
Abstract
Background
This study aimed to investigate the expression profile of immune response-related proteins of Behcet’s disease (BD) patients and identify potential biomarkers for this disease.
Methods
Plasma was collected from BD patients and healthy controls (HC). Immune response-related proteins were measured using the Olink Immune Response Panel. Differentially expressed proteins (DEPs) were used to construct prediction models via five machine learning algorithms: naive Bayes, support vector machine, extreme gradient boosting, random forest, and neural network. The prediction performance of the five models was assessed using the area under the curve (AUC) value, recall (sensitivity), specificity, precision, accuracy, F1 score, and residual distribution. Subtype analysis of BD was performed using the consensus clustering method.
Results
Proteomics results showed 43 DEPs between BD patients and HC (P < 0.05). These DEPs were mainly involved in the Toll-like receptor 9 and NF-κB signaling pathways. Five models were constructed using DEPs [interleukin 10 (IL10), Fc receptor like 3 (FCRL3), Mannan-binding lectin serine peptidase 1 (MASP1), NF2, moesin-ezrin-radixin like (MERLIN) tumor suppressor (NF2), FAM3 metabolism regulating signaling molecule B (FAM3B), and O-6-methylguanine-DNA methyltransferase (MGMT)]. Among these models, the neural network model showed the best performance (AUC = 0.856, recall: 0.692, specificity: 0.857, precision: 0.900, accuracy: 0.750, F1 score: 0.783). BD patients were divided into two subtypes according to the consensus clustering method: one with high disease activity in association with higher expression of tripartite motif-containing 5 (TRIM5), SH2 domain-containing 1A (SH2D1A), phosphoinositide-3-kinase adaptor protein 1 (PIK3AP1), hematopoietic cell-specific Lyn substrate 1 (HCLS1), and DNA fragmentation factor subunit alpha (DFFA) and the other with low disease activity in association with higher expression of C–C motif chemokine ligand 11 (CCL11).
Conclusions
Our study not only revealed a distinctive immune response-related protein profile for BD but also showed that IL10, FCRL3, MASP1, NF2, FAM3B, and MGMT could serve as potential immune biomarkers for this disease. Additionally, a novel molecular disease classification model was constructed to identify subsets of BD.
Similar content being viewed by others

Introduction
Behcet’s disease (BD) is a chronic, multisystem autoinflammatory disorder characterized by recurrent oral and genital ulcerations, uveitis, and skin lesions, as well as vascular, neurological, and gastrointestinal manifestations [1, 2]. BD, also called Silk Road disease or Behcet’s syndrome, mainly occurs in countries along the ancient Silk Road from the Mediterranean Basin across Asia to Japan [3]. BD is considered as one of the most common causes of uveitis and the primary cause of blindness [4]. Our recent study involving 15 373 uveitis patients showed that BD accounted for 10.6% of cases [5].
Although the etiology of BD remains unclear, genetic susceptibility, environmental factors, viral and bacterial infections, inflammation, and immune dysregulation are involved in its development [6,7,8,9]. Immune dysfunction of both adaptive and innate immunity plays an essential role in the pathogenesis and progression of BD [10]. The levels of pro-inflammatory and anti-inflammatory cytokines have been extensively studied in the serum and plasma of patients with BD [11,12,13]. These inflammatory cytokines produced by immune cells can regulate or activate other immune cells, causing tissue damage. For example, T helper 17 (Th17) cells, which are the major subsets of CD4+ T cells, are essential to the process of BD. The differentiation of human naïve CD4+ T cells into Th17 cells is regulated by cytokines such as interleukin 6 (IL 6), transforming growth factor-β (TGF-β), interleukin 21 (IL 21), and interleukin 23 (IL 23) [14, 15]. Several studies have demonstrated that cytokines could serve as potential drug targets for the treatment of BD or candidate biomarkers for the prediction of disease activity, severity, and prognosis [16,17,18].
Evidences also indicate that some immune response-related proteins can regulate the secretion of inflammatory cytokines and differentiation of immune cells via the Janus kinase—signal transducer and activator of transcription (JAK-STAT), nuclear factor-κB (NF-κB), and P38 mitogen-activated protein kinase (P38-MAPK) signaling pathway [19,20,21]. For example, increased tripartite motif-containing 21(TRIM21) can activate the NF-κB signaling pathway to promote the secretion of IL6, interleukin 1β (IL 1β), and IL 23 and induce the differentiation of Th17 cells in BD [22]. However, the potential role of immune response-related proteins in immune and inflammatory function modulation in BD is less well studied.
The aim of this study was to investigate the expression profile of immune response-related proteins in the plasma of patients with BD and identify potential plasma biomarkers in BD.
Methods
Study population
Active BD patients ((training cohort n = 27, validation cohort n = 28) and healthy controls [HC (training cohort n = 25, validation cohort n = 28)] matched by age and sex were enrolled in the study from the First Affiliated Hospital of Zhengzhou University. BD was strictly diagnosed by rheumatologists according to the diagnostic criteria developed by the International Study Group for Behçet’s disease [1]. BD activity was evaluated using the Behçet Disease Current Activity Form (BDCAF) [23]. Uveitis was diagnosed by an ophthalmologist. Intraocular inflammation was evaluated according to the standardized uveitis nomenclature (SUN) working group classification [24]. Detailed demographic information and clinical details of the BD patients are listed in Table 1 and Supplementary Table S1.
Plasma collection
Fresh peripheral blood (10 ml) was collected in EDTA tubes, and plasma was isolated by centrifugation at 2000 g for 10 min, and then stored at − 80 °C until use.
Measurement of plasma proteins
The plasma levels of 92 immune response-related proteins were measured using a proximity extension assay (PEA, Olink Proteomics, Shanghai, China) [25]. The data are presented as normalized protein expression (NPX) values on a log2 scale. Twelve proteins were excluded from downstream analysis with intra- and inter-assay coefficient of variance (%CV) and the frequency of missing values of more than 20% in each sample. One patient sample was excluded because of quality control failure (Supplementary Figure S1a). In addition, an NPX value of less than 0 was replaced by the intragroup mean in some samples.
Data analysis and statistics methods
Principal component analysis (PCA) was performed using “FactoMiner” and “factoextra” R packages. Categorical variables are described as numbers (percentages) and compared using the chi-square test or Fisher’s exact test. Continuous variables are presented as median and interquartile range (IQR). Differences between two and three groups were compared using the non-parametric Mann–Whitney U test and Kruskal–Wallis test with Dunn’s correction, respectively. The results are presented in the form of tables or boxplots. Volcano and heatmap plots were drawn using the “ggpubr” and “pheatmap” packages. The correlated heatmap was plotted to visualize the Pearson’s correlations between differentially expressed proteins (DEPs) using the “ggcorrplot” package.
Bioinformatics analysis
Gene ontology (GO) and the Kyoto Encyclopedia of Genes and Genomes (KEGG) enrichment analyses were performed using the R package “clusterProfiler” (version 3.18.1) [26]. To further investigate the correlation between DEPs, a protein network interaction diagram (PPI) was constructed using the online tool STRING (version 11.5, https://cn.string-db.org/).
Feature selection and prediction model creation
The recursive feature elimination (RFE) algorithm, which includes feature extraction, feature selection, and model training, was performed for the features selected based on the random forest (RF) with fivefold repeated cross-validation. All DEPs were used to train the prediction model, and the feature importance of the variables was calculated and ranked using accuracy and kappa metrics. An optimal subset of features was selected from all DEPs for the prediction model creation. To construct the prediction model, five algorithms were used based on the package “caret”: naive Bayes (NB), support vector machine (SVM), extreme gradient boosting (XGB), random forest (RF), and neural network (NNET). Receiver operating characteristic (ROC) analysis, recall (sensitivity), specificity, precision, accuracy, F1 score, and residual distribution were used to assess the prediction performance of the different models on the testing set. ROC curves were plotted using the “pROC” package.
Consensus clustering
To investigate the role of differentially expressed immune response-related proteins, different clinical phenotypes, sex, and age in BD patients, K-means consensus clustering with k from 2 to 7 was performed using the R package “ConsensusClusterPlus.” The clustering results were visualized using t-distributed stochastic neighbor embedding (tSNE) based on the “Rtsne” R package. All analyses were carried out using the R language, version 4.0.3.
Results
DEPs between BD and HC
To identify DEPs in the plasma of BD patients and HC, 92 immune response-related proteins were measured using a PEA. The expression of 43 immune response-related proteins differed between BD patients and HC (P < 0.05). Six proteins were upregulated and 37 proteins were downregulated in our study. The upregulated proteins included IL6, IL10, killer cell lectin like receptor D1 (KLRD1), natural cytotoxicity triggering receptor 1 (NCR1), amphiregulin (AREG), and C-type lectin domain-containing 6A (CLEC6A) and the downregulated proteins mainly included MGMT, interleukin 1 receptor-associated kinase 1 (IRAK1), FAM3B, interleukin 1 receptor-associated kinase 4 (IRAK4), SH2D1A, and DFFA. All the DEPs are listed in Supplementary Table S2. Boxplots were constructed to represent the top 25 DEPs (Fig. 1). PCA based on the 43 DEPs was able to discriminate BD from HC samples (Fig. 2a). DEPs were visualized using a volcano plot (Supplementary Figure S1b). A clustering heatmap was plotted to show the DEPs in the different samples (Fig. 2b).

Boxplots were made to present the top 25 differential immune-related proteins between Behcet’s disease and healthy controls

Bioinformatics analysis of differentially expressed proteins of Behcet’s disease. A PCA is based on 43 differentially expressed proteins (DEPs). B Clustering heatmap of DEPs. C GO (BP) enrichment analysis. D KEGG enrichment analysis of differential proteins. E Correlation heatmap between DEPs
GO and KEGG pathway analysis
Bioinformatics analysis was performed to investigate the biological functions of DEPs. GO enrichment and KEGG pathway analyses were performed using the upregulated and downregulated DEPs, respectively. The top 10 GO biological process (BP) terms and KEGG pathways are shown in Fig. 2c, d.
The downregulated DEPs were mainly enriched in toll-like receptor 9, positive regulation of I-kappaB kinase/NF-kappaB, toll-like receptor, NIK/NF-kappaB, and regulation of I-kappaB kinase/NF-kappaB signaling pathway, and the upregulated DEPs were mainly enriched in regulation of adaptive immune response, regulation of lymphocyte mediated immunity, regulation of adaptive immune response based on somatic recombination of immune receptors built from immunoglobulin superfamily domains, regulation of leukocyte-mediated immunity, and adaptive immune response based on somatic recombination of immune receptors built from immunoglobulin superfamily domains signaling pathway in GO (biological process (BP)) terms, respectively (P.adjust < 0.05). The downregulated DEPs were mainly enriched in NF-kappa B, toxoplasmosis, arrhythmogenic right ventricular cardiomyopathy, ECM-receptor interaction, and hypertrophic cardiomyopathy signaling pathway, and the upregulated DEPs were mainly enriched in C-type lectin receptor, malaria, intestinal immune network for IgA production, graft-versus-host disease, and African trypanosomiasis signaling pathway in the KEGG pathway analyses, respectively (P.adjust < 0.05).
Several infection pathways were identified by KEGG pathway analysis in the present study, including toxoplasmosis, pathogenic Escherichia coli infection, Epstein-Barr virus infection, human immunodeficiency virus 1 infection, malaria, African trypanosomiasis, pertussis, amoebiasis, Yersinia infection, and tuberculosis (P.adjust < 0.05), highlighting an essential role of pathogenic infection in BD (Supplementary Figure S2a). The pathways of toxoplasmosis and malaria were significantly enriched using the upregulated and downregulated DEPs, respectively (Supplementary Figure S2b and c).
Protein–protein interactions and correlations
To gain further insight into the protein–protein interactions between DEPs, correlation heatmaps and protein network interaction diagrams were constructed (Fig. 2e and Supplementary Figure S1c). Spearman’s correlation analysis showed that eukaryotic translation initiation factor 4 gamma 1 (EIF4G1) and (HEXIM P-TEFb complex subunit 1) HEXIM1 had the highest positive correlation (r = 0.93, P = 6.07e − 06), whereas tryptase alpha/beta 1 (TPSAB1) and IL10 had the highest negative correlation (r = − 0.59, P = 2.14e − 22).
Construction of the prediction model
To identify potential biomarkers, five machine learning models were constructed using NB, SVM, XGB, RF, and NNET. First, a random forest algorithm was applied for the key feature selection. Six DEPs (IL10, FCRL3, MASP1, NF2, FAM3B, and MGMT) were selected as key features (Fig. 3a). NB, SVM, XGB, RF, and NNET models were constructed, and the prediction performance for BD was assessed using the AUC value and residual distribution. The results showed that the NNET and SVM models had the best performance (NNET, AUC value: 0.856, recall: 0.692, specificity: 0.857, precision: 0.900, accuracy:0.750, F1 score: 0.783; SVM, AUC value: 0.846, recall: 0.667, specificity: 0.750, precision: 0.800, accuracy: 0.700, F1 score: 0.727), followed by the RF model (RF, AUC value: 0.817, recall: 0.727, specificity: 0.778, precision: 0.800, accuracy: 0.750, F1 score: 0.762), whereas the NB and XGB models had the poorest and most unstable performance (Fig. 3b and Table 2). In addition, the SVM and NNET models had the lowest residual distribution compared to the other models (Fig. 3c). NNET model still had the best performance (AUC value: 0.941, recall: 0.684, specificity: 0.889, precision: 0.929, accuracy: 0.750, F1 score: 0.788) compared to the other models in the validation cohort (Supplementary Table S3).

Construction of the prediction model. A The accuracy of the cross-validated RF model. B ROC curve and AUC value of NB, SVM, XGB, RF, and NNET models. C Boxplots of the residual distribution of NB, SVM, XGB, RF, and NNET models. D The importance of explanatory variables ranked by the SVM model
Based on these results, the NNET model exhibited the best prediction performance. The explanatory variables were ranked according to their importance (Fig. 3d). Besides, we further validated the biomarkers expression of IL10, FCRL3, MASP1, NF2, FAM3B, and MGMT in the validation cohort (Supplementary Figure S3). The results in the validation cohort were consistent with those in the training cohort. In addition, the correlation between these potential biomarkers and disease activity or disease duration was performed in our study, but no significant correlations were identified. The results were shown in (Supplementary Figure S4 and S5).
To further investigate the potential effects of treatments on plasma proteins, the protein expression level was compared between treated (glucocorticoids (GCs) or other immunosuppressive agents) and non-treated groups in BD patients. Four proteins were identified to be weak different between groups (Supplementary Figure S6a and b and Supplementary Table S4). Overall, the effect of treatments on the protein expression levels was very weak.
Consensus clustering analysis in BD
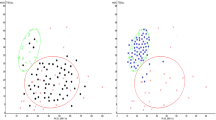
We constructed consensus clusters of BD patients based on the 43 DEPs, clinical phenotypes, sex, and age. The results of the cumulative distribution function (CDF) curves (Fig. 4a) and the relative change in area under for the CDF curve (K = 2–7) (Fig. 4b) demonstrated that consensus clustering was the most stable when K = 2 (Fig. 4c). Patients with BD were divided into two distinct clusters, cluster 1 and cluster 2 (Fig. 4d, e). We also plotted a clustering heatmap to present the expression levels of immune response-related proteins in both BD patient subsets (Fig. 4f). Protein expression levels were compared between cluster 1 and cluster 2. There were 21 upregulated proteins and one downregulated protein in cluster 1 compared to cluster 2 (Table 3).

Consensus clustering of BD patients. A The consensus clustering CDF curve for K = 2–7. B The delta area score of the CDF curve for k = 2–7. C Tracking plot for k = 2–7 in BD patients. D Consensus clustering was the most stable when K = 2. E PCA based on 43 DEPs, different clinical phenotype, sex, age. F Heatmap showing the expression of 43 DEPs between the cluster 1 and cluster 2 groups. G Comparison of the score of BDCAF between the cluster 1 and cluster 2 groups
The demographic and clinical features between two subsets of BD patients
We compared the differences in protein expression levels and clinical features between cluster 1 and cluster 2. In addition, to assess the scores BDCAF, patients were asked about the presence of clinical symptoms over the 4 weeks prior to when they visited us. Clinical features and BDCAF scores are shown in Table 4. A total of 14 BD patients were grouped into cluster 1, while 12 BD patients were grouped into cluster 2. The mean age of cluster 1 and cluster 2 patients were 22.57 ± 7.70 years and 45.25 ± 9.84 years, respectively. A significant difference in age distribution was observed between the two subsets (P < 0.001). Although the patients from cluster 1 had higher BDCAF scores (3.93 ± 1.44 versus (vs). 3.08 ± 1.38)), this difference was not significant. Furthermore, there was no significant difference in the clinical features between the two groups. A higher frequency of mouth ulcers (13 (92.9%) vs. 6 (50.0%)), and genital ulcers (10 (71.4%) vs. 4 (33.3%)) was observed for cluster 1. There were no statistical differences in the use of immunosuppression between the two groups. Besides, a significant difference (P < 0.05) was found in terms of disease duration between cluster 1 (24.0 (17.25–54.50)) and cluster 2 (80.0 (36.0–215.2)). We further investigated the correlation between the expression level of DEPs and disease duration. Pearson correlation tests revealed that the expression level of TRIM5, Egl-9 family hypoxia inducible factor 1 (EGLN1), SH2D1A, and DFFA were positive correlation with disease duration (P < 0.05) (Supplementary Figure S7) and age positively correlated with disease duration (r = 0.42, P = 0.032).
DEPs between Behcet’s disease with and without uveitis
To investigate whether there are any differences between Behcet’s disease with and without uveitis, we compared the protein expression levels (Supplementary Table S5). The expression of PLXNA4 was significantly differentially expressed between BD with uveitis (BDU) and that without uveitis (BDNU) in the training cohort (P = 0.0054) and in the validation cohort (P = 0.0008) (Supplementary Figure S8).
Discussion
BD is a chronic, multisystem autoinflammatory disorder. The diagnosis of BD mainly relies on clinical symptoms. In this study, we examined the expression levels of immune response-related proteins in the plasma of patients with BD using the Olink Immune Response panel. The results demonstrated aberrant expression of immune response-related proteins profiles in BD patients. Potential biomarkers were identified by constructing predictive models using machine learning algorithms. We also constructed a novel molecular disease classification model to identify the subsets of BD.
The etiology of BD remains unknown. We measured the expression levels of immune response-related protein to investigate the immunopathogenesis of BD. A total of 43 DEPs were identified in the BD and HC groups. The results of GO and KEGG enrichment analyses highlighted that the NF-κB signaling pathway and Toll like receptor 9 (TLR9) signaling pathway are involved in the occurrence of BD. These results are consistent with those of a previous study. Verrou et al. performed RNA-sequencing analysis in peripheral blood mononuclear cells and found that the NF-κB signaling pathway is related to BD [27]. Previous studies also reported that the NF-κB signaling pathway could protect T cells against CD95-mediated apoptosis in BD [28]. The NF-κB signaling pathway is considered a typical pro-inflammatory pathway, and the activation of signaling pathways induces the production of various proinflammatory cytokines such as IL-6 and IL-8 [29]. The NF-κB signaling pathway is also involved in the development of other rheumatic autoimmune diseases [30]. Activation of the NF-κB signaling pathway induces chronic inflammation of the synovium in rheumatoid arthritis [31].
TLR9 signaling pathway is essential for the regulation of both innate and adaptive immunity, and it is also involved in the production of type I interferons (IFNs) [32]. A recent study reported that dysregulation of TLR9 contributes to the production of IFN-γ and leads to fatal inflammatory disease in neonates [33]. Activation of the TLR9 signaling pathway has been observed in patients with primary Sjögren’s syndrome based on single cell phosphorylation profiling [34]. Additionally, in an experimental autoimmune encephalomyelitis (EAE) animal model of multiple sclerosis, pathogens have been attributed to TLR9-mediated innate immunity [35]. Overall, our study further identified the activation of the NF-κB and TLR9 signaling pathways in the plasma of BD. Together, these studies indicate that NF-κB and TLR9 signaling pathways are involved in the immunopathogenesis of BD. The DEPs were also enriched in infections-related signaling pathways such as toxoplasmosis and Epstein-Barr virus infection. Although the role of toxoplasmosis and Epstein-Barr virus infection in the pathogenesis of BD is less well understood, some studies have demonstrated that toxoplasmosis and Epstein-Barr virus infection are the risk factors for other systemic immune diseases, including rheumatoid arthritis and systemic lupus erythematosus [36, 37], and were associated with the activation of the NF-κB signaling pathway [38, 39]. In addition, a recent plasma proteomic study in BD patients also revealed that several infection pathways, for example, pertussis, amoebiasis, and tuberculosis, were associated with the pathogenesis of BD [40]. These pathways implicated the role of infection in the pathogenesis of BD.
IL-10, FCRL3, MASP1, NF2, FAM3B, and MGMT are potential candidate biomarkers for BD. The diagnosis of BD was made based on clinical symptoms [41]. To the best of our knowledge, the current study is the first to use machine learning algorithms to identify the potential candidate biomarkers in BD.
IL-10 is an anti-inflammatory cytokine that can inhibit Th1 cytokine production and Th1 cell differentiation [6]. Our results are consistent with the results reported by Aridogan et al., which described the elevated level of IL-10 in the serum of active BD [42]. In addition, our previous study assessed the aqueous cytokine levels in BD and senile cataract patients. However, the expression level of IL-10 was not statistically significant, which might be because the intraocular inflammations of BD were in the inactive phase [43]. Overall, the overexpression of IL 10 may represent a compensatory mechanism in response to chronic inflammation in BD. The overexpression of IL 10 may play an important role in dampening excessive inflammation by inhibiting IL 6, which is also highly expressed in our study [44]. Another possible explanation is that IL-10 may have a dual role in immune responses. While IL 10 is generally considered to be anti-inflammatory, it can also promote inflammation under certain circumstances [45]. For example, IL 10 has been shown to enhance the inflammatory response in some autoimmune diseases, such as systemic lupus erythematosus (SLE) [46]. It is possible that IL 10 has a similar pro-inflammatory effect in BD.
FCRL3 is an orphan receptor, which is only expressed on the lymphocyte cell surface. it can inhibit the secretion of TNF-α, IL 1β, IL 6, and IL-8 by promoting the expression of IL 10 in multiple sclerosis [47]. In addition, a single nucleotide polymorphism in the FCRL3 promoter region binding of the NF-κB is associated with rheumatoid arthritis, autoimmune thyroid disease, and systemic lupus erythematosus [48]. Our previous study also found associations between a single nucleotide polymorphism of FCRL3 and BD susceptibility in the Chinese population [49]. MASP1 is a serine protease involved in complement system. It is essential for defense against invading pathogens and altering host structures [50]. NF2, FAM3B, and MGMT are primarily involved in regulating the tumor immune microenvironment [51,52,53]. We reported, for the first time, a significant difference in the expression levels of NF2, FAM3B, and MGMT between BD and HC. However, further experiments are needed to explore the functional role of NF2, FAM3B, and MGMT in BD and other autoimmune diseases.
We report a novel molecular disease classification model for BD based on an unsupervised consensus clustering algorithm. DEPs, clinical phenotypes, sex, and age were used to construct the model. BD patients were divided into two subsets, cluster 1 with 14 patients and cluster 2 with 12 patients, characterized by distinct cytokine production profiles and disease activity. The characterization of cluster 1 was high disease activity and high TRIM5, SH2D1A, PIK3AP1, HCLS1, and DFFA expression. The characterization of cluster 2 showed low disease activity associated with a higher expression of CCL11. Our molecular disease model differed from the previous clinical classification model in that it is a novel immunophenotype for BD [54]. This model provides insight into the immunopathogenesis of BD and might help further refine the classification and diagnosis of BD. Besides, TRIM5, EGLN1, SH2D1A, and DFFA were correlated with disease duration, which may explain the classification model.
Another interesting finding from our study was that PLXNA4 (plexin A4) is a DEP between BDU and BDNU, whereby PLXNA4 expression was down-regulated in BDU. A previous study indicated that cytokines could impair vascular integrity by downregulating the expression of PLXNA4 [55]. This may explain the occurrence of retinal vasculitis in BDU.
Our study had some limitations. Most patients in our study previously received small doses of immunosuppressants; however, the effect of treatments was weak. Further clinical significance and function of candidate biomarkers need to be comprehensively investigated. It is undeniable that sample sizes are small in our study. We only compared the uveitis phenotype and without uveitis phenotype in BD patients. Further expanded experimental sample size and analysis of the relationship between immune response-related proteins and other phenotypes of BD patients will be necessary.
Conclusions
In summary, our results revealed that immune response-related proteins were differentially and significantly expressed in the plasma of patients with BD compared with HC. Based on machine learning algorithms, we confirmed that IL-10, FCRL3, MASP1, NF2, FAM3B, and MGMT may be promising biomarkers for BD. Furthermore, PLXNA4 may be a valuable biomarker to predict the occurrence of uveitis in patients with BD. A novel disease classification model using proteomic and clinical data has been constructed to identify subsets of patients with BD. However, further prospective studies are required to validate these findings.
Availability of data and materials
Supplementary data are available at Arthritis Research & Therapy online.
Abbreviations
- AUC:
-
Area under the curve
- BD:
-
Behcet’s disease
- BDCAF:
-
Behçet Disease Current Activity Form
- BDNU:
-
Behcet’s disease without uveitis
- BDU:
-
Behcet’s disease with uveitis
- BP:
-
Biological process
- CCL11:
-
C-C motif chemokine ligand 11
- CV:
-
Coefficient of variance
- DEPs:
-
Differentially expressed proteins
- DFFA:
-
DNA fragmentation factor subunit alpha
- FAM3B:
-
FAM3 metabolism regulating signaling molecule B
- FCRL3:
-
Fc receptor like 3
- GCs:
-
Glucocorticoids
- GO:
-
Gene ontology
- HC:
-
Healthy controls
- HCLS:
-
Hematopoietic cell-specific Lyn substrate 1
- IL10:
-
Interleukin 10
- IL6:
-
Interleukin 6
- KEGG:
-
Kyoto Encyclopedia of Genes and Genomes
- MASP:
-
Mannan-binding lectin serine peptidase 1
- MGMT:
-
O-6-Methylguanine-DNA methyltransferase
- NB:
-
Naive Bayes
- NF2:
-
NF2, moesin-ezrin-radixin like (MERLIN) tumor suppressor
- NF-ΚB:
-
Nuclear factor-κB
- NNET:
-
Neural network
- NPX:
-
Normalized protein expression
- PCA:
-
Principal component analysis
- PEA:
-
Proximity extension assay
- PIK3AP1:
-
Phosphoinositide-3-kinase adaptor protein 1
- PLXNA4:
-
Plexin A4
- PPI:
-
Protein network interaction
- RF:
-
Random forest
- ROC:
-
Receiver operating characteristic
- SH2D1A:
-
SH2 domain-containing 1A
- SVM:
-
Support vector machine
- TH17:
-
T helper 17
- TRIM21:
-
Tripartite motif-containing 21
- TRIM5:
-
Tripartite motif-containing 5
- tsne:
-
T-distributed stochastic neighbor embedding
- VS:
-
Versus
- XGB:
-
Extreme gradient boosting
References
Criteria for diagnosis of Behçet’s disease. International Study Group for Behçet’s Disease. Lancet. 1990;335(8697):1078-1080. PMID: 1970380.
Sakane T, Takeno M, Suzuki N, Inaba G. Behçet’s disease. N Engl J Med. 1999;341(17):1284–91.
Verity DH, Marr JE, Ohno S, Wallace GR, Stanford MR. Behçet’s disease, the Silk Road and HLA-B51: historical and geographical perspectives. Tissue Antigens. 1999;54(3):213–20.
Yang P, Fang W, Meng Q, Ren Y, Xing L, Kijlstra A. Clinical features of chinese patients with Behçet’s disease. Ophthalmology. 2008;115(2):312-318.e314.
Yang P, Zhong Z, Du L, Li F, Chen Z, Zhu Y, Zhang W, Huang F, Ye X, Su G, et al. Prevalence and clinical features of systemic diseases in Chinese patients with uveitis. Br J Ophthalmol. 2021;105(1):75–82.
Salmaninejad A, Zamani MR, Shabgah AG, Hosseini S, Mollaei F, Hosseini N, Sahebkar A. Behçet’s disease: an immunogenetic perspective. J Cell Physiol. 2019;234(6):8055–74.
Akkoç N. Update on the epidemiology, risk factors and disease outcomes of Behçet’s disease. Best Pract Res Clin Rheumatol. 2018;32(2):261–70.
Yang P, Ohno S, Zierhut M. Editorial: New insights into uveitis: immunity, genes, and microbes. Front Immunol. 2021;12:765377.
Tan H, Pan S, Zhong Z, Su G, Kijlstra A, Yang P. Association between fine particulate air pollution and the onset of uveitis in mainland China. Ocul Immunol Inflamm. 2022;30(7–8):1810–5.
Zouboulis CC, May T. Pathogenesis of Adamantiades-Behcet’s disease. Med Microbiol Immunol. 2003;192(3):149–55.
Sadeghi A, Davatchi F, Shahram F, Karimimoghadam A, Alikhani M, Pezeshgi A, Mazloomzadeh S, Sadeghi-Abdollahi B, Asadi-Khiavi M. Serum profiles of cytokines in Behcet’s Disease. J Clin Med. 2017;6(5):49.
Gholijani N, Ataollahi MR, Samiei A, Aflaki E, Shenavandeh S, Kamali-Sarvestani E. An elevated pro-inflammatory cytokines profile in Behcet’s disease: a multiplex analysis. Immunol Lett. 2017;186:46–51.
Akkurt ZM, Bozkurt M, Ucmak D, Yuksel H, Ucak H, Sula B, Gursel Ozkurt Z, Yildiz M, Akdeniz D, Arica M. Serum cytokine levels in Behcet’s disease. J Clin Lab Anal. 2015;29(4):317–20.
Singh RP, Hasan S, Sharma S, Nagra S, Yamaguchi DT, Wong DT, Hahn BH, Hossain A. Th17 cells in inflammation and autoimmunity. Autoimmun Rev. 2014;13(12):1174–81.
Zhong Z, Su G, Kijlstra A, Yang P. Activation of the interleukin-23/interleukin-17 signalling pathway in autoinflammatory and autoimmune uveitis. Prog Retin Eye Res. 2021;80:100866.
Prasinou M, Smith R, Vrettos A, Jayne DRW. The role of IL-18 in Behcet’s disease; a potential therapeutic target. Autoimmun Rev. 2020;19(9):102613.
Zouboulis CC, Altenburg A. Interleukin-18 is a sensitive marker of flare initiation in Adamantiades-Behçet disease. Br J Dermatol. 2021;184(5):973–5.
Polat M, Vahaboglu G, Onde U, Eksioglu M. Classifying patients with Behçet’s disease for disease severity, using a discriminating analysis method. Clin Exp Dermatol. 2009;34(2):151–5.
Sun SC. The non-canonical NF-κB pathway in immunity and inflammation. Nat Rev Immunol. 2017;17(9):545–58.
O’Shea JJ, Plenge R. JAK and STAT signaling molecules in immunoregulation and immune-mediated disease. Immunity. 2012;36(4):542–50.
Arthur JS, Ley SC. Mitogen-activated protein kinases in innate immunity. Nat Rev Immunol. 2013;13(9):679–92.
Ahn Y, Hwang JH, Zheng Z, Bang D, Kim DY. Enhancement of Th1/Th17 inflammation by TRIM21 in Behcet’s disease. Sci Rep. 2017;7(1):3018.
Bhakta BB, Brennan P, James TE, Chamberlain MA, Noble BA, Silman AJ. Behçet’s disease: evaluation of a new instrument to measure clinical activity. Rheumatology (Oxford). 1999;38(8):728–33.
Jabs DA, Nussenblatt RB, Rosenbaum JT. Standardization of uveitis nomenclature for reporting clinical data. Results of the First International Workshop. Am J Ophthalmol. 2005;140(3):509–16.
Assarsson E, Lundberg M, Holmquist G, Björkesten J, Thorsen SB, Ekman D, Eriksson A, Rennel Dickens E, Ohlsson S, Edfeldt G, et al. Homogenous 96-plex PEA immunoassay exhibiting high sensitivity, specificity, and excellent scalability. PLoS one. 2014;9(4):e95192.
Yu G, Wang LG, Han Y, He QY. clusterProfiler: an R package for comparing biological themes among gene clusters. OMICS. 2012;16(5):284–7.
Verrou KM, Vlachogiannis NI, Ampatziadis-Michailidis G, Moulos P, Pavlopoulos GA, Hatzis P, Kollias G, Sfikakis PP. Distinct transcriptional profile of blood mononuclear cells in Behçet’s disease: insights into the central role of neutrophil chemotaxis. Rheumatology (Oxford). 2021;60(10):4910–9.
Todaro M, Zerilli M, Triolo G, Iovino F, Patti M, Accardo-Palumbo A, di Gaudio F, Turco MC, Petrella A, de Maria R, et al. NF-kappaB protects Behçet’s disease T cells against CD95-induced apoptosis up-regulating antiapoptotic proteins. Arthritis Rheum. 2005;52(7):2179–91.
Bonizzi G, Karin M. The two NF-kappaB activation pathways and their role in innate and adaptive immunity. Trends Immunol. 2004;25(6):280–8.
Manou-Stathopoulou S, Lewis MJ. Diversity of NF-κB signalling and inflammatory heterogeneity in rheumatic autoimmune disease. Semin Immunol. 2022;58:101649.
Simmonds RE, Foxwell BM. Signalling, inflammation and arthritis: NF-kappaB and its relevance to arthritis and inflammation. Rheumatology (Oxford). 2008;47(5):584–90.
Huang X, Yang Y. Targeting the TLR9-MyD88 pathway in the regulation of adaptive immune responses. Expert Opin Ther Targets. 2010;14(8):787–96.
Stanbery AG, Newman ZR, Barton GM. Dysregulation of TLR9 in neonates leads to fatal inflammatory disease driven by IFN-γ. Proc Natl Acad Sci USA. 2020;117(6):3074–82.
Davies R, Sarkar I, Hammenfors D, Bergum B, Vogelsang P, Solberg SM, Gavasso S, Brun JG, Jonsson R, Appel S. Single cell based phosphorylation profiling identifies alterations in toll-like receptor 7 and 9 signaling in patients with primary Sjögren’s syndrome. Front Immunol. 2019;10:281.
Prinz M, Garbe F, Schmidt H, Mildner A, Gutcher I, Wolter K, Piesche M, Schroers R, Weiss E, Kirschning CJ, et al. Innate immunity mediated by TLR9 modulates pathogenicity in an animal model of multiple sclerosis. J Clin Investig. 2006;116(2):456–64.
Hosseininejad Z, Sharif M, Sarvi S, Amouei A, Hosseini SA, Nayeri Chegeni T, Anvari D, Saberi R, Gohardehi S, Mizani A, et al. Toxoplasmosis seroprevalence in rheumatoid arthritis patients: a systematic review and meta-analysis. PLoS Negl Trop Dis. 2018;12(6):e0006545.
Wilcox MH, Powell RJ, Pugh SF, Balfour AH. Toxoplasmosis and systemic lupus erythematosus. Ann Rheum Dis. 1990;49(4):254–7.
Sangaré LO, Yang N, Konstantinou EK, Lu D, Mukhopadhyay D, Young LH, Saeij JPJ. Toxoplasma GRA15 Activates the NF-κB Pathway through interactions with TNF receptor-associated factors. mBio. 2019;10(4):e00808-19.
Chen W, Cooper NR. Epstein-Barr virus nuclear antigen 2 and latent membrane protein independently transactivate p53 through induction of NF-kappaB activity. J Virol. 1996;70(7):4849–53.
Cassetta L, Fragkogianni S, Sims AH, Swierczak A, Forrester LM, Zhang H, Soong DYH, Cotechini T, Anur P, Lin EY, et al. Human tumor-associated macrophage and monocyte transcriptional landscapes reveal cancer-specific reprogramming, biomarkers, and therapeutic targets. Cancer Cell. 2019;35(4):588-602.e510.
Zhong Z, Liao W, Gao Y, Su G, Feng X, Yang P. Evaluation of sensitivity and specificity of diagnostic criteria for Behçet’s disease in the absence of a gold standard. Rheumatology (Oxford). 2022;61(9):3667–76.
Aridogan BC, Yildirim M, Baysal V, Inaloz HS, Baz K, Kaya S. Serum levels of IL-4, IL-10, IL-12, IL-13 and IFN-gamma in Behçet’s disease. J Dermatol. 2003;30(8):602–7.
Xu J, Qin Y, Chang R, Tan H, Wang Q, Su G, Cao Q, Kijlstra A, Yang P. Aqueous cytokine levels in four common uveitis entities. Int Immunopharmacol. 2020;78:106021.
Ireland SJ, Monson NL, Davis LS. Seeking balance: potentiation and inhibition of multiple sclerosis autoimmune responses by IL-6 and IL-10. Cytokine. 2015;73(2):236–44.
Bedke T, Muscate F, Soukou S, Gagliani N, Huber S. Title: IL-10-producing T cells and their dual functions. Semin Immunol. 2019;44:101335.
Biswas S, Bieber K, Manz RA. IL-10 revisited in systemic lupus erythematosus. Front Immunol. 2022;13:970906.
Cui X, Liu CM, Liu QB. FCRL3 promotes IL-10 expression in B cells through the SHP-1 and p38 MAPK signaling pathways. Cell Biol Int. 2020;44(9):1811–9.
Kochi Y, Yamada R, Suzuki A, Harley JB, Shirasawa S, Sawada T, Bae SC, Tokuhiro S, Chang X, Sekine A, et al. A functional variant in FCRL3, encoding Fc receptor-like 3, is associated with rheumatoid arthritis and several autoimmunities. Nat Genet. 2005;37(5):478–85.
Li K, Zhao M, Hou S, Du L, Kijlstra A, Yang P. Association between polymorphisms of FCRL3, a non-HLA gene, and Behçet’s disease in a Chinese population with ophthalmic manifestations. Mol Vis. 2008;14:2136–42.
Héja D, Kocsis A, Dobó J, Szilágyi K, Szász R, Závodszky P, Pál G, Gál P. Revised mechanism of complement lectin-pathway activation revealing the role of serine protease MASP-1 as the exclusive activator of MASP-2. Proc Natl Acad Sci USA. 2012;109(26):10498–503.
Rutland JW, Gill CM, Loewenstern J, Arib H, Pain M, Umphlett M, Kinoshita Y, McBride RB, Bederson J, Donovan M, et al. NF2 mutation status and tumor mutational burden correlate with immune cell infiltration in meningiomas. Cancer Immunol Immunother. 2021;70(1):169–76.
Maciel-Silva P, Caldeira I, de Assis SI, Carreira ACO, Siqueira FR, Antonioli E, Goldberg AC, Belizário JE, Garay-Malpartida HM. FAM3B/PANDER inhibits cell death and increases prostate tumor growth by modulating the expression of Bcl-2 and Bcl-X(L) cell survival genes. BMC Cancer. 2018;18(1):90.
Lau Q, Scheithauer B, Kovacs K, Horvath E, Syro LV, Lloyd R. MGMT immunoexpression in aggressive pituitary adenoma and carcinoma. Pituitary. 2010;13(4):367–79.
Seyahi E. Phenotypes in Behçet’s syndrome. Intern Emerg Med. 2019;14(5):677–89.
Vreeken D, Bruikman CS, Stam W, Cox SML, Nagy Z, Zhang H, Postma RJ, van Zonneveld AJ, Hovingh GK, van Gils JM. Downregulation of endothelial plexin A4 under inflammatory conditions impairs vascular integrity. Front Cardiovasc Med. 2021;8:633609.
Acknowledgements
The authors had nothing to disclose.
Funding
This study was supported by the Major Program of Medical Science and Technology Project of Health Commission of Henan Province (SBGJ202101011), the Talent Development Program for the Medical College of Zhengzhou University, the National Natural Science Foundation Key Program (82230032), the National Natural Science Foundation Project (82101108), and the Medical Scientific and Technological Project of Henan Province (SBGJ2020003031).
Author information
Authors and Affiliations
Contributions
PY and HL conceived the idea and designed the study. PY, HL, FL, and PZ contributed to collecting the plasma and clinical data. HL, PZ, XX, and YZ performed the experiments and analyzed the data. HL, NL, and LD did the literature search. HL wrote the manuscript. PY, PZ, and FL reviewed data interpretation and edited the manuscript. All authors reviewed the manuscript. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Ethics Committee of the First Affiliated Hospital of Zhengzhou University. All the procedures were performed in accordance with the Declaration of Helsinki.
Informed consent was obtained from all patients before participation.
Consent for publication
The authors affirm that human research participants provided informed consent for publication of all proteomic data in Supplementary Table S2.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Supplementary Figure S1.
(a) The quality control of the sample. The red color represents the failure of quality control. (b) Volcano plot of DEPs (c) The protein-protein interaction (PPI) network of 43 DEPs.
Additional file 2: Supplementary Figure S2.
Enriched KEGG pathways associated with infection.
Additional file 3: Supplementary Figure S3.
Comparison of the expression of the biomarkers between BD and HC in the validation cohort.
Additional file 4: Supplementary Figure S4.
The correlation between biomarkers and disease activity.
Additional file 5: Supplementary Figure S5.
The correlation between biomarkers and disease duration.
Additional file 6: Supplementary Figure S6.
Comparison of the expression level between treated and non-treated groups in BD patients.
Additional file 7: Supplementary Figure S7.
The correlation between the expression level of proteins and disease duration.
Additional file 8: Supplementary Figure S8.
Comparison of the expression level of PLXNA4 between BDU and BDNU in the validation cohort.
Additional file 9: Supplementary Table S1.
Clinical features of 27 Behcet’s disease (BD) patients
Additional file 10: Supplementary Table S2.
Comparison of immune-related proteins profile between BD and HC.
Additional file 11: Supplementary Table S3.
The performance of five machine learning models in the training cohort.
Additional file 12: Supplementary Table 4.
Comparison of immune-related proteins expression level between treated and non-treated groups in BD patients.
Additional file 13: Supplementary Table S5.
Comparison of the differential expression of immune- related proteins between Behcet’s disease (BDU) with and without uveitis (BDNU).
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Liu, H., Zhang, P., Li, F. et al. Identification of the immune-related biomarkers in Behcet’s disease by plasma proteomic analysis. Arthritis Res Ther 25, 92 (2023). https://doi.org/10.1186/s13075-023-03074-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13075-023-03074-y