
Abstract
Background
The maximal lactate steady state (MLSS) is defined as the highest workload that can be maintained for a longer period of time without continued blood lactate (LA) accumulation. MLSS is one of the physiological indicators of aerobic performance. However, determination of MLSS requires the performance of a series of constant-intensity tests during multiple laboratory visits. Therefore, attempts are made to determine MLSS indirectly by means of anaerobic threshold (AT) evaluated during a single graded exercise test (GXT) until volitional exhaustion. The aim of our study was to verify whether AT determined by maximal deviation (Dmax), modified maximal deviation (ModDmax), baseline LA concentration + 1 mmol/l (+ 1 mmol/l), individual anaerobic threshold (IAT), onset of blood lactate accumulation (OBLA4mmol/l) and V-slope methods based on GXT with 3-min stages provide valid estimates of MLSS in elite cyclists.
Methods
Twelve elite male cyclists (71.3 ± 3.6 ml/kg/min) completed GXT (the increase by 40 W every 3 min) to establish the AT (by Dmax, ModDmax, + 1 mmol/l, IAT, OBLA4mmol/l and V-slope methods). Next, a series of 30-min constant-load tests to determine MLSS was performed. Agreement between the MLSS and workload (WR) at AT was evaluated using the Bland–Altman method.
Results
The analysis revealed a very high (rs > 0.90, p < 0.001) correlation between WRMLSS and WRDmax and WRIAT. The other AT methods were highly (rs > 0.70) correlated with MLSS except for OBLA4mmol/l (rs = 0.67). The Bland-Altman analysis revealed the highest agreement with MLSS for the Dmax, IAT and + 1 mmol/l methods. Mean difference between WRMLSS and WRDmax, WRIAT and WR+1mmol/l was 1.7 ± 3.9 W, 4.3 ± 7.9 W and 6.7 ± 17.2 W, respectively. Furthermore, the WRDmax and WRIAT had the lowest limits of agreement with the WRMLSS. The ModDmax and OBLA4mmol/l methods overestimated MLSS by 31.7 ± 18.5 W and 43.3 ± 17.8 W, respectively. The V-slope method underestimated MLSS by 36.2 ± 10.9 W.
Conclusions
The AT determined by Dmax and IAT methods based on the cycling GXT with 3-min stages provides a high agreement with the MLSS in elite cyclists. Despite the high correlation with MLSS and low mean difference, the AT determined by + 1 mmol/l method may highly overestimate or underestimate MLSS in individual subjects. The individual MLSS cannot be properly estimated by V-slope, ModDmax and OBLA4mmol/l methods.
Similar content being viewed by others


Background
Anaerobic threshold (AT) is a load above which internal homeostasis is suddenly disturbed and fatigue is intensified, accompanied by changes in gas exchange and blood lactate (LA) concentration during exercise [1, 2]. This point is one of the most significant physiological variables in endurance sports. Anaerobic threshold (AT) has been used to diagnose the sports performance of athletes and to determine exercise zones used during training. The AT shift towards higher loads is considered to be an indicator of improved performance in endurance sports [2, 3]. Anaerobic threshold (AT) is much more reflective of training-induced changes in aerobic performance than changes maximal oxygen uptake (VO2max) [3] and can be improved with appropriately selected training loads and training methods, even in well-trained athletes [4,5,6,7]. It should be noted, however, that AT can change depending on diets [8,9,10,11] and supplementation [12,13,14], and may be modified by environmental conditions, such as altitude or temperature [15, 16], and psychological factors [17, 18]. Paradoxically, higher AT can be observed in overtraining due to changes in LA blood levels as a response to exercise [19]. Therefore, test results should be interpreted with caution, taking into account the presence of numerous factors that may affect AT.
Over several decades, many concepts of AT determination have been developed, which are based on the observation of the increase in blood LA levels and/or changes in respiratory indices recorded during graded exercise tests (GXTs) [2]. Another approach to evaluate aerobic performance is to determine maximal lactate steady state (MLSS). MLSS is defined as the highest workload that can be maintained for a longer period of time without continued blood LA accumulation. During the exercise at and below the MLSS workload, a balance occurs between LA production and its rate of clearance. When the effort is above the MLSS workload, the rate of LA production exceeds its removal [20]. By definition, MLSS is attained when blood LA levels increases by less than 1 mmol/l between 10 and 30 min of the constant-intensity exercise test [21].
Determination of MLSS requires the performance of a series of constant-intensity tests during multiple laboratory visits, which in practice is burdensome and may disrupt the athletes’ training program. Therefore, attempts are made to determine MLSS indirectly based on AT evaluated during a single GXT until volitional exhaustion [22,23,24,25,26,27,28]. However, the results comparing various concepts of AT with MLSS are conflicting [22,23,24,25,26,27,28].
It seems that some of the discrepancies in the literature concerning the application of individual methods of evaluation of AT to determine MLSS result from differences in GXT protocol design (step duration and load) and different types of test exercise (cycling, running, rowing). The choice of the appropriate load and time between increments during GXT is critical for the evaluation of AT based on LA levels [22, 27, 29, 30]. It is suggested that in order to achieve lactate steady state during GXT and valid determinations of the lactate threshold (LT), step duration should be longer than 6 min [22, 30,31,32]. This is related to the time needed to transport LA from the intramuscular compartment to plasma, which depends on the capacity of the monocarboxylic transporters (MCT) [33]. With too short a step duration, a blood LA level can result from lower load compared to the one at which it was recorded, which can lead to AT overestimation.
In training practice, not only LT, but also VO2max and maximal heart rate (HRmax) are usually determined during GXT. The extension of the time of stages results in a significant increase in the time of the entire test, which may result in VO2max and HRmax not being achieved due to premature local muscle fatigue [30, 34, 35]. Therefore, a 3 to 4-min stages are very often used during GXT [36,37,38,39]. For this reason, it is important to determine which AT method yields the most favorable estimation of the MLSS with such a step duration.
In addition to GXT study design and exercise mode, the sports performance level of the athlete can play an important role in determining AT and its agreement with MLSS. Training adaptations lead to changes in the metabolic response to exercise loads and increased exercise tolerance [40]. The method that reflects MLSS well in people with lower levels of sports performance will not necessarily provide a favorable MLSS estimation in elite athletes.
Therefore, the aim of our study was to verify whether AT determined by Dmax, ModDmax, + 1 mmol/l, IAT, OBLA4mmol/l and V-slope methods based on GXT with 3-min stages provide valid estimates of the MLSS in elite cyclists. We hypothesize that using the GXT with AT determination allows for the indirect determination of MLSS in elite cyclists.
Methods
Participants
Fourteen male elite cyclists were recruited for this study. Two participants withdrew from participation because of infections. Twelve athletes completed all the testing and were included for analysis (aged 25.9 ± 3.2 years; body height 181.7 ± 4.4 cm; body mass 72.3 ± 5.3 kg; fat content (%) 8.6 ± 2.1%; VO2max 71.3 ± 3.5 ml/kg/min). All cyclists had at least 6 years of national and international competition experience and were familiar with our laboratory testing procedures. All athletes had current medical examinations, without any contraindications to performing exhaustive exercise in a hypoxic environment. The participants provided their written voluntary informed consent before the participation. The research project was conducted according to the Helsinki Declaration and was approved by the Ethics Committee for Scientific Research at the Jerzy Kukuczka Academy of Physical Education in Katowice, Poland.
Experimental design
The research was conducted at the end of the preparatory period. Testing procedures were identical for each athlete. The experiment was divided into two series of tests performed in a laboratory environment. All participants were familiarized with the test protocols before the first evaluations. The athletes were instructed to avoid strenuous exercise and caffeine intake for 24 h prior to each test. Throughout the experiment (from the 2 days prior to the experiment to the last MLSS test), participants consumed meals that contained the same amount of kcal, protein, fats, and carbohydrates each day (40 kcal/kg of body weight, 50% carbohydrates, 20% proteins, 30% fats). Participants stayed at the camp and consumed meals served only on the spot which were prepared according to the dietitian’s recommendations.
Experimental testing
In the first series of testing, before breakfast, body mass and body composition were evaluated using the electrical impedance technique (Inbody 220, Biospace Co., Japan). Next, 2 h after a light breakfast (5 kcal/1 kg of body weight, 50% carbohydrates, 20% proteins, 30% fats), the GXT was performed to determine metabolic thresholds and aerobic capacity with an Excalibur Sport ergometer (Lode BV, Netherlands). The GXT started at a workload of 40 W, which was increased by 40 W every 3 min until volitional exhaustion. During the test, all cyclists were instructed to remain in a sitting position and maintain a cadence of 80 rpm (±5 rpm). Each cyclist’s bike setup (saddle height, reach, handle bar height) was recorded and reproduced for all tests.
During the GXT, heart rate (HR), oxygen uptake (VO2), expired carbon dioxide (CO2) and minute ventilation (VE) were measured continuously with a gas analyzer MetaLyzer 3B-R2 (Cortex, Germany) using the breath-by-breath method. The criterion of reaching VO2max was respiratory exchange ratio (RER) above 1.1. The maximal workload (WRmax) was indicated as the last completed stage of the progressive test. If a participant terminated the test before completing a given workload, the WRmax was calculated from the formula WRmax = WRk + (t/T x WRp), where WRk is the previous workload, t is exercise duration with the workload until premature failure, T is the duration of each workload, and WRp is the amount of workload by which exercise intensity increased during the test [41]. Fingertip capillary blood samples for the assessment of LA levels (Biosen C line Clinic, EKF-diagnostic GmbH, Germany) were drawn at rest and at the end of each step of the test, as well as during the 3rd, 6th, 9th, and 12th minute of recovery.
The anaerobic threshold (AT) was determined using the Dmax method [42], modified Dmax method – ModDmax [36], the IAT method [43], + 1 mmol/l method [44], OBLA4mmol/l method [45], and the non-invasive V-slope method [46]. V-slope workload was identified in the exercise intensity which, in a plot of the minute production of CO2 over the minute utilization of oxygen (VO2), shows an increase in the slope of above 1.0 [46]. Two independent investigators detected ventilator thresholds following the criteria previously described. If they did not agree, the opinion of a third investigator was sought.
In the second series of the tests, which started after a day of active recovery, all participants started to perform a series of efforts at a constant load to determine the MLSS. Each test was preceded by a 10-min warm-up with an individually set load of 65–70% HRmax and a fixed cadence of 80 rpm. The warm-up was followed by an increase in the load to the target value at which the athlete performed exercise for 30 min. The participants started a series of tests with an individual load equal to the lowest value of the threshold load determined by selected methods during the GXT performed in the first series of tests. Capillary blood samples were obtained from the fingertip at rest, at the end of the warm-up and after every 5 min of the test (5, 10, 15, 20, 25 and 30 min) to determine the LA concentration in the blood. When the LA concentration during the last 20 min of the test was stable and did not increase by more than 1 mmol/l, the test was repeated after a day of active rest with a load increased by 20 W. Tests with constant intensity were performed until a load was reached, during which the LA gain in blood exceeded 1 mmol/l in the last 20 min, and the previous load was considered as MLSS. Furthermore, if during the first test at a threshold load the LA increase exceeded the target value, the test was analogically repeated at a load lower by 20 W until the MLSS was reached. The use of our previous experience in indirect evaluation of MLSS [23] resulted in the determination of MLSS for the 2nd or 3rd time.
Statistical analysis
The normality of the distribution of variables was checked using the Shapiro-Wilk test. A Wilcoxon test was used to assess significant differences between the MLSS and the AT determined by various methods. Agreement between the MLSS and workload at AT was evaluated using the Bland–Altman method [47]. The correlations were calculated using Spearman’s rank correlation coefficient. The statistical significance was set at p < 0.05. Statistical analyses were conducted using StatSoft Statistica 13.0 software.
Results
Maximal lactate steady state
The mean value of workload in MLSS (WRMLSS) was 298 ± 21 W. The mean values of VO2, HR and LA at the 10th and 30th min of the MLSS test are reported in Table 1.
Graded exercise test
The mean values of WRmax and VO2max were 409 ± 34 W and 71.3 ± 3.6 ml/kg/min, respectively. The HRmax and VEmax were 196 ± 5 bpm and 188.4 ± 18.4 l/min, respectively. The blood LA level increased by 7.42 ± 1.23 mmol/l during the GXT and it decreased by 2.46 ± 0.75 mmol/l during 12 min of the recovery period after the exercise.
The MLSS and the various AT concepts
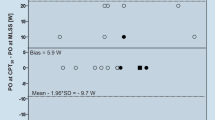
Comparisons of the WRMLSS and the workload at AT determined by the six methods were presented in Table 2. The Wilcoxon test revealed significant differences (p < 0.01) between WRMLSS and WRVAT, WRModDmax and WROBLA4mmol/l. There were no significant differences between WRMLSS and WRDmax, WR+1mmol/l and WRIAT. The analysis revealed a very high (rs > 0.90, p < 0.001) correlation between WRMLSS and WRDmax and WRIAT. Other AT methods were highly (rs > 0.70) correlated with MLSS except for OBLA4mmol/l (rs = 0.67). The Bland-Altman analysis revealed the highest agreement with MLSS (i.e., low mean difference) for the Dmax, IAT and + 1 mmol/l methods. The mean difference between WRMLSS and WRDmax, WRIAT and WR+ 1mmol/l was 1.7 ± 3.9 W, 4.3 ± 7.9 W and 6.7 ± 17.2 W, respectively. Furthermore, the WRDmax and WRIAT had the lowest limits of agreement with the WRMLSS (Table 2). The limits of agreement for + 1 mmol/l method were large (upper LOA of 40.4 W and lower LOA of 27.1 W). The WRV-slope, WRModDmax, WROBLA4mmol/l showed low agreement with MLSS (high mean difference and high limits of agreement). The ModDmax and OBLA4mmol/l methods overestimated MLSS by 31.7 ± 18.5 W and 43.3 ± 17.8 W, respectively. The V-slope method underestimated MLSS by 36.2 ± 10.9 W. The relation between the workload at AT determined by various methods and MLSS was presented in the Bland-Altman plots (Fig. 1).

Bland-Altman plots comparing MLSS and workload at AT determined by Dmax (a), ModDmax (b), IAT (c), + 1 mmol/l (d), OBLA4mmol/l, (e), V-slope (f) methods. The horizontal solid line represents the mean difference between the two measures (bias). The horizontal dashed lines represent the limits of agreement (LOA). n = 7 for IAT method and n = 12 for Dmax, ModDmax, + 1 mmol/l, OBLA4mmol/l and V-slope
Discussion
The results of our study indicate that of the six methods included in our analysis, Dmax and IAT methods yielded the most favorable estimations of the MLSS. The WRDmax and WRIAT had the highest correlation (rs > 0.90) and the lowest mean difference with the WRMLSS. The Dmax method only slightly underestimates MLSS (by 1.7 ± 3.9 W) and 95% of differences between measurements by the MLSS and Dmax method range from − 5.9 to 9.3 W. Likewise, the IAT slightly underestimates MLSS (by 4.3 ± 7.9 W), with limits of agreement between − 11.1 and 19.7 W. It should be noted that in our study, IAT was only evaluated for seven cyclists because of the rapid decline of the post-exercise LA value. This is a commonly reported issue with this method [24, 48]. For this reason, despite the favorable MLSS estimation, the IAT method may not be useful in practice for some athletes, especially those highly-trained.
Despite the lack of significant differences (p > 0.05) and low bias (MD = 6.7 ± 17.2 W) between WRMLSS and WR+ 1mmol/l, the limits of agreement for comparison between these variables suggest that the extent of disagreements is too high to allow MLSS to be accurately estimated using + 1 mmol/l method in individual participants. The V-slope, ModDmax and OBLA4mmol/l methods failed to provide valid estimates of the MLSS. We observed large mean differences (− 43 to 36 W) between AT determined by these methods and MLSS.
In our study, AT determined by the Dmax method based on the cycling GXT test with 3-min stages (GXT3) showed a high agreement with the MLSS. The results of previous research in this area are divergent. Arratibel-Imaz et al. [49] demonstrated a high agreement of Dmax with MLSS (MD = -2.1 W, r = 0.93) using cycling GXT3 in cyclists and triathletes. Similarly, Czuba et al. [23] showed a high correlation (r = 0.97) between WRDmax (GXT3) and WRMLSS in well-trained female and male cyclists. Results obtained by Pallarés et al. [25] revealed less bias (− 1.8 W) but with lower correlation (r = 0.56) between Dmax (GXT1) and MLSS in well-trained cyclists. On the contrary, Van Schuylenbergh et al. [22] showed that despite a correlation between Dmax (GXT6) and MLSS (r = 0.85), WRDmax was lower by 22 W compared to WRMLSS in elite cyclists. Similar findings were reported by Jamnick et al. [27] for four GXTs with different stage durations (3, 4, 7, and 10 min). The authors observed a high correlation between Dmax and the MLSS (r = 0.94 to 0.97) but mean differences were too large (19 to 49 W) for Dmax to provide a valid estimate of the MLSS. However, it is worth noting that in the research carried out by Jamnick et al. [27], WRDmax determined during GXT3 showed the smallest mean difference compared to MLSS. As the duration of the stage increased (from 3 to 10 min), the difference between WRMLSS and WRDmax increased. The discrepancy of the above results may result from different test protocols and different sports performance of the study participants. However, with the Dmax method used in highly-trained cyclists, GXT with 3-min stages seems to be best suited for the indirect MLSS determination by the Dmax method. Extending the stage to 6–10 min increases the MLSS underestimation by Dmax [22, 27].
Our results indicate that IAT methods (GXT3), similarly to Dmax, yielded high agreement with MLSS. To the best of our knowledge, this is the first study to analyze whether the IAT method provides valid estimates of the MLSS in elite cyclists. Previous research carried out using the cycling exercise test, De Barros et al. [48] revealed good agreement between IAT (GXT3) and MLSS (r = 0.85, MD = -0.7) in active males. The difference between MLSS and IAT was lower than 25 W for all subjects. Furthermore, Hauser et al. [24] indicated that IAT (GXT4) was highly correlated with MLSS (r = 0.83) and overestimated it by 12 W. However, the large individual differences were reported in this study, which was likely to result from heterogenous endurance level of study participants.
It should be noted that a major practical limitation of the IAT method is that the determination of AT depends on post-exercise changes in blood LA level. For this reason, the determination of AT is infeasible in athletes with a fast rate of LA utilization during restitution. Such a problem may occur more often in highly-trained endurance athletes. This is due to the increased efficiency of MCT, increased capillarity and a more efficient use of LA in metabolic processes by tissues with high oxidative potential [50,51,52]. For this reason, although MLSS can be properly estimated by IAT, the use of this method in the sports practice may be difficult.
The third method which in our study showed small mean differences with MLSS is the + 1 mmol/l method (MD = 6.7). However, focusing on the individual determination of MLSS, it should be concluded that + 1 mmol/l (GXT3) is not a valid method for MLSS estimation in elite cyclists. The lack of agreement of + 1 mmol/l with MLSS in cyclists was also previously reported by Pallarés et al. [25] but they used a different exercise protocol (ramp test; GXT1, with capillary blood sampling obtained every 2 min).
The large individual variation in the agreement of WR+ 1mmol/l and WRMLSS can be attributed to an arbitrarily imposed LA increase by 1 mmol/l above baseline [44]. The resting LA level and the rate of increase of LA level in the blood during exercise show great interindividual variation and depend on the sports performance [53, 54], diet, and supplementation [13, 55, 56], and may be modified by environmental conditions [15, 16] and psychological factors [17, 18]. Therefore, the determination of a specific absolute value of the LA level or its increment (as in the + 1 mmol/l, ModDmax, and OBLA methods) may result in the erroneous determination of method-specific points and the consequent overestimation or underestimation of AT and also MLSS. Furthermore, it should be noted that accurate determination of baseline LA concentration is needed for the + 1 mmol/l method to be reliable. This may prove problematic due to the fluctuations associated with analyzer error [57], which later affects the determination of AT. For the above reasons, attempts to use the + 1 mmol/l method for the determination of MLSS in individual athletes should be made with care, taking into account factors that may interfere with its repeatability and reliability.
The results of our study indicate that ModDmax, OBLA4mmol/l, and V-slope are not valid methods for estimation of MLSS in cyclists when GXT with 3 min stage duration is used. We showed that ModDmax and OBLA4mmol/l overestimate, and the V-slope method underestimates MLSS exercise intensity by more than 30 W, with large individual deviations. Such a large discrepancy is unacceptable in elite cyclists, who need a high degree of precision in controlling and monitoring the training process. This is especially true when this process is regulated by recording the power generated by the cyclist during the exercise.
In contrast to the presented findings, a recent study carried out by Jamnick et al. [27] and Zwingmann et al. [28] showed that the ModDmax method is a good MLSS determinant for cyclists and triathletes. However, their studies involved athletes with a lower sports performance than those examined in our study (MLSS: 264 W and 229 W vs. 298 W), which may have led to the discrepancies in the obtained results.
In the ModDmax method, an important role in determining AT is played by the first rise in blood lactate concentration of > 0.4 mmol/l. It should be taken into account that the fixed value of 0.4 mmol/l does not take into account the individual level and kinetics of LA. It can be presumed that the moment of this increase depends on stage duration, load, and sports performance of the athlete. A longer stage and a higher increase in the load result in an increase in LA at earlier stages. Furthermore, our many years of unpublished observations show that the increase in sports performance is associated with a clear flattening of the lactate curve at sub-threshold loads. This is mainly due to an increase in the consumption of fatty acids by muscles (shifting the point of intersection of carbohydrate and fat utilization towards higher loads), and an improvement in the utilization of LA [51, 58]. This phenomenon causes that a line formed by the point preceding the first rise in blood LA concentration of > 0.4 mmol/l and the final LA point has a steep profile in highly-trained athletes. Consequently, LT determined by the ModDmax method in highly trained athletes occurs at higher loads than LT determined by Dmax and IAT methods. For this reason, MLSS can also be greatly overestimated by ModDmax, as we observed in our study. Given the above, we suggest that the ModDmax method cannot be used to indirectly determine MLSS in elite cyclists. ModDmax is likely to be useful in people with lower levels of sports performance [26, 28], but this aspect requires further research.
The results obtained in this study indicate that OBLA4mmol/l (GXT3) does not provide a correct estimation of MLSS. This result is in line with several previous studies using GXT cycling with a stage length of 1–10 min. It was observed that OBLA4mmol/l significantly overestimates [25, 27] or underestimates MLSS [48] and shows a great individual variation [24]. The main reason for these discrepancies is that the OBLA4mmol/l method is based on the association of threshold load values with a specific constant blood LA level, without taking into account individual variability and dynamics of changes in circulating LA concentration (LA curve) during exercise [2]. The assumption of the OBLA4mmol/l method was to select blood LA concentration which is similar to MLSS. The vast majority of subjects achieve MLSS for LA of ca. Four millimoles per Liter, but this concentration occurs after a much longer time than the 3 min adopted in GXT3, which is related to the previously described LA outflow into the blood. Furthermore, individual variability in blood LA levels at MLSS has also been demonstrated [24, 59], as observed in our study, despite the homogeneous sports performance level of the cyclists studied. The final blood LA concentration during MLSS test ranged from 3.6 to 5.6 mmol/l. Therefore, arbitrary setting the LA level at 4 mmol/l especially during GXT3 will result in the low agreement of WROBLA4mmol/l with WRMLSS. It is suggested that extending the stage duration to 7–10 min while decreasing the set LA level to 3–3.5 mmol/l will increase OBLA agreement with MLSS [27]. However, this does not eliminate the interindividual variability in blood LA level, which in our opinion excludes the use of the OBLA method in indirect determination of MLSS in elite cyclists.
The V-slope method is based on a visual evaluation of the curve of the relationship between VO2 and VCO2. V-slope analysis detects the onset of excess CO2 production occurring in response to an increase in hydrogen ion (H+) concentration during exercise [46]. To minimize changes in blood pH, H+ ions are buffered by the bicarbonate buffer (HCO3−), which leads to the formation of carbonic acid that dissociates to H2O and CO2. Excess CO2 stimulates ventilation, whereas higher ventilation results in increased CO2 release [60].
The V-slope method is used in practice as a non-invasive method of AT determination. However, VAT and LT do not always occur at the same workload [60]. Some studies indicate the unreliability of the V-slope method both as an alternative to LT [42, 61, 62] and the MLSS in cyclists [25]. In our study, we demonstrated that AT determined using the V-slope method is achieved at lower loads than MLSS (MD = 36 W), which is consistent with the results obtained by Pallarés et al. [25]. The discrepancies between WRV-slope and WRMLSS are due to the fact that athletes improve their MCT system as a result of endurance training and increasing the intramuscular LA utilization. This adaptive mechanism does not directly affect the H+ ion concentration and thus the CO2 production [63]. The above mechanism explains the shift (towards lower loads) of the V-slope threshold (based on the increase in CO2) in relation to LT and MLSS (based on LA changes in blood).
Conclusion
The AT determined by Dmax method based on cycling GXT with 3-min stages provides high agreement with the MLSS in elite cyclists. A similar agreement with MLSS is ensured by IAT, however, in some individuals, the determination of AT using this method is unworkable due to the rapid decline of LA after exercise. Therefore, the use of the IAT method to estimate MLSS in the sports practice may be difficult. Despite the high correlation with MLSS and low mean difference, the AT determined by + 1 mmol/l method may highly overestimate or underestimate MLSS in individual subjects. The individual MLSS cannot be properly estimated by V-slope, ModDmax, and OBLA4mmo/l methods.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- MLSS:
-
Maximal lactate steady state
- AT:
-
Anaerobic threshold
- GXT:
-
Graded exercise test
- WR:
-
Workload
- Dmax :
-
Lactate threshold determined by Dmax method
- ModDmax :
-
Lactate threshold determined by modified Dmax method
- IAT:
-
Individual anaerobic threshold
- + 1 mmol/l:
-
Lactate threshold determined by + 1 mmol/l method
- OBLA4mmo/l :
-
4 mmol/l lactate threshold
- V-slope:
-
Ventilatory threshold determined by V-slope method
References
Wasserman K, Whipp BJ, Koyl SN, Beaver WL. Anaerobic threshold and respiratory gas exchange during exercise. J Appl Physiol. 1973;35:236–43.
Faude O, Kindermann W, Meyer T. Lactate threshold concepts. How valid are they? Sports Med. 2009;39(6):469–90.
Foster C, Cotter HM. Blood lactate, respiratory, heart rate markers on the capacity for sustained exercise. In: Maud PJ, Foster C, editors. Physiological assessment of human fitness. 2nd ed. Champaign: Human Kinetics; 2006. p. 63–76.
Laursen PB, Shing CM, Peake JM, Coombes JS, Jenkins DG. Influence of high-intensity interval training on adaptations in well-trained cyclists. J Strength Cond Res. 2005;19(3):527–33.
Czuba M, Waśkiewicz Z, Zając A, Poprzęcki S, Cholewa J, Roczniok R. The effects of intermittent hypoxic training on aerobic capacity and endurance performance in cyclists. J Sports Sci Med. 2011;10:175–83.
Czuba M, Fidos-Czuba O, Płoszczyca K, Zając A, Langfort J. Comparison of the effect of intermittent hypoxic training vs. the live high, train low strategy on aerobic capacity and sports performance in cyclists in normoxia. Biol Sport. 2018;35:39–48.
Płoszczyca K, Foltyn J, Goliniewski J, Krężelok J, Poprzęcki S, Ozimek M, et al. Seasonal changes in gross efficiency and aerobic capacity in well-trained road cyclists. Isokinet Exerc Sci. 2019;27(3):193–202.
Yoshida T. Effect of dietary modifications on lactate threshold and onset of blood lactate accumulation during incremental exercise. Eur J Appl Physiol. 1984;53(3):200–5.
Maassen N, Busse MW. The relationship between lactic acid and work load: a measure for endurance capacity or an indicator of carbohydrate deficiency? Eur J Appl Physiol Occup Physiol. 1989;58(7):728–37.
Langfort J, Pilis W, Zarzeczny R, Nazar K, Kaciuba-Uscilko H. Effect of low-carbohydrate-ketogenic diet on metabolic and hormonal responses to graded exercise in men. J Physiol Pharmacol. 1996;47(2):361–71.
Langfort J, Czarnowski D, Zendzian-Piotrowska M, Zarzeczny R, Gorski J. Short-term low-carbohydrate diet dissociates lactate and ammonia thresholds in men. J Strength Cond Res. 2004;18(2):260–5.
Berry MJ, Stoneman JV, Weyrich AS, Burney B. Dissociation of the ventilatory and lactate thresholds following caffeine ingestion. Med Sci Sports Exerc. 1991;23(4):463–9.
Edge J, Bishop D, Goodman C. Effects of chronic NaHCO3 ingestion during interval training on changes to muscle buffer capacity, metabolism, and short-term endurance performance. J Appl Physiol (1985). 2006;101(3):918–25.
Czuba M, Zajac A, Poprzecki S, Cholewa J, Woska S. Effects of sodium phosphate loading on aerobic power and capacity in off road cyclists. J Sports Sci Med. 2009;8(4):591–9.
Renberg J, Sandsund M, Wiggen ON, Reinertsen RE. Effect of ambient temperature on female endurance performance. J Therm Biol. 2014;45:9–14.
Drzazga Z, Schisler I, Poprzȩcki S, Michnik A, Czuba M. Serum autofluorescence and biochemical markers in athlete's response to strength effort in normobaric hypoxia: a preliminary study. Biomed Res Int. 2019;2019:5201351.
Gerra G, Zaimovic A, Mascetti GG, Gardini S, Zambelli U, Timpano M, et al. Neuroendocrine responses to experimentally-induced psychological stress in healthy humans. Psychoneuroendocrinology. 2001;26(1):91–107.
Hermann R, Lay D, Wahl P, Roth WT, Petrowski K. Effects of psychosocial and physical stress on lactate and anxiety levels. Stress. 2019;22(6):664–9.
Urhausen A, Kindermann W. Diagnosis of overtraining: what tools do we have? Sports Med. 2002;32(2):95–102.
Billat VL, Sirvent P, Py G, Koralsztein J-P, Mercier J. The concept of maximal lactate steady state: a bridge between biochemistry, physiology and sport science. Sports Med. 2003;33(6):407–26.
Snyder AC, Wolfe T, Welsh R, Foster CA. Simplified approach to estimating maximal lactate steady state. Int J Sports Med. 1994;15:27–31.
Van Schuylenbergh R, Vanden EB, Hespel P. Correlations between lactate and ventilatory thresholds and the maximal lactate steady state in elite cyclists. Int J Sports Med. 2004;25(6):403–8.
Czuba M, Zając A, Cholewa J, Poprzęcki S, Waśkiewicz Z, Mikołajec K. Lactate threshold (D-max method) and maximal lactate steady state in cyclists. J Hum Kinet. 2009;21:49–56.
Hauser T, Adam J, Schulz H. Comparison of selected lactate threshold parameters with maximal lactate steady state in cycling. Int J Sports Med. 2014;35(6):517–21.
Pallarés JG, Morán-Navarro R, Ortega JF, Fernández-Elías VE, Mora-Rodriguez R. Validity and reliability of ventilatory and blood lactate thresholds in well-trained cyclists. PLoS One. 2016;11(9):e0163389.
Wahl P, Manunzio C, Vogt F, Strutt S, Volmary P, Bloch W, et al. Accuracy of a modified lactate minimum test and reverse lactate threshold test to determine maximal lactate steady state. J Strength Cond Res. 2017;31(12):3489–96.
Jamnick NA, Botella J, Pyne DB, Bishop DJ. Manipulating graded exercise test variables affects the validity of the lactate threshold and VO2peak. PLoS One. 2018;13(7):e0199794.
Zwingmann L, Strutt S, Martin A, Volmary P, Bloch W, Wahl P. Modifications of the Dmax method in comparison to the maximal lactate steady state in young male athletes. Phys Sportsmed. 2019;47(2):174–81.
Stockhausen W, Grathwohl D, Burklin C, Spranz P, Kuel J. Stage duration and increase of workload in incremental testing on a cycle ergometer. Eur J Appl Physiol. 1997;76:295–301.
Bourdon PC, Woolford SM, Buckley JD. Effects of varying the step duration on the determination of lactate thresholds in elite rowers. Int J Sports Physiol Perform. 2018;13(6):687–93.
Foxdal P, Sjodin A, Sjodin B. Comparison of blood lactate concentrations obtained during incremental and constant intensity exercise. Int J Sports Med. 1996;17:360–5.
Kuipers H, Rietjans G, Verstappen F, Schoenmakers H, Hofman G. Effects of stage duration in incremental running tests on physiological variables. Int J Sports Med. 2003;24:486–91.
Juel C, Kristiansen S, Pilgaard H, Wojtaszewski J, Rchter EA. Kinetics of lactate transports in sarcolemmal giant vesicles from human skeletal muscle. J Appl Physiol. 1994;76:1031–6.
Pierce SJ, Hahn AG, Davie A, Lawton EW. Prolonged incremental tests do not necessarily compromise VO2max in well-trained athletes. J Sci Med Sport. 1999;2(4):356–63.
Gavin JP, Willems MET, Myers SD. Repoducibilty of lactate markers during 4 and 8 min stage incremental running: a pilot study. J Sci Med Sport. 2014;17:635–9.
Bishop D, Jenkins DG, Mackinnon LT. The relationship between plasma lactate parameters, Wpeak and 1-h cycling performance in women. Med Sci Sports Exerc. 1998;30(8):1270–5.
Baron R. Aerobic and anaerobic power characteristics of off-road cyclists. Med Sci Sports Exerc. 2001;33(8):1387–93.
Impellizzeri F, Sassi A, Rodriguez-Alonso M, Mognoni P, Marcora S. Exercise intensity during off-road cycling competitions. Med Sci Sports Exerc. 2002;34(11):1808–13.
Moseley L, Achten J, Martin JC, Jeukendrup AE. No differences in cycling efficiency between world-class and recreational cyclists. Int J Sports Med. 2004;25(5):374–9.
Jones AM, Carter H. The effect of endurance training on parameters of aerobic fitness. Sports Med. 2000;29:373–86.
Kuipers H, Verstappen FT, Keizer HA, Guerten P, van Kranenburg G. Variability of aerobic performance in the laboratory and its physiological correlates. Int J Sports Med. 1985;6:197–201.
Cheng B, Kuipers H, Snyder AC, Keizer HA, Jeukendrup A, Hesselink M. A new approach for the determination of ventilator and lactate thresholds. Int J Sports Med. 1992;13:518–22.
Stegmann H, Kindermann W, Schnabel A. Lactate kinetics and individual anaerobic threshold. Int J Sports Med. 1981;2:160–5.
Coyle EF, Martin WH, Ehsani AA, Jhagberg JM, Bloomfield SA, Sinacore DR, et al. Blood lactate threshold in some well-trained ischemic heart disease patients. J Appl Physiol Respir Environ Exerc Physiol. 1983;54(1):18–23.
Heck H, Mader A, Hess G, Mucke S, Muller R, Hollmann W. Justification of the 4 mmol/l lactate threshold. Int J Sports Med. 1985;6(3):117–30.
Beaver WL, Wasserman K, Whipp BJ. A new method for detecting anaerobic threshold by gas exchange. J Appl Physiol. 1986;60:2020–7.
Bland JM, Altman D. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet. 1986;327(8476):307–10.
De Barros CL, Mendes TT, Mortimer Lde Á, Ramos GP, Garcia ES. Individual anaerobic threshold estimates maximal lactate steady state in temperate and hot climate. J Sports Med Phys Fitness. 2016;56(1–2):27–33.
Arratibel-Imaz I, Calleja-Gonzalez JR, Emparanza JI, Terrados N, Mjaanes JM, Ostojic SM. Lack of concordance amongst measurements of individual anaerobic threshold and maximal lactate steady state on a cycle ergometer. Phys Sportsmed. 2016;44(1):34–45.
Henriksson J. Effects of physical training on the metabolism of skeletal muscle. Diabetes Care. 1992;15(11):1701–11.
Juel C, Halestrap AP. Lactate transport in skeletal muscle - role and regulation of the monocarboxylate transporter. J Physiol. 1999;517(Pt 3):633–42.
Brooks GA. Cell–cell and intracellular lactate shuttles. J Physiol. 2009;587(Pt23):5591–600.
Lucia AJ, Pardo A, Durantez J, Hoyos J, Chicharro L. Physiological differences between professional and elite road cyclists. Int J Sports Med. 1998;19:342–8.
Messonnier LA, Emhoff CW, Fattor JA, Horning MA, Carlson TJ, Brooks GA. Lactate kinetics at the lactate threshold in trained and untrained men. J Appl Physiol. 2013;114:1593–602.
Zajac A, Poprzecki S, Maszczyk A, Czuba M, Michalczyk M, Zydek G. The effects of a ketogenic diet on exercise metabolism and physical performance in off-road cyclists. Nutrients. 2014;6:2493–508.
Pilis K, Pilis A, Stec K, Pilis W, Langfort J, Letkiewicz S, et al. Three-year chronic consumption of low-carbohydrate diet impairs exercise performance and has a small unfavorable effect on lipid profile in middle-aged men. Nutrients. 2018;10:914.
Weltman A, Snead D, Seip R, Schurrer R, Levine S, Rutt R, et al. Prediction of lactate threshold and fixed blood lactate concentrations from 3200-m running performance in male runners. Int J Sports Med. 1987;8(6):401–6.
Hoppeler H. Skeletal muscle substrate metabolism. Int J Obes Relat Metab Disord. 1999;23(Suppl 3):S7–S10.
MacIntosh BR, Esau S, Svedahl K. The lactate minimum test for cycling: estimation of the maximal lactate steady state. Can J Appl Physiol. 2002;27:232–49.
Svedahl K, MacIntosh BR. Anaerobic threshold: the concept and methods of measurement. Can J Appl Physiol. 2003;28(2):299–323.
Amann M, Subudhi AW, Foster C. Predictive validity of ventilator and lactate thresholds for cycling time trial performance. Scand J Med Sci Sports. 2006;16(1):27–34.
Francis JT Jr, Quinn TJ, Amann M, LaRoche DP. Defining intensity domains from the end power of a 3-min all-out cycling test. Med Sci Sports Exerc. 2010;42(9):1769–75.
Loat CER, Rhodes EC. Relationship between the lactate and ventilatory thresholds during prolonged exercise. Sports Med. 1993;15:104–15.
Acknowledgements
Not applicable.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
Conceptualization: KP, DJ, MC; Investigation: DJ, MC; Data collection: KP, DJ, ZP, MCh; Data analysis: KP; Writing – original draft: KP. DJ, ZP, MCh; Writing – review and editing: KP, JL, MC; Supervision: JL, MC. All authors approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The research project was conducted according to the Helsinki Declaration and was approved by the Ethics Committee for Scientific Research at the Jerzy Kukuczka Academy of Physical Education in Katowice, Poland. The participants provided their written voluntary informed consent before the participation.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Płoszczyca, K., Jazic, D., Piotrowicz, Z. et al. Comparison of maximal lactate steady state with anaerobic threshold determined by various methods based on graded exercise test with 3-minute stages in elite cyclists. BMC Sports Sci Med Rehabil 12, 70 (2020). https://doi.org/10.1186/s13102-020-00219-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13102-020-00219-3