
Abstract
Introduction
Considering the effects of fatigue on athletic performance and the subsequent increase in the probability of injury, the purpose of this study was to compare the effects of slow dynamic, fast dynamic, and static stretching on the recovery of performance, range of motion (ROM), balance, and joint position sense.
Methods
Fifteen collegiate healthy females were involved in four separate sessions of slow dynamic stretching (SDS), fast dynamic stretching (FDS), static stretching (SS), and control condition (CC; without stretching), in a random order with at least 48 h of rest between sessions. After warming up, the individuals performed ROM, balance, joint position sense (JPS) maximum voluntary isometric contraction (MVIC) force as well as countermovement (CMJ) and squat jump (SJ) as pre-tests. After performing the knee fatigue protocol of 4 sets of knee extension and flexion at 60% of 1 repetition maximum (RM) to exhaustion (CC; without stretching) or stretching programs (SDS or FDS or SS), the subjects repeated all the tests at post-test 1 (after 5 min) and post-test 2 (after 60 min).
Results
A significantly lower JPS error was detected with SDS while JPS error increased in the SS and control conditions (p < 0.0001). MVIC force significantly increased with SDS and FDS but decreased in control and SS conditions (p < 0.0001). Moreover, a significant decrease in CMJ and SJ height in SS and control conditions was revealed (p < 0.0001). Also, a significant decrease in balance with the control condition was revealed. But only SDS minimized fatigue-induced balance decrements (p < 0.0001). Additionally, the control condition experienced a significant decrease in knee extensor ROM, which contrasted with the significant increase in the quadriceps flexibility with the stretching conditions.
Conclusions
The present results support the idea that SDS may increase quadriceps MVIC force, knee extensor ROM and knee JPS. So according to the present results, it is suggested that the SDS could be implemented and incorporated into a regular recovery program.
Similar content being viewed by others

Introduction
Although the health advantages of regular physical activity and sports are well known, exercise can cause muscular injury and fatigue [1]. Fatigue across training and competition periods increases injury risk, especially with high intensity training loads [2, 3]. Considering the relevance of fatigue and its effects on non-contact risk injuries (e.g., hamstrings strain injury, anterior cruciate ligament tear), several recovery strategies have been proposed to reduce the consequences of fatigue and improve sport performance, such as foam rolling, massage, and stretching [2, 4].
Stretching techniques are used to increase joint range of motion (ROM) [5, 6]. and they can assist in the prevention of musculotendinous injuries in activities of daily life or athletics [7]. Flexibility is a joint's capacity to move through its whole ROM. It has been specifically hypothesized that flexibility training's enhanced muscle–tendon compliance may increase elasticity and result in a stronger contraction force [8]. There are different types of stretching exercises, including static (SS) and dynamic stretching (DS) exercises, which are most commonly utilized among athletes and coaches [9, 10]. SS includes the limb moving to the end of its ROM and holding the stretched posture. SS traditionally has been the most popular stretching technique among athletes, because of its simple technique [11]. Nevertheless, some studies have found that prolonged SS can reduce strength, power or endurance up to 20.5% [12]. whereas DS may have no effect or improve subsequent muscle strength performance [13, 14]. As a result, DS has been recommended as a replacement to SS because it can improve agility, endurance, strength, power, and anaerobic capacity [15].
In DS, motions are performed at or near full ROM under controlled situations at slow to relatively fast velocity [5]. DS improves proprioception, muscle strength, and performance improvements by increasing the neuronal activity of the motor unit and improving kinesthetic awareness [16]. Additionally, researchers proposed that DS can maintain or enhance the stiffness of muscle-tendinous units (MTUs), boost nerve impulse transmission, and increase force output at higher velocities (force–velocity relationship) [17]. The extent of the stretch-induced effects depends on various variables, including muscle condition, stretching time, stretching intensity, contraction type, and contraction velocity. However, these mechanisms have not yet been evaluated, and it is still unclear how DS affects performance [16,17,18].
Accordingly, past research findings regarding the influence of SS and DS on muscle function and performance are conflicting. For example, recent studies have demonstrated that acute prolonged bouts of SS (> 60-s per muscle group) can impair vertical jumps, short sprints, tasks requiring maximal voluntary contractions, muscle strength-endurance performance, balancing tasks, and reaction time [12, 19, 20]. Nevertheless, these detrimental impacts of SS training are dependent on the time and intensity of stretching. Accordingly, Behm and Chaouachi [21]. recommended avoiding SS of any duration when even small performance reductions are unacceptable as with elite competitions. This suggestion might only apply to SS [21]. as studies have found that DS has trivial negative impacts on strength and power output [22]. sprint performance [23]. and vertical jump [24]. Recent research has demonstrated that DS increases muscle strength, jump height, and sprint efficiency [25]. However, the literature suggests that shorter durations of DS do not negatively affect performance and that longer durations (20–30 s) may improve performance [15, 18]. Also, DS may impair strength at slow velocity but enhances it at faster velocities [26]. Therefore, there is a lack of consensus in the literature about the effects of dynamic stretching (DS) and static stretching (SS) on muscular performance, functional abilities, and reducing risk of injury..
According to past literature, with the onset of fatigue, the athlete’s strength, performance, and neuromuscular coordination are reduced, and the athlete is more exposed to injury. Therefore, researchers have proposed different methods, such as different types of stretching for recovery, improving the effects of fatigue and reducing the risk of injury. Regarding the literature of the effects of different stretching techniques on performance and durability in future competitions, contradictory and limited results have been reported. Then, we aimed to compare the effects of slow DS, fast DS, and SS on recovery of performance, ROM, balance, and joint position sense of healthy adults and to investigate the sustainability of these effects over a subsequent hour. The main hypothesis of the present study is that after fatigue, the intergroup effects In the stretching of slow DS, fast DS and SS, there is no significant difference on the recovery factors of function, balance and proprioception of healthy adults. The researchers are looking for a response to the question, "Which type of stretching is more useful in recovering sports performance?".
Methods
Ethics Statement
The participants were instructed about any possible risks related to the present procedures and they signed a written informed consent. The present study was approved by the local Ethical Committee of Shahid Bahonar University of Kerman (IR.UK.REC.1401.028). The authors followed the principles outlined in the Declaration of Helsinki.
Participant
Fifteen collegiate healthy females (age 23.86 ± 2.57 years; height 164 ± 4.47 cm; mass 59.28 ± 7.09 kg), volunteered for the present study. Women with a body mass index (BMI) between 21 and 25 kg/m2, a history of lower limb injury, trauma, or disease within the previous six years, limited range of motion, and no participation in a lower limb stretching program were the inclusion criteria. The Physical Activity Readiness Questionnaire, or PAR-Q, (Thomas et al., 1992) was also used to assess health. The sample size of 15 physical education students was determined using the G*Power software (Version 3.1.9.4) (repeated measure ANOVA, α = 0.05, ES = 0.40) with the statistical power of 0.9 [27]. The participants were involved in four separate sessions of slow dynamic stretching (SDS), fast dynamic stretching (FDS), static stretching (SS), and control condition (CC; without stretching). The four sessions were separated by 48 h and their order was randomized [28, 29]. The participants avoided any form of intense physical activities at least two days before testing sessions. Also, during this period, participants abstained from alcohol and caffeine. Generally, participants were recreationally active in several sports but were not engaged in any official competition or regular intensive physical activities at that time of the study. Participants with lower extremity joints or muscular diseases were excluded from study. The regular use of drugs as well as the presence of any cardiovascular and pulmonary diseases or who had participated in massage, foam roller, hydrotherapy protocol, or had heavy physical activities in 24-h prior the test (based on their self–reports and medical records) were considered as exclusion criteria.
Procedure
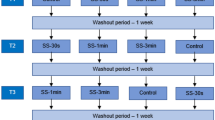
Forty-eight (48) hours prior to the testing procedure, all participants attended a 2-h familiarization session to introduce the tests and complete the personal and consent forms. Then, height, and body mass were measured. Additionally, the dominant leg, which was determined by asking the participants which leg they would predominantly use to kick a ball, was designated as the test leg [30]. One-repetition maximum (1RM) was measured by equation; 1RM = Weight/1 − 0.02 (Rep) (3). At each session after a 5-min warm-up exercise of between 70–80 revolutions per minute (RPM) at an intensity of 1 kilopond (Monark Exercise, 839 E, Sweden) [31]. participants performed tests in a random order. Measures consisted of strength and power performance (vertical jumps and maximal voluntary isometric contraction (MVIC) force / strength), ROM (flexibility), balance and joint position sense (JPS). Subsequently, participants performed a fatigue protocol (4 sets of knee extensions and knee flexion at 60% of 1 repetition maximum (RM) to exhaustion), which was followed in a randomized order by SDS, FDS, SS, and CC conditions and then performed post-tests after 5-min and 1 h (Fig. 1) [32]. During the testing process, conditions for all participants, including lighting, temperature and noise, were the same for all participants. We encouraged all participants to maintain similar eating habits and sleeping patterns. Testing measures took approximately 30-min to complete. The assessments were performed over four experimental sessions, with each session being spaced apart by a duration of 48 to 72 h [28, 29]. Each testing measurement was supervised by one of the researchers (who was blinded to each participants stretching condition) and conducted between 8 and 11 am.

Overview of the test procedure (CMJ = counter movement jump, SJ = Sargent jump, ROM, range of motion, JPS = joint position sense, CC = control condition, h = hour, min = minute)
The fatigue protocol in this study included 4 sets with 60% 1RM knee extension with a knee extension machine for quadriceps and 4 sets with 60% 1RM knee flexion movement with a Lying Leg Curl machine for the hamstrings (Fig. 2). In addition, between each set, a three-minute rest period was provided [33]. Fatigue in this study was operationally defined as the point at which participants were unable to perform full knee flexion and extension. Additionally, the Rating of Perceived Exertion (RPE) was assessed as an indicator reflecting the intensity of training, with a target RPE score exceeding 17 signifying that the participants perceived the training as "very hard." More specifically, at the end of each set, the person was considered exhausted when they could no longer complete a full knee flexion and extension repetition of movement (which meant their ROM had decreased by more than 30%) and gave the exercise a score of 17 on the RPE scale [34, 35].

Fatigue protocols with knee extension machine and lying leg curl machine
Stretching protocols
After the fatigue protocol, the stretching for the hamstrings included standing hamstrings stretch (standing position with the feet hip-width apart and extended knees, the participants flexed forward at the hips, lower their head toward the floor and finally wrapping their arms around lower legs) and lift the leg up (from the initial standing position, one leg with the knee fully extended is flexed from the hip joint and moves towards the trunk). The stretching for the quadriceps included standing quadriceps stretches (The subject stands on one leg and flexes the contralateral knee and maintains balance with one hand on the wall, then moves the flexed knee back as far as possible. If necessary, to increase the knee flexion stretch, the hand slowly pulls the heel towards the gluteal muscles.) and forward lunges (a large forward stride with the feet hip-width apart; the pelvis is lowered toward the floor; and the anterior knee is bent as much as possible). The same exercises were used in all stretching protocols (SDS, FDS and SS), but in the SDS and FDS protocols, muscles were stretched using the dynamic mode, while in the SS regime the exercises were performed in static positions after reaching the maximum amplitude [36]. With SDS and FDS, each movement was performed for 30 s, in which six repetitions were completed. FDS was performed at 100 beats/min and SDS at 50 beats/min [17]. The rest between sets and exercises (6 sets of 30 s) was 10-s as well. The total duration of the entire stretching exercises protocol was approximately 7:30-min. Furthermore, all participants rested for 5-min between the stretching protocol and measurements, also in the non-stretching (control) session participants rested for 5-min between the fatigue protocol and measurements.
Vertical Jumps
The countermovement jump (CMJ) started with the participants standing in an upright position, hands on the hips to avoid the contribution of the arms to the jumping performance. The CMJ involved a rapid downward movement of the knee to approximately 90° flexion, followed by a quick vertical upward movement as high as possible, all in one sequence. Squat jump (SJ) was used to measure leg strength in the concentric mode, with the movement starting from a static 90° knee flexion position. This study used the Jump-and-Reach Method with wall tape to assess jump height. This approach has been introduced for field evaluation in addition to its relative look among researchers. Because this approach provides the desired outcome more quickly and with less equipment [37]. (CMJ; ICC = 0.98, SJ; ICC = 0.97) [38].
Knee Extensors and Flexors MVIC Force
A hand-held dynamometer (HHD) (Lafayette manual muscle testing system model 01163; Lafayette Instrument Company, Lafayette, IN) was used to test the dominant leg. The intra-rater reliability of HHD is good to excellent (ICC = 0.80–0.96) [39]. A standard therapy bed was used with an unstretched strap to attach the dynamometer to the leg.. HHD was fixed with a rigid belt perpendicular to the ankle (five cm above the malleoli), with a pad between the tibia and the dynamometer to reduce the discomfort caused by the contact. Participants completed three MVIC for 5-s, with a 60-s rest after each trial. Participants held their arms onto the chest to stabilize their trunk and pelvis. The participants performed two submaximal efforts as a familiarization trial and then performed knee extension and knee flexion two times with 1-min rest interval [40]. The tests were conducted for quadriceps muscle while participants sitting on a leg extension machine and hamstrings muscle strength were evaluated in a prone position. In both tests, the strap was secured to limit knee flexion to 85 degrees during extensor and flexor contractions [41]. The maximum force in kilograms was recorded for each test [42].
Dynamic balance test
Dynamic balance was evaluated using the Y-balance test that is performed on a grid of three lines. Test–retest reliability were reported moderate to excellent for the right limb (ICC 0.681- 0.908) and moderate to good for left limb (ICC 0.714—0.811) [43]. The foot of the dominant leg was positioned in the center of the grid, so that the foot was bisected equally in the anteroposterior and medial–lateral planes. It was performed by pushing the prepared wooden box with the tip of the foot in the anterior, posterior, and postero-lateral directions (as far as possible along the designated line), using an instrument composed of the Y-balance test form on the floor [44]. Participants were asked to keep their hands on their iliac crests and to keep the heel of their stance leg on the ground and avoid using the reaching leg for a substantial amount of support at any time through the trials. The sum of all measured values was divided by two times the participant's limb length (limb length was measured from the anterior superior iliac spine (ASIS) to the distal end of the medial malleolus (cm)), multiplied by 100, and divided into the composite scores for the analysis (excursion distance/leg length) × 100 = %maximum reach distance) [44, 45]. The higher excursion distance reflected the greater dynamic balance.
Range of Motion (ROM)
The sit-and-reach test (SR) was used to evaluate trunk and lower extremity ROM. The SR has shown to have a high intra-class correlation coefficient, (ICC = 0.98) [46].The Baseline® (Cooper Institute/YMCA, AAHPERD) device was used for evaluation. The participants were instructed to place their heels on the device while in the sitting position with their trunk flexed at 90° flexion. After the participants’ arm length were determined by the device, they were asked to push the device with their fingertips without raising their knees and reach forward as far as possible. Participants slowly pushed the indicator forward as far as possible. The measurement was performed three times. The average of the results was recorded as the result of the SR test [47].
Knee flexion range of motion (ROM)
Knee flexion ROM was measured as the participant performed the modified Thomas test (ICC = 0.98) [48]. First, reflective markers were adhered to participants’ skin or tight-fitting garments on the lateral femoral epicondyle, greater trochanter, and lateral malleolus. Once placed, the markers were not removed until after the final testing procedure. All digital photographs were taken with a Canon camcorder (MV750i 8 megapixels). The tripod height was set at 92 cm, and the camera was fully zoomed-out and positioned exactly 1.8 m perpendicular to the end of a non-adjustable 76 cm high examination Table [49]. It was performed by having the participant hold his or her non-testing knee (non-dominant leg) to his or her chest, while letting the thigh and leg of the testing hip (dominant leg) hang freely. Each participant completed the test three times. Between each trial, the participant was asked to stand up from the table. The average of each participant's three trials was then used for analyses [50].
Joint position sense (JPS)
Knee JPS was measured using digital photography with a Canon camcorder (MV750i 8 megapixels). The reliability of this measurement method with AutoCAD software has been reported as high (ICC = 0.97) [51]. Participants were prepared for assessment with application of adhesive markers on the greater trochanter of the dominant leg, lateral tibiofemoral joint line and lateral malleolus [52]. A goniometer was fixed at 45° knee flexion on a bar next to the participant. Participant sat on the chair, then examiner passively extends the knee joint from the starting position (starting knee angle of 90° flexion) to the target angle of 45° at a very slow speed [53]. After holding the leg in this position for 5-s, the examiner returned the leg to the starting position. The participants were then asked to actively reproduce the same knee angle that was passively positioned by the examiner [30, 54]. During the experiments, participants were blindfolded and wore headphones to eliminate visual and auditory cues. The mean joint positioning error of the two measurement degrees of error from the target position were recorded for analysis. Lower mean error scores indicated the better knee JPS [51].
Statistical Analyses
Statistical analysis was performed using the SPSS Version 26 (Armonk, NY: IBM Corp.). The Levene's and Shapiro–Wilk tests were employed for assessing homogeneity of variance among conditions and normality of the distribution of scores (p > 0.05). A 2-way mixed repeated measure ANOVA with time (pre–test vs. 5-min vs. 1-h) and conditions (SDS vs. FDS vs. SS vs. CC); as factors was performed for all dependent variables. When condition-time interactions were observed, the post-hoc Bonferroni test was conducted to identify pairwise differences The effect size was assessed by partial eta squared, and considered as either small (pη2 = 0.01), medium (pη2 = 0.06), or large (pη2 = 0.14) [27]. A significant level was accepted at p-value < 0.05 for all statistical parameters.
Results
Countermovement Jump (CMJ) Height
The results showed significant condition and time interactions (F6,112 = 4.49, p < 0.0001, pη2 = 0.19) with significant jump height decreases in the CC 5-min (p = 0.001, 14.5%) and 1-h (p = 0.009, 2.1%) after the fatigue protocol. The results showed significant decreases in jump height after SS among times (F2,112 = 7.93, p = 0.001, pη2 = 0.12). Moreover, significant jump height decreases at 5-min (p = 0.017, 7.9%) after SS was revealed. But the results did not show any main effects for conditions (F3,56 = 0.880, p = 0.457), (Table 1).
Squat Jump (SJ) Height
Significant interactions between condition and time (F6,110 = 3.74, p = 0.002, pη2 = 0.17) with decreases in jump height at 5-min after fatigue protocol in the CC (p = 0.002, 10.1%) and SS (p = 0.015, 7.8%). Main effect for time showed significant decreases in jump height (F2,55 = 4.68, p = 0.013, pη2 = 0.14). But the results did not show any main effect for conditions (F3,56 = 0.966, p = 0.415), (Table 1).
MVIC of hamstrings and quadriceps
Significant interactions between condition and time for hamstrings (F6,112 = 8.14, p < 0.0001, pη2 = 0.31) and quadriceps MVIC strength (F6,112 = 6.86, p < 0.0001, pη2 = 0.27) were revealed. Significant decreases in CC 5-min after fatigue protocol in hamstrings (p = 0.001, 14.1%) and quadriceps (p = 0.001, 14.0%) MVIC strength were found. Moreover, significant decreases in hamstrings (p = 0.001, 12.3%) and quadriceps (p = 0.01, 6.9%) MVIC strength, 5-min after SS was found. The results show significant main effects for times for hamstrings (F2,55 = 6.03, p = 0.004, pη2 = 0.18) and quadriceps MVIC strength (F2,55 = 7.25, p = 0.002, pη2 = 0.21). The results show significant main effects for conditions in hamstrings (F3,56 = 3.40, p = 0.02, pη2 = 0.15) and quadriceps MVIC strength (F3,56 = 4.50, p = 0.007, pη2 = 0.19). Hamstrings MVIC strength following SDS was significantly greater than control (p = 0.035, ES = 1.9). Similarly, quadriceps MVIC strength was higher with SDS (p = 0.006, ES = 2.1) and FDS (p = 0.047, ES = 1.4) versus control (Table 1).
Balance
The results showed significant interactions between condition and time (F6,112 = 6.32, p < 0.0001, pη2 = 0.25). The results showed significant decreases in balance among times (F2,112 = 12.52, p < 0.0001, pη2 = 0.18). Significant decreases in CC after 5-min (p = 0.001, 6.7%) and 1-h (p = 0.013, 3.9%) was found. But the results did not show any main effects between conditions (F3,56 = 0.286, p = 0.835) (Table 2).
ROM (SR and Thomas tests)
The results showed significant interactions between condition and time in SR (F6,112 = 2.76, p = 0.016, pη2 = 0.13) and Thomas test (F6,110 = 6.82, p < 0.0001, pη2 = 0.27). The results showed significant main effect differences among times in SR (F2,112 = 3.84, p = 0.024, pη2 = 0.06) and Thomas (F2,55 = 7.25, p = 0.002, pη2 = 0.20) tests. Significant increase in SR scores in SDS after 5-min (p = 0.002, 10.8%), and 1-h (p = 0.017, 6.9%) were revealed. Significant increase of Thomas scores after 5-min in SDS (p = 0.001, 12.2%), FDS (p = 0.04, 9.2%), and SS (p = 0.037, 8.2%) were detected. A significant decrease in Thomas score in CC after 5-min (p = 0.004, 9.5%) was exposed. The results did not show any main effects between conditions in SR test (F3,56 = 0.36, p = 0.779). The results show significant main effect differences between conditions in Thomas test (F3,56 = 3.66, p = 0.018, pη2 = 0.16). SDS showed significantly (p = 0.014) greater ROM compared to control (Table 2).
Joint Position Sense (JPS)
The results showed significant interactions between condition and time (F6,110 = 6.13, p < 0.0001, pη2 = 0.25). The results showed significant main effect differences in JPS among times (F2,55 = 3.43, p = 0.04, pη2 = 0.11). Significant increase of JPS errors in CC (p = 0.001, 55.3%) and SS (p = 0.03, 12.2%) after 5-min were found. Significant improvement in SDS (p = 0.045, 28.6%) after 5-min was found. The results show main effect differences between conditions (F3,56 = 4.77, p = 0.005, pη2 = 0.20). The differences between SDS with CC (p = 0.006) were significant (Table 2) with SDS showing less JPS errors.
Discussion
The aim of this study was to investigate the effect of the SDS, FDS, and SS on recovery of jump height, MVIC strength, ROM, balance, and JPS of healthy collegiate girls. In accordance with the literature [9, 55]. this study showed that after a knee fatigue protocol, significant, large magnitude decreases, were observed in jump height, MVIC strength, dynamic balance, JPS and knee ROM in CC (control condition). Also, the results of present study showed that after 5-min SS led to a decrease in CMJ, SJ, MVIC, knee joint ROM (quadriceps) and JPS. It revealed that SDS was able to increase or recover the pre-test values of hamstring and quadriceps MVIC force, JPS, and knee extensors ROM after 5-min. Also, recovery of all factors to pre-test values were observed after 1-h (after the fatigue protocol) with SS, SDS, and FDS. Only SR scores after 1-h increased compared to pre-test after SDS condition.
Five minutes following the fatigue protocol, all measures were significantly reduced in CC. The results showed that after 1-h of recovery, CMJ height and balance in CC still declined. According to the literature fatigue decreases muscular power and disrupts the function of proprioceptive receptors, especially muscle spindles and Golgi tendon organs, reducing their sensitivity to neural impulses, therefore possibly increasing injury risk at the end of competitions [9, 55].
Five minutes after SS the significant decrease in jump heights, MVIC knee strength, knee joint (quadriceps) ROM and JPS were still evident. But in SS condition after 1-h, the results did not show differences with pre-test. The results suggest against using SS after a fatigue protocol to recover these factors after 5-min. The results by Robbins and Scheuermann [56]. into the effects of SS on vertical jump height demonstrated a decrease in jump height following the SS protocol [56]. The main causes may be a decrease in neuromuscular activation and musculotendinous stiffness [57]. Moreover, prior research demonstrated that acute bouts of SS could lengthen muscles, and alters the motor unit's viscoelastic characteristics [13]. Hence, a muscle may develop a less-than-optimal cross bridge overlap, reducing muscular strength. Also, the muscle length tension curve, speed of the sarcomere stretch–shortening cycle, and decreased muscle activation and reflex excitability could all be impacted by these alterations [13]. The results of the previous investigation were similar with the findings from the present study that, 30 s of SS decreased power parameters [21]. However contrary to the present findings, Holt and Lambourne [58]. observed no difference in vertical jump performance after 15 s of SS in male soccer players [58]. The possible reasons for the contradictory results with the present study are the different static stretching protocols (Holt and Lambourne performed SS of hamstrings, gluteals, lower back, quadriceps, and the hip flexors). Moreover, their subjects were male soccer players, and these differences with present study may be attributed to differences in participant sex and athletic history [59].
Earlier research revealed that an increased pain threshold due to stretching (sense of pain during joint movement), may enhance knee ROM among healthy males [60]. Hence, the relative change in muscle–tendon unit stiffness is related to SS intensity [61]. Moreover, Ghaffarinejad et al., [62]. reported that SS (30 s stretch followed by a 30 s pause) improves the sensitivity of muscle spindles and neuronal message transmission to the central nervous system among healthy males and females [62]. and this may contribute to the increased ROM after SS. Also Costa et al., [55]. reported that SS did not have a negative effect on balance beyond the fatigue protocol, but it did not reduce the negative consequences of fatigue [55]. A previous study showed that a 15 s moderate SS program can enhance dynamic balance performance by increasing postural stability. In addition, it was found that increased volumes of SS and DS result in partial balancing enhancements during the star excursion balance test [55]. The contrast with the findings of the present study may be related to the use of Biodex balance system to evaluate dynamic balance following SS.
According to Larsen et al., [63]. the static stretch protocol in healthy subjects had no impact on JPS [63]. The findings of Farshidi et al., [51]. were relatively consistent with the present study as they demonstrated that whereas SS can enhance JPS, PNF and DS had greater effects compared to SS [51]. SS can alter the sensitivity of muscle receptors [9]. (e.g., Golgi tendon organs and muscle spindles) affecting proprioception. On the other hand, the more inactive nature of SS is another factor that may have an impact on the findings of the current study. Contrary to dynamic stretching, muscular contractions are not required to enhance muscle flexibility with SS. The findings suggest that the SS has no impact on the muscles' proprioception receptors [9].
The results revealed that SDS showed more improvement compared with no-stretching conditions after 5-min in hamstrings and quadriceps MVIC force, JPS, SR and knee extensors ROM. No differences in SS and FDS compared to control group except significant differences in quadriceps MVIC force after 5-min FDS. These results support that SDS is a superior stretching technique to enhance the MVIC strength, JPS, SR and knee extensors ROM after 5-min than other stretching techniques. Previous research found that DS did not improve short-term explosive performance [64, 65]. although other studies reported improve jump performance [10, 21, 66]. Moreover, the literature has shown that after DS, EMG activity during a vertical jump task was increased [18]. In general, Behm and Chaouachi [21]. explained that DS techniques are an effective way to enhance explosive muscular contractions compared to SS. It has been hypothesized that increased body and muscle temperatures are among the mechanisms through which DS enhances muscular performance [21]. by increasing the rate of nerve impulses and sensitivity of nerve receptors. Moreover, after DS, an improvement in neuromuscular function has also been linked to improvements in reflex sensitivity [18]. In contrast, Opplert and Babault [18]. found that SS had no effect on presynaptic inhibition while DS resulted in a considerable decrease. The author stated that this reduction may be explained by the quick lengthening and contraction of the muscle fibers, which do not occur during SS [18].
Salekar et al., [67]. found that both DS and SS induced significant increases in hamstrings flexibility; however, DS was more efficient than SS. Overall, DS contracts the antagonist muscle and relaxes the lengthening muscle with reciprocal inhibition. Other researchers’ state that the slow build-up of tension and lack of soreness, reduce stretch reflex response, relaxing muscles and allowing a greater extent of stretching [18, 67]. Fletcher [17]. reported that the FDS demonstrated considerably higher jump height across all tests when compared to the SDS and no stretching conditions [17]. Although the causes of these performance changes are complicated, it seems that SDS are associated with increases in heart rate and core body temperature, whereas the FDS intervention is associated with greater nervous system activation. According to the authors' hypothesis, DS could maintain or enhance the stiffness of the musculotendinous unit (MTU) and improve nerve impulse transmission, resulting in positive changes to the force–velocity relationship. Additionally, they hypothesized that the major benefits of DS include greater sensory sensitivity and increased motor unit reflexes, which improve proprioception and pre-activation. The literature suggests that a faster dynamic stretch can improve athletic performance. However, it should be noted that all of these studies were conducted to find out the optimal warm-up, so the conclusions may not apply to recovery from fatigue [17]. The results of this study confirm the hypothesis that FDS increases fatigue and may negatively affect athlete’s performance. Therefore, the result of this study supports the hypothesis that SDS may enhance recovery after knee fatigue in MVIC strength, JPS and quadriceps’ flexibility in collegiate females. In other words, SDS may more effectively attenuate fatigue.
There are several limitations that need to be considered. First, the investigators were unable to perform the intervention for a longer period (e.g., two or three months). Second, the current study did not assess the stiffness of passive tendon and delayed onset muscle soreness (DOMS). Since SS is suggested as preferable when start a flexibility program with stiff hamstrings [8]. hamstrings tightness should be considered when deciding whether to include SS or DS in a training program.
The limited number of participants and the exclusive focus on women were identified as additional limitations of this research. Moreover, future research could address these limitations and investigate the long-term effects of SDS on sport performance and reducing the risk of injuries, also researchers could use the OMNI-RES scale for sensation of fatigue that described more precisely [68].
Conclusion
It can be concluded that knee fatigue may decrease knee modifiable risk factors such as jump height, MVIC strength, dynamic balance, knee extensor ROM and JPS. The results of the present study support that SDS may induce increases in the MVIC strength, SR, quadriceps ROM and knee JPS after 5-min. According to the present results, it is suggested that the SDS could be implemented and incorporated into regular recovery program among collegiate females.
Practical Applications
Considering the significant prevalence of knee injuries in female athletes, particularly after fatigue, this research is looking for the best method to reduce the negative effects of fatigue, maintain the athlete's performance, and potentially decrease the risk of injury. The results of the current study also revealed that after performing the fatigue protocol, the parameters of jump height, MVIC strength, dynamic balance, knee extensor ROM, and JPS significantly decreased. Therefore, a person who is exhausted will experience a decrease in performance in addition to an increase in their risk of injury. Therefore, it is crucial to determine an appropriate recovery strategy in order to maintain the health of the athlete to achieve the best possible result in competitive sports. The results of the research show that slow dynamic stretching (SDS) has the ability to significantly improve the parameters of Jump height, MVIC strength, SR, quadriceps ROM, and knee JPS after fatigue. Despite noticing that the parameters of dynamic balance and JPS reduced after performing the fast dynamic stretching (FDS) method, FDS was still able to have a positive impact on Jump height, Quadriceps MVIC, and ROM variables. But after performing static stretching (SS), other parameters decreased and the only impact was helpful on the ROM factor. This research generally recommends slow dynamic stretching at this time for use as a recovery technique.
Availability of data and material
The data that support the findings of this study are available from the corresponding author, upon reasonable request. Because the data are not publicly available due to their containing information that could compromise the privacy of research participants.
References
Ozmen T, Gunes GY, Dogan H, Ucar I, Willems M. The effect of kinesio taping versus stretching techniques on muscle soreness, and flexibility during recovery from nordic hamstring exercise. J Bodyw Mov Ther. 2017;21:41–7.
Huygaerts S, Cos F, Cohen DD, et al. Mechanisms of hamstring strain injury: Interactions between fatigue, muscle activation and function. Sports. 2020;8:65.
Bourne MN, Webster KE, Hewett TE. Is fatigue a risk factor for anterior cruciate ligament rupture? Sports Med. 2019;49:1629–35.
Edmunds R, Dettelbach A, Dito J, et al. Effects of foam rolling versus static stretching on recovery of quadriceps and hamstrings force. J Bodyw Mov Ther. 2016;20:146.
Behm DG. The science and physiology of flexibility and stretching: Implications and applications in sport performance and health. Routledge; 2018.
Behm DG AS, Daneshjoo A, Hadjizadeh Anvar S, Graham A, Zahiri A, Goudini R, Edwards C, Culleton R, Scharf C, Konrad A. Acute effects of various stretching techniques on range of motion: A systematic review with meta-analysis. Sports Medicine accepted December 13, 2022.
Behm DG, Kay AD, Trajano GS, Alizadeh S, Blazevich AJ. Effects of stretching on injury risk reduction and balance. Journal of Clinical Exercise Physiology. 2021;10:106–16.
Coons JM, Gould CE, Kim JK, Farley RS, Caputo JL. Dynamic stretching is effective as static stretching at increasing flexibility. Journal of Human Sport and Exercise. 2017;12:1153–61.
Moradi A, Rajabi R, Minoonejad H, Aghaei M. The acute effect of static stretching of quadriceps, hamstrings and gastrocnemius muscles on knee joint position sense in football players. Physical Treatments. 2014;4:83–9.
Dallas G, Smirniotou A, Tsiganos G, Tsopani D, Di Cagno A, Tsolakis C. Acute effect of different stretching methods on flexibility and jumping performance in competitive artistic gymnasts. J Sports Med Phys Fitness. 2014;54:683–90.
Stojanovic MD, Mikic M, Vucetic V, et al. Acute effects of static and dynamic stretching on vertical jump performance in adolescent basketball players. Gazzetta Medica Italiana-Archivio per le Scienze Mediche. 2022;181:417–24.
Behm DG, Blazevich AJ, Kay AD, McHugh M. Acute effects of muscle stretching on physical performance, range of motion, and injury incidence in healthy active individuals: A systematic review. Appl Physiol Nutr Metab. 2016;41:1–11.
Barbosa GM, Dantas GAF, Silva BR, Souza TO, Vieira WHB. Static or dynamic stretching program does not change the acute responses of neuromuscular and functional performance in healthy subjects: A single-blind randomized controlled trial. Revista Brasileira de Ciências do Esporte. 2018;40:418–26.
Serefoglu A, Sekir U, Gür H, Akova B. Effects of static and dynamic stretching on the isokinetic peak torques and electromyographic activities of the antagonist muscles. J Sports Sci Med. 2017;16:6–13.
Dallas G, Theodorou A, Paradisis G. The effect of different duration of dynamic stretching on sprint run and agility test on female gymnast. Journal of Physical Education and Sport. 2019;19:268–72.
Konrad A, Nakamura M, Bernsteiner D, Tilp M. The accumulated effects of foam rolling combined with stretching on range of motion and physical performance: A systematic review and meta-analysis. J Sports Sci Med. 2021;20:535–45.
Fletcher IM. The effect of different dynamic stretch velocities on jump performance. Eur J Appl Physiol. 2010;109:491–8.
Opplert J, Babault N. Acute effects of dynamic stretching on muscle flexibility and performance: An analysis of the current literature. Sports Med. 2018;48:299–325.
Gamlath HG, Wijethunga W, Weerasinghe S. Effect of static and dynamic stretching warm-up methods on agility, speed and leg power performance in school level netball players. Journal of Sports and Physical Education Studies. 2021;1:19–25.
Behm DG, Kay AD, Trajano GS, Blazevich AJ. Mechanisms underlying performance impairments following prolonged static stretching without a comprehensive warm-up. Eur J Appl Physiol. 2021;121:67–94.
Behm DG, Chaouachi A. A review of the acute effects of static and dynamic stretching on performance. Eur J Appl Physiol. 2011;111:2633–51.
Sekir U, Arabaci R, Akova B, Kadagan S. Acute effects of static and dynamic stretching on leg flexor and extensor isokinetic strength in elite women athletes. Scand J Med Sci Sports. 2010;20:268–81.
Turki O, Chaouachi A, Behm DG, et al. The effect of warm-ups incorporating different volumes of dynamic stretching on 10-and 20-m sprint performance in highly trained male athletes. The Journal of Strength & Conditioning Research. 2012;26:63–72.
Carvalho FL, Carvalho MC, Simão R, et al. Acute effects of a warm-up including active, passive, and dynamic stretching on vertical jump performance. The Journal of Strength & Conditioning Research. 2012;26:2447–52.
Matsuo S, Iwata M, Miyazaki M, et al. Changes in flexibility and force are not different after static versus dynamic stretching. Sports Medicine International. 2019;3:E89–95.
Chen C-H, Chiu C-H, Tseng W-C, et al. Acute effects of combining dynamic stretching and vibration foam rolling warm-up on lower-limb muscle performance and functions in female handball players. The Journal of Strength & Conditioning Research 2023:In press.
Pallant J. Spss survival manual: A step by step guide to data analysis using ibm spss. Routledge; 2020.
Kennedy R, Drake D. The effect of acute fatigue on countermovement jump performance in rugby union players during preseason. J Sports Med Phys Fitness. 2017;57:1261–6.
Dawson B, Gow S, Modra S, Bishop D, Stewart G. Effects of immediate post-game recovery procedures on muscle soreness, power and flexiblity levels over the next 48 hours. J Sci Med Sport. 2005;8:210–21.
Miura K, Ishibashi Y, Tsuda E, Okamura Y, Otsuka H, Toh S. The effect of local and general fatigue on knee proprioception. Arthroscopy: The Journal of Arthroscopic & Related Surgery. 2004;20:414–8.
Lowe T, Dong XN. The use of hamstring fatigue to reduce quadriceps inhibition after anterior cruciate ligament reconstruction. Percept Mot Skills. 2018;125:81–92.
Afonso J, Clemente FM, Nakamura FY, Morouço P, Sarmento H, Inman RA and Ramirez-Campillo R. The effectiveness of post-exercise stretching in short-term and delayed recovery of strength, range of motion and delayed onset muscle soreness: A systematic review and meta-analysis of randomized controlled trials. Front Physiol. 2021;12:677581. https://doi.org/10.3389/fphys.2021.677581.
Mirmoezzi M, Taheri M. Effects of closed and open kinetic chain exercise induced-localized fatigue on static and dynamic balance in trained individuals. Asian J Sports Med. 2018;9(4).
Ghotbi N, Bayat M, Malmir K, Jalaei S. The effects of lower extremity muscle fatigue on dynamic balance in volleyball players. Iran Rehabil J. 2021;19:51–8.
Harato K, Morishige Y, Niki Y, Kobayashi S, Nagura T. Fatigue and recovery have different effects on knee biomechanics of drop vertical jump between female collegiate and recreational athletes. J Orthop Surg Res. 2021;16:1–7.
Gerdijan N, Perić D, Ljubojević A, Vukić Ž. Effects of static and dynamic stretching exercises on unilateral hamstring to quadriceps strength ratio. Advances in Physical Education. 2021;11:89.
Xu J, Turner A, Comfort P, et al. A systematic review of the different calculation methods for measuring jump height during the countermovement and drop jump tests. Sports Med. 2023;53:1055–72.
Markovic G, Dizdar D, Jukic I, Cardinale M. Reliability and factorial validity of squat and countermovement jump tests. The Journal of Strength & Conditioning Research. 2004;18:551–5.
Lipovšek T, Kacin A, Puh U. Reliability and validity of hand-held dynamometry for assessing lower limb muscle strength. Isokinet Exerc Sci. 2022;30:231–40.
Baschung Pfister P, de Bruin ED, Sterkele I, Maurer B, de Bie RA, Knols RH. Manual muscle testing and hand-held dynamometry in people with inflammatory myopathy: An intra-and interrater reliability and validity study. PLoS ONE. 2018;13: e0194531.
Florencio LL, Martins J, da Silva MR, da Silva JR, Bellizzi GL, Bevilaqua-Grossi D. Knee and hip strength measurements obtained by a hand-held dynamometer stabilized by a belt and an examiner demonstrate parallel reliability but not agreement. Phys Ther Sport. 2019;38:115–22.
Sinacore JA, Evans AM, Lynch BN, Joreitz RE, Irrgang JJ, Lynch AD. Diagnostic accuracy of handheld dynamometry and 1-repetition-maximum tests for identifying meaningful quadriceps strength asymmetries. J Orthop Sports Phys Ther. 2017;47:97–107.
Greenberg ET, Barle M, Glassmann E, Jung M-K. Interrater and test-retest reliability of the y balance test in healthy, early adolescent female athletes. Int J Sports Phys Ther. 2019;14:204–13.
Jo S-H, Choi H-J, Cho H-S, Yoon J-H, Lee W-Y. Effect of core balance training on muscle tone and balance ability in adult men and women. Int J Environ Res Public Health. 2022;19:12190.
Bogalho D, Gomes R, Mendes R, Dias G, Castro MA. Impact of flexibility on vertical jump, balance and speed in amateur football players. Appl Sci. 2022;12:5425.
Henriques-Neto D, Minderico C, Peralta M, Marques A, Sardinha LB. Test–retest reliability of physical fitness tests among young athletes: The fitescola® battery. Clin Physiol Funct Imaging. 2020;40:173–82.
Akınoğlu B, Paköz B, Hasanoğlu A, Kocahan T. Investigation of the relationship between sit-and-reach flexibility and the height, the leg length and the trunk length in adolescent athletes. Baltic Journal of Health and Physical Activity. 2021;13:4.
Vigotsky AD, Lehman GJ, Contreras B, Beardsley C, Chung B, Feser EH. Acute effects of anterior thigh foam rolling on hip angle, knee angle, and rectus femoris length in the modified thomas test. PeerJ. 2015;3: e1281.
Peeler J, Leiter J. Using digital photography to document rectus femoris flexibility: A reliability study of the modified thomas test. Physiother Theory Pract. 2013;29:319–27.
Vigotsky AD, Lehman GJ, Beardsley C, Contreras B, Chung B, Feser EH. The modified thomas test is not a valid measure of hip extension unless pelvic tilt is controlled. PeerJ. 2016;4: e2325.
Farshidi B, Daneshjoo A, Sahebozamani M, Konrad A. Effects of static and pnf stretching on joint position sense and range of motion after a fatigue protocol in professional male soccer players. Med Sport. 2022;75:206–17.
Irving F, Russell J, Smith T. Reliability of knee joint position sense measurement: A comparison between goniometry and image capture methods. European Journal of Physiotherapy. 2016;18:95–102.
Herrington L. Knee-joint position sense: The relationship between open and closed kinetic chain tests. J Sport Rehabil. 2005;14:356–65.
Relph N, Herrington L. The effect of conservatively treated acl injury on knee joint position sense. Int J Sports Phys Ther. 2016;11:536–43.
Costa PB, Ruas CV, Smith CM. Effects of stretching and fatigue on peak torque, muscle imbalance, and stability. J Sports Med Phys Fitness. 2017;58:957–65.
Robbins JW, Scheuermann BW. Varying amounts of acute static stretching and its effect on vertical jump performance. The Journal of Strength & Conditioning Research. 2008;22:781–6.
Kurt C, Fırtın İ. Comparison of the acute effects of static and dynamic stretching exercises on flexibility, agility and anaerobic performance in professional football players. Turk J Phys Med Rehabil/Turkiye Fiziksel Tip Ve Rehabilitasyon Dergisi. 2016;62(3).
Holt BW, Lambourne K. The impact of different warm-up protocols on vertical jump performance in male collegiate athletes. The Journal of Strength & Conditioning Research. 2008;22:226–9.
Laffaye G, Wagner PP, Tombleson TI. Countermovement jump height: Gender and sport-specific differences in the force-time variables. The Journal of Strength & Conditioning Research. 2014;28:1096–105.
Hatano G, Matsuo S, Asai Y, Suzuki S, Iwata M. Effects of high-intensity stretch with moderate pain and maximal intensity stretch without pain on flexibility. J Sports Sci Med. 2022;21:171.
Takeuchi K, Sato S, Kiyono R, et al. High-intensity static stretching in quadriceps is affected more by its intensity than its duration. Front Physiol. 2021;12: 709655.
Ghaffarinejad F, Taghizadeh S, Mohammadi F. Effect of static stretching of muscles surrounding the knee on knee joint position sense. Br J Sports Med. 2007;41:684–7.
Larsen R, Lund H, Christensen R, Røgind H, Danneskiold-Samsøe B, Bliddal H. Effect of static stretching of quadriceps and hamstring muscles on knee joint position sense. Br J Sports Med. 2005;39:43–6.
Jaggers JR, Swank AM, Frost KL, Lee CD. The acute effects of dynamic and ballistic stretching on vertical jump height, force, and power. The Journal of Strength & Conditioning Research. 2008;22:1844–9.
Samuel MN, Holcomb WR, Guadagnoli MA, Rubley MD, Wallmann H. Acute effects of static and ballistic stretching on measures of strength and power. The Journal of Strength & Conditioning Research. 2008;22:1422–8.
Hough PA, Ross EZ, Howatson G. Effects of dynamic and static stretching on vertical jump performance and electromyographic activity. The Journal of Strength & Conditioning Research. 2009;23:507–12.
Salekar B, Sharath U, Krishnareddy P. Compare the effect of static and dynamic stretching on hamstring muscle flexibility and on agility performance in tennis players. International Journal of Physical Education, Sports and Health. 2020;7:84–90.
Pakosz P, Konieczny M, Domaszewski P, Dybek T, Gnoiński M, Skorupska E. Comparison of concentric and eccentric resistance training in terms of changes in the muscle contractile properties. J Electromyogr Kinesiol. 2023;73: 102824.
Acknowledgements
Authors would like to thank all participants in this study.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
AD, MS, DB developed conceptualization the original idea and study design, EH, SH literature review and data collection and AD data analysis and interpretation, statistical analysis. AD, EH, SH wrote the manuscript and MS, DB reviewing/editing a draft of the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
All ethical principles were considered in this article. All individuals who participated in the investigation provided their informed consent and informed about the purpose of the research and its implementation sages; they were also assured about the confidentiality of their information; Moreover, They were allowed to leave the study whenever they wish, and if desired, the results of the research would be available to them. This study was approved by the Ethics Committee of Shahid Bahonar University of Kerman (IR.UK.REC.1401.028). The authors followed the principles outlined in the Declaration of Helsinki.
Consent for publication
Not Applicable.
Competing interest
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Daneshjoo, A., Hosseini, E., Heshmati, S. et al. Effects of slow dynamic, fast dynamic, and static stretching on recovery of performance, range of motion, balance, and joint position sense in healthy adults. BMC Sports Sci Med Rehabil 16, 167 (2024). https://doi.org/10.1186/s13102-024-00841-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13102-024-00841-5