
Abstract
Microglia are increasingly shown to be key players in neuron development and synapse connectivity. However, the underlying mechanisms by which microglia regulate neuron function remain poorly understood in part because such analysis is challenging in the brain where neurons and synapses are intermingled and connectivity is only beginning to be mapped. Here, we discuss the features and function of microglia in the ordered mammalian retina where the laminar organization of neurons and synapses facilitates such molecular studies. We discuss microglia origins and consider the evidence for molecularly distinct microglia subpopulations and their potential for differential roles with a particular focus on the early stages of retina development. We then review the models and methods used for the study of these cells and discuss emerging data that link retina microglia to the genesis and survival of particular retina cell subtypes. We also highlight potential roles for microglia in shaping the development and organization of the vasculature and discuss cellular and molecular mechanisms involved in this process. Such insights may help resolve the mechanisms by which retinal microglia impact visual function and help guide studies of related features in brain development and disease.
Similar content being viewed by others


Highlights
-
Microglia maturation is highly specified in the retina.
-
Microglia play potential roles in vascularization, neuron birth and survival, and synapse refinement.
-
Diverse microglia subpopulations found in retina display distinct features.
Background
Microglia are the resident immune cells of the central nervous system (CNS), and emerging work implicates these cells in shaping diverse features of neural development, connectivity, and homeostasis (reviewed in [1,2,3,4]). However, whether and how particular neuron or synapse types are targeted by microglia and the functional consequences of these interactions are less well described. It has been difficult to answer these questions because circuits in the brain are complex and we know relatively little about them. In this review, we discuss known microglia interactions with neurons in the accessible and well-mapped neural circuits of the mammalian retina. In the first part of the review, we present an in-depth description of the features of retina microglia and discuss their origins, localization, and organization during development. We also review evidence for microglia subpopulations and present an atlas of microglial biomarkers over development. In the second part, we discuss the functions of microglia, with a focus on their roles in modulating neurogenesis and development, particularly regarding retinal ganglion cells and astrocytes. In turn, these processes may influence novel roles for microglia in modulating neurovascular organization. Finally, we provide perspectives on key goals for future research, which include potential roles for microglia subpopulations and elucidation of mechanisms by which particular synapses are spared or removed. Continued study of microglia-specific functions in the retina may help inform related studies in the brain and provide unique opportunities to develop microglia targeted treatment strategies in diverse neurological diseases.
Main text
Part 1: features of retinal microglia
Microglia origin in the retina
Microglia originate from primitive yolk sac progenitors [5, 6]. Their development and survival are regulated by several known transcription factors and cytokine receptors (Table 1). Among these, the transcription factor PU.1 (also known as spleen focus forming proviral integration oncogene, SPI1) plays an important role in microglia development in part through its binding partner interferon regulatory factor 8 (IRF8) [7, 13,14,15,16]. Pu.1-deficient mice lack microglia, circulating monocytes, and tissue macrophages due to a reduction in early myeloid progenitors, while IRF8-deficent mice display defects in myeloid cell maturation [13, 14]. Microglia genesis is also regulated by the macrophage colony-stimulating factor receptor CSF1R. CSF1R expression on microglia is maintained throughout development. Consistent with the requirement for CSF1R expression, Csf1r knockout mice lack microglia in addition to yolk sac macrophages and osteoclasts [8,9,10]. Finally, animals lacking toll-like receptor 4 (TLR4) display reduced bipolar cell numbers and altered bipolar cell dendritic density, in addition to loss of microglia in the retina. These changes correlate with a significant reduction in retinal function, suggesting a key role for TLR4 in mediating visual function. However, whether microglia are causal to these alterations remains unclear [12].
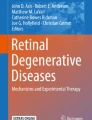
After they differentiate, microglia home to the CNS. Microglia can be identified in mouse brain rudiment as early as embryonic day (E)8.5 ~ E9.5. They are thought to migrate to the CNS via the embryonic circulatory system as mice that lack the sodium calcium exchanger 1 (Ncx-1) have defective blood circulation and microglia fail to enter the brain [9]. The origins of microglia in the retina and their precise developmental arrival have been less well studied. They are present in human retina by 10 weeks gestation and in mouse retina by E11.5, though it is likely they arrive even earlier [17, 18]. Similar timing has been documented in other species (E7 in quail, [19]; and at E12 in rat, [20]). Two waves of retinal microglia infiltration have been proposed based on the spatiotemporal localization of these cells. The first wave happens early in development prior to vascularization (Fig. 1a). At this time, microglia are thought to enter the retina by either: 1) crossing the vitreal retina surface; or 2) migrating from non-neural ciliary regions in the periphery [17, 18, 21, 22]. A second wave of infiltration has been proposed after blood vessels have formed through invasion from the optic disc or via blood vessels themselves [23]. Since much of this evidence is correlative, firm documentation of the timing and routes by which microglia enter the retina awaits more contemporary lineage tracing approaches.

Schematic of microglia development in mouse retina. a. Timeline of microglia entry to the retina. Microglia are derived from primitive yolk sac progenitors and are thought to enter the CNS via the circulatory system. Microglia have been documented in the developing murine retina at E11.5 but may be present earlier. Two waves of retinal microglia infiltration have been proposed. The first wave occurs embryonically and may involve microglia entry through the vitreal retina surface or migration from the ciliary region. A second wave may involve microglia infiltration from the optic disc or via blood vessels. b. Schematic of the adult retina. Rod (cyan) and cone (light purple) photoreceptors reside in the outer nuclear layer (ONL) and form connections with interneurons in the outer plexiform layer (OPL). Light induced signals are then relayed to neurons in the inner nuclear layer (INL), which is comprised of horizontal cells (dark blue), Müller glia (yellow), cone and rod bipolar cells (light and dark green), and amacrines (brown). Retinal ganglion cells (magenta) receive this information through synapses in the inner plexiform layer (IPL). Their somas reside in the ganglion cell layer (GCL) along with displaced amacrine cells (not pictured). Microglia cell are found predominately in the inner retina and are largely restricted to the synaptic layers
Microglia location and lamination in the retina
Microglia entry into the retina coincides with retinal neuron differentiation. Retinal neurons are derived from a precursor pool of retinal progenitor cells (RPCs) that divide to give rise to the five main types of retinal neurons: photoreceptors, bipolars, amacrines, horizontal cells, and retinal ganglion cells. As these neurons mature they become ordered into three cellular and two synaptic layers. Photoreceptors comprise the outer nuclear layer (ONL) and relay information through synapses in the outer plexiform layer (OPL) to inner retina neurons (horizontal, bipolar, and amacrine cells). Bipolar and amacrine cells synapse with retinal ganglion cells in the inner plexiform layer (IPL) (Fig. 1b). Microglia comprise 0.2% of total retinal cells and are found in addition to two other retina glia types, astrocytes and Müller glia [24,25,26]. Interestingly, microglia are predominately located in the retinal synapse layers (Fig. 2a). The adult OPL contains ~ 47% of the microglial population, while 53% are found in the IPL (Li and Samuel, unpublished). It is perhaps telling that microglia localization tracks the spatial distribution of developing retina synapses. Synapses begin to emerge as early as E17 in the nascent IPL, and at this time 99% of microglia localize to this narrow region [27, 28]. This localization persists as synapses mature and are refined. At postnatal day (P)3, ~ 80% of microglia are localized to the developing IPL and ganglion cell layer (GCL), and at P9, microglia become present within the developing OPL. This pattern persists into adulthood, with microglia and their processes localizing predominately to the inner retina and OPL, while the ONL is largely devoid of these cells (Fig. 2a) [18, 29]. Thus, microglia are at the right time and place to regulate retina synapse refinement. In line with this idea, the absolute number of retina microglia correlates with the peak of retina synapse pruning. The numbers of retina microglia increase over the first postnatal week, reaching twice that of adult levels by P7 when outer and inner retina synapses area actively refined. Microglia numbers then steadily decrease until the fourth postnatal week when they reach steady state levels and the retina circuit is considered mature [18].

Spatiotemporal distribution of microglia in the developing mouse retina. a. Representative images showing distinct spatiotemporal localization patterns of microglia across retina development (E18, P3, P9, and P17) in CX3CR1GFP/+ mice. Microglia are highly enriched at E18 and P3 in the nascent IPL where synapses are developing. At P9, microglia also become present within the developing OPL. This pattern persists into adulthood. Blue, DAPI; green, microglia. Scale bar = 50 μm. b-c. Representative images (b, scale bar = 50 μm) and single cell reconstructions (c, scale bar = 10 μm) of microglia in whole mount preparations of CX3CR1GFP/+ retina across development (P0, P3, P9, and P20). At birth, retinal microglia are amoeboid but become progressively ramified as the retina matures
Microglia morphology
Morphological changes in microglia are thought to correlate in part with their functional states [30,31,32]. Ramified microglia are often referred to as ‘resting’ while amoeboid microglia are often referred to as ‘active’ [33]. These terms can be misleading, however, as live imaging suggests that microglia are structurally dynamic in both ramified and amoeboid morphologies, though the cellular functions they carry out may differ. Ramified microglia actively retract and extend their processes, monitor neurons, and are engaged in metabolite removal and clearance in the CNS (reviewed in [3, 34, 35]). In contrast, amoeboid microglia contain numerous lysosomes and phagosomes and are thought to be engaged in synapse, axon, or cell engulfment [36, 37]. Consistent with this idea, microglia appear amoeboid in the brain during development at the peak of cell and synapse remodeling and then shift to a ramified state in the first two postnatal weeks [38, 39]. This developmental shift in microglia morphology extends to the retina. At birth, retinal microglia are amoeboid and extend their processes towards the basal side of the retina but become progressively ramified as the retina matures (Fig. 2b, c) [18]. Shifts in microglia structure also occur in response to CNS injury or pathogen invasion, leading to the formation of reactive amoeboid microglia [40, 41]. The mechanisms through which microglia alter their structural states are not well understood. Koso et al. reported that the zinc finger transcription factor Sall1 is expressed specifically in amoeboid retina microglia and that deleting Sall1 can cause ramified microglia to adopt a more amoeboid appearance [42]. Continued efforts to understand how microglia achieve different structural states and how these states impact function may aid efforts to modulate microglia activity in development or disease.
Microglia markers and subpopulations
All microglial precursors express the common macrophage markers CX3 chemokine receptor 1 (CX3CR1) and ionized calcium binding adaptor molecule 1 (Iba1) [14, 43]. Microglia transiently express additional markers during development, including F4/80, isolectin, CD45, CD68, CD11b, and inducible nitric oxide synthase (iNOS) that are typically lost or down regulated in adult cells [6, 18, 43]. Common microglia biomarkers over development are summarized in Fig. 3 [6, 14, 44,45,46,47]. Whether microglia can be considered a group of related but distinct cell populations is an area of active investigation. One possibility is that individual microglia can display fluid cellular characteristics that vary according to developmental or disease states. Alternately, microglia may be comprised of physiologically distinct cell subsets. Progress toward resolving these questions has been somewhat challenging due to the dynamic nature of microglia, their ability to migrate, and the potential for molecular similarities between macrophages that may enter the CNS under some conditions and resident microglia populations [48, 49]. However, it is clear that antigenic, structural, and transcriptional differences exist between cohorts of microglia. For example, the cytokine IL-34 appears to demark spatially distinct populations of microglia in the retina. In normal adults, IL-34 negative microglia are mainly localized to the OPL, while IL-34 positive microglia are located in the IPL [50]. In the presence of neuron degeneration, however, both populations relocate to the retinal pigment epithelium (RPE) [50]. Retina microglia also show different levels of CD11c, CD11b, and TLR4 [11, 51, 52]. For example, CD11c appears more abundant on microglia that are localized to compromised retinal neurons [53]. Thus, it is tempting to speculate that different subsets of microglia might be tuned to perform niche specific functions or regulate specific neuron types or geographic areas of the CNS.

Microglia biomarkers over CNS development. A timeline is presented that summarizes biomarkers for microglia over development in the CNS. For example, Tie2 marks microglia progenitors as early as E7.5. As microglia mature they express other markers including Csf1r, CX3CR1, and Iba1. Single-cell RNA sequencing studies have also identified potential new markers such as Tmem119, Fcrls, P2ry12, and Clec4n
Several recent molecular and sequencing based profiling studies also support the presence of microglia subpopulations in brain and retina. These populations appear dynamic and vary with developmental time and the presence or absence of disease [54,55,56]. But some common features emerge: 1) microglia are among the most transcriptionally diverse cell types in the brain; 2) their activation states can be spatially distinct within both normal and abnormal CNS environments; and 3) developing microglia can share transcriptional similarities with those in aged or diseased environments [54,55,56]. In a particularly thorough study, Hammond et al. compared 76,000 individual microglia in the brain at P5 and P30 to those derived from normal, aged, and diseased adult brain [54]. This approach identified 9 transcriptional subpopulations of microglia that remained consistent across all ages and disease states. In addition, microglia derived from various regions of the developing brain showed more heterogeneity compared to those in the adult brain [54, 55]. Related studies in retina show a similar trend. Profiling of retina microglia over development revealed 6 microglia cell clusters and indicates that retinal microglia have distinct transcriptional states over development [57]. Comparison of retinal microglia to transcriptional data from brain microglia showed that a similar set of lineage specific factors are shared by both populations, suggesting that developing retina and brain microglia may be ontogenically similar. Finally, retinal microglia early in development share many common transcriptional features with retinal microglia in disease and aging, suggesting some parallels between these conditions [54]. Whether the microglia subsets in the retina and the brain represent parallel groups is presently unclear.
Part 2: function of retinal microglia
Methods to study microglia function
Developing good methods to specifically alter microglia presence or function poses several challenges. First, molecules expressed on microglia are often found on macrophages or other cell types making cell-specific approaches difficult to achieve. Second, genes required for microglia development are often critically involved in other aspects of animal maturation or survival. Third, because microglia can migrate and are capable of repopulation or self-renewal, cell ablation approaches often result in at least some residual microglia and depletion drugs must be continuously administered. Due to these issues, the interpretation of microglia functional studies must take into account the models and methods used. We thus will briefly discuss the pros and cons of available microglia depletion models used to study retina and brain microglia (Table 2).
One category of microglia manipulation models involves deleting various effector molecules, such as complement, which are thought to alter microglia function [63, 64]. These types of models can be useful because they have more limited developmental side effects and are supported by correlative evidence implicating microglia in the phenotypes observed. Yet, in many cases, global knockouts are used that are not specific to microglia and affect other cells and systems. Such approaches do not prove the necessity and sufficiency of microglia in the observed phenotypes. To overcome this, some groups generate microglia effector molecule knockouts by crossing a Cx3cr1-Cre line [65] to conditional lines [65,66,67,68] though it should be noted that other cell populations are also targeted in this approach [65].
Available models to deplete or delete microglia also have important caveats. Three common approaches are used to prevent microglia formation. Each of these involves deleting or modifying one of three genes required for lymphoid or myeloid cell lineage cell development: PU.1, transforming growth factor beta (TGF-β), or CSF1R. These approaches can achieve 98% microglia depletion in embryonic brain [9, 14, 58]. However, knocking out any one of these genes induces a host of additional physiologic changes that cloud the interpretation of results. Pu.1−/− null mice are born alive but die of severe septicemia within days. Pu.1−/− mice are not only devoid of parenchymal microglia in the brain, but also of circulating monocytes and tissue macrophages [14]. TGF-β1−/− mice develop a lethal autoinflammatory syndrome shortly after birth and die by 3–4 weeks of age [69]. Csf1r null mice (Csf1r −/−), Csf1 homozygous mutant mice (Csf1 op/op) and Csf1r specific osteoclast knockouts [TNF Receptor Superfamily Member 11a (Tnfrsf11acre):Csf1r fl/fl] show a lack of tooth eruption, have low body weight and growth rates, misshapen skulls, and bone defects and usually die within 30 days after birth [8, 69,70,71]. A new model of Csf1r modulation in which a Csf1r enhancer is deleted (Csf1rΔFIRE/ΔFIRE) appears to circumvent many of these issues. Csf1rΔFIRE/ΔFIRE mice lack macrophages and brain microglia and are healthy and fertile up to 9 months of age without the growth and developmental abnormalities reported in Csf1r−/− or Csf1 op/op rodents [59].
Given these issues, many researchers have utilized microglia depletion models. Two pharmacological approaches are commonly used. Drugs that inhibit CSF1R (including PLX3397, PLX5562, GW2580, and BLZ945) can be administered in chow, in water, or intraperitoneally to deplete microglia. In the brain, this can result in 90% microglia depletion in adults, and 99% depletion at E15 when pregnant mice are fed inhibitor containing chow [60, 72]. Alternatively, liposomes containing chlodronate can be administered in vivo or in vitro to kill microglia that engulf them. While useful, this method likely targets other phagocytes as well, and the efficiency of microglia depletion is quite low (40~70%) [73, 74]. Genetic models of microglia depletion are also widely used. In these systems, depletion is achieved through targeted expression of the diphtheria toxin receptor (iDTR) primarily through crossing iDTR animals to CX3CR1-CreER animals to generate CX3CR1-CreER-iDTR mice [75]. CX3CR1 is found on microglia, as well as all monocytes, intestinal macrophages and dendric cells, some NK cells, and activated T cells [76,77,78]. Thus, injecting this line with alternating doses of tamoxifen and diphtheria toxin can deplete microglia but also affects subsets of other immune cells [43]. When injections are initiated at P0, this model achieves 70% microglia depletion in the retina by P6 and 98% depletion by P10–14 [61]. In brain, 99 and 85% microglia depletion are achieved after drug administration in young (~ 30 days) and adult animals (6–8 weeks), respectively [10, 79]. Following the same principle, the 10% of microglia that are CD11b positive [80, 81] can be depleted using a CD11b-DTR model [62]. Though this approach also targets other immune cell populations [82, 83]. While useful, it is important to note that these models do not achieve complete ablation, and remaining numbers of microglia can vary from animal to animal. Since it is formally possible that a small fraction of microglia could accomplish the same task as many, it is difficult to interpret negative data. Many of these models also do not allow the study of early postnatal ages since high levels of microglia depletion are not achieved for several days. Finally, these models require continual drug administration to maintain low levels of microglia since these cells can repopulate locally or from the periphery [10, 84,85,86].
Finally, we note that removing microglia or altering their abilities may cause both remaining microglia and other cell types to adopt different phenotypes or functions [60, 87, 88]. For example, when microglia are depleted astrocytes appear to take on the ability to modulate their own numbers during development through self-engulfment [61]. Depletion also alters remaining microglia, enabling them to rapidly repopulate. This leads to replenishment of microglia numbers within 3–7 days after acute depletion in a range of depletion systems [10, 84,85,86]. Where do these new microglia come from and are they comprised of the same cells as the native population? Three possibilities have been proposed: 1) they differentiate from latent microglia progenitors; 2) they are derived from residual microglia; or 3) they proliferate from peripherally invading macrophages. Evidence exists for each of these alternatives. In brain, the majority of repopulating microglia are nestin-positive (a neuroectodermal neural stem cell marker), and fate mapping analysis documented a nestin-positive microglia population that appears involved in microglia repopulation [89]. In another study, the etiology of repopulating brain microglia was investigated by comparing a Nestin-CreER:Ai14 line and a CX3CR1-CreER:Ai14 line following depletion [86]. The repopulated microglia were positive for the CX3CR1 label but negative for the nestin label, suggesting that the new cells are derived from surviving microglia (< 1%) and that these cells transiently express nestin during proliferation. Similarly, in adult retina, residual endogenous CX3CR1+ microglia near the optic nerve head were shown to undergo rapid proliferation and colonize the retina using both the CX3CR1-CreER:tdTomato and CX3CR1-CreER:Ai14 lines [90, 91]. Still, other studies have found evidence for cells that bear hallmarks of peripherally invading macrophages. Repopulating cells in which CD11b+ microglia had been eliminated expressed high levels of the peripheral macrophage markers CD45 and CCR2 and appeared associated with blood vessels [92]. Further, evidence suggests there could be two sources of repopulating retina microglia. In a CX3CR1-depletion model, microglia that repopulated the central retina appeard to be derived from residual microglia in the optic nerve, while microglia that repopulated the peripheral retina were suggested to arise from macrophages in the ciliary body or iris [91]. Whether repopulating microglia are transcriptionally, molecularly, or functionally similar to the native population remains an open question.
Microglia and retinal vascularization
In mouse, as in human, there are two phases of vascular growth in the eye. In the first phase, hyaloid vessels extend from the optic disk to the lens and supply blood and nutrients to the developing eye [93, 94]. Later in development, hyaloid vessels regress, and the retina develops its own independent vascular network [93]. Within the retina, three intraretinal vascular layers interdigitate distinct neural regions. The superficial plexus interleaves the GCL, the intermediate plexus ascends into the IPL, and the deep plexus is located within the OPL [93]. Each of these vessel layers has a characteristic location and branching pattern and thus are considered somewhat independent neurovascular units [95, 96].
Microglia have been implicated in both hyaloid vessel regression and intraretinal vascular formation in the eye via different mechanisms. Genetic or pharmacological ablation of vitreal macrophages or microglia have been shown to preserve the otherwise transient hyaloid vasculature. This process is thought to involve microglia-mediated apoptosis of vascular endothelial cells via WNT signaling [97]. After hyaloid vessels regress, endothelial cells proliferate and migrate radially into the retina from the center to the periphery, and microglia are thought to play supportive and guidance roles during this process [98]. Retinal microglia are closely apposed to endothelial tip cell filopodia, which guide blood vessel growth through the tissue [99,100,101,102]. In supporting studies, either genetic ablation or depletion of microglia reduces intraretinal vessel branching and density, while patterning was restored by intravitreal injection of exogeneous microglia [99, 103, 104]. In addition, microglia have recently been shown to regulate developmental death of astrocytes [61]. Since astrocytes form a reticular network that provides a substrate for angiogenesis and vessel patterning [105,106,107], microglia may also indirectly mediate vascular integrity through regulating astrocyte numbers [61]. However, it should be noted that the effects on blood vessel patterning in these microglia models are variable. In addition, there appear to be redundant mechanisms that compensate when microglia are not present which result in relatively normal adult blood vessel patterning in microglia deletion models [61, 104]. Finally, microglia have also been implicated in pathogenic retina angiogenesis. In diabetic retinopathy, abnormal intravitreal neovascularization coincides with an elevation of microglial TNF-α [108, 109]. Similar results were reported in an ischemic retinopathy model where activated retinal microglia were found to produce IL-1β, which maintained microglia activation and was associated with microvascular injury [110]. Given these observations, it is clear that much remains to be learned about the relationship between microglia and vasculature in the eye, particularly as microglia appear to alternatively promote developmental vascular regression, formation, or pathogenesis.
Microglia in neurogenesis and developmental cell death
Microglia have been implicated in developmental and adult neurogenesis, though the evidence remains somewhat controversial. In the retina, neurons are generated from RPCs at distinct ratios and times [111,112,113]. In zebrafish, targeted knockdown of Csf1r with RNAi delayed migration of microglia from the yolk sac to the retina and was correlated with a withdrawal of RPCs from the cell cycle, reduced neuron production, and microphthalmia [114]. The data in mice, however, are less clear. While application of a CSF1R inhibitor (PLX3397) [115] or minocycline (thought to reduce microglia activation, [116]) reduced RPC proliferation and viability, respectively, the numbers and gross organization of adult retina neuron cell bodies appear intact in the absence of microglia [61]. Finally, in the adult brain, microglia have been suggested to both enhance and inhibit neurogenesis, and results appear to vary depending on the model, brain region, disease state, and inflammatory and cytokine milieu [117,118,119,120].
More unambiguous studies have implicated microglia in developmental cell death of distinct retinal cell subsets. The majority of retina neuron and glia types are born in excess numbers and undergo a period of cell death from P0 to P13 [121]. While programed cell death accounts for the majority of this process [122], microglia-mediated phagocytosis plays a role in some cases. Depletion of microglia via the CX3CR1-CreER-iDTR system reduces astrocyte cell death, leading to anatomical changes in astrocyte distribution [61]. Similarly, microglia depletion in Csf1r−/− mice increased the developmental density of a subset of RGCs, and complement mediated engulfment was implicated in this process [57]. Though the evidence is more limited, microglia may also be involved in initiating, sensing, or responding to canonical neural apoptosis. In the developing brain, 60% of Purkinje cells that undergo apoptosis were engulfed by or in contact with microglia [123], and developmental neuronal death appeared to facilitate microglia entry and positioning into the developing zebrafish brain [124]. The list of molecular pathways that facilitate microglia-mediated phagocytosis of neurons or CNS debris is quite extensive (Table 3) and includes synaptotagmin-11 (Syt11, [125]), G protein-coupled receptor 34 (GPR34, [126]), Mer tyrosine kinase (MerTK, [127,128,129]) and spleen tyrosine kinase (Syk, [130]). It remains to be determined whether these pathways converge on a central microglia phagocytic process or whether their use is context dependent.
Microglia and synapse refinement
Microglia play active roles in synapse pruning, development, plasticity, and maintenance in the developing and adult brain [131,132,133]. Recent data suggest that the mechanisms involved in this process may be region specific. Microglia have been shown to regulate synapse refinement in the developing retinogeniculate system via the classical complement cascade proteins C1q and C3. Genetic deletion of these complement components blocks the capacity of microglia to properly remove synapses [1, 63]. However, in the developing barrel cortex, microglia appear to eliminate synapses via CX3CR1/CX3CL1 and signaling through a disintegrin and metalloproteinase domain-containing protein 10 (ADAM10). This metalloprotease cleaves CX3CL1 into a secreted form, and mice deficient in ADAM10, CX3CR1, or CX3CL1 show decreased synapse elimination and display reduced engulfment of synapse fragments by microglia [134]. Whether these pathways and processes extend to the retina is not clear. When microglia are depleted at P5, neuron and synapse organization seem to be largely unaffected at P10 [61]. However, this negative data should be interpreted with caution since: 1) a significant fraction of retina synapse formation and remodeling occurs prior to P5; 2) the models tested thus far still retained a small fraction of microglia; and 3) visualizing microglia mediated synapse pruning at single neuron resolution may show that only particular subsets of neurons are affected. In line with these ideas, adult retina depleted of microglia using the CX3CR1-CreER-iDTR model show a loss of synapses in the outer plexiform layer over time, resulting in decreased retina function as measured by scotopic electroretinography (ERG) recordings [135]. Thus, microglia may play roles in maintaining synaptic integrity and function in the adult retina. Continued efforts to understand the role of microglia mediated synapse pruning in specific retinal neuron subsets will help resolve whether microglia may target specific cell types or synapses for removal.
Conclusions
Microglia are a fascinating cell type with the potential to modulate or modify neuron development, survival, connectivity, and vascularization (Fig. 4). Studies in the retina and the brain are beginning to shed light on these processes and the mechanisms involved, but this enigmatic cell type still holds several key mysteries, including: 1) how do microglia home to the CNS and monitor and regulate their number and patterning; 2) do microglia subpopulations play region or cell-type specific roles in early neural development and neurodevelopmental disorders; 3) what are the molecular mechanisms by which microglia mediate synaptic refinement of specific neurons or synapse types; and 4) what are the interactions or signals that neurons provide to microglia that encode neuron or synapse engulfment versus sparing? Future studies that decipher these and related questions will not only enable a better fundamental understanding of neurobiology but also may provide untapped opportunities for treatment strategies aimed at preventing or reversing diverse types of neural diseases.

Proposed roles of microglia in the developing retina. Microglia play important roles in phagocytosis, vascularization, and neurogenesis through distinct mechanisms during retina development. These include modulation of both hyaloid vessel regression and intraretinal vascular patterning, regulation of the numbers of astrocytes and some RGC subsets, and RPC cycling. Roles for microglia in retina synapse pruning have also been proposed, though direct evidence for these pathways awaits further study
Availability of data and materials
Not applicable.
Abbreviations
- ADAM10:
-
a disintegrin and metalloproteinase domain-containing protein 10
- CNS:
-
central nervous system
- CSF1R:
-
colony-stimulating factor one receptor
- CX3CR1:
-
CX3 chemokine receptor 1
- DTR:
-
Diphtheria toxin receptor
- E:
-
Embryonic day
- ERG:
-
Electroretinography
- GCL:
-
Ganglion cell layer
- GPR34:
-
G protein-coupled receptor 34
- Iba1:
-
Ionized calcium binding adaptor molecule 1
- INL:
-
Inner nuclear layer
- IPL:
-
Inner plexiform layer
- IRF-8:
-
Interferon regulatory factor 8
- MerTK:
-
Mer tyrosine kinase
- Ncx-1:
-
Sodium calcium exchanger 1
- ONL:
-
Outer nuclear layer
- OPL:
-
Outer plexiform layer
- P:
-
Postnatal day
- PU.1:
-
PU box binding protein
- RPCs:
-
Retinal progenitor cells
- RPE:
-
Retinal pigment epithelium
- SPI1:
-
Spleen focus forming proviral integration oncogene
- Syk:
-
Spleen tyrosine kinase
- Syt11:
-
Synaptotagmin-11
- TGF-β:
-
Transforming growth factor beta
- TLR4:
-
Toll-like receptor 4
- Tnfrsf11a:
-
TNF Receptor Superfamily Member 11a
References
Schafer DP, Lehrman EK, Kautzman AG, Koyama R, Mardinly AR, Yamasaki R, et al. Microglia sculpt postnatal neural circuits in an activity and complement-dependent manner. Neuron. 2012;74(4):691–705.
Li Q, Barres BA. Microglia and macrophages in brain homeostasis and disease. Nat Rev Immunol. 2018;18(4):225–42.
Colonna M, Butovsky O. Microglia function in the central nervous system during health and Neurodegeneration. Annu Rev Immunol. 2017;35:441–68.
Sierra A, Abiega O, Shahraz A, Neumann H. Janus-faced microglia: beneficial and detrimental consequences of microglial phagocytosis. Front Cell Neurosci. 2013;7:6.
Ashwell K. Microglia and cell death in the developing mouse cerebellum. Brain Res Dev Brain Res. 1990;55(2):219–30.
Alliot F, Godin I, Pessac B. Microglia derive from progenitors, originating from the yolk sac, and which proliferate in the brain. Brain Res Dev Brain Res. 1999;117(2):145–52.
McKercher SR, Torbett BE, Anderson KL, Henkel GW, Vestal DJ, Baribault H, et al. Targeted disruption of the PU.1 gene results in multiple hematopoietic abnormalities. EMBO J. 1996;15(20):5647–58.
Dai XM, Ryan GR, Hapel AJ, Dominguez MG, Russell RG, Kapp S, et al. Targeted disruption of the mouse colony-stimulating factor 1 receptor gene results in osteopetrosis, mononuclear phagocyte deficiency, increased primitive progenitor cell frequencies, and reproductive defects. Blood. 2002;99(1):111–20.
Ginhoux F, Greter M, Leboeuf M, Nandi S, See P, Gokhan S, et al. Fate mapping analysis reveals that adult microglia derive from primitive macrophages. Science. 2010;330(6005):841–5.
Bruttger J, Karram K, Wortge S, Regen T, Marini F, Hoppmann N, et al. Genetic cell ablation reveals clusters of local self-renewing microglia in the mammalian central nervous system. Immunity. 2015;43(1):92–106.
Dando SJ, Naranjo Golborne C, Chinnery HR, Ruitenberg MJ, McMenamin PG. A case of mistaken identity: CD11c-eYFP(+) cells in the normal mouse brain parenchyma and neural retina display the phenotype of microglia, not dendritic cells. Glia. 2016;64(8):1331–49.
Noailles A, Kutsyr O, Maneu V, Ortuno-Lizaran I, Campello L, de Juan E, et al. The absence of toll-like receptor 4 mildly affects the structure and function in the adult mouse retina. Front Cell Neurosci. 2019;13:59.
Holtschke T, Lohler J, Kanno Y, Fehr T, Giese N, Rosenbauer F, et al. Immunodeficiency and chronic myelogenous leukemia-like syndrome in mice with a targeted mutation of the ICSBP gene. Cell. 1996;87(2):307–17.
Kierdorf K, Erny D, Goldmann T, Sander V, Schulz C, Perdiguero EG, et al. Microglia emerge from erythromyeloid precursors via Pu.1- and Irf8-dependent pathways. Nat Neurosci. 2013;16(3):273–80.
DeKoter RP, Walsh JC, Singh H. PU.1 regulates both cytokine-dependent proliferation and differentiation of granulocyte/macrophage progenitors. EMBO J. 1998;17(15):4456–68.
Beers DR, Henkel JS, Xiao Q, Zhao W, Wang J, Yen AA, et al. Wild-type microglia extend survival in PU.1 knockout mice with familial amyotrophic lateral sclerosis. Proc Natl Acad Sci U S A. 2006;103(43):16021–6.
Diaz-Araya CM, Provis JM, Penfold PL, Billson FA. Development of microglial topography in human retina. J Comp Neurol. 1995;363(1):53–68.
Santos AM, Calvente R, Tassi M, Carrasco MC, Martin-Oliva D, Marin-Teva JL, et al. Embryonic and postnatal development of microglial cells in the mouse retina. J Comp Neurol. 2008;506(2):224–39.
Martin-Estebane M, Navascues J, Sierra-Martin A, Martin-Guerrero SM, Cuadros MA, Carrasco MC, et al. Onset of microglial entry into developing quail retina coincides with increased expression of active caspase-3 and is mediated by extracellular ATP and UDP. PLoS One. 2017;12(8):e0182450.
Ashwell KW, Hollander H, Streit W, Stone J. The appearance and distribution of microglia in the developing retina of the rat. Vis Neurosci. 1989;2(5):437–48.
Provis JM, Diaz CM, Penfold PL. Microglia in human retina: a heterogeneous population with distinct ontogenies. Perspect Dev Neurobiol. 1996;3(3):213–22.
Marin-Teva JL, Calvente R, Cuadros MA, Almendros A, Navascues J. Circumferential migration of ameboid microglia in the margin of the developing quail retina. Glia. 1999;27(3):226–38.
Chen L, Yang P, Kijlstra A. Distribution, markers, and functions of retinal microglia. Ocul Immunol Inflamm. 2002;10(1):27–39.
Perry VH. Evidence for an amacrine cell system in the ganglion cell layer of the rat retina. Neuroscience. 1981;6(5):931–44.
Schlamp CL, Montgomery AD, Mac Nair CE, Schuart C, Willmer DJ, Nickells RW. Evaluation of the percentage of ganglion cells in the ganglion cell layer of the rodent retina. Mol Vis. 2013;19:1387–96.
Macosko EZ, Basu A, Satija R, Nemesh J, Shekhar K, Goldman M, et al. Highly parallel genome-wide expression profiling of individual cells using Nanoliter droplets. Cell. 2015;161(5):1202–14.
Pei YF, Rhodin JA. The prenatal development of the mouse eye. Anat Rec. 1970;168(1):105–25.
Sernagor E, Eglen SJ, Wong RO. Development of retinal ganglion cell structure and function. Prog Retin Eye Res. 2001;20(2):139–74.
Silverman SM, Wong WT. Microglia in the retina: roles in development, maturity, and disease. Annu Rev Vis Sci. 2018;4:45–77.
Kettenmann H, Hanisch UK, Noda M, Verkhratsky A. Physiology of microglia. Physiol Rev. 2011;91(2):461–553.
Harry GJ, Kraft AD. Microglia in the developing brain: a potential target with lifetime effects. Neurotoxicology. 2012;33(2):191–206.
Nayak D, Roth TL, McGavern DB. Microglia development and function. Annu Rev Immunol. 2014;32:367–402.
Ling EA, Wong WC. The origin and nature of ramified and amoeboid microglia: a historical review and current concepts. Glia. 1993;7(1):9–18.
Thomas WE. Brain macrophages: evaluation of microglia and their functions. Brain Res Brain Res Rev. 1992;17(1):61–74.
Fetler L, Amigorena S. Neuroscience. Brain under surveillance: the microglia patrol. Science. 2005;309(5733):392–3.
Kaur C, Dheen ST, Ling EA. From blood to brain: amoeboid microglial cell, a nascent macrophage and its functions in developing brain. Acta Pharmacol Sin. 2007;28(8):1087–96.
Kettenmann H, Kirchhoff F, Verkhratsky A. Microglia: new roles for the synaptic stripper. Neuron. 2013;77(1):10–8.
Perez-Pouchoulen M, VanRyzin JW, McCarthy MM. Morphological and Phagocytic Profile of Microglia in the Developing Rat Cerebellum. eNeuro. 2015;2(4).
Okajima T, Tsuruta F. Microglial dynamics during brain development. Neural Regen Res. 2018;13(2):222–3.
Davis EJ, Foster TD, Thomas WE. Cellular forms and functions of brain microglia. Brain Res Bull. 1994;34(1):73–8.
Kreutzberg GW. Microglia: a sensor for pathological events in the CNS. Trends Neurosci. 1996;19(8):312–8.
Koso H, Tsuhako A, Lai CY, Baba Y, Otsu M, Ueno K, et al. Conditional rod photoreceptor ablation reveals Sall1 as a microglial marker and regulator of microglial morphology in the retina. Glia. 2016;64(11):2005–24.
Schulz C, Gomez Perdiguero E, Chorro L, Szabo-Rogers H, Cagnard N, Kierdorf K, et al. A lineage of myeloid cells independent of Myb and hematopoietic stem cells. Science. 2012;336(6077):86–90.
Shigemoto-Mogami Y, Hoshikawa K, Goldman JE, Sekino Y, Sato K. Microglia enhance neurogenesis and oligodendrogenesis in the early postnatal subventricular zone. J Neurosci. 2014;34(6):2231–43.
Kierdorf K, Prinz M, Geissmann F, Gomez PE. Development and function of tissue resident macrophages in mice. Semin Immunol. 2015;27(6):369–78.
Erny D, Hrabe de Angelis AL, Jaitin D, Wieghofer P, Staszewski O, David E, et al. Host microbiota constantly control maturation and function of microglia in the CNS. Nat Neurosci. 2015;18(7):965–77.
Bennett ML, Bennett FC, Liddelow SA, Ajami B, Zamanian JL, Fernhoff NB, et al. New tools for studying microglia in the mouse and human CNS. Proc Natl Acad Sci U S A. 2016;113(12):1738–46.
Yin J, Valin KL, Dixon ML, Leavenworth JW. The role of microglia and macrophages in CNS homeostasis, autoimmunity, and Cancer. J Immunol Res. 2017;2017:5150678.
Martin E, Boucher C, Fontaine B, Delarasse C. Distinct inflammatory phenotypes of microglia and monocyte-derived macrophages in Alzheimer's disease models: effects of aging and amyloid pathology. Aging Cell. 2017;16(1):27–38.
O'Koren EG, Yu C, Klingeborn M, Wong AYW, Prigge CL, Mathew R, et al. Microglial function is distinct in different anatomical locations during retinal homeostasis and degeneration. Immunity. 2019;50(3):723–37 e7.
Huang W, Chamberlain CG, Sarafian RY, Chan-Ling T. MHC class II expression by beta2 integrin (CD18)-positive microglia, macrophages and macrophage-like cells in rabbit retina. Neuron Glia BiolNeuron Glia Biol. 2008;4(4):285–94.
M. K. Ko; S. Saraswathy; J. G. Parikh; G.-S. Wu; N. A. Rao. Toll-like receptor 4 in the retinal microglia leads to photoreceptor oxidative stress. ARVO Annual Meeting Abstract, April 2009.
Tang PH, Pierson MJ, Heuss ND, Gregerson DS. A subpopulation of activated retinal macrophages selectively migrated to regions of cone photoreceptor stress, but had limited effect on cone death in a mouse model for type 2 Leber congenital amaurosis. Mol Cell Neurosci. 2017;85:70–81.
Hammond TR, Dufort C, Dissing-Olesen L, Giera S, Young A, Wysoker A, et al. Single-cell RNA sequencing of microglia throughout the mouse lifespan and in the injured brain reveals complex cell-state changes. Immunity. 2019;50(1):253–71 e6.
Li Q, Cheng Z, Zhou L, Darmanis S, Neff NF, Okamoto J, et al. Developmental heterogeneity of microglia and brain myeloid cells revealed by deep single-cell RNA sequencing. Neuron. 2019;101(2):207–23 e10.
Ronning KE, Karlen SJ, Miller EB, Burns ME. Molecular profiling of resident and infiltrating mononuclear phagocytes during rapid adult retinal degeneration using single-cell RNA sequencing. Sci Rep. 2019;9(1):4858.
Anderson SR, Roberts JM, Zhang J, Steele MR, Romero CO, Bosco A, et al. Developmental apoptosis promotes a disease-related gene signature and Independence from CSF1R signaling in retinal microglia. Cell Rep. 2019;27(7):2002–13 e5.
Butovsky O, Jedrychowski MP, Moore CS, Cialic R, Lanser AJ, Gabriely G, et al. Identification of a unique TGF-beta-dependent molecular and functional signature in microglia. Nat Neurosci. 2014;17(1):131–43.
Rojo R, Raper A, Ozdemir DD, Lefevre L, Grabert K, Wollscheid-Lengeling E, et al. Deletion of a Csf1r enhancer selectively impacts CSF1R expression and development of tissue macrophage populations. Nat Commun. 2019;10(1):3215.
Rosin JM, Vora SR, Kurrasch DM. Depletion of embryonic microglia using the CSF1R inhibitor PLX5622 has adverse sex-specific effects on mice, including accelerated weight gain, hyperactivity and anxiolytic-like behaviour. Brain Behav Immun. 2018;73:682–97.
Puñal V, Paisley C, Brecha F, Lee M, Perelli R, Wang J et al. Large-scale death of retinal astrocytes during normal development is non-apoptotic and implemented by microglia. PLoS Biology, 2019:17(10).
Ueno M, Fujita Y, Tanaka T, Nakamura Y, Kikuta J, Ishii M, et al. Layer V cortical neurons require microglial support for survival during postnatal development. Nat Neurosci. 2013;16(5):543–51.
Stevens B, Allen NJ, Vazquez LE, Howell GR, Christopherson KS, Nouri N, et al. The classical complement cascade mediates CNS synapse elimination. Cell. 2007;131(6):1164–78.
Fonseca MI, Chu SH, Hernandez MX, Fang MJ, Modarresi L, Selvan P, et al. Cell-specific deletion of C1qa identifies microglia as the dominant source of C1q in mouse brain. J Neuroinflammation. 2017;14(1):48.
Yona S, Kim KW, Wolf Y, Mildner A, Varol D, Breker M, et al. Fate mapping reveals origins and dynamics of monocytes and tissue macrophages under homeostasis. Immunity. 2013:79–91.
Giera S, Luo R, Ying Y, Ackerman SD, Jeong SJ, Stoveken HM, et al. Microglial transglutaminase-2 drives myelination and myelin repair via GPR56/ADGRG1 in oligodendrocyte precursor cells. Elife. 2018;7:e33385.
Anderson SR, Zhang J, Steele MR, Romero CO, Kautzman AG, Schafer DP, et al. Complement targets newborn retinal ganglion cells for phagocytic elimination by microglia. J Neurosci. 2019;39(11):2025–40.
Sato-Hashimoto M, Nozu T, Toriba R, Horikoshi A, Akaike M, Kawamoto K, et al. Microglial SIRPα regulates the emergence of CD11c+ microglia and demyelination damage in white matter. Elife. 2019;8:e42025.
Kulkarni AB, Huh CG, Becker D, Geiser A, Lyght M, Flanders KC, et al. Transforming growth factor beta 1 null mutation in mice causes excessive inflammatory response and early death. Proc Natl Acad Sci U S A. 1993;90(2):770–4.
Marks SC Jr, Lane PW. Osteopetrosis, a new recessive skeletal mutation on chromosome 12 of the mouse. J Hered. 1976;67(1):11–8.
Jacome-Galarza CE, Percin GI, Muller JT, Mass E, Lazarov T, Eitler J, et al. Developmental origin, functional maintenance and genetic rescue of osteoclasts. Nature. 2019;568(7753):541–5.
Han J, Harris RA, Zhang XM. An updated assessment of microglia depletion: current concepts and future directions. Mol Brain. 2017;10(1):25.
Drabek T, Janata A, Jackson EK, End B, Stezoski J, Vagni VA, et al. Microglial depletion using intrahippocampal injection of liposome-encapsulated clodronate in prolonged hypothermic cardiac arrest in rats. Resuscitation. 2012;83(4):517–26.
Han X, Li Q, Lan X, El-Mufti L, Ren H, Wang J. Microglial depletion with Clodronate liposomes increases Proinflammatory cytokine levels, induces astrocyte activation, and damages blood vessel integrity. Mol Neurobiol. 2019;56(9):6184–96.
Goldmann T, Wieghofer P, Muller PF, Wolf Y, Varol D, Yona S, et al. A new type of microglia gene targeting shows TAK1 to be pivotal in CNS autoimmune inflammation. Nat Neurosci. 2013;16(11):1618–26.
Geissmann F, Manz MG, Jung S, Sieweke MH, Merad M, Ley K. Development of monocytes, macrophages, and dendritic cells. Science. 2010;327(5966):656–61.
Jung S, Aliberti J, Graemmel P, Sunshine MJ, Kreutzberg GW, Sher A, et al. Analysis of fractalkine receptor CX(3)CR1 function by targeted deletion and green fluorescent protein reporter gene insertion. Mol Cell Biol. 2000;20(11):4106–14.
Niess JH, Brand S, Gu X, Landsman L, Jung S, McCormick BA, et al. CX3CR1-mediated dendritic cell access to the intestinal lumen and bacterial clearance. Science. 2005;307(5707):254–8.
Parkhurst CN, Yang G, Ninan I, Savas JN, Yates JR 3rd, Lafaille JJ, et al. Microglia promote learning-dependent synapse formation through brain-derived neurotrophic factor. Cell. 2013;155(7):1596–609.
Murinello S, Moreno SK, Macauley MS, Sakimoto S, Westenskow PD, Friedlander M. Assessing retinal microglial phagocytic function in vivo using a flow Cytometry-based assay. J Vis Exp. 2016;116.
Greenhalgh AD, Zarruk JG, Healy LM, Baskar Jesudasan SJ, Jhelum P, Salmon CK, et al. Peripherally derived macrophages modulate microglial function to reduce inflammation after CNS injury. PLoS Biol. 2018;16(10):e2005264.
Dziennis S, Van Etten RA, Pahl HL, Morris D, Rothstein TL, Blosch CM, Perlmutter RM, Tenen DG. The CD11b promoter directs high-level expression of reporter genes in macrophages in transgenic mice. Blood. 1995;85(2):319–29.
Duffield JS, Forbes SJ, Constandinou CM, Clay S, Partolina M, Vuthoori S, Wu S, Lang R, Iredale JP. Selective depletion of macrophages reveals distinct, opposing roles during liver injury and repair. J Clin Invest. 2005;115(1):56–65.
Yao Y, Echeverry S, Shi XQ, Yang M, Yang QZ, Wang GY, et al. Dynamics of spinal microglia repopulation following an acute depletion. Sci Rep. 2016;6:22839.
Rice RA, Pham J, Lee RJ, Najafi AR, West BL, Green KN. Microglial repopulation resolves inflammation and promotes brain recovery after injury. Glia. 2017;65(6):931–44.
Huang Y, Xu Z, Xiong S, Sun F, Qin G, Hu G, et al. Repopulated microglia are solely derived from the proliferation of residual microglia after acute depletion. Nat Neurosci. 2018;21(4):530–40.
Ortega-Martinez S, Palla N, Zhang X, Lipman E, Sisodia SS. Deficits in enrichment-dependent neurogenesis and enhanced anxiety behaviors mediated by expression of Alzheimer's disease-linked Ps1 variants are rescued by microglial depletion. J Neurosci. 2019;39(34):6766–80.
De Luca SN, Sominsky L, Soch A, Wang H, Ziko I, Rank MM, et al. Conditional microglial depletion in rats leads to reversible anorexia and weight loss by disrupting gustatory circuitry. Brain Behav Immun. 2019;77:77–91.
Elmore MR, Najafi AR, Koike MA, Dagher NN, Spangenberg EE, Rice RA, et al. Colony-stimulating factor 1 receptor signaling is necessary for microglia viability, unmasking a microglia progenitor cell in the adult brain. Neuron. 2014;82(2):380–97.
Zhang Y, Zhao L, Wang X, Ma W, Lazere A, Qian HH, et al. Repopulating retinal microglia restore endogenous organization and function under CX3CL1-CX3CR1 regulation. Sci Adv. 2018;4(3):eaap8492.
Huang Y, Xu Z, Xiong S, Qin G, Sun F, Yang J, et al. Dual extra-retinal origins of microglia in the model of retinal microglia repopulation. Cell Discov. 2018;4:9.
Varvel NH, Grathwohl SA, Baumann F, Liebig C, Bosch A, Brawek B, et al. Microglial repopulation model reveals a robust homeostatic process for replacing CNS myeloid cells. Proc Natl Acad Sci U S A. 2012;109(44):18150–5.
Stahl A, Connor KM, Sapieha P, Chen J, Dennison RJ, Krah NM, et al. The mouse retina as an angiogenesis model. Invest Ophthalmol Vis Sci. 2010;51(6):2813.
McLeod DS, Hasegawa T, Baba T, Grebe R, Galtier d'Auriac I, Merges C, et al. From blood islands to blood vessels: morphologic observations and expression of key molecules during hyaloid vascular system development. Invest Ophthalmol Vis Sci. 2012;53(13):7912–27.
Rhodes JM, Simons M. The extracellular matrix and blood vessel formation: not just a scaffold. J Cell Mol Med. 2007;11(2):176–205.
Iadecola C. The neurovascular unit coming of age: a journey through neurovascular coupling in health and disease. Neuron. 2017;96(1):17–42.
Lobov IB, Rao S, Carroll TJ, Vallance JE, Ito M, Ondr JK, et al. WNT7b mediates macrophage-induced programmed cell death in patterning of the vasculature. Nature. 2005;437(7057):417–21.
Diez-Roux G, Lang RA. Macrophages induce apoptosis in normal cells in vivo. Development. 1997;124(18):3633–8.
Checchin D, Sennlaub F, Levavasseur E, Leduc M, Chemtob S. Potential role of microglia in retinal blood vessel formation. Invest Ophthalmol Vis Sci. 2006;47(8):3595–602.
Fantin A, Vieira JM, Gestri G, Denti L, Schwarz Q, Prykhozhij S, et al. Tissue macrophages act as cellular chaperones for vascular anastomosis downstream of VEGF-mediated endothelial tip cell induction. Blood. 2010:829–40.
Chen S, Tisch N, Kegel M, Yerbes R, Hermann R, Hudalla H, et al. CNS macrophages control neurovascular development via CD95L. Cell Rep. 2017;19(7):1378–93.
Penfold PL, Provis JM, Madigan MC, van Driel D, Billson FA. Angiogenesis in normal human retinal development: the involvement of astrocytes and macrophages. Graefes Arch Clin Exp Ophthalmol. 1990;228(3):255–63.
Ritter MR, Banin E, Moreno SK, Aguilar E, Dorrell MI, Friedlander M. Myeloid progenitors differentiate into microglia and promote vascular repair in a model of ischemic retinopathy. J Clin Invest. 2006;116(12):3266–76.
Kubota Y, Takubo K, Shimizu T, Ohno H, Kishi K, Shibuya M, et al. M-CSF inhibition selectively targets pathological angiogenesis and lymphangiogenesis. J Exp Med. 2009;206(5):1089–102.
O'Sullivan ML, Punal VM, Kerstein PC, Brzezinski JA, Glaser T, Wright KM, et al. Astrocytes follow ganglion cell axons to establish an angiogenic template during retinal development. Glia. 2017;65(10):1697–716.
Tao C, Zhang X. Retinal proteoglycans act as cellular receptors for basement membrane assembly to control astrocyte migration and angiogenesis. Cell Rep. 2016;17(7):1832–44.
Selvam S, Kumar T, Fruttiger M. Retinal vasculature development in health and disease. Prog Retin Eye Res. 2018;63:1–19.
Yossuck P, Yan Y, Tadesse M, Higgins RD. Dexamethasone alters TNF-alpha expression in retinopathy. Mol Genet Metab. 2001;72(2):164–7.
Yoshida S, Yoshida A, Ishibashi T. Induction of IL-8, MPC-1, and bFGF by TNF-α in retinal glial cells: implications for retinal neovascularization during post-ischemic inflammation. Graefes Arch Clin Exp Ophthalmol. 2004;242(5):409–13.
Rivera JC, Sitaras N, Noueihed B, Hamel D, Madaan A, Zhou T, et al. Microglia and interleukin-1beta in ischemic retinopathy elicit microvascular degeneration through neuronal semaphorin-3A. Arterioscler Thromb Vasc Biol. 2013;33(8):1881–91.
Cepko C. Intrinsically different retinal progenitor cells produce specific types of progeny. Nat Rev Neurosci. 2014;15(9):615–27.
Belliveau MJ, Cepko CL. Extrinsic and intrinsic factors control the genesis of amacrine and cone cells in the rat retina. Development. 1999;126(3):555–66.
Kay JN, Link BA, Baier H. Staggered cell-intrinsic timing of ath5 expression underlies the wave of ganglion cell neurogenesis in the zebrafish retina. Development. 2005;132(11):2573–85.
Huang T, Cui J, Li L, Hitchcock PF, Li Y. The role of microglia in the neurogenesis of zebrafish retina. Biochem Biophys Res Commun. 2012;421(2):214–20.
Kuse Y, Ohuchi K, Nakamura S, Hara H, Shimazawa M. Microglia increases the proliferation of retinal precursor cells during postnatal development. Mol Vis. 2018;24:536–45.
Ferrer-Martin RM, Martin-Oliva D, Sierra-Martin A, Carrasco MC, Martin-Estebane M, Calvente R, et al. Microglial activation promotes cell survival in Organotypic cultures of postnatal mouse retinal explants. PLoS One. 2015;10(8):e0135238.
Monje ML, Toda H, Palmer TD. Inflammatory blockade restores adult hippocampal neurogenesis. Science. 2003;302(5651):1760–5.
Cunningham C. Microglia and neurodegeneration: the role of systemic inflammation. Glia. 2013;61(1):71–90.
Ramesh G, MacLean AG, Philipp MT. Cytokines and chemokines at the crossroads of neuroinflammation, neurodegeneration, and neuropathic pain. Mediat Inflamm. 2013;2013:480739.
Wang WY, Tan MS, Yu JT, Tan L. Role of pro-inflammatory cytokines released from microglia in Alzheimer's disease. Ann Transl Med. 2015;3(10):136.
Young RW. Cell death during differentiation of the retina in the mouse. J Comp Neurol. 1984;229(3):362–73.
Vecino E, Acera A. Development and programed cell death in the mammalian eye. Int J Dev Biol. 2015;59(1–3):63–71.
Marín-Teva JL, Dusart I, Colin C, Gervais A, van Rooijen N, Mallat M. Microglia promote the death of developing Purkinje cells. Neuron. 2004;41(4):535–47.
Casano AM, Albert M, Peri F. Developmental apoptosis mediates entry and positioning of microglia in the Zebrafish brain. Cell Rep. 2016;16(4):897–906.
Du C, Wang Y, Zhang F, Yan S, Guan Y, Gong X. Synaptotagmin-11 inhibits cytokine secretion and phagocytosis in microglia. Glia. 2017;65(10):1656–67.
Preissler J, Grosche A, Lede V, Le Duc D, Krügel K, Matyash V, Szulzewsky F, Kallendrusch S, Immig K, Kettenmann H, Bechmann I, Schöneberg T, Schulz A. Altered microglial phagocytosis in GPR34-deficient mice. Glia. 2015;63(2):206–15.
Grommes C, Lee CY, Wilkinson BL, Jiang Q, Koenigsknecht-Talboo JL, Varnum B, Landreth GE. Regulation of microglial phagocytosis and inflammatory gene expression by Gas6 acting on the Axl/Mer family of tyrosine kinases. J NeuroImmune Pharmacol. 2008;3(2):130–40.
Caberoy NB, Alvarado G, Li W. Tubby regulates microglial phagocytosis through MerTK. J Neuroimmunol. 2012;252(1–2):40–8.
Nomura K, Vilalta A, Allendorf DH, Hornik TC, Brown GC. Activated microglia Desialylate and Phagocytose cells via neuraminidase, Galectin-3, and Mer tyrosine kinase. J Immunol. 2017;198(12):4792–801.
Scheib JL, Sullivan CS, Carter BD. Jedi-1 and MEGF10 signal engulfment of apoptotic neurons through the tyrosine kinase Syk. J Neurosci. 2012;32(38):13022–31.
Schafer DP, Stevens B. Phagocytic glial cells: sculpting synaptic circuits in the developing nervous system. Curr Opin Neurobiol. 2013;23:1034–40.
Schafer DP, Stevens B. Microglia function in central nervous system development and plasticity. Cold Spring Harb Perspect Biol. 2015;7(10):a020545.
Hong S, Dissing-Olesen L, Stevens B. New insights on the role of microglia in synaptic pruning in health and disease. Curr Opin Neurobiol. 2016;36:128–34.
Gunner G, Cheadle L, Johnson KM, Ayata P, Badimon A, Mondo E, Nagy MA, Liu L, Bemiller SM, Kim KW, Lira SA, Lamb BT, Tapper AR, Ransohoff RM, Greenberg ME, Schaefer A, Schafer DP. Sensory lesioning induces microglial synapse elimination via ADAM10 and fractalkine signaling. Nat Neurosci. 2019;22(7):1075–88.
Wang X, Zhao L, Zhang J, Fariss RN, Ma W, Kretschmer F, Wang M, Qian HH, Badea TC, Diamond JS, Gan WB, Roger JE, Wong WT. Requirement for microglia for the maintenance of synaptic function and integrity in the mature retina. J Neurosci. 2016;36(9):2827–42.
Acknowledgements
We thank members of our laboratory, Gretchen Diehl, and Wei Cao for scientific discussions and advice. This work was supported by the National Institutes of Health (NIH, R00AG044444, DP2EY02798, R56AG061808, and R01EY030458 to M.A.S.), the Cancer Prevention Research Institute of Texas (RR150005), the Brain Research Foundation, and the Ted Nash Foundation.
Funding
This work was supported by the National Institutes of Health (NIH, R00AG044444, DP2EY02798, R56AG061808, and R01EY030458 to M.A.S.), the Cancer Prevention Research Institute of Texas (RR150005), the Brain Research Foundation, and the Ted Nash Foundation.
Author information
Authors and Affiliations
Contributions
FL was the major contributor in designing the manuscript. DJ modified the manuscript and figures. MS edited the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Li, F., Jiang, D. & Samuel, M.A. Microglia in the developing retina. Neural Dev 14, 12 (2019). https://doi.org/10.1186/s13064-019-0137-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13064-019-0137-x