the effectiveness of activity monitoring devices on cardiovascular patients: an umbrella review of systematic reviews. Eur Heart J Qual Care Clin Outcomes. 2023;9(4):323–30.
Ghisi GLM, Kim WS, Cha S, Aljehani R, Cruz MMA, Vanderlei LCM, Pepera G, Liu X, Xu Z, Maskhulia L, et al. Women’s cardiac rehabilitation barriers: results of the international council of cardiovascular prevention and rehabilitation’s first global assessment. Can J Cardiol. 2023;39(11S):S375–83.
Adams KJ, Barnard KL, Swank AM, Mann E, Kushnick MR, Denny DM. Combined high-intensity strength and aerobic training in diverse phase II cardiac rehabilitation patients. J Cardpulm Rehabil. 1999;19(4):209–15.
Baranyi A, Meinitzer A, von Lewinski D, Rothenhausler HB, Amouzadeh-Ghadikolai O, Harpf H, Harpf L, Traninger H, Hodl R, Harb BM, et al. Sex-specific differences in trimethylamine N-oxide (TMAO) concentrations before and after cardiac rehabilitation in acute myocardial infarction patients. EXCLI J. 2022;21:1–10.
Caminiti G, Perrone MA, Volterrani M, Iellamo F, Marazzi G, Selli S, Franchini A, Padua E. Effects of concurrent aerobic plus resistance training on blood pressure variability and blood pressure values in patients with hypertension and coronary artery disease: gender-related differences. J Cardiovasc Dev Dis. 2022;9(6).
Deljanin Ilic M, Stojanovic M, Ilic S. The effect of cardiovascular rehabilitation on physical strain tolerance - does gender really matter? Vojnosanit Pregl. 2019;78(8):844–50.
Keating FK, Schneider DJ, Savage PD, Bunn JY, Harvey-Berino J, Ludlow M, Toth MJ, Ades PA. Effect of exercise training and weight loss on platelet reactivity in overweight patients with coronary artery disease. J Cardiopulm Rehabilitation Prev. 2013;33(6):371–7.
Maugeri FS, Campana M, Ferrari R, Giordano A, Scalvini S, Volterrani M, Bernardi L, Calciati A, Finardi G, Perlini S, et al. Experience from controlled trials of physical training in chronic heart failure - protocol and patient factors in effectiveness in the improvement in exercise tolerance. Eur Heart J. 1998;19(3):466–75.
Pabisiak A, Nowak M, Kmieae S. Rehabilitation of women with a history of myocardial infarct. Med Sportiva. 2013;17(3):113–8.
Acknowledgements
The authors would like to thank Emilia Main for her help with an updated literature search for manuscript revisions.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
MP conducted the literature search used in the review. JB, TJP, HJ, JDMD, and HE conceived of the project and conducted the systematic review (abstract and full text screening). JB and HE extracted the data from relevant citations. JB and HE drafted the initial manuscript. All authors reviewed the manuscript prior to submission.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable
Consent for publication
Not applicable
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Bouakkar, J., Pereira, T., Johnston, H. et al. Sex differences in the physiological responses to cardiac rehabilitation: a systematic review. BMC Sports Sci Med Rehabil 16, 74 (2024). https://doi.org/10.1186/s13102-024-00867-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13102-024-00867-9