
Abstract
Background
In the present systematic review and meta-analysis, the association of maternal exposure to the endocrine disrupting chemicals (EDCs) with cardio-metabolic risk factors in children during childhood for the first time.
Method
The PubMed, Scopus, EMBASE, and Web of Science databases were systematically searched, up to Feb 2023. In total 30 cohort studies had our inclusion criteria. A random-effects model was used for the variables that had considerable heterogeneity between studies. The Newcastle–Ottawa Scale (NOS) tool was used to classify the quality score of studies. All statistical analyses were conducted using Stata 14 and P-value < 0.05 considered as a significant level.
Results
In the meta-analysis, maternal exposure to the EDCs was weakly associated with higher SBP (Fisher_Z: 0.06, CI: 0.04, 0.08), BMI (Fisher_Z: 0.07, CI: 0.06, 0.08), and WC (Fisher_Z: 0.06, CI: 0.03, 0.08) z-scores in children. A significant linear association was found between maternal exposure to the bisphenol-A and pesticides with BMI and WC z-score in children (p < 0.001). Subgroup analysis showed significant linear association of BPA and pesticides, in the urine samples of mothers at the first trimester of pregnancy, with BMI and WC z-score in children from 2–8 years (p < 0.05).
Conclusion
Prenatal exposure to the EDCs in the uterine period could increase the risk of obesity in children. Maternal exposure to bisphenol-A and pesticides showed the strongest association with the obesity, especially visceral form, in the next generation.
Similar content being viewed by others

Introduction
Endocrine disruptors are defined as the exogenous chemicals that interfere with any aspect of hormone action [1]. Endocrine disruptor chemicals (EDCs) are natural and manufactured compounds that are found in pesticides, metals, plastic bottles, food containers, detergents, flame-retardants, toys, and cosmetics [1, 2]. Daily exposure to these materials is an inseparable part of contemporary life. Human are constantly exposed to these chemicals in food, air, and water. Industrial and agricultural toxins, including dioxins, perchlorates, organochlorines, organophosphates, and carbamates, are some the natural examples of EDCs. Bisphenol-A (BPA), phthalates, diethylstilbestrol and parabens are residential part of manufactured substances [3,4,5,6,7]. Regarding the importance of the developmental origin of health and disease theory, exposure to these exogenous chemicals during pregnancy predisposes the fetus to organ dysfunction and chronic diseases in adulthood because of long-lasting and permanent alterations in the molecular, cellular, and hormonal signaling pathways [8,9,10,11,12]. Identifying the most important and dangerous EDCs, and initiating preventive strategies will help to minimize the health and economic consequences of EDCs for future generations. Herein, the associations between maternal exposure to EDCs during pregnancy with the mean changes of factors related to the cardio-metabolic disorders including triglyceride (TG), total cholesterol (TC), low density lipoprotein- cholesterol (LDL-C), high density lipoprotein-cholesterol (HDL-C), fasting blood sugar (FBS), systolic and diastolic blood pressure (SBP and DBP), body mass index (BMI), and waist circumference (WC) was studied in children.
Materials and methods
Literature search
The PubMed, Scopus, EMBASE, and Web of Science databases were systematically searched by two independent researchers for relevant studies published before February 2023. Detailed search strategies have been presented in Additional file 1: Table S1. There was not any language restriction. The search was performed using search terms, that were based on a combination of indexed and free-text terms included: “endocrine-disrupting,” endocrine disruptor, endocrine-disrupting chemicals, maternal, pregnancy, "maternal exposure" "lipid profile," triglyceride, "low-density lipoprotein," high-density lipoprotein," LDL-C, HDL-C, cholesterol, "blood pressure," "systolic blood pressure," "diastolic blood pressure," "fasting blood sugar," FBS, weight, BMI, body mass index, and waist circumference. To avoid losing an article, references of all review articles were also checked manually. The reference list of the included articles was also manually searched.
Study selection
Inclusion criteria were based on the population, exposure, comparison, outcome and study design (PECOS) approach (11) as follows: (1) population: pregnant women and child, (2) exposure: exposure to EDCs during the pregnancy, (3) comparison: pregnant women with the higher degrees of exposure versus the lower degrees, (4) outcome: estimated changes in TG, TC, LDL-C, HDL-C, FBS, SBP, DBP, BMI and WC, (5) study design: cohort studies.
We evaluated studies based on the following inclusion criteria: studies with cohort design that examined the association between EDC exposure in pregnancy and its effects on a child’s outcome that have been reported as an odds ratio (OR) with a 95% confidence interval (CI) or could be calculated from the provided data. We excluded studies if they had the following criteria: case–control, and cross-sectional design, reviews, letters, interventions, and conference papers, publications with no complete reports, exposure assessment in children only. In the case of studies in which more than one article was published from the same data, a study with a larger sample size was included in the meta-analysis.
Data extraction and qualitative assessment
At the first, descriptive information was extracted from all studies. This information included the name of the first author, year of publication, the country of study, type of EDC, sample size, the mean age of participants, and the risk estimates with 95% CI. The Newcastle–Ottawa Scale (NOS) tool was used to classify the quality score of studies as follows: low quality = 0–4; moderate-quality = 5–6; high quality = 7–9 [13]. Two reviewers independently conducted the risk of bias assessment (MR and SNM); disagreements were resolved after discussion with a third reviewer (MAM).
Statistical analysis
All statistical analyses were conducted using Stata 14 (Stata Corporation, College Station, TX, U.S.A.). We aggregated the studies into four general groups according to the type of EDC including BPA, pesticides, phthalates, and other EDCs. A fixed- and random- model effects were used to estimate the effect size and heterogeneity of studies. The heterogeneity was evaluated by the χ2-Q statistics and I2 that is classified as follows: I2 < 30% mild, I2 = 30–75% moderate and high if I2 > 75% [14]. A random-effects model was used for the variables that had considerable heterogeneity between studies. To identify the potential sources of heterogeneity, the subgroup analysis was performed based on the country (the USA vs. other countries), sample type (serum or urine), pregnancy time for sampling (the first trimester of pregnancy vs. 2nd or 3th trimesters), age of child in the evaluation time (≤ 4 or > 4 yrs.), and the type of EDC (BPA, phthalates, pesticides or other EDC). The effect of each study on the overall estimates was studied by the leave-one-out method. Also, the publication bias was assessed by the funnel plots, Begg's rank correlation, and Egger's linear regression tests. We followed the conventional cut-offs to interpret the effect size (r) as weak (≤ 0.35), moderate (≤ 0.36—0.67), and strong (≤ 0.68–1.00) [15].
Results
Findings of the systematic review
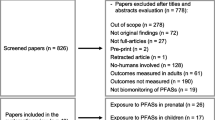
As shown in Fig. 1, the early search resulted in 7769 studies after duplicate removal. After the first screening and reading the article’s title and abstract, 6480 papers were excluded due to the unrelated titles. In the second phase of screening, 1216 articles were again excluded due to the unrelated data, animal subjects, being review articles, etc. In total, 73 papers were evaluated for eligibility, and 43 articles were excluded for the following reasons: maternal exposure was not assessed, the concentration of chemicals was not reported, risk estimate was not reported, and two studies were based on the same data. Finally, 30 studies were included for the final analysis [16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45].

PRISMA flow diagram of study selection
The characteristics of the included studies in this systematic review and meta-analysis have been presented in Table 1. These studies were published among 2008 to 2022, and all included studies had a cohort design. Among the included studies, ten studies were reported from the USA and twenty from other countries. Studies included in the final analysis were conducted in several countries, including: Spain [18, 20, 24, 29, 33, 35], China [22, 44], USA [17, 19, 26, 27, 31, 36, 40, 42], Italy [45], Netherland [21], Denmark [23, 39], Korea [25, 30, 43], Belgium [41], Canada [32, 34], and Greece [28, 29]. Except of one cohort study that evaluated prenatal exposure to the EDCs in newborns, other studies assessed this association in the age of 2 to 8 years. The number of cases varied from 105 to 4065. The type of evaluated EDCs was different in most studies. As mentioned, we categorized and evaluated EDCs into four main groups, including BPA, phthalates, pesticides, and other EDCs. Based on this category, eleven studies evaluated BPA, twelve studies assessed phthalates, ten evaluated pesticides, and finally, eleven cohorts examined other EDCs. It should be noted that some studies have examined more than one EDC. In terms of the study quality, the total score quality was shown in Table 1, and the detailed score for each study was reported in Additional file 1: Table S2. According to the total score, nine studies had moderate-quality, and others had good quality.
Association between maternal exposures to the EDCs with the glycemic profile
Only two studies evaluated the effects of maternal EDC exposure with child’s FBS [22, 45]. Warner et al. included 426 children in their study and evaluated the association between maternal 2,3,7,8-tetrachlorodibenzo-p-dioxin (TCDD) and glycemic profile in children. Maternal exposure to the TCDD showed an inverse association with serum insulin (adj-β = -1.24 μIU/mL, 95% confidence interval (CI): -2.38, -0.09) and HOMA2-B (adj-β = − 10.2% decrease, 95% CI: − 17.8, − 1.9) in girls, but these associations were not statistically significant among boys (insulin: adj-β = 0.57 μIU/mL, 95% CI: − 0.84, 1.98, P for interaction = 0.04; and HOMA2-B: adj-β = 0.8% increase, 95% CI -10.7, 13.9, P for interaction = 0.11) [45]. In addition, medium maternal prenatal BPA level showed a moderately significant association with serum plasma glucose in boys 0.36 (95% CI: 0.04 to 0.68) in another study. However, no associations were found between prenatal exposure to BPA and serum insulin level in girls and boys [22].
Association between maternal exposures to EDCs with lipid profile
Overall, six studies considered the association between the maternal exposure to the EDCs and serum TG level [19, 23, 24, 29, 30, 37]. These studies included 3334 participants. No significant association was seen between the maternal exposure to the EDCs and serum TG level (Fisher_Z: -0.02, CI: -0.05, 0.02) per doubling EDCs levels (Fig. 2).

Overall effect of maternal exposure to the EDCs on serum triglyceride level in children
There was a high heterogeneity between studies (I2 = 97.8%, P < 0.001). The results of the subgroup analysis have been reported in Additional file 1: Table S3.
In a subgroup analysis, a significant association was found between maternal exposure to the EDCs and serum TG level in children, in studies performed at the second and third trimester of pregnancy. The visual inspection of the funnel plot has been presented in Additional file 1: Fig S1. The sensitivity analysis did not show any change in the results.
There was not a significant association between maternal exposure to the EDCs with serum TC (Fisher_Z: -0.02, CI: -0.05, 0.01). A significant heterogeneity was observed among studies (I2 = 86.4%, P < 0·001) (Fig. 3).

Overall effect of maternal exposure to the EDCs on serum total cholesterol level in children
Subgroup analysis did not find any source of heterogeneity regarding serum TC. Also, there was not any evidence of publication bias in the Begg (P = 0.707), Egger's regression tests (P = 0.436) and the funnel plot (Additional file 1: Fig S2). Sensitivity analysis did not show any change in the results.
Five studies evaluated the associations between maternal exposure to the EDCs and serum HDL.C levels in children[19, 23, 24, 28, 37]. As shown in Fig. 4, there was not any significant association between EDCs and serum HDL.C (Fisher_Z: -0.02, CI: -0.06, 0.01). Studies showed a significant heterogeneity (I2 = 98.7%, P < 0·001). However, in the subgroup analysis, we found a significant association in each subgroup (Additional file 1: Table S4).

Overall effect of maternal exposure to the EDCs on serum HDL-C in children
We did not find any evidence of publication bias according to the Begg (P = 0.462), and Egger's regression tests (P = 0.990) and funnel plot (Additional file 1: Fig S3). Sensitivity analysis did not show any change in the results.
Association between maternal exposures to the EDCs with blood pressure
Eight studies with 14 effect sizes reported the association between EDCs exposure with DBP [16, 18, 21, 22, 25, 28, 29, 33]. We found that EDCs exposure during pregnancy had a weakly significant correlation with lower DBP in children (Fisher_Z: -0.16, CI: -0.19, -0.13), with a significant heterogeneity between studies (I2 = 98.6%, P < 0·001) (Fig. 5). Subgroup analysis did not report any new findings (Additional file 1:Table 5). We did not find the source of heterogeneity in the subgroup analysis. We did not find any evidence of publication bias according to the Begg (P = 0.869), Egger's regression tests (P = 0.3), and funnel plot in term of DBP (Additional file 1: Fig S4).

Overall effect of maternal exposures to the EDCs on DBP in children
Also, in eight studies with 15 effect sizes, the association between maternal exposure to the EDCs and SBP was reported. We found that maternal exposures to the EDCs had a weakly significant correlation with higher child’s SBP (Fisher_Z: 0.06, CI: 0.04, 0.08) (Fig. 6). The studies showed a significant heterogeneity (I2 = 94.2%, P < 0·001) (Fig. 5). Subgroup analysis did not find the source of the heterogeneity. We did not find any evidence of publication bias according to the Begg (P = 0.456), Egger's regression tests (P = 0.385) and the funnel plot (Additional file 1: Fig S4). Sensitivity analysis did not show any change in the results.

Overall effect of maternal exposures to the EDCs on SBP in children
Association between maternal exposures to the EDCs with child’s BMI and WC z-score
Twenty-one studies with 29 effect sizes reported the association between maternal exposures to the EDCs and child’s BMI z-score. As shown in Fig. 7, maternal exposure to the EDCs had a weakly significant correlation with higher BMI z-score in children (Fisher_Z: 0.04, CI: 0.03, 0.06). The included studies showed a significant heterogeneity (I2 = 91.3%, P < 0·001). Maternal exposures to the EDCs showed a significant effect on BMI z-score in the non-US countries, sampling the urine at the first trimester of pregnancy throughout all ages (P < 0.05) ( Additional file 1:Table 6). Moreover, maternal exposures to the BPA and pesticides showed a weakly significant correlation with BMI z-score in children (Fisher_Z: 0.14, CI: 0.08, 0.19, P < 0.001 for BPA and Fisher_Z: 0.1, CI: 0.08, 0.12, P < 0.001 for pesticides). Other EDCs showed a weak reverse association with BMI z-score in children (Fisher_Z: -0.09, CI: -0.13, -0.06, P < 0.001). The visual inspection of the funnel plot has been presented in Fig. 5S. Sensitivity analysis did not show any change in the results.

Overall effect of maternal exposures to the EDCs on BMI z-score in children
Fourteen studies with nineteen effect sizes reported the association of maternal exposures to the EDCs with a child’s WC [18, 23, 24, 26,27,28, 32,33,34, 36,37,38,39, 41]. As shown in Fig. 8, there was a weakly significant association between maternal exposures to the EDCs and WC z-score in children (Fisher_Z: 0.06, CI: 0.03, 0.08). The included studies showed a significant heterogeneity (I2 = 99%, P < 0·001). The subgroup analysis showed a significant association between the maternal exposures to the EDC with WC z-score in the studies conducted in the USA, using urine samples in the first trimester of pregnancy and children ≤ 4. Moreover, a significant association was observed between maternal exposures to the BPA and pesticide with WC z-score. However, this association was reverse in the other EDCs (Additional file 1:Table 6). We did not find any evidence of publication bias according to the Begg (P = 0.063), Egger's regression tests (P = 0.556), and the funnel plot (Additional file 1: Fig S5). Sensitivity analysis did not show any change in the results.

Overall effect of maternal exposures to the EDCs on WC z-score in children
Discussion
Results of the present systematic review and meta-analysis on previous cohort studies showed a significant linear association between maternal exposures to the EDCs with BMI, WC z-scores and SBP in children. However, our results showed an inverse correlation between maternal exposures to the EDCs with DBP. There wasn’t any significant association between maternal exposures to the EDCs with lipid profile.
The results regarding the association between maternal EDC exposure and glycemic profile in children were limited, with only two studies providing relevant data [46, 47]. While Warner et al. found an inverse association between maternal exposure to 2,3,7,8-tetrachlorodibenzo-p-dioxin (TCDD) and serum insulin and HOMA2-B in girls, no significant associations were observed in boys [48]. Another study reported a significant association between medium maternal prenatal BPA levels and serum plasma glucose in boys but not in girls [47]. The observed gender-specific associations between maternal EDC exposure and glycemic parameters in children in some studies could be attributed to differences in hormonal regulation and metabolic processes between boys and girls. It's well-established that sex hormones, such as estrogen and testosterone, play crucial roles in modulating glucose metabolism and insulin sensitivity [49]. Therefore, exposure to EDCs during critical periods of development, such as prenatal or early postnatal stages, may disrupt the normal hormonal milieu and contribute to dysregulation of glycemic control in a sex-specific manner.
One potential mechanism underlying the observed associations involves disruption of the endocrine system by EDCs, leading to alterations in insulin signaling pathways and glucose homeostasis. For instance, TCDD, a well-known EDC, has been shown to affect insulin secretion and sensitivity by binding to the aryl hydrocarbon receptor (AhR) and modulating downstream signaling pathways involved in glucose metabolism [50]. Similarly, BPA, another prevalent EDC, has been implicated in impairing pancreatic β-cell function and insulin sensitivity through its estrogenic activity and interference with insulin receptor signaling [51]. Furthermore, emerging evidence suggests that EDCs may exert epigenetic effects, leading to persistent alterations in gene expression patterns related to glucose metabolism and insulin sensitivity. Epigenetic modifications, such as DNA methylation and histone acetylation, can modulate the expression of key genes involved in glycemic regulation, potentially predisposing individuals to metabolic disorders later in life [52, 53]. Importantly, these epigenetic changes may exhibit sex-specific patterns due to differences in sex chromosome composition and hormonal regulation of epigenetic machinery [54,55,56].
In terms of lipid profile, the meta-analysis did not reveal a significant association between maternal EDC exposure during pregnancy and serum TG or TC levels in children. However, subgroup analysis identified a significant association between maternal EDC exposure and serum TG levels in studies conducted during the second and third trimesters of pregnancy. This suggests a potential window of vulnerability during later stages of gestation. Similarly, no significant association was found between maternal EDC exposure and serum HDL-C levels in children. The lack of a significant association between maternal EDC exposure during pregnancy and serum TG or TC levels in children, as indicated by the meta-analysis, suggests that the overall impact of maternal EDC exposure on lipid metabolism may be nuanced and multifactorial. However, subgroup analysis revealing a significant association between maternal EDC exposure and serum TG levels specifically in studies conducted during the second and third trimesters of pregnancy suggests a potential window of vulnerability during later stages of gestation. This observation aligns with previous evidence suggesting that fetal development during late gestation is particularly sensitive to environmental exposures, including EDCs, which may influence metabolic programming and long-term health outcomes [57,58,59].
One potential mechanism underlying the observed association between maternal EDC exposure and serum TG levels in children could involve disruption of lipid metabolism pathways. EDCs, such as BPA and phthalates, have been shown to interfere with lipid synthesis, transport, and metabolism through various mechanisms, including activation of nuclear receptors (e.g., peroxisome proliferator-activated receptors, PPARs) and modulation of lipid-related gene expression[60, 61]. For example, BPA exposure has been associated with dysregulation of lipogenic genes in animal models, leading to increased hepatic lipid accumulation and altered serum lipid profiles [62]. Similarly, phthalate exposure has been linked to impaired lipid metabolism and dyslipidemia in both animal and human studies [63, 64].
The observed association between maternal EDC exposure and lower DBP but higher SBP in children suggests that EDCs may exert differential effects on blood pressure regulation depending on various factors, including the specific types of EDCs involved, timing of exposure, and individual susceptibility. This discrepancy underscores the multifaceted nature of EDC-induced alterations in cardiovascular health. One potential mechanism underlying the observed associations involves disruption of the renin–angiotensin–aldosterone system (RAAS), a key regulator of blood pressure and fluid balance. EDCs, such as BPA and phthalates, have been shown to interfere with RAAS signaling pathways through various mechanisms, including activation of angiotensin receptors and modulation of aldosterone synthesis and secretion [65, 66]. Dysregulation of RAAS activity can lead to alterations in vascular tone, sodium retention, and fluid volume, ultimately impacting blood pressure regulation in offspring exposed to EDCs during critical periods of development [67, 68]. Furthermore, emerging evidence suggests that maternal EDC exposure may influence vascular function and endothelial homeostasis, contributing to alterations in blood pressure regulation in offspring. EDCs, including PCBs and organochlorine pesticides, have been shown to impair endothelial function and induce vascular inflammation through oxidative stress-mediated mechanisms [69, 70]. Additionally, EDC-induced alterations in neuroendocrine signaling pathways, such as the sympathetic nervous system and hypothalamic–pituitary–adrenal (HPA) axis, may also contribute to changes in blood pressure regulation in offspring. EDCs, such as phthalates and perfluoroalkyl substances (PFAS), have been implicated in dysregulation of sympathetic nerve activity and cortisol secretion, which can influence vascular tone and blood pressure responsiveness [71, 72].
The association between maternal EDC exposure and child adiposity, as assessed by BMI z-score and waist circumference (WC) z-score, was consistently significant. EDCs, such as BPA and phthalates, have been shown to interfere with endocrine systems involved in adipocyte differentiation, proliferation, and metabolism. These chemicals can disrupt hormone receptors, including peroxisome proliferator-activated receptors (PPARs) and estrogen receptors, leading to dysregulation of adipogenic and lipogenic pathways [1, 73]. For instance, BPA exposure has been associated with increased adipocyte size, altered adipokine secretion, and impaired insulin sensitivity in animal and human studies [74, 75]. Similarly, phthalate exposure has been linked to adipocyte hypertrophy, adipose tissue inflammation, and insulin resistance in both experimental models and epidemiological studies [76, 77].
The present study had some limitations that should be considered in the interpretation of the results. First, heterogeneity between studies was high in most of the evaluated variables. Second, difficulty in discriminating between the effects of exposure during pregnancy and exposure after birth. Third, some of the included studies in the meta-analysis had relatively small sample sizes, which could affect the statistical power to detect significant associations. Fourth, due to the observational nature of the included cohort studies, causal relationships between maternal exposure to EDCs and cardio-metabolic risk factors in children cannot be definitively established.
In conclusion, prenatal exposure to EDCs during the uterine period may elevate the risk of childhood obesity, particularly the visceral form. BPA and pesticides demonstrated the strongest association with WC and BMI z-score. Furthermore, urine sampling from mothers to assess BPA and pesticide concentrations in the first trimester of pregnancy revealed a significant linear association with BMI and WC z-scores in children aged 2–8 years. Therefore, identifying these pollutants and their sources is crucial for preventing childhood obesity. According to our review, no study was founded in Iran about maternal exposure to EDCs during gestation and their consequences on the growth and metabolic markers in children. Based on the differences about environmental contaminants, it is suggested to researchers on Iranian population for future studies. All community members, especially pregnant women, the next generations, policy and health decision makers will benefit from these results. However, the cause-effect of EDCs on metabolism is lacking and precise molecular mechanisms are unclear. More molecular studies are needed in this field.
Availability of data and materials
Data will be available by the corresponding author based on request.
References
Gore AC, et al. EDC-2: the Endocrine Society’s second scientific statement on endocrine-disrupting chemicals. Endocr Rev. 2015;36(6):E1–150.
Monneret C. What is an endocrine disruptor? CR Biol. 2017;340(9–10):403–5.
Encarnação T, et al. Endocrine disrupting chemicals: Impact on human health, wildlife and the environment. Sci Prog. 2019;102(1):3–42.
Birks L, et al. Occupational exposure to endocrine-disrupting chemicals and birth weight and length of gestation: a European meta-analysis. Environ Health Perspect. 2016;124(11):1785–93.
Vahdat M, et al. Effects of resistant starch interventions on circulating inflammatory biomarkers: a systematic review and meta-analysis of randomized controlled trials. Nutr J. 2020;19:1–10.
La Merrill MA, et al. Consensus on the key characteristics of endocrine-disrupting chemicals as a basis for hazard identification. Nat Rev Endocrinol. 2020;16(1):45–57.
Kassotis CD, Stapleton HM. Endocrine-mediated mechanisms of metabolic disruption and new approaches to examine the public health threat. Front Endocrinol. 2019;10: 427728.
Schug TT, et al. Minireview: endocrine disruptors: past lessons and future directions. Mol Endocrinol. 2016;30(8):833–47.
Mousavi SN, et al. Extra virgin olive oil in maternal diet increases osteogenic genes expression, but high amounts have deleterious effects on bones in mice offspring at adolescence. Iran J Basic Med Sci. 2016;19(12):1299.
Slama R, et al. Scientific issues relevant to setting regulatory criteria to identify endocrine-disrupting substances in the European Union. Environ Health Perspect. 2016;124(10):1497–503.
Papalou O, Papadakis G, Diamanti-Kandarakis E. Endocrine disrupting chemicals: an occult mediator of metabolic disease. Front Endocrinol. 2019;10: 429401.
Morvaridzadeh M, et al. Effect of ginger (Zingiber officinale) supplementation on oxidative stress parameters: a systematic review and meta-analysis. J Food Biochem. 2021;45(2): e13612.
Wells, G.A., et al., The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. 2000.
Chandler, J., M. Cumpston, and T. Li, Cochrane Handbook for Systematic Reviews of Interventions.
Taylor R. Interpretation of the correlation coefficient: a basic review. Journal of diagnostic medical sonography. 1990;6(1):35–9.
Montazeri P, et al. Prenatal exposure to phthalates and phenols and preclinical vascular health during early adolescence. Int J Hyg Environ Health. 2022;240: 113909.
Zuo L, et al. Pyrethroids exposure induces obesity and cardiometabolic diseases in a sex-different manner. Chemosphere. 2022;291: 132935.
Güil-Oumrait N, et al. Prenatal exposure to persistent organic pollutants and markers of obesity and cardiometabolic risk in Spanish adolescents. Environ Int. 2021;151: 106469.
Kupsco A, et al. Prenatal maternal phthalate exposures and trajectories of childhood adiposity from four to twelve years. Environ Res. 2022;204: 112111.
Smink A, et al. Exposure to hexachlorobenzene during pregnancy increases the risk of overweight in children aged 6 years. Acta Paediatr. 2008;97(10):1465–9.
Sol CM, et al. Associations of maternal phthalate and bisphenol urine concentrations during pregnancy with childhood blood pressure in a population-based prospective cohort study. Environ Int. 2020;138: 105677.
Ouyang F, et al. Maternal prenatal urinary bisphenol A level and child cardio-metabolic risk factors: A prospective cohort study. Environ Pollut. 2020;265: 115008.
Jensen RC, et al. Prenatal exposures to perfluoroalkyl acids and associations with markers of adiposity and plasma lipids in infancy: An odense child cohort study. Environ Health Perspect. 2020;128(7): 077001.
Manzano-Salgado CB, et al. Prenatal exposure to perfluoroalkyl substances and cardiometabolic risk in children from the Spanish INMA birth cohort study. Environ Health Perspect. 2017;125(9): 097018.
Bae S, et al. Maternal urinary bisphenol A concentration during midterm pregnancy and children’s blood pressure at age 4. Hypertension. 2017;69(2):367–74.
Vuong AM, et al. Prenatal polybrominated diphenyl ether exposure and body mass index in children up to 8 years of age. Environ Health Perspect. 2016;124(12):1891–7.
Maresca MM, et al. Prenatal exposure to phthalates and childhood body size in an urban cohort. Environ Health Perspect. 2016;124(4):514–20.
Vafeiadi M, et al. Association of prenatal exposure to persistent organic pollutants with obesity and cardiometabolic traits in early childhood: the Rhea mother–child cohort (Crete, Greece). Environ Health Perspect. 2015;123(10):1015–21.
Vafeiadi M, et al. Association of early life exposure to bisphenol A with obesity and cardiometabolic traits in childhood. Environ Res. 2016;146:379–87.
Kim JH, et al. Association of diethylhexyl phthalate with obesity-related markers and body mass change from birth to 3 months of age. J Epidemiol Community Health. 2016;70(5):466–72.
Buckley JP, et al. Prenatal phthalate exposures and body mass index among 4-to 7-year-old children: a pooled analysis. Epidemiology. 2016;27(3):449–58.
Braun JM, et al. Early-life bisphenol a exposure and child body mass index: a prospective cohort study. Environ Health Perspect. 2014;122(11):1239–45.
Valvi D, et al. Prenatal phthalate exposure and childhood growth and blood pressure: evidence from the Spanish INMA-Sabadell Birth Cohort Study. Environ Health Perspect. 2015;123(10):1022–9.
Erkin-Cakmak A, et al. In utero and childhood polybrominated diphenyl ether exposures and body mass at age 7 years: the CHAMACOS study. Environ Health Perspect. 2015;123(6):636–42.
Agay-Shay K, et al. Exposure to endocrine-disrupting chemicals during pregnancy and weight at 7 years of age: a multi-pollutant approach. Environ Health Perspect. 2015;123(10):1030–7.
Tang-Péronard JL, et al. Association between prenatal polychlorinated biphenyl exposure and obesity development at ages 5 and 7 y: a prospective cohort study of 656 children from the Faroe Islands. Am J Clin Nutr. 2014;99(1):5–13.
Warner M, et al. Prenatal exposure to dichlorodiphenyltrichloroethane and obesity at 9 years of age in the CHAMACOS study cohort. Am J Epidemiol. 2014;179(11):1312–22.
Harley KG, et al. Prenatal and postnatal bisphenol A exposure and body mass index in childhood in the CHAMACOS cohort. Environ Health Perspect. 2013;121(4):514–20.
Andersen CS, et al. Prenatal exposures to perfluorinated chemicals and anthropometry at 7 years of age. Am J Epidemiol. 2013;178(6):921–7.
Cupul-Uicab LA, et al. Prenatal exposure to the major DDT metabolite 1, 1-dichloro-2, 2-bis (p-chlorophenyl) ethylene (DDE) and growth in boys from Mexico. Environ Res. 2010;110(6):595–603.
Delvaux I, et al. Prenatal exposure to environmental contaminants and body composition at age 7–9 years. Environ Res. 2014;132:24–32.
Berger K, et al. Prenatal exposure to mixtures of phthalates, parabens, and other phenols and obesity in five-year-olds in the CHAMACOS cohort. Int J Environ Res Public Health. 2021;18(4):1796.
Lee D-W, et al. Prenatal exposure to di-(2-ethylhexyl) phthalate and decreased skeletal muscle mass in 6-year-old children: A prospective birth cohort study. Environ Res. 2020;182: 109020.
Yang C, et al. Prenatal exposure to organochlorine pesticides and infant growth: A longitudinal study. Environ Int. 2021;148: 106374.
Warner M, et al. Prenatal dioxin exposure and glucose metabolism in the Seveso Second Generation study. Environ Int. 2020;134: 105286.
Street ME, et al. Current knowledge on endocrine disrupting chemicals (EDCs) from animal biology to humans, from pregnancy to adulthood: highlights from a national Italian meeting. Int J Mol Sci. 2018;19(6):1647.
Harley KG, et al. Association of phthalates, parabens and phenols found in personal care products with pubertal timing in girls and boys. Hum Reprod. 2019;34(1):109–17.
Eskenazi B, et al. Serum dioxin concentrations and endometriosis: a cohort study in Seveso. Italy Environ Health Perspect. 2002;110(7):629–34.
Mauvais-Jarvis F, Clegg DJ, Hevener AL. The role of estrogens in control of energy balance and glucose homeostasis. Endocr Rev. 2013;34(3):309–38.
Hectors T, et al. Environmental pollutants and type 2 diabetes: a review of mechanisms that can disrupt beta cell function. Diabetologia. 2011;54:1273–90.
Alonso-Magdalena P, Quesada I, Nadal A. Endocrine disruptors in the etiology of type 2 diabetes mellitus. Nat Rev Endocrinol. 2011;7(6):346–53.
Nilsson E, et al. Environmentally induced epigenetic transgenerational inheritance of ovarian disease. PLoS ONE. 2012;7(5): e36129.
Rahimlu M, Shab-Bidar S, Djafarian K. Body mass index and all-cause mortality in chronic kidney disease: a dose–response meta-analysis of observational studies. J Ren Nutr. 2017;27(4):225–32.
Gharipour M, et al. Sex based levels of C-reactive protein and white blood cell count in subjects with metabolic syndrome: Isfahan Healthy Heart Program. J Res Med Sci. 2013;18(6):467.
Mirhafez S, et al. Serum high-sensitivity C-reactive protein as a biomarker in patients with metabolic syndrome: evidence-based study with 7284 subjects. Eur J Clin Nutr. 2016;70(11):1298–304.
Hashemi R, et al. Investigating the effect of DASH diet on blood pressure of patients with type 2 diabetes and prehypertension: Randomized clinical trial. Diabetes Metab Syndr. 2019;13(1):1–4.
Barker DJ. The developmental origins of chronic adult disease. Acta Paediatr Suppl. 2004;93(446):26–33.
Mallozzi M, et al. The effect of maternal exposure to endocrine disrupting chemicals on fetal and neonatal development: A review on the major concerns. Birth Defects Res C Embryo Today. 2016;108(3):224–42.
Rahimlou M, et al. Effects of ginger supplementation on anthropometric, glycemic and metabolic parameters in subjects with metabolic syndrome: A randomized, double-blind, placebo-controlled study. J Diabetes Metab Disord. 2019;18(1):119–25.
Grün F, Blumberg B. Endocrine disrupters as obesogens. Mol Cell Endocrinol. 2009;304(1–2):19–29.
Feige JN, et al. The endocrine disruptor monoethyl-hexyl-phthalate is a selective peroxisome proliferator-activated receptor γ modulator that promotes adipogenesis. J Biol Chem. 2007;282(26):19152–66.
Wang T, et al. Urinary bisphenol A (BPA) concentration associates with obesity and insulin resistance. J Clin Endocrinol Metab. 2012;97(2):E223–7.
Gascon M, et al. Effects of persistent organic pollutants on the developing respiratory and immune systems: a systematic review. Environ Int. 2013;52:51–65.
Hatch EE, et al. Association of urinary phthalate metabolite concentrations with body mass index and waist circumference: a cross-sectional study of NHANES data, 1999–2002. Environ Health. 2008;7:1–15.
Rezg R, et al. Bisphenol A and human chronic diseases: current evidences, possible mechanisms, and future perspectives. Environ Int. 2014;64:83–90.
Ferguson KK, McElrath TF, Meeker JD. Environmental phthalate exposure and preterm birth. JAMA Pediatr. 2014;168(1):61–7.
Fonseca MI, Lorigo M, Cairrao E. Endocrine-disrupting effects of bisphenol A on the cardiovascular system: a review. Journal of xenobiotics. 2022;12(3):181–213.
Parsi A, et al. The effects of crocus sativus extract on serum lipid profile and liver enzymes in patients with non-alcoholic fatty liver disease: a randomized placebo-controlled study. Obesity Medicine. 2020;17: 100165.
Brook RD, Rajagopalan S. Particulate matter air pollution and atherosclerosis. Curr Atheroscler Rep. 2010;12:291–300.
Adu-Gyamfi EA, Rosenfeld CS, Tuteja G. The impact of bisphenol A on the placenta. Biol Reprod. 2022;106(5):826–34.
Deierlein AL, et al. Longitudinal associations of phthalate exposures during childhood and body size measurements in young girls. Epidemiology. 2016;27(4):492–9.
Kataria A, Trasande L, Trachtman H. The effects of environmental chemicals on renal function. Nat Rev Nephrol. 2015;11(10):610–25.
Faulk C, Dolinoy DC. Timing is everything: the when and how of environmentally induced changes in the epigenome of animals. Epigenetics. 2011;6(7):791–7.
Carwile JL, Michels KB. Urinary bisphenol A and obesity: NHANES 2003–2006. Environ Res. 2011;111(6):825–30.
Hugo ER, et al. Bisphenol A at environmentally relevant doses inhibits adiponectin release from human adipose tissue explants and adipocytes. Environ Health Perspect. 2008;116(12):1642–7.
Trasande L, Attina TM, Blustein J. Association between urinary bisphenol A concentration and obesity prevalence in children and adolescents. JAMA. 2012;308(11):1113–21.
Diamanti-Kandarakis, E., et al., The impact of endocrine disruptors on endocrine targets. Hormone and Metabolic Research, 2010: p. 543–552.
Acknowledgements
All authors are very thanks from researchers of the previous related studies.
Funding
No funding received.
Author information
Authors and Affiliations
Contributions
SNM, MP and HCh designed the present study. MR, and SNM searched systematically. MR, MAM, and SNM reviewed and selected the articles and extracted data from articles. MP and HCh performed quality assessment of the trials. MR performed data analysis and interpretation. MR, SNM and MAM drafted the manuscript. All authors read the final version of manuscript and revised it.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Competing interests
The authors declare no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Table S1.
Detailed search strategies of the association between EDCs exposure and risk of EMs. Table S2. Quality assessment of studies included in the meta-analysis. Table S3. Subgroup analyses for association between maternal exposures to the EDC and serum TG in children. Fig S1. Funnel plot for serum triglyceride level. Fig S2. Funnel plot for serum total cholesterol in children. Table S4. Subgroup analysis of association between maternal exposures to the EDCs with serum HDL-C in children. Fig S3. Funnel plot for HDL- C in children. Fig S4. Funnel plot for SBP (A) and DBP (B) in children. Table S5. Subgroup analysis of association between maternal exposures to the EDCs and blood pressure in children. Table S6. Subgroup analysis of association between maternal exposures to the EDC with BMI and waist circumference z-score in children. Fig S5. Funnel plot for BMI and WC z-score in children.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Rahimlou, M., Mousavi, M.A., Chiti, H. et al. Association of maternal exposure to endocrine disruptor chemicals with cardio-metabolic risk factors in children during childhood: a systematic review and meta-analysis of cohort studies. Diabetol Metab Syndr 16, 82 (2024). https://doi.org/10.1186/s13098-024-01320-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13098-024-01320-0