
Abstract
Background
Waist circumference (WC) has been incorporated in the definition of the metabolic syndrome (MetS) but the exact WC cut-off points across populations are not clear. The Joint Interim Statement (JIS) suggested possible cut-offs to different populations and ethnic groups. However, the adequacy of these cut-offs to Brazilian adults has been scarcely investigated. The objective of the study is to evaluate possible WC thresholds to be used in the definition of MetS using data from the Longitudinal Study of Adult Health (ELSA-Brasil), a multicenter cohort study of civil servants (35–74 years old) of six Brazilian cities.
Methods
We analyzed baseline data from 14,893 participants (6772 men and 8121 women). A MetS was defined according to the JIS criteria, but excluding WC and thus requiring 2 of the 4 remaining elements. We used restricted cubic spline regression to graph the relationship between WC and MetS. We identified optimal cut-off points which maximized joint sensitivity and specificity (Youden’s index) from Receiver Operator Characteristic Curves. We also estimated the C-statistics using logistic regression.
Results
We found no apparent threshold for WC in restricted cubic spline plots. Optimal cut-off for men was 92 cm (2 cm lower than that recommended by JIS for Caucasian/Europids or Sub-Saharan African men), but 2 cm higher than that recommended for ethnic Central and South American. For women, optimal cut-off was 86, 6 cm higher than that recommended for Caucasian/Europids and ethnic Central and South American. Optimal cut-offs did not very across age groups and most common race/color categories (except for Asian men, 87 cm).
Conclusions
Sex-specific cut-offs for WC recommended by JIS differ from optimal cut-offs we found for adult men and women of Brazil´s most common ethnic groups.
Similar content being viewed by others


Background
The metabolic syndrome (MetS), a multiplex risk factor for atherosclerotic cardiovascular disease and type 2 diabetes mellitus [1], is now common throughout the world [2]. Observed in clinical practice for decades, the MetS is now recognized as having public health importance, most probably due to the growing global prevalence of obesity [3].
The inclusion of waist circumference (WC) in the definition of MetS is now supported by major bodies, although a single cut-off point for international use is not possible owed to its wide variation across populations [4]. This led the International Diabetes Federation [5] to propose population-specific thresholds for WC, a position which was endorsed by the World Health Organization [6]. The Joint Interim Statement (JIS) suggested WC cut-offs for different ethnic groups based on the literature and consensus [7].
Given the ethnic diversity and admixture of the Brazilian population, the application of WC cut-offs recommended by JIS is not straightforward. Specifically, whether values recommended for white Caucasians/Europids or black Sub-Saharan Africans (≥ 94 cm for men and ≥ 80 cm for women) are applicable to similar Brazilian adults is questionable. Additionally, cut-offs referred for ethnic Central and South American ethnic groups (≥ 90 cm for men and ≥ 80 cm for women) are unlikely to be useful to the specific Brazilian ethnic groups.
Thus, adequacy of optimal WC cut-off to define MetS needs further evaluation in Brazil. The Brazilian Longitudinal Study of Adult Health (ELSA-Brasil) permits such analyses in a large number of men and women of a broad age range (35–74 years), of different ethnic groups, living and working in different cities of Brazil. The aim of this cross-sectional study is to evaluate possible cut-off points for WC for men and women against the presence of MetS. We will also explore the application of these values for different age and ethnic groups.
Methods
ELSA-Brasil is a cohort study of 15,105 civil servants aged 35–74 years, enrolled at six universities or research institutes located in three different regions of Brazil: the Federal Universities of Bahia, Espirito Santo, Minas Gerais, and Rio Grande do Sul; the University of São Paulo; and the Oswaldo Cruz Foundation. A detailed protocol for the Study can be found else where [8, 9]. Study approval was obtained from the institutional review boards of all the centers, and all subjects signed an informed consent form.
We used baseline data after performing the following 212 exclusions: three participants who did not have complete data on WC, 174 on self-declared race/colour, and 35 on other information needed do define the MetS. The final sample was composed of 14,893 participants (6772 men and 8121 women).
After an overnight fast of 12 h we performed anthropometric and blood pressure measurements according to standard protocols [10,11,12], and then collected venous blood.
WC was measured using an inelastic tape of 150 cm (Mabis-Gulick, Waukegan, IL, USA) at the midpoint between the lowest rib margin and the iliac crest. The intra-class correlation coefficient for repeat measurements was 0.98 (95% CI 0.85–1.0) [11]. We measured height to the nearest 0.1 cm (Seca-SE-216, Hamburg, Germany). We measured body weight with an electronic scale with maximum capacity of 200 kg (Toledo, São Bernardo do Campo, Brazil). Body mass index (BMI) was calculated by dividing weight (kg) per height squared (m2).
Blood pressure was taken using an oscillometric device (Omron HEM 705CPINT) after a 5-min rest with the subject in a sitting position in a quiet, temperature-controlled room (20–24 °C). Three measurements were taken at 2-min intervals and the mean of the last two was used for these analyses. Intra-class correlation coefficients for systolic and diastolic blood pressure were 0.88 (95% CI 0.82–0.91) and 0.89 (95% CI 0.83–0.92), respectively [11].
We determined plasma glucose enzymatically by the hexokinase method (ADVIA Chemistry; Siemens, Deerfield, Illinois). High-density lipoprotein cholesterol (HDL-C), and triglycerides were determined by the enzymatic colorimetric method (ADVIA Química) [13]. Blinded quality control analyses revealed intra-class correlation coefficients for glucose, HDL-C and triglycerides of 0.99 (95% CI 0.95–1.00), 0.97 (95% CI 0.95–0.98) and 1.0 (95% CI 0.99–1.00), respectively [14].
We defined components of MetS according to JIS [7]: elevated systolic blood pressure (≥ 130 mmHg) or diastolic blood pressure (≥ 85 mmHg) or use of antihypertensive medication; high triglycerides as ≥ 150 mg/dL or use of lipid-lowering agents (fibrate and nicotinic acid); low HDL-C as < 40 mg/dL for men and < 50 mg/dL for women, or use of specific medication (fibrate and nicotinic acid); high fasting plasma glucose as ≥ 100 mg/dL or use of antidiabetic medication; WC as population-specific cut-offs. For the analyses here reported, we excluded WC from the definition of MetS, which then was defined as requiring the presence of at least two out of four components.
Sociodemographic variables were obtained by structured interviews while participants remained at the clinic center and included age, gender, education level, self-declared race. Medication use was verified against prescription, package or package inserts.
The relationship between WC and MetS was initially investigated with logistic regression using restricted cubic splines. Four “knots” were positioned in percentiles 10, 25, 75 and 90 of the empirical distribution of WC. The polynomial expansions were created by macros DASPLINE and DSHIDE (developed by Frank E Harrell Jr) for SAS (Statistical Analysis System). To test the linearity of the relationship between WC and the logit of the probability of having MetS we used the Wald statistics. The model included terms for age, sex and for the interaction between WC and sex. We used the value defining the first quartile of the sex-specific WC distribution as a reference for the estimation of odds ratios.
The probability that a randomly chosen subject with the MetS is more likely to be rated as such than a randomly chosen subject without the MetS was estimated by the total area under the curve (AUC) and its respective 95% confidence intervals using Receiver Operator Characteristics (ROC) [15] in logistic regression (SPSS—Statistical Package for the Social Sciences, version 18 for Windows). Optimal values for WC, assuming equal an importance for the sensitivity and specificity of the cut-off point were defined by the Youden index [maximum (sensitivity + specificity − 1)]. We also estimated sensitivity, specificity, positive and negative predictive values, impact on MetS prevalence, and relative increase in the odds of MetS (odds ratio, OR). Significance level was set at 5%. Unless otherwise specified, all analyses were carried out using SAS 9.4 (SAS Institute, Inc., Cary, North Carolina). Given the well-established use of sex-specific thresholds for WC, all analyzes were performed separately for men and women.
Results
Among the 14,893 participants in the ELSA-Brasil, 54.5% (8121) were women. Table 1 shows that, in men and woman, most individuals were between 45 and 64 years (67.3%) and 52.2% declared being white. About 87% had completed at least high school. Around 63% of the participants were overweight (BMI ≥ 25 kg/m2). Prevalence of individual components of MetS when defined by the JIS was higher in men, except for elevated WC (based on JIS cut-offs for Central and South American ethnic groups and white Caucasians/Europids or black Sub-Saharan Africans) and low levels of HDL-C (Table 1).
In curves derived from cubic spline regression models, the logit of the probability of having the MetS (WC not included in the definition) increased continuously with increasing values of WC, although at very high values the rate of increase slowed down (data not shown). We found a similar pattern while plotting WC values against odds ratios for having MetS, taking the value of the first quartile of gender-specific WC distributions (87.5 cm for men and 78.0 cm for women) as a reference group (Fig. 1).

Restricted cubic spline graphical analysis, showing the odds ratios for waist circumference. The dashed line shows odds ratios, and their upper and lower 95% confidence intervals are shown in grey. Reference category for WC was defined by the first quartile value for men (< 87.5 cm) and women (< 78 cm)
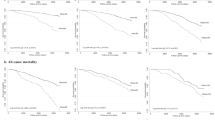
Thus, in the absence of a natural threshold for WC, we explored optimal cut-offs by examining sensitivity and 1-specificity for having MetS in ROC curves across the spectrum of WC (Fig. 2). The total area under the curve (AUC) was 0.719 (95% CI 0.707–0.732) for men, and 0.739 (95% CI 0.729–0.750) for women (Fig. 2a and b). The optimal cut-off of WC for men was 92 cm (Fig. 2a) and for women was 86 cm (Fig. 2b). Also seen in Fig. 2c and d, optimal cut-offs for those under 60 years were close to those for 60 years and over, although among women, a slightly higher cut-off was seen for those over 60 years.

ROC analyses for waist circumference in the definition of MetS by sex and age. Top panel (a and b): overall sample. Lower panels (c, d, e and f): sex/age specific analyses. Area under the curve (AUC)
Optimal cut-offs were also similar across Brazilian ethnic groups (Fig. 3), although a few observations can be made. Among women, we noted a slightly lower optimal cut-off for blacks (84 vs 86 cm for all women). Among men we noted a lower optimal cut-off for Asians (87 vs 92 cm for all men). Our sample size was insufficient to estimate optimal cut-offs the indigenous subjects, the AUC for indigenous men being 0.677 (95% CI 0.561–0.793) and for indigenous women, 0.628 (95% CI 0.484–0.773) (data not shown).

ROC analyses for optimal waist circumference cut-off in the definition of MetS according ethnic groups. Area under the curve (AUC). *Indigenous group not shown because of insufficient sample size. a Men; b women; c men <60 years; d women <60 years; e men >=60 years; f women >=60 years
Table 2 summarizes diagnostic properties for these optimal cut-offs (in italic) and for additional ones considered within a clinically relevant range. As indicated by the odds ratios, these possible cut-offs were associated with increased probability of having the MetS. Of clinical relevance, prevalence of MetS was influenced by the WC cut-off used, varying from 54.1 to 38.4% among men, and from 40.5 to 31.6% among women.
Discussion
In this large sample of Brazilian adults, we did not find a threshold indicative of increased risk for MetS. Optimal (Youden) WC cut-off points were 92 cm for men and 86 cm for women. These cut-offs were associated with increased risk of having MetS of 50% among men and of 93% among women. Optimal cut-offs were similar across age groups and most common Brazilian race/color categories. Among women, optimal cut-offs were higher than those recommended by JIS [7] for white Caucasians/Europids or black Sub-Saharan Africans and Central and South American ethnic groups. Among men, optimal cut-offs were lower than those recommended by JIS [7] for whites and higher for those recommended for blacks and Central and South American ethnic groups.
Optimal cut-off points recommended internationally vary widely. A review of 61 studies [16] found values for men ranging between 72.5 and 103 cm, and for women between 65.5 and 101.2 cm. Values suggested in the literature for the Brazilian adults range between 85 and 99 cm for men, and 80 and 87.5 cm for women [17,18,19,20,21,22,23,24,25,26,27]. Although this variation is largely due to different anthropometric characteristics of various populations, the method for WC measurement and the outcome chosen to validate WC cut-off are also important factors to explain large variation in findings across studies.
Two Brazilian studies using outcomes resembling the MetS found optimal cut-offs closer to those we found. A study conducted in the city of Pelotas, Rio Grande do Sul, using a WC measurement similar to ours and using cardiovascular risk (previous medical diagnosis of hypertension, diabetes mellitus and/or dyslipidemia) as the outcome, found values 95 cm for men, and 87 cm for women [21]. Another study using coronary risk (systolic and diastolic blood pressure, total cholesterol, HDL-C, cigarette smoking and diabetes) conducted in the state of Bahia [26], investigating only women, also found as a result the optimal cut-off point for the WC of 86 cm.
Thus, our findings, supported by these two other Brazilian studies [21, 26], question the application to Brazilian adults, of the cut-offs recommended by JIS define MetS into white, black, Central and South Americans ethnic groups. It is possible that the anthropomorphic characteristics of whites and specific ethnic groups living in Brazil differ from the Caucasians/Europids whites living in Europe, or the blacks of Sub-Saharan Africans and the ethnic groups implied in the JIS report for Central and South America. This might be the case also for Mexican adults, since the cut-offs recommended for men (98 cm) [28] and women (96.6 cm) [29] are much higher than the ones proposed by JIS.
Of note also, when we investigated optimal cut-offs for distinct ethnic groups living in Brazil we did not find important differences, except for those of Asian origin, particularly for men. These findings are in agreement with their generally described lower cut-offs for obesity/central obesity [5, 30,31,32]. The similarity we found for optimal cut-offs for whites, blacks and mixed race/color groups in Brazil contrasts with findings of Zhu et al. [33] based on The Third National Health and Nutrition Examination Survey (NHANES III) for US adults. Although for women they found only small differences in optimal cut-offs across ethnic groups, among men, whites had 5–6 cm higher cut-off points than blacks, and Mexican Americans had intermediate values.
Which values should be used to define an elevated WC has not been established for the Brazilian populations. Our findings do not support the recommendations suggested in the JIS. For example, the cut-off of 80 cm for women had very low specificity (41.9%). Although the definition of an elevated WC as a component of the MetS is challenging [7], we could suggest values for Brazilian adults close to 92 cm for men and 86 cm for women. These values are applicable to whites, blacks, and mixed race-color groups, although for men of Asian origin (mostly of Japanese ancestry) perhaps slightly lower cut-offs could be used, which is consistent with the JIS recommendations. We did not have enough sample size to evaluate cut-offs for indigenous groups living in Brazil. Additionally, within the age range of our study (35–74 years), we did not find WC differences with age suggesting the need to establish specific cut-offs for specific age groups.
Despite the limitations of a cross-sectional study of this nature, our analyses have some strengths. First, measurements of WC and MetS were highly standardized. Second, the sample size for whites, blacks and mixed color groups allowed specific evaluation of the most common ethnic groups in living in Brazil. Third, the wide age range allowed evaluation of cut-offs for adults and the elderly.
We believe that the choice of the Youden Index to define the optimal cut-off point is adequate, as the MetS has been described as a clustering of risk factors. The Youden index detects the cut-off point which identifies maximum sensitivity and specificity of clusters (2 or more) of the other MetS factors being present when suggested by a high WC value and being absent when suggested by a low WC value. As such, it maximizes the correct identification of clusters.
Conclusions
In conclusion, sex-specific cut-offs for WC we found for white and black Brazilian adult men (92 cm) and women (86 cm) are 2 cm lower and 6 cm higher, respectively, than those recommended by JIS. Consistent with the literature, the WC cut-off for Brazilian men of Japanese ancestry was lower. Optimal WC cut-offs identified in ELSA-Brasil can be applied to the definition of MetS for Brazilian adults and the elderly.
Abbreviations
- AUC:
-
area under the curve
- BMI:
-
body mass index
- ELSA-Brasil:
-
The Brazilian Longitudinal Study of Adult Health
- HDL-C:
-
high-density lipoprotein cholesterol
- JIS:
-
Joint Interim Statement
- MetS:
-
metabolic syndrome
- NHANES III:
-
The Third National Health and Nutrition Examination Survey
- OR:
-
odds ratio
- ROC:
-
Receiver Operator Characteristics
- SAS:
-
Statistical Analysis System
- SPSS:
-
Statistical Package for the Social Sciences
- WC:
-
waist circumference
References
Grundy SM. Metabolic syndrome: a multiplex cardiovascular risk factor. J Clin Endocrinol Metab. 2007;92:399–404.
Grundy SM. Metabolic syndrome pandemic. Arterioscler Thromb Vasc Biol. 2008;28:629–36.
NCD Risk Factor Collaboration (NCD-RisC). Trends in adult body-mass index in 200 countries from 1975 to 2014: a pooled analysis of 1698 population-based measurement studies with 19·2 million participants. Lancet. 1975;2016(387):1377–96.
Physical status: the use and interpretation of anthropometry. Report of a WHO Expert Committee. World Health Organization. Technical Report Series No. 854. 1995. p. 1–452.
Alberti KGMM, Zimmet P, Shaw J. Metabolic syndrome—a new world-wide definition. A consensus statement from the international diabetes federation. Diabet Med. 2006;23:469–80.
World Health Organization. WHO STEPwise approach to surveillance (STEPS). Geneva: World Health Organization; 2008.
Alberti KGMM, Eckel RH, Grundy SM, Zimmet PZ, Cleeman JI, Donato KA, et al. Harmonizing the metabolic syndrome: a joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation. 2009;120:1640–5.
Aquino EML, Barreto SM, Bensenor IM, Carvalho MS, Chor D, Duncan BB, et al. Brazilian longitudinal study of adult health (ELSA-Brasil): objectives and design. Am J Epidemiol. 2012;175:315–24.
Schmidt MI, Duncan BB, Mill JG, Lotufo PA, Chor D, Barreto SM, et al. Cohort profile: longitudinal study of adult health (ELSA-Brasil). Int J Epidemiol. 2015;44:68–75.
Bensenor IM, Griep RH, Pinto KA, de Faria CP, Felisbino-Mendes M, Caetano EI, et al. Routines of organization of clinical tests and interviews in the ELSA-Brasil investigation center. Rev Saúde Pública. 2013;47(Suppl 2):37–47.
Schmidt MI, Griep RH, Passos VM, Luft VC, Goulart AC, de Menezes GMS, et al. Strategies and development of quality assurance and control in the ELSA-Brasil. Rev Saúde Pública. 2013;47(Suppl 2):105–12.
Mill JG, Pinto K, Griep RH, Goulart A, Foppa M, Lotufo PA, et al. Medical assessments and measurements in ELSA-Brasil. Rev Saúde Pública. 2013;47(Suppl 2):54–62.
Fedeli LG, Vidigal PG, Leite CM, Castilhos CD, Pimentel RA, Maniero VC, et al. Logistics of collection and transportation of biological samples and the organization of the central laboratory in the ELSA-Brasil. Rev Saúde Pública. 2013;47(Suppl 2):63–71.
Ladwig R, Vigo A, Fedeli LMG, Chambless LE, Bensenor I, Schmidt MI, et al. Variability in baseline laboratory measurements of the Brazilian longitudinal study of adult health (ELSA-Brasil). Braz J Med Biol Res. 2016;49. http://www.scielo.br/scielo.php?script=sci_abstract&pid=S0100-879X2016000900701&lng=en&nrm=iso&tlng=en. Accessed 13 Apr 2017.
Hanley JA, McNeil BJ. The meaning and use of the area under a receiver operating characteristic (ROC) curve. Radiology. 1982;143:29–36.
Wang Z, Ma J, Si D. Optimal cut-off values and population means of waist circumference in different populations. Nutr Res Rev. 2010;23:191–9.
Barbosa PJB, Lessa Í, Filho A, De N, Magalhães LBNC, Araújo J. Critério de obesidade central em população brasileira: impacto sobre a síndrome metabólica. Arq Bras Cardiol. 2006;87:407–14.
Ferreira MG, Valente JG, Gonçalves-Silva RMV, Sichieri R. Accuracy of waist circumference and waist-to-hip ratio as predictors of dyslipidemia in a cross-sectional study among blood donors in Cuiabá, Mato Grosso State, Brazil. Cad Saúde Pública. 2006;22:307–14.
Peixoto MDRG, Benício MHD, Latorre MDRDD, Jardim PCBV. Waist circumference and body mass index as predictors of hypertension. Arq Bras Cardiol. 2006;87:462–70.
Picon PX, Leitão CB, Gerchman F, de Azevedo MJ, Silveiro SP, Gross JL, et al. Medida da cintura e razão cintura/quadril e identificação de situações de risco cardiovascular: estudo multicêntrico em pacientes com diabetes melito tipo 2. Arq Bras Endocrinol Amp Metabol. 2007;51:443–9.
de Almeida RT, de Almeida MMG, Araújo TM. Abdominal obesity and cardiovascular risk: performance of anthropometric indexes in women. Arq Bras Cardiol. 2009;92:375–80.
Gus M, Cichelero FT, Moreira CM, Escobar GF, Moreira LB, Wiehe M, et al. Waist circumference cut-off values to predict the incidence of hypertension: an estimation from a Brazilian population-based cohort. Nutr Metab Cardiovasc Dis NMCD. 2009;19:15–9.
Matos LN, de Giorelli GV, Dias CB. Correlation of anthropometric indicators for identifying insulin sensitivity and resistance. Sao Paulo Med J. 2011;129:30–5.
Gouveia L, de Marucci MFN, Lebrão ML, Duarte YAO. Association between waist circumference (WC) values and hypertension, heart disease (HD) and diabetes, reported by the elderly—SABE survey: health, wellness and aging, 2000 and 2006. Arch Gerontol Geriatr. 2014;59:62–8.
de Oliveira A, Cocate PG, Hermsdorff HHM, Bressan J, de Silva MF, Rodrigues JA, et al. Waist circumference measures: cutoff analyses to detect obesity and cardiometabolic risk factors in a Southeast Brazilian middle-aged men population—a cross-sectional study. Lipids Health Dis. 2014;13:141.
Vianna CA, da Silva Linhares R, Bielemann RM, Machado EC, González-Chica DA, Matijasevich AM, et al. Accuracy and adequacy of waist circumference cut-off points currently recommended in Brazilian adults. Public Health Nutr. 2014;17:861–9.
Rodrigues SL, Baldo MP, Mill JG. Associação entre a razão cintura-estatura e hipertensão e síndrome metabólica: estudo de base populacional. Arq Bras Cardiol. 2010;95:186–91.
Alonso AL, Munguía-Miranda C, Ramos-Ponce D, Hernandez-Saavedra D, Kumate J, Cruz M. Waist perimeter cutoff points and prediction of metabolic syndrome risk. A study in a Mexican population. Arch Med Res. 2008;39:346–51.
Sánchez-Castillo CP, Velázquez-Monroy O, Berber A, Lara-Esqueda A, Tapia-Conyer R, James WPT, et al. Anthropometric cutoff points for predicting chronic diseases in the Mexican National Health Survey 2000. Obes Res. 2003;11:442–51.
Hara K, Matsushita Y, Horikoshi M, Yoshiike N, Yokoyama T, Tanaka H, et al. A proposal for the cutoff point of waist circumference for the diagnosis of metabolic syndrome in the Japanese population. Diabetes Care. 2006;29:1123–4.
Ogawa D, Kahara K, Shigematsu T, Fujii S, Hayakawa N, Okazaki M, et al. Optimal cut-off point of waist circumference for the diagnosis of metabolic syndrome in Japanese subjects. J Diabetes Invest. 2010;1:117–20.
Fu S, Luo L, Ye P, Liu Y, Zhu B, Bai Y, et al. The abilities of new anthropometric indices in identifying cardiometabolic abnormalities, and influence of residence area and lifestyle on these anthropometric indices in a Chinese community-dwelling population. Clin Interv Aging. 2014;9:179–89.
Zhu S, Heymsfield SB, Toyoshima H, Wang Z, Pietrobelli A, Heshka S. Race-ethnicity-specific waist circumference cutoffs for identifying cardiovascular disease risk factors. Am J Clin Nutr. 2005;81:409–15.
Authors’ contributions
TRC: Conceived this study, analyzed and interpreted data, and wrote the manuscript. AV: Conceived this study, analyzed and interpreted data, and revised the manuscript. MIS: Conceived this study, interpreted data and revised the manuscript. BBD, SMAM, MJMF and SMB: Conceived this study, interpreted data and revised the manuscript. All authors read and approved the final manuscript.
Acknowledgements
Ministério de Ciência e Tecnologia (FINEP- Financiadora de Estudos e Projetos e CNPq), Ministério da Saúde (DECIT- Departamento de Ciência e Tecnologia) (nº 01 06 0010.00 RS, 01 06 0212.00 BA, 01 06 0300.00 ES, 01 06 0278.00 MG, 01 06 0115.00 SP, 01 06 0071.00 RJ). Doctoral scholarship from CAPES and a Post Doctoral scholarship from CNPq (INCT IATS—Proces 88887.145232/2017-00).
Competing interests
The authors declare that they have no competing interests.
Availability of data and materials
The data sets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics approval and consent to participate
Study approval was obtained from the institutional review boards of all centers (IRB0000921, project ELSA-RS 06-194), and all subjects signed informed consent.
Funding
Ministério de Ciência e Tecnologia (FINEP-Financiadora de Estudos e Projetos e CNPq), Ministério da Saúde (DECIT-Departamento de Ciência e Tecnologia) (nº 01 06 0010.00 RS, 01 06 0212.00 BA, 01 06 0300.00 ES, 01 06 0278.00 MG, 01 06 0115.00 SP, 01 06 0071.00 RJ). Doctoral scholarship from CAPES and a Post Doctoral scholarship from CNPq (INCT IATS—Proces 88887.145232/2017-00).
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Cardinal, T.R., Vigo, A., Duncan, B.B. et al. Optimal cut-off points for waist circumference in the definition of metabolic syndrome in Brazilian adults: baseline analyses of the Longitudinal Study of Adult Health (ELSA-Brasil). Diabetol Metab Syndr 10, 49 (2018). https://doi.org/10.1186/s13098-018-0347-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13098-018-0347-0