
Abstract
Cardiopulmonary exercise testing (CPET) is an important tool to measure the cardiopulmonary fitness of an individual and has been widely used in athletic, clinical and research settings. Most CPET focus on analyzing physiological responses during exercise. We contend that the post-CPET recovery physiological responses offer further diagnostic and prognostic information about the health of the cardiopulmonary and metabolic systems, especially when testing apparently healthy middle-aged and older adults. However, there are limited studies that investigate physiological responses during the post-CPET recovery, and even less so in middle-aged and older adults. Therefore, this current review is aimed at discussing the contribution of post-CPET recovery parameters to cardiopulmonary health and their potential applications in aging populations. In addition to the existing methods, we propose to examine the aerobic and anaerobic recovery threshold post-CPET as novel potential diagnostic and/or prognostic tools.
Key points
-
1.
This current review discusses the contribution of post-cardiopulmonary exercise testing (CPET) recovery parameters to cardiopulmonary health and their potential applications in aging populations.
-
2.
In addition to the existing methods, we propose to examine the aerobic and anaerobic recovery thresholds post-CPET as novel potential diagnostic and/or prognostic tools.
Similar content being viewed by others
Introduction
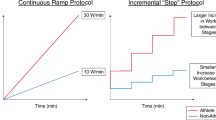
Cardiopulmonary exercise testing (CPET) is used to measure cardiorespiratory fitness and physiological responses to aerobic exercise in a wide variety of settings. As such, a plethora of exercise testing protocols (progressive incremental exercise to volitional exhaustion, time to exhaustion, constant load etc.) and modes (e.g. treadmill run/walk, cycling, rowing) are available to cater for different populations, ranging from athletes to geriatric and clinical populations. Often, the examined variables include maximal/peak oxygen consumption (V̇O2max/peak), and threshold variables (e.g. ventilatory thresholds (VT), lactate thresholds (LT) and gas exchange thresholds) [1, 2]. These threshold variables are often used to determine aerobic and anaerobic threshold of an individual, representing an individual’s submaximal cardiorespiratory fitness [1, 2].
To determine an individual’s cardiorespiratory fitness, individuals will strive to achieve his or her maximal/submaximal capacity, thereby also delineating their aerobic and anaerobic thresholds. In theory, all thresholds, in relation to either aerobic or anaerobic, should happen at the same time, for example gas exchange aerobic threshold = VT1 = LT1, but in a complex physiological system, one may happen before the other or vice versa, which depends on the individuals’ physiological system [2]. For example, the physiological system deficit in individual “A” might be the metabolic system while in individual “B” might be the pulmonary system, where both individuals may achieve similar V̇O2max/peak with distinct threshold points [1,2,3,4,5]. These distinct thresholds can thus be used for diagnosis or prognosis for specific diseases/risk factors/deficits in a complex system.
While it is certainly informative to measure cardiopulmonary fitness during CPET, the physiological state during post-exercise recovery remains an important, yet under-studied physiological parameter. The most commonly studied parameters during recovery from exercise are excess post-exercise oxygen consumption (EPOC) and heart rate recovery (HRR) [6]. The degree to which gas exchange parameters may influence post-CPET recovery have not been studied in detail. Since many physiological parameters can diagnose a risk factor or disease from exercise testing, the purpose of this review is to discuss the potential contribution of recovery parameters post-aerobic exercise (CPET and/or constant power output/speed/inclination aerobic exercise e.g. 100W cycling load for 30 min) to cardiopulmonary health, and their potential applications in middle-aged and older adults.
The aging cardiovascular, pulmonary and skeletal muscle system
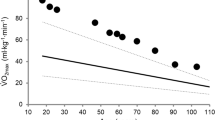
Chronological aging is associated with functional decline in the cardiovascular, pulmonary and skeletal muscle systems, particularly during dynamic, aerobic exercise. Specifically, chronological aging is associated with a gradual age-related decline in V̇O2max/peak as well as in the associated metabolic thresholds [7]. Cross-sectional studies suggest that the rate of decline in V̇O2max was faster across chronological age (males = ~ 26.0%, females = ~ 27.0% ml/min/kg per decade; 68 males/103 females [7]), while the decrease in ventilatory threshold (VT) (males = ~ 13.0%, females = ~ 13.5% ml/min/kg per decade) was less rapid with age [7]. In addition, studies suggest that the rate of decrease in V̇O2max accelerates after the ages of 40–50 years old, from ~ 0.3 to 0.6% per year around 20–30 years old to > 2.0% per year in 70–79 years old [8, 9]. The rate of decline in V̇O2max and shift in VT may be due, in part, to the age-related changes in the respiratory system [10, 11], cardiovascular system [11] and/or skeletal muscle system [12,13,14], given these are the major organ systems affecting an individual’s aerobic capacity [15, 16]. In addition, the rate of decline in VT being slower compared with the rate of decline in V̇O2max has been suggested to be due, in part, to the selective loss of type 2 skeletal muscle fibres [12,13,14], resulting in a relative increase in type 1 fibres [17]. The age-related decline in V̇O2max was also different between training status of adults in the same age group; endurance-trained adults have a higher V̇O2max than physically-active adults, while both groups also have higher V̇O2max than sedentary individuals [18]. While it is important to understand the physiological responses during CPET, analysing physiological responses during post-CPET recovery can elucidate further details of one’s cardiopulmonary/ metabolic health.
Post-CPET recovery analyses have revealed age-associated differences in cardiovascular and pulmonary variables. One study examined the effect of 70% V̇O2max exercise on post-exercise recovery gas exchange variables in older (~ 67.8 ± 7.5 years old; 6 males/2 females) and younger (~ 29.5 ± 6.4 years old; 16 males/6 females) adults [19]. The authors found that the recovery half-time kinetics of minute ventilation (V̇E), volume of carbon dioxide production per min (V̇CO2) and volume of oxygen consumption per min (V̇O2) during recovery was significantly slower in older adults compared with younger adults [19]. Age-related reduction in the central and/ or peripheral CO2 chemosensitivity contribute to the slower recovery kinetics of V̇E, V̇CO2 and V̇O2 in older adults, as there is delayed removal of exercise-induced CO2 production [20]. It has been postulated that age-related changes in lung mechanics and/or lung muscle strength in older adults are insufficient to explain the age-related reduction in ventilatory responses, therefore suggesting the reduced ability of chemoreceptors and mechanoreceptors to sense and generate appropriate neural and ventilatory response [21]. Therefore, more research is needed to establish the key age-related changes affecting the ventilatory responses. However, when comparing between well-trained younger (~ 24.5 ± 3.7 years old; 8 males, 4 females) and well-trained older adults (~ 47.3 ± 8.6 years old; 8 males, 4 females) there were no significant differences between post-exercise recovery kinetics [22]. These studies suggest that although aging leads to slower post-exercise recovery kinetics, exercise training status of an individual can mitigate this age-related decline which highlights the importance of maintaining regular exercise training across the lifespan.
As described above, chronological aging is associated with functional decline in the cardiovascular and pulmonary systems, observed during, and after dynamic exercise. This begs the questions as to whether individuals with age-related diseases will present with unique physiological differences during recovery from aerobic exercise. Therefore, it is important, in the context of age-related diseases, to examine physiological changes not limited to only during exercise, but also during the recovery period. Physiological measurements obtained in the post-exercise state will provide valuable insight into physiological changes during the aging process, as well as recovery from aerobic exercise in individuals with or without age-associated chronic diseases. At present, these two areas remain poorly understood. Therefore, we need to explore existing studies that have examined post-CPET variables in disease states, and how they related to the integration or malintegration of the cardiopulmonary/ metabolic systems.
Diseased states and the determination of post-CPET variables
Excess post-exercise oxygen consumption (EPOC)
Excess post-exercise oxygen consumption (EPOC) occurs after an acute bout of exercise, with an immediate increase in V̇O2. EPOC has been explained by the oxygen debt hypothesis, where this process is necessary for the replenishment of oxygen debt incurred to remove lactate at the onset of exercise [23,24,25]. EPOC has also been suggested to play a role, in part, in maintaining physiological and biochemical homeostasis, for example, by: (i) restoring adenosine triphosphate (ATP)-phosphocreatine (PCr) in skeletal muscle [26,27,28], (ii) replenishing blood and muscle oxygen, and (iii) redistributing ions (increased sodium–potassium pump activity) [29]. Often, EPOC is analysed for its magnitude, duration and recovery half-life. With further understanding of exercise physiology, the concept of EPOC has evolved, with the definition now stating that EPOC consists of a fast (within 1 h post-exercise) and a slow (after 1 h post-exercise) component [30]. The duration of fast and slow components are dependent on the type, intensity, and duration of exercise being performed [30]. The slow component of EPOC also supports the removal of lactate, and increased body temperature, blood flow and ventilation [30]. Hence, EPOC represents an accurate and precise means of evaluating the amount of exercise of optimal energy consumption required for health promotion [31]. Individuals with heart failure and coronary artery disease have a prolonged EPOC [32] (Fig. 1).

Variables that can be analyzed post-CPET, for the study of systemic function during post-exercise
The EPOC half-life recovery is the time taken for V̇O2 to decrease from its maximal value during aerobic exercise, to 50% of V̇O2max during post-exercise recovery. In this context, a prolonged EPOC half-life was observed in patients with chronic heart failure (~ 97 to 155 s; 72 males; ~ 50 years old) after a bout of maximal aerobic exercise, compared with healthy individuals (~ 77 s; 13 males; ~ 50 years old) [33]. The speed of half-life recovery is related to the severity of chronic heart failure [34]. The delayed time constants of V̇O2 and V̇E during recovery in individuals with chronic heart failure have been explained, in part, by a delay in the recovery of energy stores in the skeletal muscle, as demonstrated by Cohen-Solal and colleagues [33]. Other factors, such as microcirculatory changes, sustained hyperpnea, carbon dioxide retention, prolonged recovery of cardiac output, and increased cost of breathing [32, 33, 35] may also contribute to the delayed EPOC in patients with chronic heart failure.
The rate at which V̇O2 recovers to resting values has been used, in part, as an index of systemic oxidative capacity (mainly attributed to the oxidative capacity of skeletal muscle, cardiovascular, and pulmonary) in healthy individuals [26, 33]. Thus, differences in oxygen kinetics post-CPET from individuals with age-related chronic disease can be used as a diagnostic and/or prognostic tool, for example, in individuals with chronic heart failure [32, 33] and in individuals with type 2 diabetes [36]. The differences in post-CPET oxygen kinetics can be explained, for example, by impairments in metabolic [37] and/or cardiac function [33], which can affect physiological responses post-CPET. When the analysis of post-CPET oxygen kinetics is combined with other post-CPET variables, there is potential to identify specific physiological impairments for recovery.
V̇O2 recovery delay
V̇O2 recovery delay is a measure of time from the end of exercise until V̇O2 falls permanently below V̇O2peak, defined and illustrated by Bailey et al. [38], where longer duration of the recovery delay represents an impaired cardiac reserve capacity in individuals with heart failure. Heart failure patients with preserved ejection fraction (64 ± 10 years old; 15 males, 15 females), or with reduced ejection fraction (62 ± 11 years old; 18 males, 2 females) had prolonged V̇O2 recovery delays, compared with healthy control (58 ± 13 years old; 13 males, 9 females) participants (25 s vs. 28 s vs. 5 s, respectively) [38]. Further, V̇O2 recovery delay was inversely related to cardiac output augmentation during exercise in both types of heart failure patients [38]. Therefore, measuring V̇O2 recovery delay could be used to assess cardiac reserve capacity [38]. Future work should also determine whether V̇O2 recovery delay is associated with other age-related conditions, such as peripheral vascular disease, and whether it has prognostic potential.
Peak oxygen pulse
Peak oxygen pulse is calculated by dividing V̇O2max by maximal heart rate (HR) during exercise and is an indicator of stroke volume and arteriovenous oxygen (a-vO2) difference when corrected for lean body mass [39]. In cardiac patients with mild-to-moderate heart failure (HF) followed for 19 ± 12 months, those without major cardiac events had higher absolute (11.4 vs. 9.2 ml/beat) and body fat-adjusted peak oxygen pulse (15.6 vs. 11.9 ml/beat), compared with patients that suffered major cardiac events [39]. Low peak oxygen pulse was the strongest predictor of clinical events (chi sq 10.5), independent of body fat, while peak oxygen pulse adjusted for body fat showed an even stronger prediction (chi sq 12.4) [39]. In the same study, even in most subgroups (including women, obese subjects, those receiving beta-blockers, and those with class III HF), peak O2 pulse normalized for lean mass was similar to, or superior to peak VO2 for predicting major clinical events [39]. Therefore, oxygen pulse during recovery from CPET offers an attractive means to uncover potential pathophysiological outcomes in the cardiopulmonary system.
Respiratory exchange ratio (RER)
Respiratory exchange ratio (RER), CO2 produced/O2 consumed, is an indirect measure of skeletal muscle capacity for oxidative phosphorylation [40]. Post-exercise RER can be used to measure the RER overshoot- defining the highest RER value during exercise (A) and recovery (B), and defining the percentage magnitude between these 2 points (A) and (B) [41]. Time to RER max was defined by duration between (A) and (B) [41]. Individuals with kidney transplant (51.4 ± 13.0 years old) showed significant RER overshoot, with a RER magnitude lower than healthy individuals; further, the RER magnitude was able to stratify according to fitness levels [41]. This could be due to the reductions in capillary density, mitochondria density and/or the increased diffusion distance within skeletal muscle of individuals with kidney failures [42].
Heart rate recovery (HRR)
Heart rate recovery (HRR) has been suggested to reflect the balance between the reactivation of the parasympathetic nervous system and the withdrawal of the sympathetic nervous system- a delayed HRR would suggest a potential ailment in these systems. Indeed, parasympathetic nervous system reactivation is the main contributor to HRR differences obtained post-CPET, as observed between athletes (20 ± 2 years old) and patients with chronic heart failure (55 ± 12 years old) but not with healthy, but sedentary age-matched young (20 ± 4 years old) and old adults (56 ± 6 years old), with the differences being most significant at 30 s post-CPET [43].
As well, HRR has been used to predict the onset of coronary heart disease [44], cardiovascular-related mortality [45], non-cardiovascular mortality [46], and all-cause mortality [44, 47]. Up to one minute post-CPET HRR can predict mortality, with HRR at 10 s after CPET being the greatest predictor [48]. In addition, HRR does not coincide with the return of V̇O2, V̇CO2 and V̇E to pre-exercise levels, particularly in older adults [49], suggesting that HRR is an independent marker of aging.
Heart rate recovery index (HRRI)
Heart rate recovery index (HRRI) is another measure of HRR and is defined as the ratio of acceleration time of HR during exercise (time from baseline HR to HR max) to the deceleration time of HR (time from HR max to baseline HR) post-CPET [50]. Cozlac and colleagues [50] assessed whether HRRI can be used to predict the response of cardiac patients to cardiac resynchronization therapy, a therapy to normalize patients’ heart rhythm. They found that responders and non-responders to cardiac resynchronization therapy had significant differences in HRRI post-CPET [50]. The differences were associated with the cardiac phenotype and function, where responders to cardiac resynchronization therapy had significant left ventricular reverse modelling and larger left ventricular ejection fraction as compared to non-responders [50].
HRRI has also been used to assess aerobic fitness in a healthy cohort, where HRRI can predict V̇O2max, and maximum speed during CPET at 1 min post-exercise, and up to 2 and 3 min post-exercise for females (n = 130; average age = 24.6 years old), and males respectively (n = 718; average age = 27.6 years old) [51]. Future studies can examine the potential for HRRI post-CPET in middle-aged and older adults.
Prognostics for healthy aging
Given that the above recovery variables can be used to diagnose individuals with diseases, the next section will discuss the potential use of these recovery variables as a prognostics tool for healthy aging.
EPOC
In older adults (67.8 ± 7.5 years old), the slower recovery kinetics of V̇E, V̇CO2 and V̇O2, as compared to younger (29.5 ± 6.4 years old) adults [19], were attributed partly to age-related decreases in central and/or peripheral CO2 chemosensitivity, which delay the removal of exercise-induced CO2 [20] In addition, for functionally impaired older adults, EPOC was a better predictor for functional performance than either VO2peak or VO2 during exercise [52], compared with age-matched, functionally competent adults, whose VO2 values during exercise testing were better predictors for functional performance [52].
In another study, oxygen uptake in physically inactive, middle-aged adults during aerobic exercise was similar between continuous cycling (30 min at 60% V̇O2max) or interval cycling (alternating bouts of 80% V̇O2max (2 min) and 40% V̇O2max (1 min) repeated 6 times) [53]. However, interval cycling resulted in significantly higher EPOC, compared with continuous cycling, despite similar energy expenditure during both exercise modalities [53]. One explanation could be due to the energy demands between the two exercise modalities, with interval exercise more reliant on anaerobic glycolysis, compared with continuous cycling. Thus, there is greater production of H+ ions, decreased efficiency of recovery of metabolic pathways, thereby increasing oxygen demand post-exercise (observed as EPOC) during recovery.
RER
The training status of an individual indicates exercise tolerance. Frey and colleagues examined RER during post-exercise recovery from low- (LI; ~ 65% V̇O2max) versus high-intensity (HI; ~ 80% V̇O2max) aerobic exercise, between trained (27.8 ± 2.6 years old; 6 females) and untrained individuals (24.3 ± 1.6 years old; 7 females), and found no significant differences between groups [54]. However, HI exercise resulted in higher RER compared with LI exercise in both groups [54]. Furthermore, RER decreased rapidly within the first 10 min following LI and HI, and was lower than baseline throughout 60 min of recovery in untrained individuals [54]. In the trained individuals, RER also decreased rapidly through the first 10 min after LI exercise, and 20 min after HI exercise [54]. The lower RER observed during post-exercise in untrained participants suggests that untrained individuals relied more on fat oxidation during post-exercise recovery, compared with trained individuals. Also, lower RER during the post-exercise period may implicate CO2 retention in bicarbonate pools, leading to a state of acidosis by increasing hydrogen ions and lowering of pH.
Advantages of measuring post-CPET variables
Although some recovery kinetics are associated with cardiorespiratory fitness variables measured during exercise, the recovery oxygen kinetics has advantages of being independent of the level of exercise [32, 33, 55], allowing its use as a prognostics biomarker when individuals are unable to achieve maximal efforts during exercise. In addition, V̇O2peak determination depends on each individual’s motivation and test termination criteria, where both do not influence the oxygen kinetics of recovery.
Indeed, recovery oxygen kinetics is able to further prognose individuals with heart failure, where lower recovery V̇O2 is associated with higher mortality, apart from using only oxygen kinetics during CPET [56]. In addition, recovery V̇O2 is a better predictor than V̇O2peak at mortality of individuals with cardiac heart failure [56].
Combined post-CPET variables such as gas exchange and heart rate have been observed to differentiate three different forms of congenital heart lesions [57]. Although this example is not an age-related disease, it provides insights into how post-CPET variables can indicate impairment in human physiology. More studies are necessary to establish how post-CPET variables are related to the physiological systems.
Given the limited studies available for post-CPET variables on the aging population, more research is needed to further understand whether recovery kinetics can prognose other age-related diseases and improve understanding of aging physiology.
Concept of recovery variables analysis (absolute values vs. thresholds)
By further establishing which other gas exchange variables is able to indicate health risk factors, exercise interventions can be explored and recommended to prevent or minimise the potential age-related pathologies. However, most studies have analysed absolute points on individual gas exchange variables. For example, EPOC is commonly analysed for its magnitude (highest point), duration (back to baseline), and half-life (mid-point) (Fig. 2), similar to other variables measured during recovery such as HRR. These recovery variables have not been observed from a recovery threshold perspective (aerobic and anaerobic recovery thresholds; Fig. 2), where V̇O2 and V̇CO2 can be plotted to determine the point where recovery aerobic threshold occurs (inflection during recovery). Based on the concept where the 2 thresholds (aerobic and anaerobic) occur, we propose in this paper, for future studies to examine recovery thresholds in the healthy and diseased population.

An example of a typical EPOC absolute measurements (red boxes and arrows: magnitude, duration, and area under curve) and the proposed recovery threshold measurements (blue boxes and arrows: anaerobic and aerobic recovery thresholds)
Applying the concept of determining an individual’s aerobic threshold rather than absolute V̇O2peak [2], here we propose the measurement of recovery threshold during post-CPET, apart from the absolute points of an individual variable such as EPOC.
Recovery threshold measurement
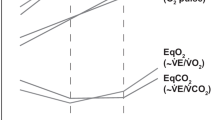
Traditionally, to detect the aerobic threshold during a bout of exercise, one would examine two variables against each other, for example, plotting V̇CO2 against V̇O2; the inflection point would then indicate the aerobic threshold (Fig. 3a), or plot V̇E against V̇CO2; the inflection point would indicate anaerobic threshold. From a recovery perspective, these recovery thresholds have not been explored and we speculate whether the inflection point (Fig. 3b) could suggest the recovery of aerobic or anaerobic threshold systems (Fig. 2). These recovery thresholds (aerobic or anaerobic systems) can indicate the demands on the cardiopulmonary/metabolic systems to return to baseline and to provide prognostic value for identifying age-related physiological decline. In addition, the slope of the recovery variable of interest, for example, the initial slope prior to the recovery threshold, and the slope after the recovery threshold (Fig. 3b) can be used to identify age-related physiological deficits, where they can be compared across age-related conditions (Fig. 3c and d). In addition, when Fig. 3a–d are combined together in a proposed 3-dimensional model (Fig. 3e), the area under the 3-dimensional curve can be compared (Fig. 3e). In addition, this concept can be applied to the proposed anaerobic recovery threshold, by using the V̇E against V̇CO2 graph for example. Of course, future studies are required to examine this potentially novel method of measuring recovery aerobic and anaerobic thresholds.

Schematic illustration plots of ̇V̇CO2 against V̇O2 a during exercise and b post-exercise of a younger female adult, and c during exercise and d post-exercise of a middle-aged female adult e hypothetical 3-dimensional graph across time (during CPET and post-CPET), comparing one younger and one middle-aged adults, where a to d are expressed in a 3-dimensional graph across time (illustration not drawn to scale). Dotted lines represent aerobic threshold of a younger (a; blue dotted line) and a middle-aged adult (c; red dotted line). Proposed recovery aerobic threshold of a younger (b; blue dotted line) and a middle-aged female adult (d; red dotted line) (unpublished results)
Given that populations with age-related diseases such as individuals with type 2 diabetes, having metabolic impairment such as lower capacity to utilise carbohydrate [58] and individuals with heart failure with impaired cardiac reserve capacity has been observed with a delayed V̇O2 recovery [38], these populations may potentially have a slower recovery threshold with a larger area under the curve for post-exercise, compared with the healthy population.
Conclusions
The use of CPET has mostly been explored during the exercise phase, with limited number of studies reporting the post-exercise recovery phase. Typically, variables (EPOC, HRR, RER) that were examined during post-exercise recovery phase were individually analysed. In this narrative review, we have proposed the idea of analysing the post-exercise recovery relationship between variables, such as plotting V̇CO2 against V̇O2, for the analysis of recovery thresholds, and the time taken to achieve these thresholds post-exercise. The analysis of post-CPET variables could potentially provide further understanding of aerobic and anaerobic recovery thresholds, and the potential to have significant utility in age-associated disease prognostication.
Availability of data and materials
Not applicable.
Abbreviations
- EPOC:
-
Excess post-exercise oxygen consumption
- HR:
-
Heart rate
- HRR:
-
Heart rate recovery
- HI:
-
High intensity
- L:
-
Liters
- LI:
-
Low intensity
- LT:
-
Lactate Threshold
- V̇O2max/peak:
-
Maximal/Peak oxygen consumption
- V̇E:
-
Minute ventilation
- min:
-
Minute
- RER:
-
Respiratory exchange ratio
- VT:
-
Ventilatory threshold
- V̇CO2 :
-
Volume of carbon dioxide produced per min
- V̇O2 :
-
Volume of oxygen consumed per min
References
Meyer T, Lucia A, Earnest CP, Kindermann W. A conceptual framework for performance diagnosis and training prescription from submaximal gas exchange parameters-theory and application. Int J Sports Med. 2005;26(S1):S38–48.
Mann T, Lamberts RP, Lambert MI. Methods of prescribing relative exercise intensity: physiological and practical considerations. Sports Med. 2013;43(7):613–25.
Scharhag-Rosenberger F, Meyer T, Gäßler N, Faude O, Kindermann W. Exercise at given percentages of VO2max: heterogeneous metabolic responses between individuals. J Sci Med Sport. 2010;13(1):74–9.
Poole DC, Rossiter HB, Brooks GA, Gladden LB. The anaerobic threshold: 50+ years of controversy. J Physiol. 2021;599(3):737–67.
Patessio A, Casaburi R, Carone M, Appendini L, Donner CF, Wasserman K. Comparison of gas exchange, lactate, and lactic acidosis thresholds in patients with chronic obstructive pulmonary disease. Am Rev Respir Dis. 1993;148:622.
Mann TN, Webster C, Lamberts RP, Lambert MI. Effect of exercise intensity on post-exercise oxygen consumption and heart rate recovery. Eur J Appl Physiol. 2014;114(9):1809–20.
Posner JD, Gorman KM, Klein HS, Cline CJ. Ventilatory threshold: measurement and variation with age. J Appl Physiol. 1987;63(4):1519–25.
McGavock JM, Hastings JL, Snell PG, McGuire DK, Pacini EL, Levine BD, et al. A forty-year follow-up of the Dallas Bed Rest and Training study: the effect of age on the cardiovascular response to exercise in men. J Gerontol Ser A Biomed Sci Med Sci. 2009;64(2):293–9.
Fleg JL, Morrell CH, Bos AG, Brant LJ, Talbot LA, Wright JG, et al. Accelerated longitudinal decline of aerobic capacity in healthy older adults. Circulation. 2005;112(5):674–82.
Lalley PM. The aging respiratory system—pulmonary structure, function and neural control. Respir Physiol Neurobiol. 2013;187(3):199–210.
Burtscher M. Exercise limitations by the oxygen delivery and utilization systems in aging and disease: coordinated adaptation and deadaptation of the lung-heart muscle axis-a mini-review. Gerontology. 2013;59(4):289–96.
Tzankoff S, Norris A. Effect of muscle mass decrease on age-related BMR changes. J Appl Physiol. 1977;43(6):1001–6.
Faulkner JA, Davis CS, Mendias CL, Brooks SV. The aging of elite male athletes: age-related changes in performance and skeletal muscle structure and function. Clin J Sport Med. 2008;18(6):501.
Nilwik R, Snijders T, Leenders M, Groen BB, van Kranenburg J, Verdijk LB, et al. The decline in skeletal muscle mass with aging is mainly attributed to a reduction in type II muscle fiber size. Exp Gerontol. 2013;48(5):492–8.
Hawley JA, Hargreaves M, Joyner MJ, Zierath JR. Integrative biology of exercise. Cell. 2014;159(4):738–49.
Wasserman K, Van Kessel AL, Burton GG. Interaction of physiological mechanisms during exercise. J Appl Physiol. 1967;22(1):71–85.
Larsson L, Sjödin B, Karlsson J. Histochemical and biochemical changes in human skeletal muscle with age in sedentary males, age 22–65 years. Acta Physiol Scand. 1978;103(1):31–9.
Fitzgerald MD, Tanaka H, Tran ZV, Seals DR. Age-related declines in maximal aerobic capacity in regularly exercising vs. sedentary women: a meta-analysis. J Appl Physiol. 1997;83(1):160–5.
Chick TW, Cagle TG, Vegas FA, Poliner JK, Murata GH. The effect of aging on submaximal exercise performance and recovery. J Gerontol. 1991;46(1):B34–8.
Brischetto M, Millman R, Peterson D, Silage D, Pack A. Effect of aging on ventilatory response to exercise and CO2. J Appl Physiol. 1984;56(5):1143–50.
Peterson DD, Pack AI, Silage DA, Fishman AP. Effects of aging on ventilatory and occlusion pressure responses to hypoxia and hypercapnia. Am Rev Respir Dis. 1981;124(4):387–91.
Hottenrott L, Möhle M, Feichtinger S, Ketelhut S, Stoll O, Hottenrott K. Performance and recovery of well-trained younger and older athletes during different HIIT protocols. Sports. 2022;10(1):9.
Hill AV, Long C, Lupton H. Muscular exercise, lactic acid, and the supply and utilisation of oxygen—Parts I-III. Proc R Soc Lond Ser B Contain Pap Biol Character. 1924;96(679):438–75.
Hill AV, Long C, Lupton H. Muscular exercise, lactic acid, and the supply and utilisation of oxygen—Parts IV–VI. Proc R Soc Lond Ser B Contain Pap Biol Character. 1924;97(681):84–138.
Hill AV, Long C, Lupton H. Muscular exercise, lactic acid and the supply and utilisation of oxygen—Parts VII–VIII. Proc R Soc Lond Ser B Contain Pap Biol Character. 1924;97(682):155–76.
Gaesser GA, Brooks CA. Metabolic bases of excess post-exercise oxygen. Med Sci Sports Exerc. 1984;16(1):29–43.
Harris R, Edwards R, Hultman E, Nordesjö L, Nylind B, Sahlin K. The time course of phosphorylcreatine resynthesis during recovery of the quadriceps muscle in man. Pflugers Arch. 1976;367(2):137–42.
Piiper J, Spiller P. Repayment of O2 debt and resynthesis of high-energy phosphates in gastrocnemius muscle of the dog. J Appl Physiol. 1970;28(5):657–62.
Pinz I, Pörtner H-O. Metabolic costs induced by lactate in the toad Bufo marinus: New mechanism behind oxygen debt? J Appl Physiol. 2003;94(3):1177–85.
Børsheim E, Bahr R. Effect of exercise intensity, duration and mode on post-exercise oxygen consumption. Sports Med. 2003;33(14):1037–60.
Gaesser GA, Poole DC. Lactate and ventilatory thresholds: disparity in time course of adaptations to training. J Appl Physiol. 1986;61(3):999–1004.
Pavia L, Myers J, Cesare R. Recovery kinetics of oxygen uptake and heart rate in patients with coronary artery disease and heart failure. Chest. 1999;116(3):808–13.
Cohen-Solal A, Laperche T, Morvan D, Geneves M, Caviezel B, Gourgon R. Prolonged kinetics of recovery of oxygen consumption after maximal graded exercise in patients with chronic heart failure: analysis with gas exchange measurements and NMR spectroscopy. Circulation. 1995;91(12):2924–32.
Myers J, Gianrossi R, Schwitter J, Wagner D, Dubach P. Effect of exercise training on postexercise oxygen uptake kinetics in patients with reduced ventricular function. Chest. 2001;120(4):1206–11.
Tanabe Y, Takahashi M, Hosaka Y, Ito M, Ito E, Suzuki K. Prolonged recovery of cardiac output after maximal exercise in patients with chronic heart failure. J Am Coll Cardiol. 2000;35(5):1228–36.
Asano RY, Sales MM, Browne RAV, Moraes JFVN, Júnior HJC, Moraes MR, et al. Acute effects of physical exercise in type 2 diabetes: a review. World J Diabetes. 2014;5(5):659.
Lima LC, Assis GV, Hiyane W, Almeida WS, Arsa G, Baldissera V, et al. Hypotensive effects of exercise performed around anaerobic threshold in type 2 diabetic patients. Diabetes Res Clin Pract. 2008;81(2):216–22.
Bailey CS, Wooster LT, Buswell M, Patel S, Pappagianopoulos PP, Bakken K, et al. Post-exercise oxygen uptake recovery delay: a novel index of impaired cardiac reserve capacity in heart failure. JACC Heart Fail. 2018;6(4):329–39.
Lavie CJ, Milani RV, Mehra MR. Peak exercise oxygen pulse and prognosis in chronic heart failure. Am J Cardiol. 2004;93(5):588–93.
Simonson DC, DeFronzo RA. Indirect calorimetry: methodological and interpretative problems. Am J Physiol Endocrinol Metab. 1990;258(3):E399–412.
Patti A, Neunhaeuserer D, Gasperetti A, Baioccato V, Vecchiato M, Battista F, et al. Overshoot of the respiratory exchange ratio during recovery from maximal exercise testing in kidney transplant recipients. Int J Environ Res Public Health. 2021;18(17):9236.
Painter P, Krasnoff JB, Kuskowski M, Frassetto L, Johansen KL. Effects of modality change and transplant on peak oxygen uptake in patients with kidney failure. Am J Kidney Dis. 2011;57(1):113–22.
Imai K, Sato H, Hori M, Kusuoka H, Ozaki H, Yokoyama H, et al. Vagally mediated heart rate recovery after exercise is accelerated in athletes but blunted in patients with chronic heart failure. J Am Coll Cardiol. 1994;24(6):1529–35.
Lipinski MJ, Vetrovec GW, Froelicher VF. Importance of the first two minutes of heart rate recovery after exercise treadmill testing in predicting mortality and the presence of coronary artery disease in men. Am J Cardiol. 2004;93(4):445–9.
Myers J, Tan SY, Abella J, Aleti V, Froelicher VF. Comparison of the chronotropic response to exercise and heart rate recovery in predicting cardiovascular mortality. Eur J Prev Cardiol. 2007;14(2):215–21.
Jouven X, Escolano S, Celermajer D, Empana J-P, Bingham A, Hermine O, et al. Heart rate and risk of cancer death in healthy men. PLoS ONE. 2011;6(8):e21310.
Cole CR, Foody JM, Blackstone EH, Lauer MS. Heart rate recovery after submaximal exercise testing as a predictor of mortality in a cardiovascularly healthy cohort. Ann Intern Med. 2000;132(7):552–5.
van de Vegte YJ, van der Harst P, Verweij N. Heart rate recovery 10 seconds after cessation of exercise predicts death. J Am Heart Assoc. 2018;7(8):e008341.
Farinatti P, Cunha F, Monteiro W, Silva N, Venturini G. Oxygen uptake, carbon dioxide production, minute ventilation and heart rate during post exercise recovery in healthy and unmed-icated elderly and young men. Int J Sports Exerc Med. 2018;4:095.
Cozlac A-R, Petrescu L, Crisan S, Luca CT, Vacarescu C, Streian CG, et al. A novel and simple exercise test parameter to assess responsiveness to cardiac resynchronization therapy. Diagnostics. 2020;10(11):920.
Mongin D, Chabert C, Courvoisier DS, García-Romero J, Alvero-Cruz JR. Heart rate recovery to assess fitness: comparison of different calculation methods in a large cross-sectional study. Res Sports Med. 2021;1–14.
Alexander NB, Dengel DR, Olson RJ, Krajewski KM. Oxygen-uptake (VO2) kinetics and functional mobility performance in impaired older adults. J Gerontol A Biol Sci Med Sci. 2003;58(8):M734–9.
Jung W-S, Hwang H, Kim J, Park H-Y, Lim K. Comparison of interval vs continuous exercise on a cycle ergometer on excess post-exercise oxygen consumption in middle-age. FASEB J. 2020;34(S1):1.
Frey GC, Byrnes WC, Mazzeo RS. Factors influencing excess postexercise oxygen consumption in trained and untrained women. Metabolism. 1993;42(7):822–8.
Nanas S, Nanas J, Kassiotis C, Nikolaou C, Tsagalou E, Sakellariou D, et al. Early recovery of oxygen kinetics after submaximal exercise test predicts functional capacity in patients with chronic heart failure. Eur J Heart Fail. 2001;3(6):685–92.
Fortin M, Turgeon P-Y, Nadreau É, Grégoire P, Maltais L-G, Sénéchal M, et al. Prognostic value of oxygen kinetics during recovery from cardiopulmonary exercise testing in patients with chronic heart failure. Can J Cardiol. 2015;31(10):1259–65.
Greutmann M, Rozenberg D, Le TL, Silversides CK, Granton JT. Recovery of respiratory gas exchange after exercise in adults with congenital heart disease. Int J Cardiol. 2014;176(2):333–9.
Bruce CR, Hawley JA. Improvements in insulin resistance with aerobic exercise training: a lipocentric approach. Med Sci Sports Exerc. 2004;36(7):1196–201.
Acknowledgements
Not applicable.
Funding
This work was supported by funds from the National University Health System (NUHS) seed Fund: NUHSRO/2020/005/RO5+5/Seed-Aug/03.
Author information
Authors and Affiliations
Contributions
ZX and JG conceptualized the work. ZX performed literature review, drafted and revised the manuscript. JG edited the manuscript. BG, JS, ASK, JG critically evaluated the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
All authors do not have conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Lim, Z.X., Gyanwali, B., Soh, J. et al. The potential benefits of assessing post-cardiopulmonary exercise testing (CPET) in aging: a narrative review. BMC Sports Sci Med Rehabil 15, 68 (2023). https://doi.org/10.1186/s13102-023-00671-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13102-023-00671-x