
Abstract
Background
Pulmonary arterial hypertension (PAH) and interstitial lung disease (ILD) are leading causes of systemic sclerosis (SSc)-related death. In this study, we aimed to identify biomarkers for detecting SSc pulmonary complications that are mild and in the early stages to improve the prognosis.
Methods
We screened for serum biomarkers using a proteomic antibody microarray that simultaneously assessed 1000 proteins. Differentially expressed proteins were further verified using ELISA. Finally, we performed a correlation analysis using clinical data.
Results
We identified 125 differentially expressed proteins, of which calcitonin, sclerostin (SOST), CD40, and fibronectin were selected for further verification. Serum calcitonin and SOST levels were significantly elevated in all SSc pulmonary complication subgroups, whereas serum calcitonin levels were higher in the SSc with PAH subgroup than in the SSc without PAH and ILD subgroup. Serum SOST levels were possibly associated with the presence of ILD and positively related to the presence of cardiac and gastrointestinal involvement. Serum CD40 and calcitonin levels appeared to be positively related to the presence of renal involvement, and serum calcitonin was also positively related to the presence of gastrointestinal involvement.
Conclusions
This study indicated that serum calcitonin and SOST levels may be promising biomarkers for SSc-related PAH and ILD, respectively. Further research is needed to verify this result and understand the underlying mechanisms.
Similar content being viewed by others


Background
Systemic sclerosis (SSc) is a multi-organ involved autoimmune disease with one of the highest mortality rates among connective tissue diseases [1]. Pulmonary arterial hypertension (PAH) and interstitial lung disease (ILD) remain the leading causes of SSc-related deaths, representing 30–40% of mortalities [2,3,4,5]. High mortality rates are largely due to the lack of specific treatments for end-stage tissue fibrosis [1]. Therefore, early diagnosis and treatment may improve outcomes in patients with SSc, especially those with pulmonary complications (including PAH and ILD). We aimed to identify early biomarkers of pulmonary complications in patients with SSc to detect pulmonary complications in its mild form or at an early stage.
Proteomic antibody microarrays allow the simultaneous analysis of many proteins in patient serum samples. In this study, we performed a proteomic chip-based analysis to identify differentially expressed serum proteins among 1000 proteins in patients with SSc and PAH or ILD. Finally, we identified 125 differentially expressed proteins (DEPs), of which calcitonin and sclerostin (SOST) levels were confirmed to be differentially expressed by further verification. These proteins may be promising early biomarkers for SSc and pulmonary complications in patients with SSc.
Methods
Study population and samples
This study was approved by the Medical Ethics Committee of Peking Union Medical College Hospital (PUMCH) and the Ethics Committee of the European League Against Rheumatism Scleroderma Trial and Research Group (EUSTAR). Patients with SSc included in this study received a first and confirmed diagnosis at PUMCH between 2009 and 2016 and were prospectively registered in the EUSTAR database. The patients fulfilled the 1980 American Rheumatism Association classification criteria for SSc. All participants (patients with SSc and healthy controls [HCs]) provided informed consent, and their serum samples at baseline were collected and stored at − 80 °C.
Proteomic antibody microarray
The antibody array (RayBio® L-Series human antibody array 1000 kit; RayBiotech, Norcross, GA, USA) assessed the serum expression levels of 1000 proteins, following the manufacturer’s instructions. The GenePix 4000B microarray scanner (Molecular Devices, LLC; 1311 Orleans Drive Sunnyvale, CA, USA) captured and quantified the signals. We calculated spot intensities by subtracting the background and normalizing the data to the positive controls on individual slides. Independent-sample t-test and fold change values were used to determine the DEPs between each SSc subgroup and the HC group. DEPs were confirmed by a p-value below 0.05, and a fold change over 1.2 (upregulated) or under 0.8 (downregulated).
Bioinformatics analysis
We used the R package clusterProfiler to analyze the DEPs in each SSc subgroup. In the Gene Ontology (GO) functional analysis, we displayed the top 10 enriched biological activities in which these proteins primarily participated for each SSc subgroup.
Evaluation of the serum levels of calcitonin and SOST in additional individuals
Serum calcitonin and SOST levels were measured using Human Calcitonin ELIST Kit (LifeSpan BioSciences Inc.) and Human SOST Immunoassay (R&D Systems), respectively, following the manufacturer’s instructions. The optical density of each well was determined at 450 nm using a microplate reader. The concentration was calculated from the optical density according to the manufacturer’s instructions.
Statistical analysis
All data were processed using the Statistical Package for the Social Sciences version 21.0 (SPSS, Chicago, IL, USA). An independent-sample t-test was used to analyze normally distributed continuous variables. Correlation analysis between serum protein levels and clinical data was performed using Pearson’s correlation analysis (for normally distributed continuous variables of clinical data) and the point biserial correlation test (for classified variables of clinical data). In the correlation analysis, the degree of correlation was higher when the correlation coefficient was close to 1.0 or − 1.0. For all statistical analyses, a two-tailed p-value < 0.05 was considered statistically significant.
Results
Serum protein profiles in patients with SSc with different pulmonary complications
Characteristics of study participants
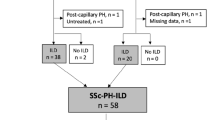
In total, 15 patients with SSc who were not receiving treatment were included in the protein microarray study: in the subgroup of SSc with PAH (n = 5), PAH was defined as a mean pulmonary arterial pressure (mPAP) no less than 25 mmHg and pulmonary arterial wedge pressure (PAWP) no more than 15 mmHg in the right heart catheter, and ILD was excluded by high-resolution computerized tomography (HRCT); in the subgroup of SSc with ILD (n = 5), ILD was diagnosed using HRCT, and PAH was excluded when the tricuspid regurgitation velocity (TRV) was no more than 2.8 m/s on echocardiography; in the subgroup of SSc without PAH and ILD (n = 5), PAH and ILD were respectively excluded by echocardiography and HRCT. Five age- and sex-matched HC volunteers were recruited and their blood samples were donated. Twenty participants were recruited for the antibody microarray study. Detailed information on these participants is provided in Table 1.
Differentially expressed proteins in each SSc subgroup
Serum samples from 15 patients with SSc and five HCs were tested using an antibody microarray (RayBiotech, USA), which detected 1000 proteins (for detailed data, see Additional file 1). In this study, we screened out 125 DEPs from three SSc subgroups (59 DEPs from the SSc with PAH group, 26 DEPs from the SSc with ILD group, and 67 DEPs from the SSc without PAH and ILD group), compared with the HCs (Figs. 1 and 2A). Four specific proteins were selected as possible biomarkers of SSc or associated pulmonary complications for further validation. Because calcitonin and fibronectin were upregulated and downregulated, respectively, in all three SSc subgroups, they were chosen as possible biomarkers for SSc. Thus, CD40 was chosen as a possible biomarker for PAH in SSc because of its unique upregulation in the SSc with PAH group compared with the SSc without PAH and ILD group and HCs. SOST was chosen as a possible biomarker of ILD in SSc because of its unique upregulation in the SSc with the ILD group (Fig. 2B).

Differentially expressed proteins and functional analysis in each SSc subgroup. Comparison of each SSc subgroup (A–C for SSc with PAH group, SSc with ILD group, and SSc without PAH and ILD group successively) with HCs. Volcano plots on the left show differentially expressed proteins with a p-value < 0.05, fold change > 1.2 or < 0.8. The circle diagrams on the right show the top 10 terms based on a p-value < 0.05 in the GO functional analysis

The expression of serum protein profiles in patients with SSc with different pulmonary complications using the high-throughput antibody microarray. A The heatmap of the log2 (fold change) of the 125 differentially expressed proteins in the microarray test. A total of 20 participants were equally divided into four groups, including the SSc with PAH (SSc-PAH), SSc with ILD (SSc-ILD), SSc without PAH and ILD (SSc-nonPAH-nonILD), and HC groups. A protein was considered differentially expressed when the p-value was < 0.05 and the fold change was > 1.2 or < 0.8. B Comparison of the four selected differentially expressed protein (CD40, SOST, fibronectin, and calcitonin) levels between each subgroup of patients with SSc and the HCs
The GO analysis of differentially expressed proteins
The enormous amount of microarray data may reveal the intrinsic mechanism of SSc in addition to diagnostic biomarkers. We performed GO functional analysis for the top 10 biological activities in which the DEPs primarily participated for each SSc subgroup. GO analysis of the SSc with PAH group indicated that the processes of peptidyl-tyrosine phosphorylation, peptidyl-tyrosine modification, protein autophosphorylation, leukocyte migration, positive regulation of kinase activity, positive regulation of protein kinase activity, regulation of tissue remodeling, and cell chemotaxis were activated, and the processes of acute-phase response and negative regulation of endopeptidase activity were inhibited (Fig. 1A). For the SSc with ILD group, the processes of regulation of protein secretion, acute-phase response, positive regulation of secretion by cell, positive regulation of protein production, positive regulation of protein secretion, positive regulation of secretion, protein secretion, and establishment of protein localization to extracellular region were all activated (Fig. 1B). Finally, for the SSc without PAH and ILD group, the processes of acute inflammatory response, acute-phase response, negative regulation of hydrolase activity, complement-dependent cytotoxicity, and negative regulation of endopeptidase activity were inhibited, while the processes of positive regulation of protein production, humoral immune response, and regulation of lymphocyte proliferation were activated (Fig. 1C).
Further validation and correlation analysis in SSc patients
Validation of differentially expressed proteins by ELISA
ELISA was performed to validate the four selected DEPs in additional samples from treatment-naïve patients with SSc and HCs. This indicated that calcitonin and SOST serum levels were both significantly increased in all three SSc subgroups compared to the HCs (n = 20), while the calcitonin level was much higher in the SSc with PAH group (n = 19) and the SOST level was much lower in the SSc with ILD group (n = 22) than in the SSc without PAH and ILD group (n = 17). However, the CD40 level was not uniquely increased in the SSc with PAH group but was significantly decreased in the SSc with ILD group compared with the other SSc subgroups and HCs. Fibronectin levels did not differ between the groups (Fig. 3A).

The validation and correlation analysis of the four selected proteins. A Comparison of serum levels of the four selected proteins between each SSc subgroup and the HCs using ELISA tests. B, C Correlation analysis of the clinical features/laboratory results/examination results and serum protein levels performed by the Pearson correlation analysis (B) and the point biserial correlation test (C). * indicated p-value < 0.05, ** indicated p-value < 0.01
Correlation study of protein levels and clinical characteristics
These four proteins were differentially expressed in patients with SSc in a protein microarray study. We also discovered that the correlation between SOST levels and the presence of ILD in SSc was controversial because SOST levels were negatively correlated with both the diffusing capacity of the lungs for carbon monoxide (DLCO%) and the presence of ILD on HRCT. Calcitonin levels may be positively correlated with the presence of PAH in SSc. In addition, calcitonin and CD40 levels might be positively related to renal damage in SSc because of their positive correlation with urea nitrogen levels, creatinine levels, and the presence of renal crisis. The SOST level was likely to be positively related to damage to liver cells, biliary system, gastrointestinal system, and myocardium, while calcitonin levels were likely to be positively related to gastrointestinal damage (Fig. 3B, C).
Discussion
The causes of SSc-related deaths have changed over the past 50 years, possibly because of increasing knowledge about the pathogenic mechanism and proper treatment of SSc [3, 6, 7]. Currently, the main causes of death in patients with SSc, including SSc-related and SSc-unrelated deaths, are ILD (16.8%), PAH (14.7%), and cardiac disease (12.0%) [3]. Pulmonary complications are still the leading cause of death in SSc, whereas cardiac disease is an emerging cause of death, with a mortality ratio only second to pulmonary complications [3, 8]. Renal crisis was once the leading cause of death in patients with SSc, while it now accounts for only 2.9% of deaths [3, 6]. However, SSc renal crisis remains a critical internal complication that requires large doses of an angiotensin-converting enzyme inhibitor [9,10,11]. Gastrointestinal dysmotility is the most frequent complication of SSc and manifests as gastroesophageal reflux disease, dysphagia, early satiety, vomiting, diarrhea, and constipation [12,13,14]. Severe gastrointestinal disease in SSc correlates with high mortality, accounting for 3.9% of SSc deaths [12, 14]. Because of the poor prognosis, we aimed to identify specific biomarkers for the early detection of these major organ complications, especially pulmonary complications, in SSc.
Previous studies have investigated serum biomarkers for SSc pulmonary complications owing to the convenience of measuring them. For SSc-related ILD, it has been reported that high levels of anti-U11/U12 antibodies, human epididymis protein 4, secreted frizzled receptor protein 4, transcription factor scleraxis, endothelin-1, cold-inducible RNA-binding protein, Krebs von den Lungen-6, surfactant protein D, CA15-3, and intercellular adhesion molecule 1 were potential serum biomarkers for early detection and severity assessment of ILD [15,16,17,18,19,20,21,22]. Serum anti-U11/U12 antibodies are strongly associated with moderate-to-severe gastrointestinal dysmotility [22]. For SSc-related PAH, it has been reported that serum levels of anti-centromere antibody (especially the anti-p4.2 antibody subset), anti-vinculin antibody, IL-32, midkine, follistatin-like 3, osteopontin, chemerin, and specific long noncoding RNAs (e.g., ANCR and SPRY4-IT1) are positively correlated with the presence of PAH, whereas serum anti-topoisomerase antibody levels are negatively correlated with the presence of PAH [23,24,25,26,27,28,29,30]. In this microarray study, we identified 125 serum protein biomarkers in different pulmonary complication subgroups of patients with SSc. The selected four proteins (calcitonin, fibronectin, CD40, and SOST) were further verified by ELISA tests, among which the serum calcitonin level was confirmed to be upregulated in both SSc and SSc-PAH patients, and the serum SOST level was confirmed to be equally upregulated in each pulmonary complication subgroups of patients with SSc. Further analysis of the clinical data revealed a possible correlation between serum SOST levels and the presence of ILD. Moreover, serum CD40 and calcitonin levels appeared to be positively related to the presence of renal involvement, serum calcitonin, and SOST levels to the presence of gastrointestinal involvement, and serum SOST levels to the presence of cardiac involvement. The mechanisms underlying the differential expression of these proteins in SSc require further investigation.
The pathogenesis of SSc is characterized by endothelial injury, vasculopathy, tissue fibrosis, inflammation, and autoimmunity [31, 32]. Endothelial injury is proposed to be the initial event in SSc pathogenesis, whereas tissue fibrosis may be the culminating event [33]. Immune cells, including dendritic, Th2, and Treg cells, appear to be involved in both the early inflammatory response and the late fibrotic process [33]. These crucial events are regulated by the complex orchestration of genetic backgrounds, epigenetic modifications, environmental cues, molecular triggers, and intracellular signaling pathways [1, 32]. Bone metabolism appears to play a role in the pathogenesis of SSc; therefore, numerous skeletal disorders (including calcinosis, osteoporosis, and osteolysis) can occur in the early stages of SSc [34,35,36]. The pathogenesis of bone damage in SSc remains uncertain; however, microvascular dysfunction and hypoxic shock have been proposed as possible driving factors [34]. Both calcitonin and SOST are primarily considered bone metabolism regulators and were positively correlated with the presence of SSc and SSc-related pulmonary complications in this study. Calcitonin also participates in the regulation of extracellular matrix deposition, fibroblast activation, immune responses, inflammation, and endothelial dysfunction [37,38,39,40,41]. Additionally, SOST has been confirmed to be a Wnt signaling antagonist that is very important in SSc pathogenesis [1, 42]. SOST has also been reported to modulate immune cell development and differentiation of B, Th17, and Treg cells [43]. Therefore, serum calcitonin and SOST were proposed as biomarkers for patients with SSc and SSc-related pulmonary complications in this study. However, further verification is required because of the existence of controversial studies.
All patients with SSc recruited in this study were treatment-naïve; therefore, their serum protein profiles were undisturbed. PAH was diagnosed using a right heart catheter instead of echocardiography. Therefore, the results of this study are considered credible. However, this study has some limitations, such as the small sample size and lack of mechanistic studies. CD40 and fibronectin have been proposed to participate in the pathogenesis of SSc in previous studies, and their levels have been proposed to be elevated in patients with SSc [44,45,46,47,48,49]. However, there was no significant difference between the patients with SSc and HCs in this study. There are contradictory results regarding serum SOST levels in a few small-sample studies that showed no difference between patients with SSc and HCs [50, 51]. However, it has been suggested that serum SOST levels positively correlate with the severity of skin fibrosis [51]. Therefore, the results of this study need to be validated with more evidence from intensive studies.
Conclusions
In conclusion, serum protein biomarkers may be useful for the early detection of vital organ involvement in SSc, which may lead to a poor prognosis. This study indicates that serum calcitonin and SOST levels are promising biomarkers for SSc-related PAH and ILD, respectively. Further research is needed to verify these results and understand the underlying mechanisms.
Availability of data and materials
The datasets used during the current study are available from the corresponding author on reasonable request.
Abbreviations
- SSc:
-
Systemic sclerosis
- PAH:
-
Pulmonary arterial hypertension
- ILD:
-
Interstitial lung disease
- SOST:
-
Sclerostin
- HC:
-
Healthy control
- GO:
-
Gene Ontology
- mPAP:
-
Mean pulmonary arterial pressure
- PAWP:
-
Pulmonary arterial wedge pressure
- HRCT:
-
High-resolution computerized tomography
- TRV:
-
Tricuspid regurgitation velocity
- DEP:
-
Differentially expressed protein
- DLCO:
-
Diffusing capacity of the lungs for carbon monoxide
References
Mouawad JE, Feghali-Bostwick C. The molecular mechanisms of systemic sclerosis-associated lung fibrosis. Int J Mol Sci. 2023;24(3):2693.
Barkhane Z, Nimerta F, Zulfiqar S, Dar S, Afzal MS, Zaree A, Adwani R, Palleti SK. Independent predictors of mortality in systemic sclerosis-associated pulmonary arterial hypertension: a systematic review and meta-analysis. Cureus. 2023;15(5):e39730.
Elhai M, Meune C, Boubaya M, Avouac J, Hachulla E, Balbir-Gurman A, Riemekasten G, Airò P, Joven B, Vettori S, et al. Mapping and predicting mortality from systemic sclerosis. Ann Rheum Dis. 2017;76(11):1897–905.
Rahaghi FF, Hsu VM, Kaner RJ, Mayes MD, Rosas IO, Saggar R, Steen VD, Strek ME, Bernstein EJ, Bhatt N, et al. Expert consensus on the management of systemic sclerosis-associated interstitial lung disease. Respir Res. 2023;24(1):6.
Ngo K. Systemic sclerosis and pulmonary disease. Adv Exp Med Biol. 2021;1303:173–82.
Steen VD, Medsger TA. Changes in causes of death in systemic sclerosis, 1972–2002. Ann Rheum Dis. 2007;66(7):940–4.
Tyndall AJ, Bannert B, Vonk M, Airò P, Cozzi F, Carreira PE, Bancel DF, Allanore Y, Müller-Ladner U, Distler O, et al. Causes and risk factors for death in systemic sclerosis: a study from the EULAR Scleroderma Trials and Research (EUSTAR) database. Ann Rheum Dis. 2010;69(10):1809–15.
Hu S, Hou Y, Wang Q, Li M, Xu D, Zeng X. Prognostic profile of systemic sclerosis: analysis of the clinical EUSTAR cohort in China. Arthritis Res Ther. 2018;20(1):235.
Scheen M, Dominati A, Olivier V, Nasr S, De Seigneux S, Mekinian A, Issa N, Haidar F. Renal involvement in systemic sclerosis. Autoimmun Rev. 2023;22(6): 103330.
Cole A, Ong VH, Denton CP. Renal disease and systemic sclerosis: an update on scleroderma renal crisis. Clin Rev Allergy Immunol. 2023;64(3):378–91.
Ida T, Ikeda K, Ohbe H, Nakamura K, Furuya H, Iwamoto T, et al. Early initiation of angiotensin-converting enzyme inhibitor in patients with scleroderma renal crisis: A nationwide inpatient database study. Rheumatology (Oxford). 2023:kead343. https://doi.org/10.1093/rheumatology/kead343. Epub ahead of print. PMID: 37458488.
McMahan ZH, Kulkarni S, Chen J, Chen JZ, Xavier RJ, Pasricha PJ, Khanna D. Systemic sclerosis gastrointestinal dysmotility: risk factors, pathophysiology, diagnosis and management. Nat Rev Rheumatol. 2023;19(3):166–81.
Quinlivan A, McMahan ZH, Lee EB, Nikpour M. Gastrointestinal tract considerations: part II: how should a rheumatologist best manage common lower gastrointestinal tract complaints in systemic sclerosis? Rheum Dis Clin North Am. 2023;49(2):319–36.
Quinlivan A, McMahan ZH, Lee EB, Nikpour M. Gastrointestinal tract considerations part I: how should a rheumatologist best manage common upper gastrointestinal tract complaints in systemic sclerosis? Rheum Dis Clin North Am. 2023;49(2):295–318.
Zhang M, Zhang L, Linning E, Xu K, Wang XF, Zhang B, Su J, Meng Z. Increased levels of HE4 (WFDC2) in systemic sclerosis: a novel biomarker reflecting interstitial lung disease severity? Therapeut Adv Chron Dis. 2020;11:2040622320956420.
Tinazzi I, Mulipa P, Colato C, Abignano G, Ballarin A, Biasi D, et al. SFRP4 expression is linked to immune-driven fibrotic conditions, correlates with skin and lung fibrosis in SSc and a potential EMT biomarker. J Clin Med. 2021;10(24):5820.
Ramírez-Aragón M, Hernández-Sánchez F, Rodríguez-Reyna TS, Buendía-Roldán I, Güitrón-Castillo G, Núñez-Alvarez CA, et al. The transcription factor SCX is a potential serum biomarker of fibrotic diseases. Int J Mol Sci. 2020;21(14):5012.
Pulito-Cueto V, Genre F, López-Mejías R, Mora-Cuesta VM, Iturbe-Fernández D, Portilla V, et al. Endothelin-1 as a biomarker of idiopathic pulmonary fibrosis and interstitial lung disease associated with autoimmune diseases. Int J Mol Sci. 2023;24(2):1275.
Omori I, Sumida H, Sugimori A, Sakakibara M, Urano-Takaoka M, Iwasawa O, Saito H, Matsuno A, Sato S. Serum cold-inducible RNA-binding protein levels as a potential biomarker for systemic sclerosis-associated interstitial lung disease. Sci Rep. 2023;13(1):5017.
Kilinc AA, Arslan A, Yildiz M, Kucur M, Adrovic A, Barut K, Sahin S, Cokugras H, Kasapcopur O. Serum KL-6 level as a biomarker of interstitial lung disease in childhood connective tissue diseases: a pilot study. Rheumatol Int. 2020;40(10):1701–6.
Jee AS, Stewart I, Youssef P, Adelstein S, Lai D, Hua S, Stevens W, Proudman S, Ngian GS, Glaspole IN, et al. A composite serum biomarker index for the diagnosis of systemic sclerosis-associated interstitial lung disease: a multicenter, observational cohort study. Arthritis Rheumatol (Hoboken, NJ). 2023;75(8):1424–33.
Fritzler MJ, Bentow C, Beretta L, Palterer B, Perurena-Prieto J, Sanz-Martínez MT, et al. Anti-U11/U12 antibodies as a rare but important biomarker in patients with systemic sclerosis: a narrative review. Diagnost (Basel, Switzerland). 2023;13(7):1257.
Senturk B, Akdeniz B, Yilmaz MB, Ozcan Kahraman B, Acar B, Uslu S, Birlik M. Whole blood viscosity in systemic sclerosis: a potential biomarker of pulmonary hypertension? Clin Rheumatol. 2020;39(1):49–56.
Rice LM, Mantero JC, Stratton EA, Warburton R, Roberts K, Hill N, Simms RW, Domsic R, Farber HW, Layfatis R. Serum biomarker for diagnostic evaluation of pulmonary arterial hypertension in systemic sclerosis. Arthritis Res Ther. 2018;20(1):185.
Ibrahim NH, Fawzy IM, Gouda TM, El Sayed RAH, Morsi MH, Sabry ASM, Hashaad NI. Anti-vinculin antibodies as a novel biomarker in Egyptian patients with systemic sclerosis. Clin Rheumatol. 2022;41(11):3401–9.
Favoino E, Catacchio G, Mininni A, Ruscitti P, Riccieri V, Liakouli V, Corrado A, Navarini L, Ciccia F, Cipriani P, et al. Novel biomarker for pulmonary vascular disease in systemic sclerosis patients. Clin Exp Rheumatol. 2022;40(10):1956–63.
Di Benedetto P, Guggino G, Manzi G, Ruscitti P, Berardicurti O, Panzera N, Grazia N, Badagliacca R, Riccieri V, Vizza CD, et al. Interleukin-32 in systemic sclerosis, a potential new biomarker for pulmonary arterial hypertension. Arthritis Res Ther. 2020;22(1):127.
Bellan M, Piccinino C, Tonello S, Minisini R, Giubertoni A, Sola D, et al. Role of osteopontin as a potential biomarker of pulmonary arterial hypertension in patients with systemic sclerosis and other connective tissue diseases (CTDs). Pharmaceuticals (Basel, Switzerland). 2021;14(5):394.
Abd-Elmawla MA, Hassan M, Elsabagh YA, Alnaggar A, Senousy MA. Deregulation of long noncoding RNAs ANCR, TINCR, HOTTIP and SPRY4-IT1 in plasma of systemic sclerosis patients: SPRY4-IT1 as a novel biomarker of scleroderma and its subtypes. Cytokine. 2020;133:155124.
Sanges S, Rice L, Tu L, Valenzi E, Cracowski JL, Montani D, Mantero JC, Ternynck C, Marot G, Bujor AM, et al. Biomarkers of haemodynamic severity of systemic sclerosis-associated pulmonary arterial hypertension by serum proteome analysis. Ann Rheum Dis. 2023;82(3):365–73.
Volkmann ER, Andréasson K, Smith V. Systemic sclerosis. Lancet (London, England). 2023;401(10373):304–18.
Truchetet ME, Brembilla NC, Chizzolini C. Current concepts on the pathogenesis of systemic sclerosis. Clin Rev Allergy Immunol. 2023;64(3):262–83.
Di Battista M, Lepri G, Codullo V, Da Rio M, Fiorentini E, Della Rossa A, Guiducci S. Systemic sclerosis: one year in review 2023. Clin Exp Rheumatol. 2023;41(8):1567–74.
Sciacca S, Corrado A, Rotondo C, Cantatore FP. Bone metabolism alterations in systemic sclerosis: an insight into bone disease in SSc: from the radiographic findings to their potential pathogenesis and outcome. Curr Rheumatol Rev. 2022;18(4):286–97.
Davuluri S, Lood C, Chung L. Calcinosis in systemic sclerosis. Curr Opin Rheumatol. 2022;34(6):319–27.
Guerra MG, Rodrigues M, Águeda A, Rodrigues J, Marona J, Violante A, Oliveira M. Osteolysis in systemic sclerosis: a scoping review. J Rheumatol. 2023;50(7):863–72.
Yang R, Deng H, Hou J, Li W, Zhang C, Yu M, Tang Y, Li Q, Li F, Song B, et al. Investigation of salmon calcitonin in regulating fibrosis-related molecule production and cell-substrate adhesion in frozen shoulder synovial/capsular fibroblasts. J Orthopaed Res. 2020;38(6):1375–85.
Moreira LM, Takawale A, Hulsurkar M, Menassa DA, Antanaviciute A, Lahiri SK, Mehta N, Evans N, Psarros C, Robinson P, et al. Paracrine signalling by cardiac calcitonin controls atrial fibrogenesis and arrhythmia. Nature. 2020;587(7834):460–5.
Maleitzke T, Hildebrandt A, Dietrich T, Appelt J, Jahn D, Otto E, Zocholl D, Baranowsky A, Duda GN, Tsitsilonis S, et al. The calcitonin receptor protects against bone loss and excessive inflammation in collagen antibody-induced arthritis. iScience. 2022;25(1):103689.
Kanbay M, Yilmaz MI, Afsar B, Saglam M, Akgul EO, Cayci T, Caglar K, Unal HU, Gok M, Vural A, et al. Serum calcitonin and endothelial dysfunction in chronic kidney disease: a novel risk factor? Int Urol Nephrol. 2013;45(1):151–6.
Jablonski H, Wedemeyer C, Bachmann HS, Schlagkamp M, Bernstein A, Jäger M, Kauther MD. A single dose of the anti-resorptive peptide human calcitonin paradoxically augments particle- and endotoxin-mediated pro-inflammatory cytokine production in vitro. Hormone Metab Res Hormon- und Stoffwechselforschung Hormones et metabolisme. 2016;48(9):607–12.
Li X, Zhang Y, Kang H, Liu W, Liu P, Zhang J, Harris SE, Wu D. Sclerostin binds to LRP5/6 and antagonizes canonical Wnt signaling. J Biol Chem. 2005;280(20):19883–7.
Sun M, Chen Z, Wu X, Yu Y, Wang L, Lu A, Zhang G, Li F. The roles of sclerostin in immune system and the applications of aptamers in immune-related research. Front Immunol. 2021;12:602330.
Komura K, Fujimoto M, Yanaba K, Matsushita T, Matsushita Y, Horikawa M, Ogawa F, Shimizu K, Hasegawa M, Takehara K, et al. Blockade of CD40/CD40 ligand interactions attenuates skin fibrosis and autoimmunity in the tight-skin mouse. Ann Rheum Dis. 2008;67(6):867–72.
Komura K, Fujimoto M, Matsushita T, Yanaba K, Kodera M, Kawasuji A, Hasegawa M, Takehara K, Sato S. Increased serum soluble CD40 levels in patients with systemic sclerosis. J Rheumatol. 2007;34(2):353–8.
Kawai M, Masuda A, Kuwana M. A CD40-CD154 interaction in tissue fibrosis. Arthritis Rheum. 2008;58(11):3562–73.
Jun JB, Kim TH, Na YI, Yoo DH. High expression of CD40 on skin fibroblasts from patients with systemic sclerosis. Rheumatol Int. 2007;28(1):95–7.
Bhandari R, Yang H, Kosarek NN, Smith AE, Garlick JA, Hinchcliff M, Whitfield ML, Pioli PA. Human dermal fibroblast-derived exosomes induce macrophage activation in systemic sclerosis. Rheumatology (Oxford, England). 2023;62(Si):s114–24.
Mouawad JE, Sanderson M, Sharma S, Helke KL, Pilewski JM, Nadig SN, Feghali-Bostwick C: Extracellular vesicles propagate lung fibrosis in systemic sclerosis. Arthritis Rheumatol (Hoboken, NJ) 2023.
Fernández-Roldán C, Genre F, López-Mejías R, Ubilla B, Mijares V, Cano DS, Robles CL, Callejas-Rubio JL, Fernández RR, Ruiz ME, et al. Sclerostin serum levels in patients with systemic autoimmune diseases. BoneKEy Rep. 2016;5:775.
Taylan A, Birlik M, Kenar G, Toprak B, Gundogdu B, Gurler O, Karakas B, Akıncı B, Sisman AR. Osteoprotegrin interacts with biomarkers and cytokines that have roles in osteoporosis, skin fibrosis, and vasculopathy in systemic sclerosis: a potential multifaceted relationship between OPG/RANKL/TRAIL and Wnt inhibitors. Mod Rheumatol. 2019;29(4):619–24.
Acknowledgements
We acknowledge the work of the Rheumatology group of PUMCH for providing patients’ serum samples and clinical data.
Funding
This study was supported by CAMS Innovation Fund for Medical Sciences (CIFMS) (2021-I2M-1–005).
Author information
Authors and Affiliations
Contributions
Jing Huang drafted the manuscript and carried out the experiments. Honglin Zhu helped analyze the data. Xiaoxia Zuo, Yisha Li and Hui Luo supervised the findings of this work. Sijia Liu and Mengtao Li designed the study and supervised the experiment. The authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This study was approved by the medical ethics committee of Peking Union Medical College Hospital (PUMCH) and the ethics committee of the European League Against Rheumatism Scleroderma Trial and Research Group (EUSTAR).
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Serum samples from 15 patients with SSc and five HCs.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Huang, J., Zhu, H., Liu, S. et al. Protein profiling in systemic sclerosis patients with different pulmonary complications using proteomic antibody microarray. Arthritis Res Ther 26, 29 (2024). https://doi.org/10.1186/s13075-024-03267-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13075-024-03267-z