
Abstract
Background
Type 1 diabetes (T1D) is a major risk factor for cardiovascular disease (CVD). Matrix metalloproteinase-14 (MMP-14) is involved in the development of atherosclerosis and CVD. The main aim was to explore the associations between MMP-14 and selected inflammatory and metabolic variables, CVD, depression, physical activity, smoking and medication in patients with T1D. The secondary aim was to explore associations with CVD.
Methods
Cross-sectional design. The participants were consecutively recruited from one specialist diabetes out-patient clinic. Depression was assessed by a self-report instrument. Blood samples, anthropometrics and blood pressure were collected, supplemented with data from electronic health records. High MMP-14 was defined as ≥ 5.81 ng/mL. Non-parametric tests, Chi2 tests and multiple logistic regression analyses were performed.
Results
Two hundred and sixty-eighth T1D patients aged 18–59 years participated (men 58%, high MMP-14 25%, CVD 3%). Sixty-seven patients with high MMP-14, compared to 201 patients with lower MMP-14, had higher prevalence of CVD (8% versus 1%, p = 0.012), and had higher levels of galectin-3 (p < 0.001) and MMP-2 (p = 0.018). Seven patients with CVD, compared to 261 without, were older (p = 0.003), had longer diabetes duration (p = 0.027), and had higher prevalence of high MMP-14 (71% versus 24%, p = 0.012), abdominal obesity (p = 0.014), depression (p = 0.022), usage of antidepressants (p = 0.008), antihypertensive drugs (p = 0.037) and statins (p = 0.049).
Galectin-3 (per ng/mL) [adjusted odds ratio (AOR) 2.19, p < 0.001], CVD (AOR 8.1, p = 0.027), and MMP-2 (per ng/mL) (AOR 1.01, p = 0.044) were associated with high MMP-14. Depression (AOR 17.4, p = 0.006), abdominal obesity (15.8, p = 0.006), high MMP-14 (AOR 14.2, p = 0.008), and diabetes duration (AOR 1.10, p = 0.012) were associated with CVD.
Conclusions
The main findings of this study were that galecin-3, MMP-2, and CVD were independently associated with high levels of MMP-14 in T1D patients. The association between MMP-14 and galectin-3 is a new finding. No traditional risk factors for CVD were associated with MMP-14. Depression, abdominal obesity and MMP-14 were independently associated with CVD.
Similar content being viewed by others


Background
Type 1 diabetes (T1D) is a major risk factor for cardiovascular disease (CVD) [1, 2]. The risk for developing CVD in people with T1D is increased by early onset, female sex, metabolic and inflammatory disturbances, unhealthy behaviour, depression, and chronic kidney disease [1,2,3,4,5,6].
Metalloproteinases (MPs) are vital for extracellular matrix (ECM) remodelling and degradation activities in multiple organ systems such as the cardiovascular (CV) and central nervous systems, as well as the kidneys [7,8,9,10,11,12]. MPs target a wide range of substrates, are involved in inflammatory and immune responses, and are regulated by their endogenous inhibitors—the tissue inhibitors of metalloproteinases (TIMPs) [7,8,9,10,11,12].
Several MPs are involved in the development of atherosclerosis which may lead to severe CVD such as ischemic heart disease, heart failure, stroke, and death [7,8,9, 11, 12]. Matrix metalloproteinases (MMPs) are expressed in atherosclerotic plaques, promoting vascular remodelling, contributing to atherothrombosis, and plaque disruption [9, 12,13,14]. They are also involved in cardiac remodelling after myocardial infarction, leading to dilated cardiomyopathy [9]. MMP-14, is a type 1 transmembrane proteinase (MT1-MMP) which modifies both the pericellular microenvironment in the ECM and the cell function, and is inhibited by TIMP-2 and TIMP-3 [15]. MMP-14 and TIMP-2 are both necessary for the activation of pro-MMP-2 [15]. MMP-14 has been confirmed in human atherosclerotic plaques and in cardiomyocytes [7, 13, 14]. It has been demonstrated that MMP-14 is upregulated in a particularly harmful macrophage phenotype (MMP14+TIMP3−), which contributes to increased risk for plaque rupture and myocardial infarction [14]. MMP-14 is also upregulated post-infarction contributing to cardiac remodelling [16]. Decreased levels of TIMP-3 have been linked to ventricular remodelling after myocardial infarction [17].
Increased plasma levels of MMP-2 have been demonstrated in people with T1D compared to non-diabetic controls [18]. MMP-2 has been linked to CVD and all-cause mortality [12, 19]. MMP-2 was in a previous study of heart failure correlated with Galectin-3 [20], which in turn previously was linked to atherosclerosis and CVD [21]. Increased MMP-9 levels have been linked to CVD [19, 22, 23]. Both increased levels of MMP-2 and MMP-9 stimulate the rupture of vulnerable arterial plaques [7]. Several cardiovascular risk factors, such as hyperglycemia, increased serum-lipids, and smoking, contribute to oxidative stress or the formation of advanced glycation end products, which in turn promote the activation of MMPs [9, 24].
We hypothesize that MMP-14 in a complex manner is involved in the development of CVD. The main aim was to explore theQuery associations between MMP-14 and selected inflammatory and metabolic variables, CVD, depression, physical activity, smoking, and medication, in patients with T1D. The secondary aim was to explore variables associated with CVD.
Materials and methods
Participants and study design
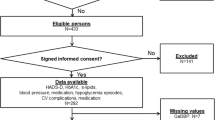
The study has a cross sectional design and included 268 (65%) patients out of 415 eligible patients with T1D. Inclusion criteria were T1D patients aged 18–59 years, diabetes duration ≥ 1-year, and performed measurements of MMP-14. Exclusion criteria were pregnancy, severe somatic and psychiatric disorders such as cancer, hepatic failure, end-stage renal disease, Cushing’s disease, severe autoimmune disorders, psychotic, bipolar or severe personality disorders, severe substance abuse, cognitive deficiency (due to stroke, dementia or intellectual disability), use of systemic corticosteroids, and inadequate knowledge of the Swedish language. The patients were consecutively recruited during a 9-month period, from 25 March to 28 December 2009, from the largest out of two hospital diabetes outpatient clinics in Region Kronoberg, Sweden. The catchment population was 1,25,000. A self-report questionnaire was used to assess depression. Blood samples, anthropometrics and blood pressure were collected, supplemented with data from electronic health records.
Cardiovascular disorder
CVD was defined as ischemic heart disease [angina pectoris, previous myocardial infarction, performed percutaneous transluminal coronary angioplasty (PTCA), and/or coronary artery bypass graft (CABP) surgery], heart failure, stroke, and/or transient ischemic attack (TIA).
Depression
Self-reported depression was assessed by Hospital Anxiety and Depression Scale- the depression subscale (HADS-D), and was defined as HADS-D ≥ 8 points [25, 26].
Thyroid disease
Patients treated for hypothyroidism or hyperthyroidism were identified, but not excluded.
Biochemical analyses
Plasma levels of MMP-2, MMP-14, TIMP-2, and TIMP-3, were analysed by using commercial human DuoSet enzyme linked immunosorbent assays (ELISAs) and supplementary ancillary kit (R&D Systems, Minneapolis, MN, USA). Before the analyses, the plasma samples were diluted in phosphate-buffered saline (PBS) supplemented with 1% bovine serum albumin (BSA), and were run in duplicates. The dilution factors were for MMP-2: 1:30; MMP-9: 1:400; MMP-14: 1:3 (1:25/1:50); TIMP-2: 1:400; TIMP-3: 1:16; and Galectin-3: 1:2. The ELISA analyses were performed according to the manufacturer’s instructions. Absorbance was measured at 450–580 nm in a FLOUstar optima plate reader (BMG Labtech Gmbh, Ortenberg, Germany). Concentrations of unknown samples were calculated using a 4-parameter logistic regression curve. The intra-assay coefficients of variation were for MMP-2: 3.7%; MMP-9: 2.2%; MMP-14: 2.8%; TIMP-2: 2.0%; TIMP-3: 1.6%; and galectin-3: 4.3%. The analyses were performed at the Diabetes Laboratory, BMC, Lund University, Lund.
For MMP-14 there were exact values for 173 patients, but for 95 patients the MMP-14 values were under the detection limit of 0.154 ng/mL. The undetected values were approximated by “zero”.
Hemoglobin A1c (HbA1c) and serum (s)-lipids were collected after overnight fasting and analysed with an Olympus automated clinical chemistry analyser with high specificity (Olympus AU®, Tokyo, Japan). The intra-coefficients of variation were for HbA1c < 1.2%; total cholesterol < 2.1%; High-density lipoprotein (HDL)-cholesterol < 3.0%; low-density lipoprotein (LDL)-cholesterol < 2.6%; and for triglycerides < 2.2%.
S-creatinine was assayed by an AU2700® instrument (Beckman Coulter, Brea, CA, USA). The intra-coefficient of variation was < 3%. HbA1c, s-lipids and s-creatinine were analysed at the department of Clinical Chemistry, Växjö Central Hospital.
CRP was assayed by spectrophotometry on a Roche Cobas C501® at the diabetes laboratory, Lund University Hospital, Lund.
Anthropometrics and blood pressure
Waist circumference, weight and length were measured by a nurse. Body mass index (BMI) (kg/m2) was calculated. Abdominal obesity was defined as WC ≥ 1.02 m for men and as WC ≥ 0.88 m for women [27]. Blood pressure was measured according to standard procedures in the sitting position by a nurse.
Smoking and physical activity
Smokers were defined as having smoked any amount of tobacco during the last year [27]. Information regarding levels of physical activity was collected by interviews performed by skilled nurses or physicians. Five levels were initially registered as in the Swedish National Diabetes Register (S-NDR) [28]: ≥ 30 min of moderate activities were performed either (1) never, (2) less than once a week, (3) 1–2 times a week, (4) 3–5 times a week, or (5) daily. In this study, level 1 and 2 were merged into one level: less than once a week.
Treatment for T1D
The patients used either multiple daily insulin injections (MDII) or continuous subcutaneous insulin infusion (CSII) administered by a pump.
Antihypertensive drugs and indications for treatment of hypertension
Antihypertensive drugs included ACE inhibitors (ATC codes C09AA-BA); (ARB) (ATC codes C09CA-DA); calcium antagonists (ATC codes C08CA01-02); diuretics (ATC codes C03AA03 or C03CA01); and/or selective beta-adrenoreceptor antagonists (ATC code C07AB). Indications for antihypertensive drugs were systolic BP > 130 mm Hg and/or BP > 80 mm Hg and/or CVD according to the Swedish national guidelines in 2009 [29]. The use of antihypertensive drugs was dichotomized into users and non-users.
Lipid-lowering drugs and indications for treatment of hyperlipidemia
Lipid-lowering drugs were hydroxy-methylglutaryl coenzyme A (HMG-CoA) reductase inhibitors (statins) (ATC-code C10AA). Indications for lipid-lowering drugs were total cholesterol > 4.5 mmol/L (> 1.74 mg/dL) and/or LDL-cholesterol > 2.5 mmol/L (> 97 mg/dL) or present CVD according to the Swedish national guidelines in 2009 [29]. The use of lipid-lowering drugs was dichotomized into users and non-users.
Antidepressants
Antidepressants were SSRIs, SNRIs and/or specific serotonergic antidepressants (N06AB, N06AX16, or N06AX11). The use of antidepressants was dichotomized into users and non-users.
Statistical analysis
Analysis of data distribution using histograms revealed that age, diabetes duration, and the inflammatory plasma biomarkers were not normally distributed. Data were presented as median [quartile (q)1, q3; min–max], and analyses were performed with Mann–Whitney U test. Fisher’s Exact Test (two-tailed) and Linear-by-linear association were used to analyse categorical data, and data were presented as N (%). Medians and prevalence rates for the included variables were compared between patients with high MMP-14 (≥ 5.81 ng/mL) and low MMP-14 (< 5.81 ng/mL), and between patients with and without CVD.
Variables with P values < 0.10 were included in the further analyses and crude odds ratios (CORs) were calculated. Variables with P values < 0.10 for the CORs were included in multiple logistic regression analyses (Backward: Wald) with high MMP-14 (one model) and CVD (three models) as dependent variables. In the first model, only baseline variables were included. In the second model, variables with P values < 0.10 in model 1 and MMP-14 used as a continuous variable were included. In the third model, continuous MMP-14 was exchanged by high MMP-14, otherwise the variables were the same as in model 2. The Hosmer and Lemeshow test for goodness-of-fit and Nagelkerke R2 were used to evaluate each multiple logistic regression analysis model. The area under the receiver operating characteristics curve (AUC of ROC) was performed for MMP-14 tried against CVD, in order to establish a cut-off value for MMP-14, based on the combined optimal sensitivity and specificity. To evaluate the statistical power, a post-hoc calculation was performed for high MMP-14 and CVD and showed a power of 79.7%: the result was calculated using the following data: group 1, 7 patients had CVD and the prevalence of high MMP-14 was 71%; group 2, 261 patients did not have CVD and the prevalence of high MMP-14 was 24% [30]. P values < 0.05 were considered statistically significant. SPSS® version 25 (IBM, Chicago, Il, USA) was used.
Results
In the study 268 patients with T1D (aged 18–59 years, 58% men) participated. Nine percent used CSII and 91% used MDII.
The AUC (CI 95%) for MMP-14 tried against CVD was 0.75 (0.55–0.95), p = 0.023, and the cut-off value MMP-14 ≥ 5.81 ng/mL corresponded to a sensitivity of 0.71 and specificity of 0.70. MMP-14 ≥ 5.81 ng/mL corresponded to the 75th percentile.
In Table 1, baseline characteristics are compared between patients with and without high levels of MMP-14 (≥ 5.81 ng/mL), and between patients with and without CVD. The 67 patients with high MMP-14, compared to the 201 patients with low MMP-14, had a higher prevalence of a CVD (p = 0.012). The 7 T1D patients with CVD, compared to the 261 patients without CVD, were older (p = 0.001), had longer diabetes duration (p = 0.027), and had higher prevalence of abdominal obesity (p = 0.014), depression (p = 0.022), and use of antihypertensive drugs (p = 0.037), statins (p = 0.049), and antidepressants (p = 0.008).
In Table 2, the results of all biochemical analyses are compared between patients with and without high levels of MMP-14, and between patients with and without CVD. The patients with high MMP-14 levels had higher levels of MMP-2 (p = 0.018) and galectin-3 (p < 0.001). The patients with CVD had higher median levels of MMP-14 (p = 0.020) and TIMP-2 (p = 0.028). The prevalence of high MMP-14 was three times higher in patients with CVD compared to patients without CVD (71% versus 24%, p = 0.012).
In Table 3, associations with high MMP-14 are presented. CVD (adjusted odds ratio (AOR) 8.1, p = 0.027), MMP-2 (per ng/mL) (AOR 1.01, p = 0.044), and galectin-3 (per ng/mL) (AOR 2.19, p < 0.001) were associated with high MMP-14 levels.
In Table 4, associations with CVD are presented for three models. In model 1, diabetes duration (AOR 1.10, p = 0.016) and abdominal obesity (AOR 10.2, p = 0.011) were associated with CVD. In model 2, diabetes duration (AOR 1.13, p = 0.008), abdominal obesity (24.5, p = 0.004), depression (AOR 22.1, p = 0.006), and MMP-14 (per ng/mL) (AOR 1.01, p = 0.005), were associated with CVD. In model 3, diabetes duration (AOR 1.10, p = 0.012), abdominal obesity (15.8, p = 0.006), depression (AOR 17.4, p = 0.006), and high MMP-14 (AOR 14.2, p = 0.008), were associated with CVD.
Discussion
The primary findings of this study of 268 adult patients with T1D were that galectin-3, CVD and MMP-2 were independently associated with high levels of MMP-14 (≥ 5.81 ng/mL). Second, depression, abdominal obesity, high MMP-14, and diabetes duration, were independently associated with CVD (Fig. 1).

Illustration of the associations with high MMP-14 and CVD which were found in the study
High levels of MMP-14 were associated with CVD, which is in line with previous research showing that MMP-14 is involved in the development of atherosclerosis with consequent cardiovascular disease [7, 13, 14, 16]. The demonstrated association between MMP-14 and MMP-2 is important as MMP-14 together with TIMP-2 enables the activation of pro-MMP-2 [15]. According to previous research, activated MMP-2 is another contributor to the development of CVD [12, 19], and increased MMP-2 levels have been demonstrated in patients with T1D [18]. Galectin-3, previously likewise linked to CVD [21], was associated with MMP-14, which to our knowledge is a new finding. Galectin-3 was previously linked to MMP-2 [20]. The strength of the association between high levels of MMP-14 and CVD was similar to the strengths of the associations between abdominal obesity, depression and CVD. Abdominal obesity is since long a well-established risk factor for atherosclerosis, coronary artery disease, stroke, and heart failure [6, 31]. The awareness of depression as a risk factor for CVD disease and mortality is lower, but clearly demonstrated in previous research [3].
To explore biomarkers is important for several reasons. First, identification of substances involved in the development of disease may lead to the development of new therapeutics [7]. In addition, biomarkers may be used for diagnosing CVD or evaluation of CVD risk [9, 32]. None of the traditional risk factors for CVD such as low grade inflammation (increased CRP), increased HbA1c, dyslipidaemia, increased blood pressure, physical inactivity, smoking, or the less established risk factor—depression, was associated with MMP-14 [1,2,3, 5]. The lack of associations between MMP-14 and the traditional risk factors makes MMP-14 a potentially interesting addition to traditional risk assessments.
Strengths of our study are that patients with severe comorbidities such as cancer, severe autoimmune disorders, hepatic failure, end-stage renal disease, psychotic and bipolar disorders were excluded as these disorders, or medication for these disorders, may have impact on the immune system including MMPs and galectin-3 [7, 33]. We explored and adjusted for relevant variables previously linked to CVD: MMP-2, MMP-9, MMP-14, TIMPS, galectin-3, CRP, metabolic variables, life style variables, depression, and thyroid disease [2, 3, 7,8,9, 11,12,13,14, 16, 17, 19, 21,22,23, 34,35,36]. The logistic regression models were elaborated for the associations, and calibrated and validated for goodness of fit with the data variables. By using a cut-off value for MMP-14, the problem with the very low and therefore unmeasurable MMP-14 levels was eliminated. Finally, precise ELISA techniques were used and the analyses showed low intra-assay coefficients of variation for all included plasma biomarkers.
Causality cannot be confirmed due to the cross-sectional design, which is a limitation. Another limitation was the restricted number of patients with CVD. The low prevalence of CVD was most likely due both to the exclusion of patients with end-stage renal disease [4], and the exclusion of patients with cognitive deficiencies induced by stroke or other causes of dementia. Despite the limited number of patients with CVD, the AUC was significant for MMP-14 tried against CVD. The post-hoc analyses of the power for the association between high MMP-14 and CVD was acceptable. However, the large CI intervals for high MMP-14 in the multiple logistic regression analyses adds uncertainty to the results, and shows that the results have to be tried and confirmed in a larger population of T1D patients with CVD. Due to the large CI intervals, continuous MMP-14 was tried against CVD which showed clear significance without broad CI intervals. A third limitation was that we did not identify patients suffering from peripheral artery disease. We cannot exclude that the levels of MMP-14 are influenced by the presence of a potential peripheral artery disease. A fourth limitation was that depression was only assessed by a self-report instrument, not by a structured interview. HADS has, however, shown high validity for assessing symptoms of depression both at an individual and a collective level in previous research [25]. Fifth, the levels of physical activity were not objectively measured, but data collected and categorized as in the S-NDR has shown strong associations between low physical activity and CVD [28]. Sixth, we have no information regarding dietary habits.
In future research we suggest evaluation of MMP-14 as a risk marker in larger and longitudinal studies in addition to conventional risk factors for CVD, and potentially in addition to other new biomarkers of CVD [32]. We also suggest further exploration of causes and mechanisms of the demonstrated association between MMP-14 and galectin-3.
Conclusions
The main findings of this study of 268 patients with T1D were that galecin-3, MMP-2, and CVD were independently associated with high levels of MMP-14. The association between MMP-14 and galectin-3 is a new finding. No traditional risk factors for CVD in T1D patients were associated with MMP-14. Depression, abdominal obesity and high MMP-14 levels were independently and to an almost equal degree associated with CVD.
Availability of data and materials
The data set analyzed during the current study is not available publicly as individual privacy could be compromised, and we have no permission from the Regional Ethical Board to share the research data publicly. The data set is stored at the department for Research and Development, Region Kronoberg, Växjö, Sweden, and is available from the corresponding author on reasonable request.
Abbreviations
- AOR:
-
Adjusted odds ratio
- AUC:
-
Area under the curve
- BMI:
-
Body mass index
- COR:
-
Crude odds ratio
- ELISA:
-
Enzyme linked immunosorbent assays
- HADS-D:
-
Hospital anxiety and depression scale-depression subscale
- HbA1c:
-
Hemoglobin A1c
- HDL-cholesterol:
-
High-density lipoprotein cholesterol
- LAS:
-
Left anterior descending artery stenosis
- LDL-cholesterol:
-
Low-density lipoprotein cholesterol
- MMP:
-
Matrix metalloproteinase
- ROC:
-
Receiver operating characteristics curve
- TIMP:
-
Tissue inhibitors of metalloproteinases
- T1D:
-
Type 1 diabetes
- TIA:
-
Transient ischemic attack
- WC:
-
Waist circumference
References
Rawshani A, Sattar N, Franzén S, Rawshani A, Hattersley AT, Svensson A-M, et al. Excess mortality and cardiovascular disease in young adults with type 1 diabetes in relation to age at onset: a nationwide, register-based cohort study. Lancet. 2018;392:477–86.
De Ferranti SD, De Boer IH, Fonseca V, Fox CS, Golden SH, Lavie CJ, et al. Type 1 diabetes mellitus and cardiovascular disease: a scientific statement from the American Heart Association and American Diabetes Association. Circulation. 2014;130:1110–30.
Egede LE, Nietert PJ, Zheng D. Depression and all-cause and coronary heart disease mortality among adults with and without diabetes. Diabetes Care. 2005;28:1339–45.
Ravarotto V, Simioni F, Pagnin E, Davis PA, Calò LA. Oxidative stress—chronic kidney disease—cardiovascular disease: a vicious circle. Life Sci. 2018;210:125–31.
Lind M, Svensson A-M, Kosiborod M, Gudbjörnsdottir S, Pivodic A, Wedel H, et al. Glycemic control and excess mortality in type 1 diabetes. N Engl J Med. 2014;371:1972–82.
Powell-Wiley TM, Poirier P, Burke LE, Després J-P, Gordon-Larsen P, Lavie CJ, et al. Obesity and cardiovascular disease: a scientific statement from the American Heart Association. Circulation. 2021;143:e984-1010.
Raeeszadeh-Sarmazdeh M, Do LD, Hritz BG. Metalloproteinases and their inhibitors: potential for the development of new therapeutics. Cells. 2020;9:1313.
Newby AC. Metalloproteinase expression in monocytes and macrophages and its relationship to atherosclerotic plaque instability. Arterioscler Thromb Vasc Biol. 2008;28:2108–14.
Liu P, Sun M, Sader S. Matrix metalloproteinases in cardiovascular disease. Can J Cardiol. 2006;22:25B-30B.
Nagase H, Visse R, Murphy G. Structure and function of matrix metalloproteinases and TIMPs. Cardiovasc Res. 2006;69:562–73.
Di Gregoli K, Johnson JL. Role of matrix metalloproteinases in the development and progression of atherosclerosis. In: Proteases in human diseases. Singapore: Springer; 2017. p. 425–46.
Peeters S, Engelen L, Buijs J, Jorsal A, Parving H-H, Tarnow L, et al. Plasma matrix metalloproteinases are associated with incident cardiovascular disease and all-cause mortality in patients with type 1 diabetes: a 12-year follow-up study. Cardiovasc Diabetol. 2017;16:55.
Rajavashisth TB, Xu X-P, Jovinge S, Meisel S, Xu X-O, Chai N-N, et al. Membrane type 1 matrix metalloproteinase expression in human atherosclerotic plaques: evidence for activation by proinflammatory mediators. Circulation. 1999;99:3103–9.
Newby AC. Metalloproteinase production from macrophages—a perfect storm leading to atherosclerotic plaque rupture and myocardial infarction. Exp Physiol. 2016;101:1327–37.
Itoh Y, Seiki M. MT1-MMP: a potent modifier of pericellular microenvironment. J Cell Physiol. 2006;206:1–8.
DeLeon-Pennell KY, Meschiari CA, Jung M, Lindsey ML. Matrix metalloproteinases in myocardial infarction and heart failure. Prog Mol Biol Transl Sci. 2017;147:75–100.
Xie Y-T, Dang Y, Zhang F-F, Zhang Q-H, Wu H-B, Liu G. Combination of serum TIMP-3, CA125, and NT-proBNP in predicting ventricular remodeling in patients with heart failure following acute myocardial infarction. Cardiovasc Diagn Ther. 2020;10:1184.
Thrailkill KM, Bunn RC, Moreau CS, Cockrell GE, Simpson PM, Coleman HN, et al. MMP-2 dysregulation in type 1 diabetes mellitus. Diabetes Care. 2007. https://doi.org/10.2337/dc07-0162.
Rempe RG, Hartz AM, Bauer B. Matrix metalloproteinases in the brain and blood–brain barrier: versatile breakers and makers. J Cereb Blood Flow Metab. 2016;36:1481–507.
Lin Y-H, Lin L-Y, Wu Y-W, Chien K-L, Lee C-M, Hsu R-B, et al. The relationship between serum galectin-3 and serum markers of cardiac extracellular matrix turnover in heart failure patients. Clin Chim Acta. 2009;409:96–9.
Suthahar N, Meijers WC, Silljé HHW, Ho JE, Liu F-T, de Boer RA. Galectin-3 activation and inhibition in heart failure and cardiovascular disease: an update. Theranostics. 2018;8:593–609. https://doi.org/10.7150/thno.22196.
Tanindi A, Sahinarslan A, Elbeg S, Cemri M. Relationship between MMP-1, MMP-9, TIMP-1, IL-6 and risk factors, clinical presentation, extent and severity of atherosclerotic coronary artery disease. Open Cardiovasc Med J. 2011;5:110.
Morishita T, Uzui H, Mitsuke Y, Amaya N, Kaseno K, Ishida K, et al. Association between matrix metalloproteinase-9 and worsening heart failure events in patients with chronic heart failure. ESC Heart Fail. 2017;4:321–30.
Ayuk SM, Abrahamse H, Houreld NN. The role of matrix metalloproteinases in diabetic wound healing in relation to photobiomodulation. J Diabetes Res. 2016. https://doi.org/10.1155/2016/2897656.
Bocéréan C, Dupret E. A validation study of the Hospital Anxiety and Depression Scale (HADS) in a large sample of French employees. BMC Psychiatry. 2014;14:1–11. https://doi.org/10.1186/s12888-014-0354-0.
Melin EO, Dereke J, Thunander M, Hillman M. Depression in type 1 diabetes was associated with high levels of circulating galectin-3. Endocr Connect. 2018;7:819–28.
Melin EO, Thunander M, Svensson R, Landin-Olsson M, Thulesius HO. Depression, obesity and smoking were independently associated with inadequate glycemic control in patients with type 1 diabetes. Eur J Endocrinol Eur Fed Endocr Soc. 2013;168:861–9.
Zethelius B, Gudbjörnsdottir S, Eliasson B, Eeg-Olofsson K, Cederholm J. Level of physical activity associated with risk of cardiovascular diseases and mortality in patients with type-2 diabetes: report from the Swedish National Diabetes Register. Eur J Prev Cardiol. 2014;21:244–51.
The National Board of Health and Welfare. Swedish national guidelines for diabetes. https://www.socialstyrelsen.se/nationellariktlinjerfordiabetesvard. Accessed 23 March 2009.
Kane SP. Post-hoc power calculator. https://clincalc.com/stats/Power.aspx. Accessed 8 Sep 2021.
Lavie CJ, Milani RV, Ventura HO. Obesity and cardiovascular disease: risk factor, paradox, and impact of weight loss. J Am Coll Cardiol. 2009;53:1925–32.
Hoogeveen RM, Pereira JPB, Nurmohamed NS, Zampoleri V, Bom MJ, Baragetti A, et al. Improved cardiovascular risk prediction using targeted plasma proteomics in primary prevention. Eur Heart J. 2020;41:3998–4007. https://doi.org/10.1093/eurheartj/ehaa648.
Newlaczyl AU, Yu L-G. Galectin-3—a jack-of-all-trades in cancer. Cancer Lett. 2011;313:123–8.
Elmore JR, Keister BF, Franklin DP, Youkey JR, Carey DJ. Expression of matrix metalloproteinases and TIMPs in human abdominal aortic aneurysms. Ann Vasc Surg. 1998;12:221–8.
Wang A, Liu J, Li C, Gao J, Li X, Chen S, et al. Cumulative exposure to high-sensitivity C-reactive protein predicts the risk of cardiovascular disease. J Am Heart Assoc. 2017;6:e005610.
Jabbar A, Pingitore A, Pearce SH, Zaman A, Iervasi G, Razvi S. Thyroid hormones and cardiovascular disease. Nat Rev Cardiol. 2017;14:39–55.
Acknowledgements
The authors are grateful to Anna Lindgren, PhD at the Department of Mathematical Statistics, Lund University, Lund, Sweden, for her statistical skills.
Funding
This research was supported by the Research and Development Fund of Region Kronoberg, Växjö, Sweden, and by the Research Council of South Eastern Sweden (FORSS), Linköping, Sweden, and the Southern Healthcare Region, Lund, Sweden. The funding sources were not involved in the collection, analysis and interpretation of data, in the writing of the report, or in the decision to submit the article for publication.
Author information
Authors and Affiliations
Contributions
EOM, JD and MH participated as investigators and reviewed, edited and approved the final version of the manuscript. EOM initiated the study of depression and CVD in patients with T1D, performed the statistical analysis, is the guarantor of this work and, as such, had full access to all the data in the study, and takes responsibility for the integrity of the data and the accuracy of the data analysis. JD and MH contributed with their knowledge of immunology, proposed relevant biomarkers, performed the ELISA analyses, and they take the full responsibility for these analyses. All authors read and approved the final manuscript.
Authors’ information
EOM is MD and PhD and works at the department for Research and Development, Region Kronoberg, Växjö, Sweden, and is affiliated to the Diabetes Research Laboratory, Lund University, Lund, Sweden. MH is Associate Professor and works at the Diabetes Research Laboratory. JD is PhD and worked until recently at the Diabetes Research Laboratory.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Regional Ethical Review Board of Linköping University, Linköping (Registration no. M120-07, T89-08). All participants provided written informed consent.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Melin, E.O., Dereke, J. & Hillman, M. Galectin-3, metalloproteinase-2 and cardiovascular disease were independently associated with metalloproteinase-14 in patients with type 1 diabetes: a cross sectional study. Diabetol Metab Syndr 13, 118 (2021). https://doi.org/10.1186/s13098-021-00727-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13098-021-00727-3