
Abstract
Background
Knee osteoarthritis (KOA) presents a prevalent orthopedic condition causing substantial impairment in the quality of life and imposing a significant societal and economic burden. Mesenchymal stromal/stem cells (MSCs), known for their regenerative properties and immunomodulatory effects, have emerged as a promising therapeutic avenue in regenerative medicine. Despite MSCs' therapeutic potential, their precise mechanisms of action in KOA remain underexplored.
Methods
Conducted as a randomized, open-label clinical trial, 20 patients will be enrolled, with 10 in the intervention group and 10 in the control group. The primary focus will be to explore the molecular mechanisms associated with MSC therapy. Biomarkers and gene expressions related to cartilage metabolism, inflammation, immune modulation, and pain in the synovial fluid, blood, and tissue samples will be analyzed. Patients will undergo pre- and post-treatment evaluations using patient-reported outcome measures (PROMs) and comprehensive clinical assessments.
Discussion
This is an exploratory study with the goal to provide comprehensive insights into the therapeutic effects of MSCs on a molecular level, potentially paving the way for optimized and more effective MSC-based therapies in the management of KOA, as well as furthering the development of novel treatment strategies.
Trial registration
ClinicalTrials.gov, NCT06078059. Registered on 5 October 2023.
Similar content being viewed by others


Background
Knee osteoarthritis (KOA) is one of the most common orthopedic diseases that can significantly impact the quality of life [1]. Among people over the age of 50, KOA is second only to cardiovascular disease in terms of diseases that cause long-term disability [2]. The disease not only involves a decrease in the patient’s quality of life but also represents a significant social and economic burden [3]. KOA is characterized by pathological changes in the cartilage, bone, synovium, ligaments, muscles, and periarticular fat, leading to joint dysfunction, pain, stiffness, functional limitation, and associated loss of daily activities (e.g., walking, exercise, etc.). The main risk factors for the development of KOA include age (33% of individuals older than 75 years suffer from symptomatic and radiologically diagnosed KOA), female sex, obesity, genetic factors, and major joint injuries. People suffering from KOA are accompanied by higher mortality and are characterized by an increased amount of sedentary lifestyle [3].
Mesenchymal stromal/stem cells (MSCs) originate from the mesodermal layer, from which the bone, muscle, fat, and other connective tissues develop during embryogenesis. In adults, MSCs represent a heterogeneous cell population, which also includes multipotent stem cells capable of differentiation into the cartilage, bone, and fat cells. They are often called adult stem cells, as they possess regenerative abilities and are often part of research in the field of regenerative medicine [4]. The most common biological sources for the manufacture of MSC-based therapeutics are the bone marrow, adipose tissue, umbilical cord tissue, and others. The cultivation of MSCs is a relatively simple and safe process, without major ethical concerns. MSCs are characterized by low or zero expression of molecules of the major histocompatibility complex (making them essentially “invisible” to immune recognition), which makes them useful even in an allogeneic environment. An additional phenotypic feature is the simultaneous expression of various markers, including CD73, CD90, and CD105, and the lack of expression of hematopoietic markers, such as CD45.
Although a certain part of the MSC population can differentiate into different cell types, there is a growing consensus that their main therapeutic action originates from paracrine effects through the secretion of various active biomolecules. In this way, factors secreted by MSCs can have angiogenic, anti-apoptotic, regenerative, and immunomodulatory effects [5]. Indeed, MSCs possess unique immunomodulatory effects among all types of stem cells. They can exert their action by expressing immunomodulatory enzymes such as indoleamine-2,3-dioxygenase (IDO) and inducible nitric oxide synthase (iNOS), immunosuppressive biomolecules such as prostaglandin E2 (PGE2) and hepatocyte growth factor (HGF), or by producing immunosuppressive cytokines, namely interleukin (IL)-10 and transforming growth factor (TGF)-β, or by expression of surface inhibitory molecules such as HLA-G, and programmed death ligand (PDL)-1 and PDL-2 [6]. Due to such an extensive repertoire of immunomodulatory mechanisms, MSCs can regulate the activity of several types of immune cells belonging to both innate and acquired immunity. These include monocytes/macrophages, as well as the most important antigen-presenting cells, dendritic cells (DCs). They can also suppress the activity of T and B lymphocytes, NK cells, neutrophils, and mast cells. On the other hand, MSCs have been shown to stimulate the formation of regulatory subsets of immune cells, such as regulatory T cells (Treg), tolerogenic DCs, as well as myeloid suppressor cells [7]. MSCs significantly inhibit the proliferation of T cells both in an allogeneic environment and after exposure to various mitogens [8, 9]. In cocultures with Th1 helper T cells, MSCs can greatly reduce the secretion of pro-inflammatory cytokines (e.g., IFN-γ and TNF-α) and increase the percentage of T cells that produce anti-inflammatory cytokines (e.g., IL-10), such as Tr1 cells [10]. They can also inhibit the activation of cytotoxic CD8 + T cells, resulting in a reduced response to allo-antigens and reduced Ag-specific lysis of allogeneic cells [11, 12]. All the abovementioned characteristics logically coincide with MSCs’ potential therapeutic efficacy in KOA, a pathology which is now known to be importantly accompanied with both innate and adaptive immune processes [13].
MSC-based treatment is one of the latest therapeutic approaches for KOA. Since their mechanisms of action are most likely multifaceted, they seem a suitable therapeutic candidate for KOA by merit of complex and versatile disease pathology. Although these cells are already naturally present in the synovial fluid, their number is too low for adequate differentiation and immunomodulation. After intra-articular administration, MSCs are known to be retained at the joint site and in adjacent bone marrow lesions [14, 15]. The use of MSCs for the treatment of KOA is becoming increasingly prevalent with a growing body of evidence endorsing their application, particularly for alleviating symptoms (e.g., pain) and improving joint function [16,17,18].
The main purpose of our study is to investigate the mechanisms of early action of allogeneic MSCs obtained from umbilical cord tissue in a cohort of patients with terminal KOA (Kellgren–Lawrence grade 4), scheduled for joint arthroplasty. In this regard, our main clinical question is what are the early molecular (as well as clinical) effects of allogeneic umbilical cord-derived MSCs in these patients. Therefore, we hypothesize that treatment will modulate biomarkers related to cartilage metabolism, inflammation, immune modulation, and pain in these patients.
Methods
Study objectives, design, and setting
The aim of the study is to evaluate pharmacological mechanisms at the molecular level, which could be associated with therapeutic benefit of MSC therapy. The study protocol was approved by the National Medical Ethics Committee, no. 0120–273/2022/3. The study is registered in www.clinicaltrials.gov database under identifier NCT06078059.
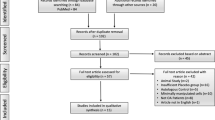
The research will be carried out at the Orthopedic Clinic of the University Medical Center (UMC) Ljubljana in cooperation with the Slovenian Institute of Transfusion Medicine (SITM). We will invite 20 patients (10 intervention group, 10 control group) to participate in the study, who will shortly be scheduled for knee arthroplasty due to primary or post-traumatic KOA at the Orthopedic Clinic of UMC Ljubljana. It is a randomized, single-center, open-label, pharmacological clinical study. The timeline of the study is presented in Fig. 1.

The study timeline
Randomization and blinding
Participants will be randomized into two groups in a 1:1 ratio. The randomization to either MSC or non-MSC group will be performed using a computer-assisted algorithm (www.randomizer.org). The allocation sequence will be generated by an independent researcher who is not involved in the enrollment or assignment of participants. The allocation sequence will be concealed until interventions are assigned to ensure unbiased participant assignment. Participants will be enrolled by study coordinators who will be blinded to the allocation sequence. After enrollment, the participants will be assigned to the intervention or control group by the independent researcher.
The study will not be blinded.
Inclusion of patients
Patients will be recruited during the routine preoperative assessment in the anesthesiology outpatient clinic, typically 4–6 weeks before the scheduled surgery. After the evaluation, once they have been approved as eligible for surgery by the anesthesiologist and have given their informed consent for the anesthesia, the study will be presented to those who will meet the basic inclusion criteria. If the patients agree, they will provide written informed consent to participate.
The patients will receive comprehensive explanations regarding the clinical trial, covering the following aspects: (1) the purpose of the study, (2) its research background, (3) the number of participants and duration of involvement, (4) the study procedures, (5) potential treatment risks, (6) anticipated benefits, (7) confidentiality and privacy protection measures, and (8) the voluntary nature of participation. Only after ensuring full comprehension of these points will each patient sign the informed consent form. Following consent, clinicians will record the patients’ baseline characteristics. The timeline of events is presented in Table 1.
Eligibility criteria
Patients scheduled for knee arthroplasty due to primary or post-traumatic KOA at the Orthopedic Clinic of UMC Ljubljana. Inclusion and exclusion criteria are presented in Table 2.
Pre- and post-treatment assessments
Demographic data, medical history, and baseline clinical status of the index knee will be recorded. The subjects will complete a package of patient-reported outcome measures (PROMs) questionnaires to evaluate patients’ perceived knee status, pain, functioning, and quality of life. The visual analog scale for pain assessment (VAS-P), Knee Injury and Osteoarthritis Outcome Score (KOOS), European Quality of Life in Five Dimensions Three-Level (EQ-5D-3L), and EuroQol self-rated health on visual analog scale (EQ-VAS) will be included [21,22,23]. At inclusion, the patients will be assigned consecutive numbers.
In both groups, an aspiration of the index knee in aseptic conditions will be performed initially to determine baseline synovial cartilage markers. Afterwards, the intervention group will receive an intra-articular infiltration of 20 million cultured allogeneic MSCs in the form of 4 ml cell dispersion through the same needle that aspiration was performed. After a short observation, both groups will be discharged to home care with instructions. Patients will receive a diary to record the level of pain on VAS-P twice daily (morning, evening) and any mild deviations in the knee status (e.g., swelling, stiffness, increased pain, etc.). Strict instructions and contact information will be given for any serious adverse events (e.g., fever, local signs of infection, allergies, etc.), which will be closely monitored. Upon admission, typically on the day before surgery, the patients will fill out the same package of PROMs questionnaires prior to the intervention.
On the day of the surgery, during the standard operative procedure of knee arthroplasty under general or spinal anesthesia, control samples of the synovial fluid, blood, and urine will be obtained, just before the start of the procedure with the joint closed. After the surgical exposure of the knee, three samples of the joint capsule and the resected cartilage surfaces will be collected. Both, the removed parts of the joint capsule and the resected articular surfaces, represent waste during the operative interventions; therefore, their collection will not affect the performance of the arthroplasty in any way. All samples will be immediately transferred to SITM for further processing in the appropriate conditions (using transport media and cooling elements). Samples will be systematically coded to conceal the patients’ identity outside the clinical facility. The presence of soluble analytes in the samples will be determined using the Luminex® multiplex method or the ELISA method. Real-time gene expression in chondrocyte and synoviocyte cells will be determined using the qRT-PCR method.
Objectives and outcome measures
The main objective of our study is to contribute to in-depth understanding of mechanisms of action of MSC use for KOA treatment. For this reason, we have selected key biomarkers that have had the strongest literature correlation with KOA using BIPED (Burden of disease, Investigative, Prognostic, Efficacy of intervention and Diagnostic) criteria [24,25,26]. We also predict that the impact of our results will not only carry an academic meaning but will also serve as a platform for future optimization of KOA-related approaches in regenerative medicine.
Primary outcome measures
-
1.
Soluble biomarker analysis with multiplex immunoassays (e.g., Luminex) in synovial fluid. The following biomarkers will be analyzed: FGF basic, TIMP-1, osteoprotegerin, adiponectin, CCL2, CD14, Dkk-1, IL-6, Leptin, MMP-3, MMP-9, sclerostin, Tenascin C, VCAM-1, BMP-2, CCL5, CD163, ICAM-1, IL-8, MMP-1, MMP-7, MMP-13, Syndecan-4, TNF-α, and VEGF.
-
2.
Soluble biomarker analysis using enzyme-linked immunosorbent assay (ELISA) in synovial fluid. The following biomarkers will be analyzed: aggrecan, COMP, hyaluronan, and PIIANP.
-
3.
Quantitative real-time PCR (qRT-PCR) analysis of gene expression in chondrocytes and synoviocytes. Analysis of gene expressions, which are associated with chondrocyte function (collagen type II (COL2), COL1, and SOX9), cartilage and synovia degradation (MMP-13, ADAMTS-4, ADAMTS-5), pain (NGF), and inflammation (IL-1β, IL-6, and TNF-α), will be performed.
Secondary outcome measures
-
4.
Knee Injury and Osteoarthritis Outcome Score (KOOS)
This knee-specific instrument measures patients’ perceived pain (9 items), other symptoms (7 items), function in daily living (17 items), function in sports and recreation (5 items), and knee-related quality of life (4 items). Scores range from 0 to 100, with a score of 0 indicating the worst possible knee status and 100 indicating no knee symptoms. Assessment will be performed 4–6 weeks prior to the surgery and at admission.
-
5.
Pain on visual analog scale (VAS-P)
This measure of pain intensity consists of a 10-point line, with endpoint 0 representing “no pain” and 10 “the worst pain imaginable”. Assessment will be performed 4–6 weeks prior to the surgery and at admission.
-
6.
European Quality of Life in Five Dimensions Three-Level (EQ-5D-3L) questionnaire
The system contains five dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Every dimension has three levels: no problems, some problems, and extreme problems. The respondent is asked to indicate his or her health state by ticking the box that marks the most appropriate level of problems in each dimension. Health states are converted into a single summary index by a formula that attaches values to each level in each dimension. Assessment will be performed 4–6 weeks prior to the surgery and at admission.
-
7.
EuroQol self-rated health on visual analog scale (EQ-VAS)
The assessment records the patient’s self-rated health on a vertical visual analog scale from 0 to 100, where 0 represents the worst health state imaginable and 100 represents the best health state imaginable. Assessment will be performed 4–6 weeks prior to the surgery and at admission.
-
8.
Serious adverse events (SAEs) monitoring
Safety will be monitored from day 0 (MSCs application) through up to 6 months after the surgery.
Intervention
The investigational medicinal product (IMP) will be based on umbilical cord-derived, allogeneic MSCs, prepared at the Slovenian Institute for Transfusion Medicine (SITM) according to validated standard operating procedures, also approved by the National Medical Ethics Committee (No. 0120–60/2018/7, approved on 24.4.2018). For the manufacture of IMP, the umbilical cord tissue, used as the primary biological source of MSCs, is first seeded during an ex vivo expansion protocol. After the initial 10–14 days, where the cells are cultured in passage 0, the adherent cells begin to proliferate exponentially, achieving adequate confluence within 7 days. Subsequently, the cells are harvested at an approximate 80% confluency and reseeded for additional expansion in passage 1. At the end of passage 1, the cells are harvested and then redistributed into identical aliquots to be cryopreserved as “off-the-shelf” units in the cryostorage facility at SITM. As such, the units are available for “per patient” order. For every patient, an aliquot of MSCs will be thawed and seeded in ex vivo cell culture for 3–5 days (passage 2) prior to application. This additional culturing in passage 2 ensures optimal cell numbers, cell viability, and functional fitness of the final cellular product. The final formulation will represent 5 × 106 MSCs/ml in a physiological solution supplemented with 0.5% human albumin. The cellular dispersion will be filled in syringes in 4 ml (20 × 106 cells overall). For application, an 18-G 1.2 × 50 mm hypodermic needle will be used.
In the intervention group, each patient will receive an intra-articular injection of 20 × 106 MSCs, without anesthesia. The injection of MSCs will be performed 4–6 weeks prior to the scheduled arthroplasty.
Termination guidelines
Termination of the study will proceed if serious adverse events (SAEs) will be observed during the intervention or up to the day of the surgery. Additionally, monitoring for SAEs will be performed up to 6 months after surgery. We will also consider as a discontinuation criterion any allergic reaction, infection at the injection site, or other local/systemic events determined as possibly/probably/surely related to MSC injection and graded grade 3 or higher according to CTCAE v5.0 (serious adverse reaction, SAR). In case of registration of a SAR, the PI of the study will notify the study coordinator within the time frame of 24 h, as well as the National Center for Pharmacovigilance of the Agency for Medicinal Products and Medical Devices of the Republic of Slovenia.
Adverse events
Adverse events (AEs) are occurrences of medical issues that arise from the time subjects or their guardians consent to participation until the conclusion of the study visit. These events encompass abnormal laboratory findings, symptoms, or diagnosed diseases. Each AE will be documented on a case report Form (CRF), accompanied by detailed clinical reports provided by the researcher.
Upon the potential onset of AEs, our priority is the well-being of the participants. We will administer appropriate treatment based on individual patient needs and assess whether to halt the clinical research. The PI is responsible for promptly notifying National Center for Pharmacovigilance of the Agency for Medicinal Products and Medical Devices of the Republic of Slovenia. A serious adverse event (SAE) report must be submitted within 24 h in writing, followed by a subsequent report to the National Medical Ethics Committee for further review.
Confidentiality
The patients will be identified only by code on all documents, which will be collected for data analysis. The responsibility for maintaining the log of subject identification data lies with the PI. No document leaving the research center shall contain the patient’s name or any other information that could potentially disclose their identity, nor shall such information be used for clinical research data analysis.
As a participant in the study, the patient retains the right to access information regarding their personal data collected and processed by the research provider, request corrections or deletions when necessary, and file complaints with supervisory authorities. These authorities include the Information Commissioner of the Republic of Slovenia.
Data collection and monitoring committee
As an impartial entity separate from research, sponsors, and any potential conflicts of interest, the guardian’s Center for Clinical Research at UMCL is responsible for reviewing and monitoring all active studies conducted within the clinic. Annually, throughout the duration of the study, the PI compiles a progress report detailing the study’s advancements, recorded adverse effects, and any serious adverse events (SAEs). This report is the subjected to evaluation by the aforementioned committee.
The information produced throughout the trial will be documented both in the primary medical records and the case report form (CRF). Quality control staff will verify the alignment of CRF data with the original records to guarantee accurate entry into the CRF. Four data collection timepoints are scheduled: baseline, intervention (d = 0), 4 weeks, and 6 months post-intervention. After complete data collection, research records will be submitted to the research leader or revision within 48 h and all data will be submitted to the PI within 1 week. Afterwards, the data will be analyzed by the statisticians.
Dissemination of data acquired in this trial will be performed through international and national conferences and via peer-reviewed publications. After the trial’s completion, our data set will be available.
Availability of data and materials
The electronic study records will be securely stored on the hospital’s servers, and access will be granted only through password-protected network computers. These data will be preserved for a period of 10 years; after which, these will be permanently removed.
Statistical methods
Since this will be an academic, exploratory study, no formal sample size calculation was performed.
We will compare the values of the presence of selected molecular markers in the synovial fluid, blood, and urine within the intervention group of patients who will receive MSC therapy. We will compare baseline values with values at the time of surgery (4–6 weeks after MSC application), as well as with values in control group samples. We will compare gene expression in chondrocytes and synoviocytes between the intervention and control groups, which will be isolated from biopsy samples obtained during surgery of both arms. Numeric variables will be compared with unpaired or paired t-test or appropriate non-parametric test. We will also compare the values of subjective questionnaires (KOOS, VAS) and the clinical status of the treated knee (IKDC examination) between the two groups and the two time intervals. We will also record any side effects in the period between MSC application and surgery, as well as up to 6 months after surgery. Missing data will be handled according to standard protocols. To assess the normality of data, we will use graphical methods and tests (e.g., Shapiro–Wilk or Kolmogorov–Smirnov). Log transformation will be applied if assumed it could help normalize data distribution and interpretation.
Data will be analyzed using databases with Excel spreadsheets and statistical analysis software such as SPSS, GraphPad Prism, or similar tools.
Discussion
This exploratory study will assess the rarely addressed effect of MSC therapy on KOA biological markers, associated with BIPED criteria. This is a pharmacological clinical study. Taking into account the ethical aspect of such study types, only the patients with terminal KOA (Kellgren–Lawrence grade 4) designated to undergo knee arthroplasty in the near future will be evaluated. Given that the safety of MSCs use for KOA has been confirmed in numerous clinical studies within the EU and worldwide, and MSC therapy of KOA is regularly performed on a hospital exemption basis within the EU implying active pharmacovigilance, the assessment of safety is not the primary goal of this study.
Regardless of the widespread use of MSCs in the field of orthopedics in the last two decades, very little is still known about the molecular mechanisms or the way this type of therapy works in the treatment of osteoarthritis [27]. Usually, the external application aims to increase their number and take advantage of their anti-inflammatory, mitogenic, angiogenic, and antiapoptotic properties. In doing so, we rely on the knowledge we have about the way they work, mainly from basic in vitro and preclinical research, and the clinical response is most often monitored using imaging diagnostics and subjective assessment of patients. Such monitoring, which is based on symptomatic, physical, and imaging methods, does not reflect pathophysiological processes or treatment effects at the molecular level. Thus, the results of clinical laboratory investigations in patients with KOA treated with the use of MSCs are largely unknown.
In this context, larger amounts of specific molecular markers can definitely be detected in various body fluids of patients with KOA, which can represent an important source of information regarding the disease state of KOA, the diagnosis, and the effectiveness of the selected therapeutic approach [28]. Here, the identification of markers of this layer is particularly important in the synovial fluid, as it represents direct information from the target anatomical location, without signals from other joints that could interfere with the analysis in systemic fluids (e.g., blood or urine). An additional source of high-quality information could be obtained from biopsy samples of the cartilage and synovium, where chondrocyte cells or synoviocytes would be monitored for the expression of KOA-specific genes.
In addition to BIPED classification, biomarkers found in the synovial fluid can also be designated into four classes, based on their molecular characteristics. These include biomarkers related to collagen metabolism, those related to aggrecan metabolism, other non-collagenous proteins, and biomarkers related to other processes (e.g., inflammation or fibrosis) [24, 29]. Based on a recent systematic review published recently by Boffa et al., more than 200 biomarkers in the synovial fluid have been identified at various degrees of their correlation with osteoarthritis [24]. For our study, we have made a selection of biomarkers, whose association with KOA was most strongly supported by literature (considering the number of publications for individual biomarker). At the same time, we aimed at analyzing at least one biomarker from each of the four classes of the molecular characteristics. We selected a total of 29 biomarkers in the aftermath.
The N-propeptide of collagen IIA or PIIANP is a splice form of type II collagen. Synthesized by chondrocytes, it correlates to increased collagen synthesis [30]. Its increased concentrations are therefore related to a lesser burden of KOA and predict decreased odds of KOA progression in the future [31]. Aggrecan is the most represented proteoglycan in the extracellular matrix and thus plays a critical role in cartilage function/joint function [32]. Its increased level in the synovial fluid have been associated with early knee injury and were elevated radiographic KOA [33]. During KOA, the enzyme aggrecanase-1 (ADAMTS-4) can cleave aggrecan which leads to the progression of disease [34].
In the context of non-collagenous proteins associated with KOA, we will analyze the levels of COMP, hyaluronan, TIMP-1, and several MMPs (MMP-1/3/7/9 and 13). Non-collagenous proteins such as COMP provide a resilient meshwork for knee cartilage. COMP is synthesized by chondrocytes and provides many roles for proper cartilage functioning. Numerous studies have shown elevated levels of COMP were associated with KOA severity [35,36,37]. Hyaluronan associates with aggrecan in the knee and provides a lubricant function to the joint and its resistance to compression forces [38]. Increased inflammation within the synovial fluid can decrease its viscosity due to increased water presence, which can affect the fluid volume within the joint and affect hyaluronan levels. These can be further affected by increased enzymatic degradation of hyaluronan [39]. TIMP-1 (an inhibitor of metalloprotease-1) has been shown to be significantly increased in synovial fluid of KOA patients compared to controls [40]. Matrix metalloproteinases, particularly MMP-1/3/13 and to some extent others, are all detected in the synovial fluid and frequently observed in relation to KOA, with various predictive powers [41]. Particularly MMP-3 has been shown a predictive value between healthy controls and patients [42]. Syndecan 4, a heparan sulfate proteglycan and important regulator of cartilage degradation, can be shed by MMPs into the synovial fluid. It was demonstrated by Bollmann et al. that elevated Syndecan 4 levels correlate with KOA severity, with MMP-9 showing the highest shedding activity in vitro [43]. Tenascin C, a glycoprotein expressed in ECM, has been designated as potential marker of intervention efficacy. It was found to be inversely correlated with improvements in VAS pain after the treatment in KOA [44].
By merit of immune-mediated mechanisms involved in KOA, a great number of immune-related biomarkers have been studied in this relation. Indeed, infiltration of various immune cell types (e.g., T cells, mast cells, macrophages, etc.) and their molecular products is detectable in KOA, although their pathophysiological importance is still inadequately understood [45]. Among cytokines, the most studied have been IL-6, followed by IL-8 and TNF-α, all belonging to innate inflammatory cytokines [24, 46]. Macrophages represent one of the central immune cells in KOA pathology and the presence of soluble markers CD14 and CD163 have been correlated with KOA symptoms and macrophage activation status [47, 48]. Immune cell infiltration is mediated by chemokines present in the SF. In particular, CCL2 is a known monocyte/macrophage chemoattractant and is significantly increased in KOA patients [49, 50]. Other chemokines, such as CCL5, have also been shown important for KOA development. Besides attracting immune cells, chemokines such as CCL5 can directly amplify synovitis by inducing IL-6 production and can cause cartilage degeneration [51, 52].
We also chose to analyze key markers associated with bone and cartilage metabolism in KOA. Bone morphogenetic proteins such as BMP-2 play an anabolic role and have been assigned a chondroprotective effect [53]. Regarding KOA, increased KL grades along with WOMAC scores positively correlated with BMP-2 presence in serum and SF [54]. A protein member of the dickkopf family, DKK-1, is known for its inhibitory activity of Wnt signaling, a master regulatory pathway of joint homeostasis and a potential drug target in KOA, since active Wnt pathway promotes cartilage breakdown [55]. DKK-1 is inversely correlated with KOA severity and its presence has been shown to ameliorate disease progression [56, 57]. Similarly to DKK-1, sclerostin is also a Wnt signaling antagonist and correlates inversely with disease severity [58]. In addition to Wnt, the osteoprotegerin-RANK-RANKL signaling system is the other key player in joint homeostasis. Besides subchondral bone, osteoprotegerin can be expressed in the cartilage, particularly in advanced KOA [59], where it is readily detected in SF [60]. Bone metabolism is importantly affected by growth factors (e.g., TGF-β, VEGF, FGF-2, etc.), with VEGF playing a key role. Wnt pathway inhibition downregulates VEGF expression, an advantageous process in KOA development. Indeed, VEGF showed a positive correlation with KOA severity in six out of seven studies analyzing its presence in SF [24].
As obesity is a major risk factor for KOA development, biomolecules released from fat tissue cells (adipokines), in addition to increased load on joints, have been shown to impact disease development [61]. One of the key adipokines in this regard is the hormone leptin, produced by white adipocytes and normally regulates appetite and energy homeostasis [62]. In SF, leptin can be detected in correlation with BMI and is known to influence immune processes and can trigger catabolic effects within the cartilage, leading to its destruction. In association with KOA severity, three out of four studies reported a positive correlation with leptin presence in SF [24].
The impact that MSC therapy could reflect on key transcriptional markers in bioptic tissue, namely in chondrocytes and synoviocytes, we believe is an aspect worthy of investigation in regard to their efficacy in KOA therapy. For analysis of gene expression, we selected ten genes associated with chondrocyte function, cartilage catabolism, pain, and inflammation.
In OA cartilage, chondrocytes have impaired function as characterized by a reduced ratio of COL2/COL1 [63] and decreased SOX9 expression [64]. Additionally, the destruction of cartilage in OA results from the inability of chondrocytes to maintain homeostasis between ECM synthesis and degradation [65]. MMP-13 [66], ADAMTS-4, and ADAMTS-5 [67] are especially important proteinases involved in the degradation of main components of cartilage ECM, aggrecan, and type II collagen.
Pain is one of the main symptoms of OA, and NGF emerged as one of the key regulators of chronic pain. Increased expression of NGF has been associated with KOA pain [68], which according to clinical studies has been significantly reduced by anti-NGF antibodies [69]. Moreover, as NGF inhibition using monoclonal antibodies has also been associated with increased adverse events and progression of disease in the long-term [70], it will be of particular importance to see how MSC therapy can affect NGF. Although no similar negative long-term effects specific to MSC treatment in KOA have been described so far, their impact on key biomarkers in this aspect is crucial for in-depth understanding of their actions.
IL-1β and TNF-α are considered key cytokines in the development of OA, expressed in various joint tissues [71]. Levels of IL-6 are also elevated in the synovial fluid of OA patients and correlate with cartilage lesions [72]. All above-listed cytokines share similar catabolic effects during OA, such as inhibition of cartilage ECM synthesis and induction of matrix-degrading enzymes [73].
Conclusion
To our knowledge, there is yet no data on the pharmacological effects of allogeneic, umbilical cord-derived MSCs in the treatment of KOA. We believe our analytical approach could give us important and integral insights into presumed and largely unknown mechanisms of action of MSC therapy in joint diseases. The study protocol is also designed in such a manner to allow for future application in various randomized trials that will pursue to assess MSC efficacy and its comparison with other therapeutic modalities in KOA. Lastly, we believe that the recognition of key mechanisms of action associated with MSC therapy can serve as important groundwork for future optimization and development of more efficient MSC-based advanced therapy medicinal products.
Trial status
Protocol version: version 1.0, 2021.06.28.
Start date of recruitment: November 2022.
Expected end date of recruitment: November 2024.
Status at the time of this submission: Recruiting (13 patients out of 20 recruited).
Availability of data and materials
All data acquired in this trial will be available to all interested after the publication of our results.
Abbreviations
- AE:
-
Adverse events
- BIPED:
-
Burden of disease, Investigative, Prognostic, Efficacy of Intervention and Diagnostic
- BMP:
-
Bone morphogenetic protein
- CCL:
-
Chemokine ligand
- CD:
-
Cluster of differentiation
- COMP:
-
Cartilage oligomeric matrix protein
- CRF:
-
Case report form
- CTCAE:
-
Common Terminology Criteria for Adverse Events
- DKK:
-
Protein member of the Dickkopf family
- ECM:
-
Extracellular matrix
- ELISA:
-
Enzyme-linked immunosorbent assay
- EQ-5D-3L:
-
European Quality of Life in Five Dimensions Three-Level
- EQ-VAS:
-
EuroQoL self-rated health on visual analog scale
- HGF:
-
Hepatocyte growth factor
- HLA:
-
Human leukocyte antigen
- ICAM:
-
Intercellular adhesion molecule
- IDO:
-
Indoleamine-2,3-dioxygenase
- IFN:
-
Interferon
- IL:
-
Interleukin
- IMP:
-
Investigational medicinal product
- iNOS:
-
Inducible nitric oxide synthase
- KOA:
-
Knee osteoarthritis
- KOOS:
-
Knee Injury and Osteoarthritis Outcome Score
- MMP:
-
Matrix metalloproteinase
- MSCs:
-
Mesenchymal stromal stem cells
- NGF:
-
Nerve growth factor
- NK:
-
Natural killer
- PDL:
-
Programmed death ligand
- PGE2:
-
Prostaglandin E2
- PI:
-
Principal investigator
- PIIANP:
-
N-Propeptide of collagen IIA
- SAE:
-
Serious adverse events
- SF:
-
Synovial fluid
- SITM:
-
Slovenian Institute for Transfusion Medicine
- TGF:
-
Transforming growth factor
- TIMP:
-
Tissue inhibitor of metalloproteinase
- TNF:
-
Tumor necrosis factor
- UMC:
-
University Medical Center
- VAS-P:
-
Visual analog scale for pain assessment
- VCAM:
-
Vascular cell adhesion protein
- VEGF:
-
Vascular endothelial growth factor
References
Chang CB, et al. The radiographic predictors of symptom severity in advanced knee osteoarthritis with varus deformity. Knee. 2011;18(6):456–60.
Felson DT, Zhang Y. An update on the epidemiology of knee and hip osteoarthritis with a view to prevention. Arthritis Rheum. 1998;41(8):1343–55.
Katz JN, Arant K, Loeser RF. Review of hip and knee osteoarthritis-reply. JAMA. 2021;325(24):2505.
Uccelli A, Moretta L, Pistoia V. Mesenchymal stem cells in health and disease. Nat Rev Immunol. 2008;8(9):726–36.
Jiang W, Xu J. Immune modulation by mesenchymal stem cells. Cell Prolif. 2020;53(1):e12712.
Huang Y, Wu Q, Tam PKH. Immunomodulatory mechanisms of mesenchymal stem cells and their potential clinical applications. Int J Mol Sci. 2022;23(17):10023.
Li N, Hua J. Interactions between mesenchymal stem cells and the immune system. Cell Mol Life Sci. 2017;74(13):2345–60.
Di Nicola M, et al. Human bone marrow stromal cells suppress T-lymphocyte proliferation induced by cellular or nonspecific mitogenic stimuli. Blood. 2002;99(10):3838–43.
Tse WT, et al. Suppression of allogeneic T-cell proliferation by human marrow stromal cells: implications in transplantation. Transplantation. 2003;75(3):389–97.
Roncarolo MG, et al. Tr1 cells and the counter-regulation of immunity: natural mechanisms and therapeutic applications. Curr Top Microbiol Immunol. 2014;380:39–68.
Rasmusson I, et al. Mesenchymal stem cells inhibit the formation of cytotoxic T lymphocytes, but not activated cytotoxic T lymphocytes or natural killer cells. Transplantation. 2003;76(8):1208–13.
Angoulvant D, et al. Human mesenchymal stem cells suppress induction of cytotoxic response to alloantigens. Biorheology. 2004;41(3–4):469–76.
Malemud CJ. Biologic basis of osteoarthritis: state of the evidence. Curr Opin Rheumatol. 2015;27(3):289–94.
Ilas DC, et al. Targeting subchondral bone mesenchymal stem cell activities for intrinsic joint repair in osteoarthritis. Future Sci OA. 2017;3(4):FSO228.
McGonagle D, Baboolal TG, Jones E. Native joint-resident mesenchymal stem cells for cartilage repair in osteoarthritis. Nat Rev Rheumatol. 2017;13(12):719–30.
Hudetz D, et al. The effect of intra-articular injection of autologous microfragmented fat tissue on proteoglycan synthesis in patients with knee osteoarthritis. Genes (Basel). 2017;8(10):270.
Hudetz D, et al. Early results of intra-articular micro-fragmented lipoaspirate treatment in patients with late stages knee osteoarthritis: a prospective study. Croat Med J. 2019;60(3):227–36.
Boric I, et al. A 24-month follow-up study of the effect of intra-articular injection of autologous microfragmented fat tissue on proteoglycan synthesis in patients with knee osteoarthritis. Genes (Basel). 2019;10(12):1051.
Webster AC, et al. Chronic kidney disease. Lancet. 2017;389(10075):1238–52.
Caraballo C, et al. Clinical implications of the New York Heart Association classification. J Am Heart Assoc. 2019;8(23):e014240.
Carlsson AM. Assessment of chronic pain. I. Aspects of the reliability and validity of the visual analogue scale. Pain. 1983;16(1):87–101.
Roos EM, Lohmander LS. The Knee injury and Osteoarthritis Outcome Score (KOOS): from joint injury to osteoarthritis. Health Qual Life Outcomes. 2003;1:64.
EuroQol G. EuroQol–a new facility for the measurement of health-related quality of life. Health Policy. 1990;16(3):199–208.
Boffa A, et al. Synovial fluid biomarkers in knee osteoarthritis: a systematic review and quantitative evaluation using BIPEDs criteria. Cartilage. 2021;13(1_suppl):82S-103S.
Kraus VB, Karsdal MA. Osteoarthritis: current molecular biomarkers and the way forward. Calcif Tissue Int. 2021;109(3):329–38.
Convill JG, et al. Clinically relevant molecular biomarkers for use in human knee osteoarthritis: a systematic review. Cartilage. 2021;13(1_suppl):1511S-1531S.
Primorac D, et al. Comprehensive review of knee osteoarthritis pharmacological treatment and the latest professional societies’ guidelines. Pharmaceuticals (Basel). 2021;14(3):205.
Munjal A, et al. Advances in molecular biomarker for early diagnosis of osteoarthritis. Biomol Concepts. 2019;10(1):111–9.
Lotz M, et al. Value of biomarkers in osteoarthritis: current status and perspectives. Ann Rheum Dis. 2013;72(11):1756–63.
Oganesian A, Zhu Y, Sandell LJ. Type IIA procollagen amino propeptide is localized in human embryonic tissues. J Histochem Cytochem. 1997;45(11):1469–80.
Kraus VB, et al. Predictive validity of biochemical biomarkers in knee osteoarthritis: data from the FNIH OA Biomarkers Consortium. Ann Rheum Dis. 2017;76(1):186–95.
Roughley PJ, Mort JS. The role of aggrecan in normal and osteoarthritic cartilage. J Exp Orthop. 2014;1(1):8.
Sobue Y, et al. Prediction of progression of damage to articular cartilage 2 years after anterior cruciate ligament reconstruction: use of aggrecan and type II collagen biomarkers in a retrospective observational study. Arthritis Res Ther. 2017;19(1):265.
Larsson S, Lohmander LS, Struglics A. Synovial fluid level of aggrecan ARGS fragments is a more sensitive marker of joint disease than glycosaminoglycan or aggrecan levels: a cross-sectional study. Arthritis Res Ther. 2009;11(3):R92.
Arellano RD, et al. Cartilage oligomeric matrix protein levels in synovial fluid in patients with primary knee osteoarthritis and healthy controls: a preliminary comparative analysis with serum cartilage oligomeric matrix protein. Arch Rheumatol. 2017;32(3):189–96.
Wu Q, Sun X, Du L. Association of fibulin-3 concentrations with the presence and severity of knee osteoarthritis: a cross-sectional study. Knee. 2017;24(6):1369–73.
Georgiev T, et al. Cartilage oligomeric protein, matrix metalloproteinase-3, and Coll2-1 as serum biomarkers in knee osteoarthritis: a cross-sectional study. Rheumatol Int. 2018;38(5):821–30.
Schmidt TA, Sah RL. Effect of synovial fluid on boundary lubrication of articular cartilage. Osteoarthritis Cartilage. 2007;15(1):35–47.
Band PA, et al. Hyaluronan molecular weight distribution is associated with the risk of knee osteoarthritis progression. Osteoarthritis Cartilage. 2015;23(1):70–6.
Li X, et al. Expression of tissue inhibitor of metalloproteinases-1 and B-cell lymphoma-2 in the synovial membrane in patients with knee osteoarthritis. Exp Ther Med. 2018;15(1):885–9.
Saberi Hosnijeh F, Bierma-Zeinstra SM, Bay-Jensen AC. Osteoarthritis year in review 2018: biomarkers (biochemical markers). Osteoarthritis Cartilage. 2019;27(3):412–23.
Singh S, Jindal D, Khanna R. Can serum MMP-3 diagnose early knee osteoarthritis? J Orthop. 2023;38:42–6.
Bollmann M, et al. MMP-9 mediated Syndecan-4 shedding correlates with osteoarthritis severity. Osteoarthritis Cartilage. 2021;29(2):280–9.
Hasegawa M, et al. Changes in biochemical markers and prediction of effectiveness of intra-articular hyaluronan in patients with knee osteoarthritis. Osteoarthritis Cartilage. 2008;16(4):526–9.
de Lange-Brokaar BJ, et al. Synovial inflammation, immune cells and their cytokines in osteoarthritis: a review. Osteoarthritis Cartilage. 2012;20(12):1484–99.
Kalaitzoglou E, Griffin TM, Humphrey MB. Innate immune responses and osteoarthritis. Curr Rheumatol Rep. 2017;19(8):45.
Ohashi Y, et al. Correlation between CD163 expression and resting pain in patients with hip osteoarthritis: possible contribution of CD163+ monocytes/macrophages to pain pathogenesis. J Orthop Res. 2022;40(6):1365–74.
Daghestani HN, Pieper CF, Kraus VB. Soluble macrophage biomarkers indicate inflammatory phenotypes in patients with knee osteoarthritis. Arthritis Rheumatol. 2015;67(4):956–65.
Monibi F, et al. Identification of synovial fluid biomarkers for knee osteoarthritis and correlation with radiographic assessment. J Knee Surg. 2016;29(3):242–7.
Watt FE, et al. Acute molecular changes in synovial fluid following human knee injury: association with early clinical outcomes. Arthritis Rheumatol. 2016;68(9):2129–40.
Tang CH, Hsu CJ, Fong YC. The CCL5/CCR5 axis promotes interleukin-6 production in human synovial fibroblasts. Arthritis Rheum. 2010;62(12):3615–24.
Alaaeddine N, et al. Production of the chemokine RANTES by articular chondrocytes and role in cartilage degradation. Arthritis Rheum. 2001;44(7):1633–43.
Whitty C, et al. Sustained delivery of the bone morphogenetic proteins BMP-2 and BMP-7 for cartilage repair and regeneration in osteoarthritis. Osteoarthritis Cartilage Open. 2022;4(1):100240.
Liu Y, et al. Correlation of bone morphogenetic protein-2 levels in serum and synovial fluid with disease severity of knee osteoarthritis. Med Sci Monit. 2015;21:363–70.
Deshmukh V, et al. A small-molecule inhibitor of the Wnt pathway (SM04690) as a potential disease modifying agent for the treatment of osteoarthritis of the knee. Osteoarthritis Cartilage. 2018;26(1):18–27.
Honsawek S, et al. Dickkopf-1 (Dkk-1) in plasma and synovial fluid is inversely correlated with radiographic severity of knee osteoarthritis patients. BMC Musculoskelet Disord. 2010;11:257.
Funck-Brentano T, et al. Dkk-1-mediated inhibition of Wnt signaling in bone ameliorates osteoarthritis in mice. Arthritis Rheumatol. 2014;66(11):3028–39.
Mabey T, et al. Plasma and synovial fluid sclerostin are inversely associated with radiographic severity of knee osteoarthritis. Clin Biochem. 2014;47(7–8):547–51.
Upton AR, et al. The expression of RANKL and OPG in the various grades of osteoarthritic cartilage. Rheumatol Int. 2012;32(2):535–40.
Pilichou A, et al. High levels of synovial fluid osteoprotegerin (OPG) and increased serum ratio of receptor activator of nuclear factor-kappa B ligand (RANKL) to OPG correlate with disease severity in patients with primary knee osteoarthritis. Clin Biochem. 2008;41(9):746–9.
Xie C, Chen Q. Adipokines: new therapeutic target for osteoarthritis? Curr Rheumatol Rep. 2019;21(12):71.
Friedman J. 20 years of leptin: leptin at 20: an overview. J Endocrinol. 2014;223(1):T1-8.
Martin I, et al. Quantitative analysis of gene expression in human articular cartilage from normal and osteoarthritic joints. Osteoarthritis Cartilage. 2001;9(2):112–8.
Zhang Q, et al. SOX9 is a regulator of ADAMTSs-induced cartilage degeneration at the early stage of human osteoarthritis. Osteoarthritis Cartilage. 2015;23(12):2259–68.
Martel-Pelletier J, Welsch DJ, Pelletier JP. Metalloproteases and inhibitors in arthritic diseases. Best Pract Res Clin Rheumatol. 2001;15(5):805–29.
Mehana EE, Khafaga AF, El-Blehi SS. The role of matrix metalloproteinases in osteoarthritis pathogenesis: an updated review. Life Sci. 2019;234:116786.
Verma P, Dalal K. ADAMTS-4 and ADAMTS-5: key enzymes in osteoarthritis. J Cell Biochem. 2011;112(12):3507–14.
Aso K, et al. Associations of symptomatic knee osteoarthritis with histopathologic features in subchondral bone. Arthritis Rheumatol. 2019;71(6):916–24.
Lane NE, et al. Tanezumab for the treatment of pain from osteoarthritis of the knee. N Engl J Med. 2010;363(16):1521–31.
Cho Y, et al. Disease-modifying therapeutic strategies in osteoarthritis: current status and future directions. Exp Mol Med. 2021;53(11):1689–96.
Melchiorri C, et al. Enhanced and coordinated in vivo expression of inflammatory cytokines and nitric oxide synthase by chondrocytes from patients with osteoarthritis. Arthritis Rheum. 1998;41(12):2165–74.
Stannus O, et al. Circulating levels of IL-6 and TNF-alpha are associated with knee radiographic osteoarthritis and knee cartilage loss in older adults. Osteoarthritis Cartilage. 2010;18(11):1441–7.
van den Bosch MHJ, van Lent P, van der Kraan PM. Identifying effector molecules, cells, and cytokines of innate immunity in OA. Osteoarthritis Cartilage. 2020;28(5):532–43.
Acknowledgements
We would like to acknowledge the entire staff of the Department for Therapeutic Services, Slovenian Institute for Transfusion Medicine and the staff of Orthopedics Clinic, University Medical Centre Ljubljana, for their help and support.
Protocol version
Version 1, 28 June 2021.
Funding
This trial is partially supported by the program P3-0371 of the Slovenian Research Agency.
Author information
Authors and Affiliations
Contributions
UŠ and MD were the principal investigators of this trial and coordinated the trial. MK contributed to the trial design and assisted in coordinating the implementation of the trial. UŠ wrote the original draft of this manuscript. MD was involved in oversight of writing. AK contributed to writing. AK and MK will be responsible for data collection. MD and UŠ will be responsible for data integrity and analysis. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study has been approved by the National Medical Ethics Committee of Slovenia on 27 July, 2022. The approval number is 0120–273/2022/3.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Švajger, U., Kolar, M., Kobold, A. et al. Mechanisms of treatment effects using allogeneic, umbilical cord-derived mesenchymal stromal stem cells (MSCs) in knee osteoarthritis: a pharmacological clinical study protocol. Trials 25, 533 (2024). https://doi.org/10.1186/s13063-024-08360-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13063-024-08360-x