
Abstract
Background
Interventions promoting adherence to exercise-based cardiac rehabilitation (exCR) are important to achieve positive physical and psychological outcomes, but knowledge of the added value of behavioral medicine interventions for these measures is limited. The aim of the study was to investigate the added value of a behavioral medicine intervention in physical therapy (BMIP) in routine exCR on psychological outcomes and health-related quality of life (HRQoL) versus routine exCR alone (RC).
Methods
A total of 170 patients with coronary artery disease (136 men), mean age 62.3 ± 7.9 years, were randomized at a Swedish university hospital to a BMIP plus routine exCR or to RC for four months. The outcome assessments included HRQoL (SF-36, EQ-5D), anxiety and depression (HADS), patient enablement and self-efficacy and was performed at baseline, four and 12 months. Between-group differences were tested with an independent samples t-test and, for comparisons within groups, a paired t-test was used. An intention-to-treat and a per-protocol analysis were performed.
Results
No significant differences in outcomes between the groups were shown between baseline and four months or between four and 12 months. Both groups improved in most SF-36 domains, EQ-VAS and HADS anxiety at the four-month follow-up and sufficient enablement remained at the 12-months follow-up.
Conclusion
A BMIP added to routine exCR care had no significant effect on psychological outcomes and HRQoL compared with RC, but significant improvements in several measures were shown in both groups at the four-month follow-up. Since recruited participants showed a better psychological profile than the general coronary artery disease population, further studies on BMIP in exCR, tailored to meet individual needs in broader patient groups, are needed.
Trial registration number NCT02895451, 09/09/2016, retrospectively registered.
Similar content being viewed by others

Background
Depression and anxiety are common in patients with coronary artery disease (CAD) [1, 2] and are associated with an increased risk of mortality [1, 3] and reduced health-related quality of life (HRQoL) [4]. The benefits of exercise-based cardiac rehabilitation (exCR) for the secondary prevention of CAD are well established in clinical outcomes, such as reduced mortality and the risk of hospital readmission [5, 6], improved cardiovascular risk factor control [6] and aerobic exercise capacity [7]. ExCR has also shown positive effects on HRQoL [8, 9], anxiety and depression [10]. However, these patient-reported outcome measurements have been less studied in exCR than clinical outcomes.
Despite its proven efficacy, exCR remains widely underused [11]. At present, there is weak evidence of the effects of interventions aiming to increase adherence to exCR [12]. Behavioral medicine interventions have been used in a few studies of exCR to increase adherence to exercise programs and improve their physical and psychological outcomes [12,13,14,15,16]. Focht et al [16] reported favorable changes in HRQoL after participation in a behavioral medicine intervention within exCR [16]. Our present study used behavior change techniques based on control theory [17] to support an increase in self-efficacy for adherence to exCR [18]. Interventions using combinations of behavioral change techniques, derived from the control theory, such as self-monitoring, specific goal setting and feedback, have been shown to be effective in promoting exercise behavior in healthy adults [19]. These behavior change techniques have also shown to be positively associated with rehabilitation outcomes in patients with cardiac disease [13, 20].
The published main results [18], comparing exCR with or without a behavioral intervention in physical therapy (BMIP) added to routine care, showed significant intra-group improvements in exercise capacity for both groups at the end of the intervention. However, these changes did not differ significantly between the groups. In addition, improved exercise adherence was shown if a BMIP was added to exCR compared with routine exCR care alone (RC) [18]. Promoting adherence to exCR is important to improve positive health benefits [21]. However, more studies that evaluate the added value of behavioral medicine interventions in exCR on psychological outcomes and HRQoL are needed. The purpose of this pre-defined secondary analysis of the current study was to investigate the added value of a BMIP in routine exCR care on psychological outcomes and HRQoL versus routine exCR care alone.
Methods
Study design
This is an open-labeled, randomized, controlled trial.
Participants
Patients were screened consecutively for study inclusion at a coronary care unit at a Swedish university hospital based on the following inclusion criteria: an index event due to type 1 myocardial infarction and/or percutaneous coronary intervention, age ≥ 18 years and < 75 years. The exclusion criteria were: the inability to understand the Swedish language and serious physical or mental health issues interfering with participation in exCR. Ethical approval was received from the Regional Ethical Review Board in Linköping, Sweden (registration number: 2015/209-31) and an amendment (registration number: 2018/383-32). Each participant provided informed written consent before entering the study. All methods were performed in accordance with the Declaration of Helsinki. The study is retrospectively registered at ClinicalTrials.gov (NCT02895451, 09/09/2016).
Procedure
Physical therapists at the coronary care unit, received daily information about patients eligible for inclusion in the study and asked potential patients about participation. Baseline testing took place within two to three weeks after discharge. After finishing the baseline tests, the patients were randomized 1:1, using sealed, opaque envelopes, to a BMIP, combined with routine exCR care, or to routine exCR care alone (RC) for four months. Due to organizational reasons, the physical therapists performing the tests were not blinded to the intervention given. Three experienced physical therapists were responsible for the tests, and one experienced physical therapist, not involved in the testing procedure, was responsible for the BMIP intervention. The methods have been described in detail elsewhere [18, 22].
Intervention
Table 1 describes behavior change techniques included in the present study and illustrates the differences in these behavior change techniques between BMIP and RC. The following behavior change techniques, based on the control theory, were used; prompt specific goal setting, prompt review of behavior goals, prompt self-monitoring of behavior, and the provision of feedback on performance [23]. The control theory describes a model of self-regulation [17] and is part of the Social Cognitive Theory of Self-Regulation [24] in which self-efficacy is important when it comes to changing a behavior [25]. Exercise adherence was defined as meeting at least 75% of the recommended exercise dose according to exCR guidelines [21, 26].
Routine exCR care
The RC group followed routine exCR care. The exercise program was individually prescribed, based on tests of physical fitness, and was performed at the exCR center twice a week, under the supervision of a physical therapist. Each session included aerobic exercise for 20–60 min at an intensity of 40–85% of VO2max, corresponding to 12–17 according to Borg´s Rating of Perceived Exertion Scale, in combination with resistance exercise containing 8–10 different exercises, 10–15 repetitions in 1–3 sets [21, 26]. Patients were also instructed to perform one home-based aerobic exercise session/week, to achieve the recommendation of at least three aerobic exercise sessions/week. When preferred by patients, the choice to perform the exCR in a home-based setting was accepted. Three visits to a physical therapist for outcome assessment at baseline, four- and 12-months follow-up was part of the routine exCR care. Patients who performed the exCR program in a hospital-based setting also interacted with the physical therapist during the exercise sessions. Routine care did not include any structured intervention to control or increase adherence. However, since certain behavior change techniques, such as social support and verbal persuasion, already are included in routine exCR care, these were equal to all participants in the study. Furthermore, following routine exCR care, general goal setting for the exercise program were included. Patients also reported their home-based exercise sessions in an exercise diary, but no further feed-back or follow-up was provided in the RC arm.
Behavioral medicine intervention
Specific goal setting and re-evaluation of goals
The BMIP intervention began with a meeting with a physical therapist for detailed planning and specific goal setting for the exCR program including a discussion about motivation and self-efficacy. Facilitators and barriers, together with an appropriate action plan in relation to achieving the exercise goals, were identified. The exercise goals were re-evaluated both during and at the end of the intervention.
Self-monitoring and feedback
The performed exercise dose was self-monitored and documented in an exercise diary. The physical therapist gave feedback on the exercise diary every three weeks, comprising feedback on achieved goals, potential barriers, and the opportunity to discuss strategies to increase adherence. Visual feedback on physical activity levels, using accelerometer data, was also given at nine weeks. At the four-month follow-up, a meeting with the physical therapist to discuss goal achievement, intervention perception and long-term exercise goals took place.
To summarize, the behavioral medicine intervention included one meeting at baseline, four follow-ups during the intervention, one follow-up at the end of the intervention and one long-term follow-up at 12 months.
Outcomes
Demographic and clinical patient characteristics were collected from patient interviews and medical records. Outcome assessment included the variables listed below and was performed at baseline, four and 12 months, except for patient enablement, which was measured at four and 12 months.
Health-related quality of life
The Short Form-36 (SF-36) comprises eight dimensions (physical functioning, role limitations due to physical problems, bodily pain, general health, vitality, social functioning, role limitations due to emotional problems and mental health), and two summary components, a physical component score and a mental component score. Items in each dimension are transformed into a score from 0 to 100, where a higher score indicates better health [27]. The EuroQoL 5 dimensions (EQ-5D) consists of five different aspects of health compiled to create an index score and a visual analog scale ranging from 0 (worst state of health) to 100 (best state of health) [28]. Both the SF-36 and the EQ-5D have been found to be reliable and valid for patients with CAD [29, 30].
Psychological outcomes
Anxiety and depression
The Hospital Anxiety and Depression Scale (HADS) consists of seven anxiety items and seven depression items from which separate anxiety (HADS-A) and depression (HADS-D) scores are calculated on a scale from 0 to 21. A cut-off score of ≥ 11 for definite cases of both HADS-A and HADS-D is recommended [31]. HADS has been shown to be reliable and valid for patients with CAD [32, 33] and lowering the cut-off score for definite cases of HADS-D from 11 to 8 has been found to improve the sensitivity of the instrument [33].
Self-efficacy
The Self Efficacy for Exercise Scale comprises nine situations that could affect participation in exercise, rated on a scale from 0 (not confident) to 10 (very confident), with a total score of 0–90. The Self Efficacy for Exercise Scale is considered reliable and valid for older adults [34] and for patients with CAD (Cavrak et al., unpublished data).
Patient enablement
The Patient Enablement Instrument consists of six questions, graded on a three-point scale ranging from 0 to 2, with a total score of 0–12, focusing on the ability to understand and cope with health issues and illness. A higher score indicates better patient enablement. The Patient Enablement Instrument has been found to be reliable and valid for patients in a primary care setting [35].
Statistical methods
Sample size calculation has previously been reported in detail [18, 22]. Descriptive statistics were used for demographic data and are presented as the means and SD, or numbers and proportions (%), as appropriate.
Missing values were handled with multiple imputation. Patient characteristics and outcome measurements at baseline were included as independent variables, while outcome measurements at four and 12 months were entered as both independent and dependent variables in the multiple imputation model. The model used the chained equations procedure (fully conditional specification method in SPSS) to complete 10 data sets [36]. Constraints were applied according to the minimum and maximum value of each variable. Entering the EQ-5D index as a variable in the imputation model posed a problem and it was therefore not included in the analyses.
The within-group change, from baseline to four months and from four to 12 months, for each outcome was analyzed with paired-samples t-tests. Between-group differences, at each time point and the change between time points, were analyzed with an independent-samples t-test. The mean with 95% confidence intervals and p-values, based on the pooled results of each analysis, is presented.
A response analysis based on demographic data and outcome measurements at baseline was conducted, comparing responders and non-responders (participants with complete missing data) at the four-month follow-up. The response analysis revealed no substantial differences, whereby missing at random could be assumed. A statistical analysis was performed using SPSS statistical software for Windows (SPSS Version 25, IBM Corporation, New York, USA).
Results
Study population and demographic data
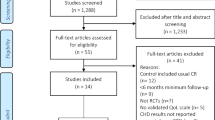
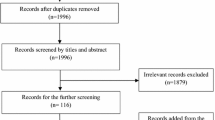
Of 453 patients, screened consecutively for study inclusion, a total of 170 patients (mean age 62.3 ± 7.9 years, 136 men) were recruited between January 2016 and October 2018. The study flowchart is presented in Fig. 1.

CONSORT flowchart of study participants
There was a significantly higher proportion of patients with unstable angina (p = 0.011) and a lower proportion of patients with non-ST-elevation myocardial infarction (p = 0.037), as the index event, in the BMIP group, compared to the RC group. No other significant differences in baseline demographics between the groups were found (Table 2).
No statistical differences between the groups were found in HRQoL or psychological outcomes at baseline, except for a significantly higher SF-36 general health (p = 0.035) and a significantly lower HADS-A (p = 0.043) in the BMIP group compared with the RC group. The EQ-5D index showed a ceiling effect at baseline in both groups (BMIP: 0.895 (SD 0.12) and RC: 0.857 (SD 0.18)).
Setting and adherence
The setting and adherence to the exCR program have previously been reported in detail [18]. Twenty patients in each group participated in hospital-based exCR, whereas 55 (BMIP) and 58 (RC) patients chose to perform the exCR in a home-based setting. Ten (BMIP) and 5 (RC) patients respectively participated in hospital-based exCR once a week in combination with home-based exercise. Twenty-three patients in the BMIP group and 13 patients in the RC group were defined as fully adherent to the exCR program [18]. This study had no serious adverse events related to exCR or the BMIP to report.
Results of psychological outcomes and health-related quality of life
No significant differences between the groups were found for any of the outcomes between baseline and four months or between four and 12 months (Tables 3 and 4). Both groups improved significantly between baseline and four months in the EQ-VAS and in all SF-36 domains, except for bodily pain, mental health, and general health, and reported a significantly lower HADS-A. Significant improvements were also shown in the SF-36 general health in the RC group and in the SF-36; mental health in the BMIP group between baseline and four months. No significant difference in the change within groups between the four- and 12-month follow-ups were found, except for a significant decline in Self Efficacy for Exercise Scale in the BMIP group (Tables 3 and 4).
Discussion
This study contributes to previous research by presenting the effects of a BMIP added to routine exCR care on psychological outcomes and HRQoL versus routine exCR care alone. The four-month follow-up showed significant improvements in most SF-36 domains, EQ-VAS and HADS-A for both groups, but no significant differences in outcomes between the groups were found between baseline and four months or between four and 12 months.
The lack of differences between the groups in psychological outcomes and HRQoL after exCR in the present study, irrespective of an addition of a BMIP, confirm the previously reported challenges of trying to achieve a behavioural change to exercise in patients as part of work to enhance rehabilitation outcomes [37,38,39,40]. The inability to detect differences between the groups in the current study, is also in line with a recent Cochrane review, concluding that no significant differences between the groups for theory-based interventions that aimed to increase adherence in a CR-setting was found [12]. Increasing adherence to exCR is important since this will improve the effect of the treatment [41]. The current BMIP was intended to increase adherence to the exCR program and to assess the benefits of exercise on psychological outcomes and HRQoL. As previously reported, although adherence was higher in the BMIP group (31%) compared with RC (19%), it was lower than expected which may be one factor to explain the non-significant differences between groups [18].
Another possible explanation for the lack of group differences in the current study is the selection of included patients. Partcipating patients in the present study reported better HRQoL compared with previously published studies in patients with CAD [42,43,44]. Moreover, in comparison with the general Swedish population, the baseline EQ-5D index was higher in our study [45], in contrast to a European study reporting a lower EQ-VAS in patients with CAD compared with a general population [42]. For the SF-36, the baseline values in our study were higher compared with previously reported reference values in patients with CAD [44] but lower compared with the general Swedish population [46]. In terms of anxiety and depression, patients in the current study reported lower baseline values as compared to a previous cardiac population and a reference population in a study by Hansen et al. [47]. This means that healthy patients with CAD with a potentially greater interest in their own health are more likely to attend this kind of study. This may lead to selection bias and the risk of underestimating possible effects of the intervention, since the room for improvement is reduced by already favorable values at baseline.
Despite this, we found significant improvements for both groups in most SF-36 domains, EQ-VAS and HADS-A at the four-month follow-up. Our results are consistent with two recently published meta-analyses, showing significant improvements in multiple SF-36 domain scores after exCR [8, 9]. Focht et al. [16] reported favorable changes in domains of SF-36 in a behavioral medicine intervention group and in men in a routine exCR group, compared with women in the routine exCR group, with the greatest improvement in patients with low baseline values [16]. A recently published European position statement describes a 10% improvement in HRQoL and anxiety/depression score after participation in exCR as a relevant quality indicator for CR [48]. However, due to the favorable baseline values in our study, the potential for an improvement of this kind in all outcomes was limited. Furthermore, consideration also needs to be taken to the fact that HRQoL and psychological outcomes typically improves by clinical course after an index cardiac event, irrespectively of intervention given [49,50,51].
Except for a significant decline in Self Efficacy for Exercise Scale in the BMIP group between the four- and 12-month follow-ups, no significant difference within or between the groups was found regarding self-efficacy for exercise. Probably this could be due to high levels of self-efficacy for exercise in both groups at baseline. In line with this, a previous study reported the highest level of self-efficacy at the beginning of the CR programme [52]. Cederbom et al. [53] found significant improvements in self-efficacy for exercise within a behavioral medicine intervention group for older women compared with receiving regular physical activity advice, however, consistent with the results of the present study, no significant difference in self-efficacy between the groups was found [53].
Patient enablement represents patients’ empowerment and ability to cope, understand, and manage with their illness [54], and has to our knowledge not previously been reported in patients with CAD. The Patient Enablement Instrument values illustrating the self-rated effect on enablement after the intervention at four months showed levels similar to the previously reported median values after treatment for other diagnostic groups [55]. A Patient Enablement Instrument value of ≥ 6 has been reported to be relevant as an indication of meaningful effect in studies of primary care [56]. The Patient Enablement Instrument values in the current study are consistent for both groups at the 12-month follow-up, showing that adequate enablement remains. This aspect is important for patients´ active role in their treatment, which in turn may have a positive impact on adherence [41].
The lack of group differences in the current study could also be explained by the design of the BMIP and the fact that certain elements of behavior change techniques, such as social support, are already included in routine exCR care. The importance of social support from healthcare providers, peers and family members has been found to be one of the most frequently described factors influencing patients participation in exCR [57, 58] and were equal to all participants in the present study. Behavior change techniques used in the present BMIP included structured and comprehensive goal setting, self-monitoring and feedback. However, general goal setting for the exercise program, some elements of general feedback and keeping record of exercise in a diary, were also provided to patients within routine exCR care. Furthermore, it was difficult to completely control for what education, support, and encouragement physical therapists and other caregivers within the comprehensive CR program gave to patients in both groups. Consequenly, it is possible that both groups were provided with enough support, and that the added value of the current BMIP, was not sufficient to make a difference between the groups.
The settings where exCR was delivered could also possibly have an impact on the results since different settings include different possibilities to provide behavior change techniques. Advantages of supervised exercise programs include access to knowledge, feedback, and support from the healthcare provider during the exercise sessions [41] as well as vicarious experiences from the group-based exCR, together with social support received by peers [59]. Unsupervised exercise programs can, on the other hand, provide increased flexibility as they can be performed whenever the patient wishes without having to adapt to specific exercise schedules [41]. In the present study, however, the proportion of patients in the different settings was equally distributed in both groups with a majority of patients taking part in a home-based setting. Behavior change techniques such as goal setting, self-monitoring and social support from family and friends have been expressed as important aspects for continued exercise after the end of an exCR program [60], while lack of support and guidance from the healthcare provider has been stated as a factor that made the maintenance of exercise more challenging [59, 60]. Supervised exercise includes advantages in possibilities to provide behavior change support during the exercise sessions, which may increase self-efficacy for the exercise program [41]. Exercise as being adaptable to the environment of the patient, has on the other hand been described as a facilitator in home-based settings [61] and may in this sense involve a minor change in the transition to maintain the exercise behavior after the completion of a phase 2 exCR program. The possible long-term effects of a BMIP in exCR need to be further explored.
In the current study, the same content of the BMIP was given to all participants and tailoring to meet indivudal needs was limited in the context of a randomized controlled trial. Nor was it possible to adapt and tailor the design of the BMIP based on aspects associated with non-attendance at exCR in an individual, such as low self-efficacy and depression [62]. The present study included a selection of patients with a better psychological profile compared with the general CAD population, highlighting the need to investigate the effect of a BMIP in broader patient groups and to use psychological screening of each patient to adapt and tailor interventions based on individual needs.
Strengths and limitations
We used a randomized, controlled design with a long-term follow-up, which is a strength when it comes to assessing the effectiveness of treatments. Reliable and validated questionnaires were used for collecting outcome data. The behavior change techniques are grounded in a theoretical framework [17], shown to be positively associated with rehabilitation outcomes in interventions in both healthy adults [19] and in patients with cardiac disease [13, 20]. Moreover, since the intervention does not require any additional education, it is easy to implement in the existing routine exCR care. The study population was mainly representative of typical Swedish exCR programs [63] which affects the generalizability of the results. On the other hand, the patients included reported better HRQoL and psychological outcome measures compared with previously published studies [42, 43, 47], and were motivated to take part in an exCR program. The sample size calculation was performed on the primary outcome in the current study and not on psychological outcomes and HRQoL which is a limitation in the study as well as the use of a single-center design. Due to organizational circumstances, physical therapists could not be blinded to the group allocation of patients. However, group allocation was kept confidential in relation to patients and the test procedure was validated by the involved physical therapists.
Conclusions
A BMIP added to routine exCR care showed no significant difference in effects on psychological outcomes and HRQoL compared with routine exCR care alone. Despite favorable baseline values, both groups improved significantly in multiple domains of the SF-36, EQ-VAS and HADS-A after completing the exCR program and sufficient enablement remained at the 12-month follow-up. There is still room for further development of BMIP in exCR, including greater tailoring to individual needs in a more heterogenous population of patients with CAD, but this needs to be investigated in future studies.
Availability of data and materials
The datasets generated and/or analyzed during the current study are not publicly available due to identifying patient data should not be shared but are available from the corresponding author on reasonable request.
Abbreviations
- BMIP:
-
Behavioral medicine intervention in physical therapy
- CAD:
-
Coronary artery disease
- EQ-5D:
-
EuroQol 5 dimensions
- exCR:
-
Exercise-based cardiac rehabilitation
- HADS:
-
Hospital anxiety and depression scale
- HADS-A:
-
Anxiety subscale of HADS
- HADS-D:
-
Depression subscale of HADS
- HRQoL:
-
Health-related quality of life
- RC:
-
Routine care
- SD:
-
Standard deviation
- SF-36:
-
Short-form 36
- VAS:
-
Visual analogue scale
References
Roest AM, Martens EJ, Denollet J, et al. Prognostic association of anxiety post myocardial infarction with mortality and new cardiac events: a meta-analysis. Psychosom Med. 2010;72:563–9. https://doi.org/10.1097/PSY.0b013e3181dbff97.
Thombs BD, Bass EB, Ford DE, et al. Prevalence of depression in survivors of acute myocardial infarction. J Gen Intern Med. 2006;21:30–8. https://doi.org/10.1111/j.1525-1497.2005.00269.x.
Meijer A, Conradi HJ, Bos EH, et al. Prognostic association of depression following myocardial infarction with mortality and cardiovascular events: a meta-analysis of 25 years of research. Gen Hosp Psychiatry. 2011;33:203–16. https://doi.org/10.1016/j.genhosppsych.2011.02.007.
Pogosova N, Saner H, Pedersen SS, et al. Psychosocial aspects in cardiac rehabilitation: from theory to practice. A position paper from the Cardiac rehabilitation section of the European association of cardiovascular prevention and rehabilitation of the European society of cardiology. Eur J Prev Cardiol. 2015;22:1290–306. https://doi.org/10.1177/2047487314543075.
Dibben G, Faulkner J, Oldridge N, et al. Exercise-based cardiac rehabilitation for coronary heart disease. Cochrane Database Syst Rev. 2021;11:Cd001800. https://doi.org/10.1002/14651858.CD001800.pub4.
Lawler PR, Filion KB, Eisenberg MJ. Efficacy of exercise-based cardiac rehabilitation post-myocardial infarction: a systematic review and meta-analysis of randomized controlled trials. Am Heart J. 2011;162:571-584.e572. https://doi.org/10.1016/j.ahj.2011.07.017.
Sandercock G, Hurtado V, Cardoso F. Changes in cardiorespiratory fitness in cardiac rehabilitation patients: a meta-analysis. Int J Cardiol. 2013;167:894–902. https://doi.org/10.1016/j.ijcard.2011.11.068.
McGregor G, Powell R, Kimani P, et al. Does contemporary exercise-based cardiac rehabilitation improve quality of life for people with coronary artery disease? A systematic review and meta-analysis. BMJ Open. 2020;10:e036089. https://doi.org/10.1136/bmjopen-2019-036089.
Candelaria D, Randall S, Ladak L, et al. Health-related quality of life and exercise-based cardiac rehabilitation in contemporary acute coronary syndrome patients: a systematic review and meta-analysis. Qual Life Res. 2020;29:579–92. https://doi.org/10.1007/s11136-019-02338-y.
Verschueren S, Eskes AM, Maaskant JM, et al. The effect of exercise therapy on depressive and anxious symptoms in patients with ischemic heart disease: a systematic review. J Psychosom Res. 2018;105:80–91. https://doi.org/10.1016/j.jpsychores.2017.11.018.
Kotseva K, Wood D, De Bacquer D. Determinants of participation and risk factor control according to attendance in cardiac rehabilitation programmes in coronary patients in Europe: EUROASPIRE IV survey. Eur J Prev Cardiol. 2018;25:1242–51. https://doi.org/10.1177/2047487318781359.
de Araujo Pio CS, Chaves GS, Davies P, et al. Interventions to promote patient utilisation of cardiac rehabilitation. Cochrane Database Syst Rev. 2019;2:Cd007131. https://doi.org/10.1002/14651858.CD007131.pub4.
Ferrier S, Blanchard CM, Vallis M, et al. Behavioural interventions to increase the physical activity of cardiac patients: a review. Eur J Cardiovasc Prev Rehabil. 2011;18:15–32. https://doi.org/10.1097/HJR.0b013e32833ace0e.
Lynggaard V, Nielsen CV, Zwisler AD, et al. The patient education - learning and coping strategies - improves adherence in cardiac rehabilitation (LC-REHAB): a randomised controlled trial. Int J Cardiol. 2017;236:65–70. https://doi.org/10.1016/j.ijcard.2017.02.051.
Sniehotta FF, Scholz U, Schwarzer R. Action plans and coping plans for physical exercise: a longitudinal intervention study in cardiac rehabilitation. Br J Health Psychol. 2006;11:23–37. https://doi.org/10.1348/135910705x43804.
Focht BC, Brawley LR, Rejeski WJ, et al. Group-mediated activity counseling and traditional exercise therapy programs: effects on health-related quality of life among older adults in cardiac rehabilitation. Ann Behav Med. 2004;28:52–61. https://doi.org/10.1207/s15324796abm2801_7.
Carver CS, Scheier MF. Control theory: a useful conceptual framework for personality-social, clinical, and health psychology. Psychol Bull. 1982;92:111–35.
Borg S, Öberg B, Nilsson L, et al. The added value of a behavioral medicine intervention in physiotherapy on adherence and physical fitness in Exercise-based cardiac rehabilitation (ECRA): a randomized, controlled trial. Patient Prefer Adher. 2020;14:2517–29. https://doi.org/10.2147/ppa.S285905.
Michie S, Abraham C, Whittington C, et al. Effective techniques in healthy eating and physical activity interventions: a meta-regression. Health Psychol. 2009;28:690–701. https://doi.org/10.1037/a0016136.
Chase JA. Systematic review of physical activity intervention studies after cardiac rehabilitation. J Cardiovasc Nurs. 2011;26:351–8. https://doi.org/10.1097/JCN.0b013e3182049f00.
Ambrosetti M, Abreu A, Corrà U, et al. Secondary prevention through comprehensive cardiovascular rehabilitation: From knowledge to implementation. 2020 update. A position paper from the Secondary Prevention and rehabilitation section of the european association of preventive cardiology. Eur J Prev Cardiol. 2020. https://doi.org/10.1177/2047487320913379.
Borg S, Oberg B, Nilsson L, et al. The role of a behavioural medicine intervention in physiotherapy for the effects of rehabilitation outcomes in exercise-based cardiac rehabilitation (ECRA) - the study protocol of a randomised, controlled trial. BMC Cardiovasc Disord. 2017;17:134. https://doi.org/10.1186/s12872-017-0557-7.
Abraham C, Michie S. A taxonomy of behavior change techniques used in interventions. Health Psychol. 2008;27:379–87. https://doi.org/10.1037/0278-6133.27.3.379.
Bandura A. Human agency in social cognitive theory. Am Psychol. 1989;44:1175–84. https://doi.org/10.1037/0003-066x.44.9.1175.
Bandura A. Social cognitive theory of self-regulation. Organ Behav Hum Decis Processes. 1991;50:248–87.
Balady GJ, Williams MA, Ades PA, et al. Core components of cardiac rehabilitation/secondary prevention programs: 2007 update: a scientific statement from the American heart association exercise, cardiac rehabilitation, and prevention committee, the council on clinical cardiology; the councils on cardiovascular nursing, epidemiology and prevention, and nutrition, physical activity, and metabolism; and the American association of cardiovascular and pulmonary rehabilitation. Circulation. 2007;115:2675–82. https://doi.org/10.1161/circulationaha.106.180945.
Ware JE Jr, Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care. 1992;30:473–83.
Rabin R, de Charro F. EQ-5D: a measure of health status from the EuroQol group. Ann Med. 2001;33:337–43. https://doi.org/10.3109/07853890109002087.
Failde I, Ramos I. Validity and reliability of the SF-36 Health Survey Questionnaire in patients with coronary artery disease. J Clin Epidemiol. 2000;53:359–65. https://doi.org/10.1016/s0895-4356(99)00175-4.
Schweikert B, Hahmann H, Leidl R. Validation of the EuroQol questionnaire in cardiac rehabilitation. Heart. 2006;92:62–7. https://doi.org/10.1136/hrt.2004.052787.
Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. 1983;67:361–70. https://doi.org/10.1111/j.1600-0447.1983.tb09716.x.
Norris CM, Ljubsa A, Hegadoren KM. Gender as a determinant of responses to a self-screening questionnaire on anxiety and depression by patients with coronary artery disease. Gend Med. 2009;6:479–87. https://doi.org/10.1016/j.genm.2009.09.001.
Stafford L, Berk M, Jackson HJ. Validity of the hospital anxiety and depression scale and patient health questionnaire-9 to screen for depression in patients with coronary artery disease. Gen Hosp Psychiatry. 2007;29:417–24. https://doi.org/10.1016/j.genhosppsych.2007.06.005.
Resnick B, Jenkins LS. Testing the reliability and validity of the self-efficacy for exercise scale. Nurs Res. 2000;49:154–9.
Roost M, Zielinski A, Petersson C, et al. Reliability and applicability of the Patient enablement instrument (PEI) in a Swedish general practice setting. BMC Fam Pract. 2015;16:31. https://doi.org/10.1186/s12875-015-0242-9.
Azur MJ, Stuart EA, Frangakis C, et al. Multiple imputation by chained equations: what is it and how does it work? Int J Methods Psychiatr Res. 2011;20:40–9. https://doi.org/10.1002/mpr.329.
Martin LR, Williams SL, Haskard KB, et al. The challenge of patient adherence. Ther Clin Risk Manag. 2005;1:189–99.
Sabate E. Adherence to long-term therapies: evidence for action. Geneva: WHO; 2003.
Dunbar-Jacob J, Erlen JA, Schlenk EA, et al. Adherence in chronic disease. Annu Rev Nurs Res. 2000;18:48–90.
De Bacquer D, Astin F, Kotseva K, et al. Poor adherence to lifestyle recommendations in patients with coronary heart disease: results from the EUROASPIRE surveys. Eur J Prev Cardiol. 2022;29:383–95. https://doi.org/10.1093/eurjpc/zwab115.
Collado-Mateo D, Lavín-Pérez AM, Peñacoba C, et al. Key factors associated with adherence to physical exercise in patients with chronic diseases and older adults: an umbrella review. Int J Environ Res Public Health. 2021. https://doi.org/10.3390/ijerph18042023.
De Smedt D, Clays E, Annemans L, et al. Self-reported health status in coronary heart disease patients: a comparison with the general population. Eur J Cardiovasc Nurs. 2015;14:117–25. https://doi.org/10.1177/1474515113519930.
De Smedt D, Clays E, Annemans L, et al. Health related quality of life in coronary patients and its association with their cardiovascular risk profile: results from the EUROASPIRE III survey. Int J Cardiol. 2013;168:898–903. https://doi.org/10.1016/j.ijcard.2012.10.053.
Huber A, Oldridge N, Höfer S. International SF-36 reference values in patients with ischemic heart disease. Qual Life Res. 2016;25:2787–98. https://doi.org/10.1007/s11136-016-1316-4.
Burström K, Johannesson M, Diderichsen F. Swedish population health-related quality of life results using the EQ-5D. Qual Life Res. 2001;10:621–35. https://doi.org/10.1023/a:1013171831202.
Sullivan M, Karlsson J, Taft C. SF-36 Hälsoenkät: Svensk Manual och Tolkningsguide, 2:a upplagan (Swedish Manual and Interpretation Guide, 2nd edition). Gothenburg: Sahlgrenska University Hospital; 2002.
Hanssen TA, Nordrehaug JE, Eide GE, et al. Anxiety and depression after acute myocardial infarction: an 18-month follow-up study with repeated measures and comparison with a reference population. Eur J Cardiovasc Prev Rehabil. 2009;16:651–9. https://doi.org/10.1097/HJR.0b013e32832e4206.
Abreu A, Frederix I, Dendale P, et al. Standardization and quality improvement of secondary prevention through cardiovascular rehabilitation programmes in Europe: the avenue towards EAPC accreditation programme: A position statement of the Secondary prevention and rehabilitation section of the European association of preventive cardiology (EAPC). Eur J Prev Cardiol. 2020. https://doi.org/10.1177/2047487320924912.
Murphy B, Le Grande M, Alvarenga M, et al. Anxiety and depression after a cardiac event: prevalence and predictors. Front Psychol. 2019;10:3010. https://doi.org/10.3389/fpsyg.2019.03010.
Salazar A, Dueñas M, Fernandez-Palacin F, et al. Factors related to the evolution of Health related quality of life in coronary patients. A longitudinal approach using Weighted generalized estimating equations with missing data. Int J Cardiol. 2016;223:940–6. https://doi.org/10.1016/j.ijcard.2016.08.300.
Jernberg T. SWEDEHEART annual report. Matador Kommunikation AB, Uppsala Sweden 2019.
Howarter AD, Bennett KK, Barber CE, et al. Exercise self-efficacy and symptoms of depression after cardiac rehabilitation: predicting changes over time using a piecewise growth curve analysis. J Cardiovasc Nurs. 2014;29:168–77. https://doi.org/10.1097/JCN.0b013e318282c8d6.
Cederbom S, Rydwik E, Soderlund A, et al. A behavioral medicine intervention for older women living alone with chronic pain - a feasibility study. Clin Interv Aging. 2014;9:1383–97. https://doi.org/10.2147/CIA.S66943.
Howie JG, Heaney DJ and Maxwell M. Measuring quality in general practice. Pilot study of a needs, process and outcome measure. Occas Pap R Coll Gen Pract 1997; i-xii, 1–32
Enthoven P, Peolsson A, Ludvigsson ML, et al. Validity, internal consistency and self-rated change of the patient enablement instrument in patients with chronic musculoskeletal pain. J Rehabil Med. 2019;51:587–97. https://doi.org/10.2340/16501977-2573.
Howie JG, Heaney DJ, Maxwell M. Care of patients with selected health problems in fundholding practices in Scotland in 1990 and 1992: needs, process and outcome. Br J Gen Pract. 1995;45:121–6.
Campkin LM, Boyd JM, Campbell DJT. Coronary artery disease patient perspectives on exercise participation. J Cardiopulm Rehabil Prev. 2017;37:305–14. https://doi.org/10.1097/hcr.0000000000000195.
Heron N, Kee F, Donnelly M, et al. Behaviour change techniques in home-based cardiac rehabilitation: a systematic review. Br J Gen Pract. 2016;66:e747-757. https://doi.org/10.3399/bjgp16X686617.
Back M, Oberg B, Krevers B. Important aspects in relation to patients’ attendance at exercise-based cardiac rehabilitation - facilitators, barriers and physiotherapist’s role: a qualitative study. BMC Cardiovasc Disord. 2017;17:77. https://doi.org/10.1186/s12872-017-0512-7.
Coull A, Pugh G. Maintaining physical activity following myocardial infarction: a qualitative study. BMC Cardiovasc Disord. 2021;21:105. https://doi.org/10.1186/s12872-021-01898-7.
Platz K, Kools S, Howie-Esquivel J. Benefits, facilitators, and barriers of alternative models of cardiac rehabilitation: a qualitative systematic review. J Cardiopulm Rehabil Prev. 2022. https://doi.org/10.1097/hcr.0000000000000738.
Resurreccion DM, Moreno-Peral P, Gomez-Herranz M, et al. Factors associated with non-participation in and dropout from cardiac rehabilitation programmes: a systematic review of prospective cohort studies. Eur J Cardiovasc Nurs. 2019;18:38–47. https://doi.org/10.1177/1474515118783157.
SWEDEHEART. SWEDEHEART annual report 2021, https://www.ucr.uu.se/swedeheart/dokument-sh/arsrapporter-sh/1-swedeheart-annual-report-2021-english/viewdocument/3384. Accessed 27 Jan 2023.
Acknowledgements
The authors thank the physical therapists at the current coronary care unit for their practical support
Funding
Open access funding provided by Linköping University. This work was supported by the Swedish Heart and Lung Association (E 133-15, E 118-16); the Swedish Society of Medical Research (main applicant Maria Bäck); and Region Östergötland (RÖ-827011, RÖ-725541, RÖ-938232). These funding sources had no role in the design of the study, data collection, analysis, and interpretation of data, or in writing the manuscript.
Author information
Authors and Affiliations
Contributions
SB, MB, BÖ, LN and AS were responsible for the conception and design of the study. SB was responsible for the data collection. SB, MB, BÖ, LN, AS and JA were involved in the analysis and/or interpretation of data. SB were responsible for the first drafts of this paper, which was revised critically by MB, BÖ, LN, AS and JA. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval was granted by the Regional Ethical Review Board in Linköping, Sweden (registration number: 2015/209-31) and an amendment (registration number: 2018/383-32). The study was performed in accordance with the Declaration of Helsinki. Informed written consent was obtained from the patients before entering the study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Borg, S., Öberg, B., Nilsson, L. et al. Effectiveness of a behavioral medicine intervention in physical therapy on secondary psychological outcomes and health-related quality of life in exercise-based cardiac rehabilitation: a randomized, controlled trial. BMC Sports Sci Med Rehabil 15, 42 (2023). https://doi.org/10.1186/s13102-023-00647-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13102-023-00647-x