
Abstract
Background
For the potential benefits of trials to reach all that they should, trials must be designed to ensure that those taking part reflect the population who will receive the intervention. However, adults with impaired capacity to consent are frequently excluded from trials — partly because researchers are unfamiliar with the legal and ethical frameworks and lack the necessary methodological expertise. Researchers identified a need for guidance on designing more inclusive trials. Building on the NIHR INCLUDE initiative, we developed the INCLUDE Impaired Capacity to Consent Framework to help researchers design inclusive trials.
Methods
The framework was developed over five phases: (1) establishing the scope and content of the framework and adapting the INCLUDE Ethnicity Framework for this population; (2) scoping the relevance of the framework to different populations and piloting in a range of trials; (3) consulting people living with impairing conditions and carers to explore their views about the framework and identify missing content areas; (4) refining the framework; and (5) the development of an implementation toolkit of resources to support researchers using the framework.
Results
The framework has two parts: a set of four key questions to help researchers identify who should be included in their trial, and a series of worksheets covering intervention design, recruitment and consent processes, data collection and analysis, and public involvement and dissemination. It is supported by a summary of the ethical and legal frameworks and a website of resources on capacity and consent. Implementation resources include infographics and animations, a library of completed frameworks, and facilitated workshops for researchers.
The framework and toolkit were launched at a webinar (November 2022), with polling demonstrating an increase in attendees’ awareness about research involving adults lacking capacity. A post-webinar survey found that stakeholders viewed the framework and toolkit as valuable tools to facilitate greater inclusion of this under-served population in trials. The framework is available online: https://www.capacityconsentresearch.com/include-impaired-capacity-to-consent-framework.html.
Conclusions
The INCLUDE Impaired Capacity to Consent Framework and implementation toolkit can support researchers to design more inclusive trials and other types of research studies. Further engagement, including with funders who are key to ensuring uptake, and evaluation is needed.
Similar content being viewed by others

Background
Randomised controlled trials (RCTs) play a vital role in evaluating the safety and effectiveness of health and care interventions — including medical treatments and services — and generating practice-changing evidence [1]. However, some populations are routinely excluded from trials, which often means little is known about which treatments are safe and work best for these under-served groups [2]. Ensuring that populations included in RCTs actually reflect the groups the intervention is intended to benefit is key to ensuring that the intervention is safe and effective in these populations, and to address the health inequalities that many of these groups experience [3]. One example of an under-served group is people who have cognitive impairment and are unable to provide consent to take part in a trial [4]. Cognitive impairment may be due to a neurodegenerative condition such as dementia, an acute illness such as a stroke, or may be experienced by people with a learning disability, a mental health condition, or those at the end of life. Trials involving adults with impaired capacity to consent encounter a range of ethical, legal, and methodological challenges, resulting in these populations frequently being excluded from research [5].
Exclusion of adults with impaired capacity to consent
Ethical concerns about the inclusion of people considered ‘vulnerable’, including those with impaired mental capacity, have been described as a major barrier to research in areas such as palliative care [6]. Selection bias based on participants’ (in)ability to provide consent has been reported in trials in a wide range of clinical conditions including stroke [7] and aphasia [8], and in populations including older people [9, 10], with negative consequences for these excluded groups as a result. For example, as an older population, one in three patients with hip fractures have concomitant cognitive impairment [11]. This group have a substantially higher postoperative mortality risk compared to patients without cognitive impairment [12], yet systematic reviews found that 8 out of 10 RCTs evaluating the management of hip fractures [13] and of rehabilitation interventions [14] exclude or ignore this population. There is a similar picture in emergency research where despite approximately 40% of older adults presenting to emergency departments having cognitive impairment [15], this population is excluded from 25% of RCTs in emergency care [16]. Additionally, trials that are designed to include adults with impaired capacity to consent frequently struggle to obtain ethical approval and to recruit and retain participants [17, 18].
Improving inclusion of this under-served group
Trials must be better designed so that they are more inclusive of groups that are under-served by research [19]. Improving the inclusion of under-served groups in research is a priority strategic area for international research funders including in the UK and USA [20, 21]. As part of the UK’s response to this international drive towards more inclusive research, the National Institute for Health and Care Research (NIHR) recently commissioned the INCLUDE initiative which developed guidance to help researchers to design more inclusive trials [2]. INCLUDE called for the development of tools to help researchers to design clinical studies that effectively recruit and retain such groups [2]. This led to the development of the INCLUDE Ethnicity Framework which aims to help researchers to design a trial that is inclusive of ethnic minority groups [22]. The next phase of INCLUDE is to develop tools and initiatives to improve the inclusion of other under-served groups in trials, including adults with impaired capacity to consent.
Our previous research found that researchers struggle to design and conduct trials involving people with a cognitive impairment due the complex challenges involved, describing a lack of knowledge and support to help them overcome these challenges [17]. They identified a need for more guidance on how trials can be designed to ensure that people with impaired capacity can participate in, and benefit from, research.
Working with researchers and people affected by capacity-affecting conditions and their carers, we developed the NIHR INCLUDE Impaired Capacity to Consent Framework to help researchers to design trials that are more inclusive of these groups [23]. Evidence from the development and evaluation of a previous INCLUDE framework — the Ethnicity Framework — showed that implementation activities are needed to help researchers to use a new framework in practice and are key for it to achieve similarly successful impact [24]. In this paper, we firstly outline the methods used in the development of the framework and the theoretically-informed implementation project that aims to support researchers to use the framework to design more inclusive trials in the future. We then outline the contents of the framework and implementation toolkit (see the “Results” section) alongside providing guidance and recommendations to support researchers to use them in practice. The framework and toolkit are available online: https://www.capacityconsentresearch.com/include-impaired-capacity-to-consent-framework.html
Methods
Development of the INCLUDE Impaired Capacity to Consent Framework
The development of the framework was led by members of the Inclusivity sub-group of the MRC-NIHR Trials Methodology Research Partnership (TMRP) Trial Conduct Working Group in the UK. It was carried out in conjunction with researchers from relevant specialties, people living with capacity-affecting conditions, and their carers. It also builds on a wider programme of research exploring the ethical and methodological issues around the inclusion of adults lacking the capacity to consent in research, and the development of interventions to address the challenges (CONSULT) [25]. As part of an implementation project, underpinned by theoretical approaches to the implementation and sustainability of interventions, we then worked with a range of stakeholders and people with lived experience to develop a toolkit to help researchers to implement the framework in their work.
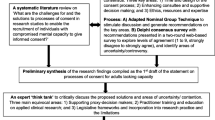
The development process (see Fig. 1) comprised five phases: (1) an initial phase established the scope of the framework and adapted the INCLUDE Ethnicity Framework structure for this population; (2) a ‘proof of concept’ phase explored the relevance of the framework to different populations through stakeholder consultation and piloted the framework in a range of studies and settings; (3) a consultation phase explored the views of carers and people living with capacity-affecting conditions about the framework and identified missing content areas; (4) the framework was refined based on the feedback received, and (5) an implementation phase led to the development of a theoretically-informed toolkit of resources to support research teams to use the framework.

INCLUDE Impaired Capacity to Consent Framework development process. *Groups involved: C, core development team; S, stakeholders; P, public involvement contributors
Phase 1: establishing the scope and content of the framework
Development of the framework started during the first half of 2021 with a core development group (VS, KJ, SF, MC, AL) who have experience in conducting trials in a range of populations who experience impaired decision-making. The group held a series of online meetings to discuss the scope and content of framework, the feasibility and utility of adapting the INCLUDE Ethnicity Framework [22], and to iteratively develop the first draft version of the framework. The four key questions from the INCLUDE Ethnicity Framework [22] were retained, although Q4 (which asks whether the intervention/comparator will make it harder for people with impaired capacity to take part) was expanded to explicitly include retention. This was considered necessary in order to reflect circumstances where a participant’s capacity is lost during trial participation as this often results in participants being withdrawn from a trial unless it has been designed to take account of this.
The framework is intended to apply to all populations with conditions or disabilities which may impair their capacity to consent to the trial (or who may lose capacity during the trial). Capacity may be impaired as a result of the condition or disability that is the focus of the trial, or the impairing condition or disability may be co-existing with the condition that the trial is focused on. It may arise from an acute event leading to a sudden loss of capacity, from a long-term condition or disability, or be a combination of the two. Therefore, the challenges needing to be addressed will vary with each trial, and the communication and capacity support needs of each population (and between members of each population) will differ.
The heterogenous nature of individuals and groups who may experience impaired capacity to consent, and therefore the contextual issues that trials involving these populations encounter, was forefront in these discussions. It was also acknowledged that trials may involve a broad range of conditions, intervention types, and settings. Discussions focused on whether a single framework could take account of these contextual differences, or whether context-specific versions were needed. However, the commonality of many of the underlying principles and challenges [17] led to the decision to develop a single framework. It was agreed that in the next phase of the project, we would explore whether the framework was applicable to a range of contexts and to consider whether additional context-specific implementation tools or resources might be needed.
In order to explore contextual factors affecting the applicability and utility of the framework in different populations, we approached national research leaders from the UK (e.g. NIHR CRN National Specialty Leads, Health and Care Research Wales (HCRW) Specialty Leads) who work with populations where there may be challenges around consent. Contact details were obtained through funders’ websites that listed relevant specialty leads. Those kindly agreeing to provide feedback were emailed a copy of the draft framework, an appendix outlining a summary of the legal frameworks governing research with adults who lack capacity, and a background document about using the framework. Specialty leads were asked to provide feedback either via an online form or by email and to focus on a series of four questions (see Table 1). They were also able to add any specific comments about the contents directly into the documents and return them by email.
Feedback was obtained from research leaders (n=5) across a range of specialties including emergency and critical care, stroke, and ageing. The framework and contents were generally viewed as an important and valuable tool, with the legal summary being viewed as particularly useful. Although the rationale for using the four key questions with corresponding worksheets was not clear to one. Suggestions were provided about how to take account of different populations and settings in order to maximise the utility of the framework, including emphasising that inclusion of all groups is the starting point. Other suggestions included providing completed examples of the worksheets. One questioned whether the worksheets could be tailored further (perhaps by the user) to the study setting to help focus on the key factors that will impact on inclusion need to be addressed.
The core development group discussed the feedback and considered that the utility of the framework had been established in principle. The feedback was used to refine the contents of the framework ahead of Phase 2.
Phase 2: ‘proof of concept’ scoping and piloting the framework
‘Proof of concept’ [26] was defined in this project as a process to establish the utility of using the structure of the INCLUDE Ethnicity Framework to design trials involving this population, and whether it was feasible to apply a single framework to a range of studies involving different populations. Invitations to pilot the framework were distributed in Autumn 2021 through UK research networks (e.g. UKTMN, South West Research Hub, learning disability researcher groups), existing collaborators (e.g. Trial Forge https://www.trialforge.org/), and via social media (Twitter/X). Researchers who were interested in piloting the framework were asked to email the lead author to express their interest.
To guide researchers or research teams who agreed to pilot the framework, we developed a set of standard instructions. These asked teams to select a trial which may include adults with impaired capacity to consent, which could be a real (ongoing or completed) trial, a trial that was currently being developed, or a hypothetical trial. Researchers were asked to go through the framework and apply it to their trial and complete and return the worksheets. They were asked to comment on any wording or sections that they found unclear or which required amending, and whether they found any areas particularly helpful or unhelpful.
A total of 20 expressions of interest (EOI) were received by email, who were subsequently sent further information. The framework and instructions were sent out to 13 researchers/research teams who subsequently agreed to pilot the framework. Of these, 11 provided comments or feedback. Brief characteristics of the studies or research contexts which informed the basis for their feedback are shown in Table 2.
Researchers could pilot the framework and provide feedback either as an individual or as a group. In addition to providing information about the trial used to pilot the framework (e.g. whether hypothetical or real, a brief summary of the trial), researchers were asked to provide responses to a series of questions (see Table 3) which were based on those used in Phase 1 and to return the completed framework document. Of the 11 who provided feedback, five returned worked examples of the framework, one of which was only partially completed. The questions and responses are summarised in Table 3 below.
Researchers reported that piloting the framework led to a change in some of the research teams’ knowledge and attitudes towards the inclusion of people with impaired capacity. One described it as ‘an enjoyable process’ that had made them think more deeply about the issues around inclusion of adults with impaired capacity to consent and encouraged them to think of potential practical solutions that might help such as discussions with their public involvement group. Others reported that they found the guidance especially helpful as they usually excluded people who cannot consent to research (or do not have a study partner) from their studies without really considering whether they could take part. One research team reported that during the design phase of the study, they would not usually consider the nature of impaired capacity that may affect their participant population and so they found the question relating to that issue very useful as it had initiated helpful conversations.
Phase 3: stakeholder consultation
For this project, in line with the MRC guidance for developing and evaluating complex interventions, stakeholders were considered to be individuals or groups whose personal or professional interests are affected by the framework, with patients and members of the public being considered key stakeholders [27]. Stakeholder consultation was embedded throughout the five phases of the development and implementation of the framework. Phase 3 particularly focused on stakeholders with lived experience of living with a condition that may affect memory or understanding and family members caring for someone living with a capacity-affecting condition and was conducted iteratively throughout the development of the framework and toolkit. This built on the public and patient involvement activities as part of developing the INCLUDE Ethnicity Framework [22] which was subsequently adapted to form the basis of this framework.
Public stakeholder consultation during development of the framework
Two discussion groups were held online in May 2022. Invitations to join the discussion groups were shared with a lay advisory group that supports a parallel project exploring adults who lack the capacity to consent (CONSULT [25]) and also disseminated by Health and Care Research Wales to their involvement community who could submit an expression of interest to the framework development team. Prior to the discussion groups, information was circulated to the four attendees which included information about clinical trials (a link to the NIHR website and an easy read guide produced by NIHR [28]) and a discussion document about ensuring trials are inclusive of people with impaired capacity to consent that was created by the team alongside an easy read version of the discussion document.
Members of the framework development team gave a brief presentation about the background to the framework, its purpose, and the contents of the draft framework. Attendees were asked for their views about the contents, what information was currently missing which should be included, and what could support families and other groups to use the framework as public involvement contributors. Discussions with the groups highlighted the importance of ensuring that information is useful to carers (e.g. avoiding terminology which may not be widely understood) and provided in an accessible format (e.g. using mixed media such as video), and ensuring diversity and inclusivity is reflected in any visual imagery used. It was also suggested that facilitating workshops with research teams and public involvement contributors would be helpful and could be a way of ‘humanising’ the issues. Attendees also had the opportunity to provide written comments on the framework document by email following the group meetings. Two members of the discussion groups provided detailed feedback.
Public stakeholder consultation during the development of the implementation toolkit
Following the development of draft materials for the implementation toolkit (see Phase 5), we held further consultation to seek feedback on the content and format. Online discussion groups were held in September 2022 with seven members of the public who were living with a condition that may affect memory or understanding or had experience as a carer. The groups included the four attendees from the previous discussion group together with three additional members who were identified through the same routes to ensure more diverse perspectives were represented. Draft versions of a two-page infographic and an animated explainer video were shared with the group.
Attendees discussed the presentation of the information and the use of shape and colour to illustrate concepts of ‘under-served groups’, ‘exclusion’, and ‘widening participation’ rather than photographic images. This approach had been chosen by the development team due to the challenges of accurately representing the many heterogenous populations and settings where impaired capacity to consent may be encountered. There were mixed views about the use of abstract shapes, with some suggesting it was difficult to follow, although others viewed it more positively particularly as they became more familiar with the images being used.
Feedback was provided on the optimal ordering of information. They suggested dissemination routes for sharing information about the framework and implementation toolkit and highlighted the need for a coordinated strategy or campaign for engagement with stakeholders including funders. The group also suggested it would be helpful to create additional context- or population-specific materials, such as videos with different populations sharing their diverse experiences (e.g. someone from a minority ethnic group who is living with dementia or an acute brain injury).
Co-production of an easy read guide to the framework
As public involvement is a key part of designing inclusive trials, an important component of the implementation toolkit is accessible information about the framework that could be provided to public involvement contributors. We worked with Thinklusive [29], a specialist designer of inclusive communications, to develop an easy read user guide for people with communication and cognitive disabilities. Creating accessible information can support people with additional support needs to understand the information being provided, including people with a learning disability, people with other types of disability and people who are not fluent in English. Using the framework document as the basis, we worked collaboratively with Thinklusive to establish the aims of the accessible version and to develop a broad outline of the content. The Thinklusive team then co-produced the user guide content and layout with the Thinklusive Advisory Group, a group of experts by experience, over several workshops.
The easy read guide consists of four sections which help to support understanding by introducing and structuring the concepts involved including an introduction to the framework and the need to design inclusive trials, a guide to clinical trials, capacity and consent to research, and the structure and content of the framework. The user guide contains links to more information and is illustrated by ‘real world’ examples of decision-making suggested by the advisory group drawn from their own experiences.
Phase 4: refining and finalising the framework
Following the consultation, the content and format of the framework was finalised by the development team. The contents of the framework are described in the Results section below.
Phase 5: implementation project
An implementation project was planned to identify and address any barriers to the uptake of the framework, some of which were identified during the pilot stage of the framework development and those identified by Trial Forge [22, 24] during the implementation and evaluation if its ‘sister’ framework — the INCLUDE Ethnicity Framework. As a complex intervention that is intended to disrupt current systems for designing trials [30], we recognised the need for theorising how it would work in practice, which takes account of how it interacts with the context in which it is implemented [27]. The project was underpinned by implementation science (IS) which helps to identify the contextual barriers and facilitators that enhance innovation uptake [31] and using Normalisation Process Theory (NPT) which addresses factors which affect the integration of interventions into routine work [32].
This phase of the project was led by the implementation team ((VS, ST, BN, JS) and consisted of a series of activities to identify and address the barriers to implementation of the framework. The key activities are outlined in the following section.
Stakeholder analysis and development of an impact plan
A stakeholder and public analysis was conducted to identify the organisations and groups who are the beneficiaries of this research, prioritise the stakeholders, and develop strategies to engage with them effectively in order to generate impact [33]. An impact plan was then developed to map these stakeholders against the planned activities that were intended to engage them in the project, to identify any barriers to engagement, and to develop tailored approaches where necessary [34]. Stakeholders included: funders of health and care research (e.g. NIHR), policy and research governance organisations (e.g. Health Research Authority), researchers, and patients and members of the public. Activities to support engagement included a stakeholder consultation (see section below).
Development of a logic model
Using theories of change, a logic model was developed to help identify the inputs, processes, outputs, and outcomes required for the successful implementation of the framework and the causal mechanisms [35] (Fig. 2). The underlying assumptions were also included in the logic model, alongside the external and contextual factors that may affect implementation. The logic model was used to identify barriers to implementation, including the need to raise awareness with researchers and patient and public involvement groups about the issues around the lack of inclusion of this population and the purpose of the framework.

INCLUDE Impaired Capacity to Consent Framework logic model
NPT analysis for implementing the framework
The process of intervention development and implementation requires a strong theoretical foundation, with NPT being previously found to support the implementation and sustainability of interventions [32]. As a behavioural approach, NPT can help to explain how complex interventions work, identify factors that promote and prevent their incorporation into everyday practice, and ultimately lead to the point where an intervention becomes so embedded into routine practice that it is normalized [36]. NPT is considered to have four generative mechanisms: coherence, cognitive participation, collective action, and reflexive monitoring [36]. These mechanistic components are considered to have dynamic relationships between themselves and with the wider context of the intervention [32]. Using an analytical approach that has previously supported the wide-scale implementation of complex interventions [32], we conducted an NPT analysis for implementing the framework (see Table 4).
During this analysis, a series of questions enabled us to explore how the four components of NPT might affect the uptake and use of the framework, and identify the actions needed to support its implementation. Questions such as ‘Does it have a clear purpose for all relevant participants?’ and ‘Will they see the point easily?’ led us to identify a need for an implementation toolkit to accompany the framework which would provide additional information to stakeholders about the purpose of the framework and practical support to help research teams to use it. Uncertainties about the format and contents of the implementation toolkit were then the focus of the stakeholder survey which followed this analysis.
Stakeholder consultation survey
Informed by the NPT analysis, we conducted a stakeholder consultation to help finalise our implementation plans. A short survey was created using Microsoft Forms (https://support.microsoft.com/en-us/forms) and shared with relevant organisations (e.g. NIHR Emergency Care Incubator, TCWG, BSG Care Home Special Interest Group, RECs) and individuals (e.g. NIHR/HCRW Specialty Leads) and via social media (Twitter/X). The survey was open June-August 2022 and consisted of a combination of multiple-choice options and open-text responses. Characteristics of stakeholders who responded to the survey (n=25) and their main area of interest are shown in Table 5. The survey questions are shown in Table 6 together with a thematical summary of the responses.
Those responding to the survey could also provide the details of organisations they thought would be interested in hearing about the framework or receiving details of a webinar being planned, and responses included a range of research networks, funders, and advocacy/support groups for relevant populations. They could also indicate if they were happy to be contacted about the next stage of the framework implementation process.
Development of an implementation toolkit to support the use of the framework
A multi-media toolkit was developed to support implementation. This included a short animated ‘explainer video’ which we commissioned an external design company to create to raise awareness with researchers and other stakeholders about the issues surrounding the exclusion of this under-served group and the purpose of the framework. This was used to develop a set of infographics to reinforce the message in increasing levels of detail and a ‘user guide’ which provides more detailed instructions about how and when the frameworks should be used (Supplementary file 1). The video, layered infographics, and user guide were intended for use on relevant websites (e.g. universities involved in the development and other relevant research networks) and to be shared via social media. Welsh language versions were also developed, and an easy read version of the user guide was co-produced (see Phase 3 for more details about the co-production process and who was involved). Collaboration with graphic design teams ensured that the toolkit materials are visually appealing and provide a professional and cohesive ‘brand identity’ to the framework and accompanying resources. The framework is supported by a website of collated resources on capacity and consent in research that has been developed in a parallel project (CONSULT [25]). The framework and implementation toolkit are available via the resources website (https://www.capacityconsentresearch.com/include-impaired-capacity-to-consent-framework.html).
Online webinar to introduce the framework
The framework and toolkit were launched at an online workshop (November 2022) with 250 attendees comprising researchers, ethics committee members, healthcare professionals, and members of the public including public involvement contributors. The aim of the webinar was twofold - firstly to introduce the framework and explain how, when, and by whom it should be used, and secondly to highlight it as one of the methodological tools being developed that are supporting the wider strategic work around equality, diversity and inclusivity by funders (e.g. NIHR) and policy-makers (e.g. Department of Health and Social Care) both in the UK and beyond. This was achieved through a series of presentations followed by a panel discussion. A recording of the webinar is available (https://www.youtube.com/watch?v=bJt84ZjqMjc).
Of those who responded to a poll of attendees (n=180), responses showed that the audience consisted primarily of researchers (64%), health and social care professionals (16%), members of the public (5%), research ethics committee members (2%), and others (13%). Pre- and post-webinar polls showed an overall increase in stakeholders’ awareness about research involving adults lacking capacity, rising from a pre-webinar mean score 5.27 (‘Out of 10 how aware did you feel about the topic before the webinar?’) to post-webinar mean score 7.25 (After watching the presentations and discussion, out of 10 how aware do you feel now in applying this in your practice?’).
Following the launch, a feedback survey found that the framework was welcomed by researchers, who considered the framework and accompanying resources to be valuable tools that help facilitate greater inclusion of under-served populations when designing future trials. Questions that were asked during the webinar and in the feedback survey were collated thematically and used to create a ‘frequently asked questions’ (FAQs) document that formed an additional part of the implementation toolkit (Supplementary file 2). This included questions about how the framework applies to research conducted in different jurisdictions where the legal frameworks will differ, whether it can be used for different types of research beyond clinical trials, and how the burden of using the framework can be reduced for busy research teams.
Workshop activities to support researchers to implement the framework effectively
As our previous research showed that research teams often lack the knowledge and methodological expertise to design and conduct studies involving this population [17, 37], we also developed more active forms of support. The development team considered that the questions included in the framework could act as a sensitising device to enable research teams to consider the barriers and facilitators, rather than solely having the framework document as the focal point. Facilitated workshops were thought to be the best way to support research teams to work through the framework questions, identify the barriers, and signpost them to tools and resources to address them. They would also provide a mechanism for the development team to observe researchers implementing the framework in practice, and to gather feedback. Therefore, as an additional part of the implementation toolkit, we developed workshop materials to support research teams’ discussions.
Over a 3-month period we piloted facilitated workshops with trial teams (n=4) who were designing trials involving adults with impaired capacity to consent, including those who lack capacity. Workshops were held online, lasted 1–1.5 h, and explored the frameworks questions in a range of trial contexts. Trials included those in settings where the population would predominantly lack the capacity to consent (e.g. critical care, stroke) and where cognitive impairment is prevalent in the population but the focus of the trial is a health condition unrelated to the impairing condition (e.g. care home residents living with diabetes, people living with cancer and multiple long term conditions). They also included different trial designs (e.g. RCTs, platform trials), types of interventions (e.g. medicines, medical devices, complex interventions), and at different stages of development (e.g. funding application, protocol development). Each workshop was led by two members of the framework project team (VS, BN) and involved a range of research team members including chief investigators, trial managers, research nurses, and public involvement contributors. Some teams were experienced in conducting research involving adults with impaired capacity and for others it was their first study involving this population. Informal feedback was collected from research teams and the framework project team created summaries of the discussions following each workshop. The workshop materials were iteratively refined where needed.
The workshops received overwhelmingly positive feedback. Research teams described it as being a useful and informative experience, which provided them with a lot to think about — including those who were experienced in research involving adults with impaired capacity. They reported that the discussions and information arising from the workshops had enabled them to incorporate the additional actions and resources identified as being necessary to conduct an inclusive trial into the funding application or include the actions and processes in the protocol being developed. Our observations highlighted the contextualised nature of the issues arising when designing trials to include adults with impaired capacity, and therefore which aspects of the framework may be more or less relevant for each trial. For example, Q3 of the framework which relates to the intervention/comparator and how people with impaired capacity may respond to or engage with it may be less relevant in critically ill patients who are sedated and ventilated compared to a complex intervention involving care home residents. By contrast, other items such as worksheet C which explores issues around consent and the involvement of consultees and legal representatives are relevant to all trials although the exact consent process and timings involved may well vary between different trial contexts. The need for further education and training on the legal and practical issues surrounding capacity and consent in research was commonly highlighted by research teams.
Results
The INCLUDE Impaired Capacity to Consent Framework has been developed for researchers designing trials involving a range of populations where the capacity to consent may be impaired. A multi-media implementation toolkit (https://www.capacityconsentresearch.com/include-impaired-capacity-to-consent-framework.html) has been developed to raise awareness about the framework, support researchers to use it, and engage with stakeholders including funders who will be key to ensuring uptake of the framework.
The INCLUDE Impaired Capacity to Consent Framework is an editable document (Microsoft Word) containing two parts (Fig. 3). A set of four key questions help researchers identify which groups of people with impairing conditions should be included in their trial, and whether particular aspects of their condition, the intervention being tested, or the way the trial has been designed will affect their ability to take part. For each question, there are worksheets to help researchers answer the questions and identify what actions and resources are needed, with signposting to information and resources on capacity and consent [38] including summaries of the ethical and legal frameworks and practical guidance such as how to assess capacity and create accessible information sheets.

Structure of the INCLUDE Impaired Capacity to Consent Framework
The worksheets cover areas including eligibility criteria, accessibility of trial information, informed consent arrangements, where and how data are collected, and how results are analysed and shared with these groups. Researchers then summarise the actions that could improve inclusivity in their trial, and any relevant resources needed, using the links to further information provided. Instructions for researchers about when the framework should be used, who by, and how much time and resource is involved are provided in Table 7 below.
Based on our observations of research teams implementing the framework in a diverse range of trial contexts during the facilitated workshops, feedback from stakeholders during and following the webinar, and subsequent discussions with other stakeholders, we developed a series of recommendations for research teams which provides a breakdown about what to consider when using the framework (Table 8).
Conclusions
Addressing consent-based recruitment bias will ensure that people with impaired capacity to consent have an equitable opportunity to participate in research, and for the interventions they receive to be evaluated as safe and effective for them. Inclusion in research is essential in order to improve care for this under-served population and to reduce the health inequalities they experience. The INCLUDE Impaired Capacity to Consent Framework is intended to help researchers to design and conduct trials that are better quality and more inclusive of this population. Further work is needed to evaluate the effectiveness of the framework and identify implementation factors, to understand the multi-level contextual factors affecting its implementation in specific trial contexts [41], and to explore the wider intersectional factors affecting this and other under-served groups. The development and implementation process may serve as a guide to groups developing similar frameworks or tools that are intended to support researchers to design more inclusive research.
Availability of data and materials
The NIHR INCLUDE Impaired Capacity to Consent Framework and accompanying resources are available online at: https://www.capacityconsentresearch.com/include-impaired-capacity-to-consent-framework.html
Abbreviations
- BSG :
-
British Society of Gerontology
- CRN:
-
Clinical Research Networks
- EOI:
-
Expression of interest
- HCRW:
-
Health and Care Research Wales
- IS:
-
Implementation science
- TCWG:
-
MRC-NIHR Trials Methodology Research Partnership’s Trial Conduct Working Group
- TMRP:
-
MRC-NIHR Trials Methodology Research Partnership
- MRC:
-
Medical Research Council
- NIHR:
-
National Institute for Health and Care Research
- NPT:
-
Normalisation Process Theory
- RCT:
-
Randomised controlled trial
- REC:
-
Research ethics committee
- UKTMN:
-
UK Trial Management Network
References
Curley LE, Lin JC. Randomised Controlled Trials and Pharmacy Practice Research. In: Babar Z-U-D, editor. Pharmacy Practice Research Methods. Singapore: Springer; 2020. p. 203–18.
Witham MD, Anderson E, Carroll C, Dark PM, Down K, Hall AS, et al. Developing a roadmap to improve trial delivery for under-served groups: results from a UK multi-stakeholder process. Trials. 2020;21:694.
Clark LT, Watkins L, Piña IL, Elmer M, Akinboboye O, Gorham M, et al. Increasing Diversity in Clinical Trials: Overcoming Critical Barriers. Curr Probl Cardiol. 2019;44:148–72.
Shepherd V, Wood F, Griffith R, Sheehan M, Hood K. Protection by Exclusion? The (lack of) inclusion of adults who lack capacity to consent to research in clinical trials in the UK. Trials. 2019; https://doi.org/10.1186/s13063-019-3603-1.
Shepherd V. An under-represented and underserved population in trials: methodological, structural, and systemic barriers to the inclusion of adults lacking capacity to consent. Trials. 2020;21:445.
Evans CJ, Yorganci E, Lewis P, Koffman J, Stone K, Tunnard I, et al. Processes of consent in research for adults with impaired mental capacity nearing the end of life: systematic review and transparent expert consultation (MORECare_Capacity statement). BMC Med. 2020;18:221.
Hotter B, Ulm L, Hoffmann S, Katan M, Montaner J, Bustamante A, et al. Selection bias in clinical stroke trials depending on ability to consent. BMC Neurol. 2017;17:206.
Brady MC, Fredrick A, Williams B. People with Aphasia: Capacity to Consent, Research Participation and Intervention Inequalities. Int J Stroke. 2013;8:193–6.
Taylor JS, DeMers SM, Vig EK, Borson S. The Disappearing Subject: Exclusion of People with Cognitive Impairment and Dementia from Geriatrics Research. J Am Geriatr Soc. 2012;60:413–9.
Feldman MA, Bosett J, Collet C, Burnham-Riosa P. Where are persons with intellectual disabilities in medical research? A survey of published clinical trials. J Intellect Disabil Res. 2014;58:800–9.
Seitz DP, Adunuri N, Gill SS, Rochon PA. Prevalence of Dementia and Cognitive Impairment Among Older Adults With Hip Fractures. J Am Med Dir Assoc. 2011;12:556–64.
Ioannidis I, Mohammad Ismail A, Forssten MP, Ahl R, Cao Y, Borg T, et al. The mortality burden in patients with hip fractures and dementia. Eur J Trauma Emerg Surg. 2022;48:2919–25.
Mundi S, Chaudhry H, Bhandari M. Systematic review on the inclusion of patients with cognitive impairment in hip fracture trials: a missed opportunity? Can J Surg. 2014;57:E141–5.
Sheehan KJ, Fitzgerald L, Hatherley S, Potter C, Ayis S, Martin FC, et al. Inequity in rehabilitation interventions after hip fracture: a systematic review. Age Ageing. 2019;48:489–97.
Clevenger CK, Chu TA, Yang Z, Hepburn KW. Clinical care of persons with dementia in the emergency department: a review of the literature and agenda for research. J Am Geriatr Soc. 2012;60:1742–8.
Southerland LT, Benson KK, Schoeffler AJ, Lashutka MA, Borson S, Bischof JJ. Inclusion of older adults and reporting of consent processes in randomized controlled trials in the emergency department: A scoping review. Journal of the American College of Emergency Physicians Open. 2022;3:e12774.
Shepherd V, Hood K, Wood F. Unpacking the ‘Black Box of Horrendousness’: A Qualitative Exploration of the Barriers and Facilitators to Conducting Trials Involving Adults Lacking Capacity to Consent. Trials. 2022;23
Griffiths S, Manger L, Chapman R, Weston L, Sherriff I, Quinn C, et al. Letter on “Protection by exclusion? The (lack of) inclusion of adults who lack capacity to consent to research in clinical trials in the UK” | Trials | Full Text. Trials. 2020;21
Bodicoat DH, Routen AC, Willis A, Ekezie W, Gillies C, Lawson C, et al. Promoting inclusion in clinical trials—a rapid review of the literature and recommendations for action. Trials. 2021;22:880.
National Institute for Health Research. Best Research for Best Health: The Next Chapter. 2021.
NIH Minority Health and Health Disparities Strategic Plan 2021-2025. National Institutes of Health.
Treweek S, Banister K, Bower P, Cotton S, Devane D, Gardner HR, et al. Developing the INCLUDE Ethnicity Framework—a tool to help trialists design trials that better reflect the communities they serve. Trials. 2021;22:337.
Implementation of the ‘INCLUDE Impaired Capacity to Consent Framework’ for researchers. Cardiff University. https://www.cardiff.ac.uk/centre-for-trials-research/research/studies-and-trials/view/implementation-of-the-include-impaired-capacity-to-consent-framework-for-researchers. Accessed 9 Aug 2022.
Morris L, Dumville J, Treweek S, Miah N, Curtis F, Bower P. Evaluating a tool to improve engagement and recruitment of under-served groups in trials. Trials. 2022;23:867.
CONSULT. Cardiff University. https://www.cardiff.ac.uk/centre-for-trials-research/research/studies-and-trials/view/consult. Accessed 12 Oct 2021.
Kendig CE. What is Proof of Concept Research and how does it Generate Epistemic and Ethical Categories for Future Scientific Practice? Sci Eng Ethics. 2016;22:735–53.
Skivington K, Matthews L, Simpson SA, Craig P, Baird J, Blazeby JM, et al. A new framework for developing and evaluating complex interventions: update of Medical Research Council guidance. BMJ. 2021;n2061
Clinical trials: an easy read guide. National Institue for Health and Care Research.
Thinklusive | Accessible information design for health and social care. Thinklusive. https://thinklusive.org/. Accessed 22 Jan 2023.
Hawe P, Shiell A, Riley T. Theorising Interventions as Events in Systems. Am J Community Psychol. 2009;43:267–76.
Bauer MS, Kirchner J. Implementation science: What is it and why should I care? Psychiatry Res. 2020;283:112376.
Murray E, Treweek S, Pope C, MacFarlane A, Ballini L, Dowrick C, et al. Normalisation process theory: a framework for developing, evaluating and implementing complex interventions. BMC Med. 2010;8:63.
Reed MS, Graves A, Dandy N, Posthumus H, Hubacek K, Morris J, et al. Who’s in and why? A typology of stakeholder analysis methods for natural resource management. J Environ Manag. 2009;90:1933–49.
Reed MS. The Research Impact Handbook. 2nd ed. Fast Track Impact; 2018.
Funnell Sue C, Rogers Patricia J. Purposeful Program Theory: Effective Use of Theories of Change and Logic Models; 2011.
May CR, Mair F, Finch T, MacFarlane A, Dowrick C, Treweek S, et al. Development of a theory of implementation and integration: Normalization Process Theory. Implement Sci. 2009;4:29.
Shepherd V, Griffith R, Sheehan M, Wood F, Hood K. Healthcare professionals’ understanding of the legislation governing research involving adults lacking mental capacity in England and Wales: a national survey. J Med Ethics. 2018; https://doi.org/10.1136/medethics-2017-104722.
Capacity and consent to research. CONSULT. https://www.capacityconsentresearch.com/. Accessed 27 Sep 2021.
Shepherd V. Research involving adults lacking capacity to consent: the impact of research regulation on “evidence biased” medicine. BMC Medical Ethics. 2016;17:8.
Jayes M, Palmer R. Initial evaluation of the Consent Support Tool: A structured procedure to facilitate the inclusion and engagement of people with aphasia in the informed consent process. International Journal of Speech-Language Pathology. 2014;16:159–68.
Mielke J, Brunkert T, Zúñiga F, Simon M, Zullig LL, De Geest S. Methodological approaches to study context in intervention implementation studies: an evidence gap map. BMC Med Res Methodol. 2022;22:320.
Acknowledgements
The authors would like to thank the members of the lay advisory group who provided invaluable insight and support for this project, including the Thinklusive Advisory Group who are experts by experience who co-designed the Easy Read guide with Maximilian Clark from Thinklusive. We would like to thank the wider contributors to the development of the INCLUDE Impaired Capacity to Consent Framework who kindly helped to pilot the Framework (including Amy M Russell, Lindsay Mizen, Nicola Farrar, Julia Wade, Edward Carlton, Clare Clements, Holly McKeon, Liz Coulthard, Laura Goodwin, Sarah Voss, Anna Mulvihill, Jennifer McAnuff, Phillip Whitehead, Tim Rapley, Adwoa Parker, Alexandra Dean, Callum Kaye, Liz Cook, Joanne Laycock, Anne Cochrane, Ashley Scrimshire, Marian Brady, Donna C. Tippett, Jonathan Hewitt, Ceri Battle, Paul Dark, Matthew Costa, and Khalid Ali) and members of the Inclusivity subgroup of the MRC-NIHR Trial Conduct Working Group who have participated in discussions at various stages of this work.
Funding
VS is supported by a National Institute of Health Research Advanced Fellowship (CONSULT) funded by the Welsh Government through Health and Care Research Wales (NIHR-FS(A)-2021). The implementation project was funded by Cardiff University through an Innovation for All award. This work was supported by the MRC-NIHR Trials Methodology Research Partnership (MR/S014357/1). The Centre for Trials Research is funded by Health and Care Research Wales and Cancer Research UK. The Bristol Trials Centre, a UKCRC registered clinical trials unit (CTU), is in receipt of NIHR CTU support funding. The Health Services Research Unit, University of Aberdeen, receives core funding from the Chief Scientist Office of the Scottish Government Health Directorates.
Author information
Authors and Affiliations
Contributions
VS conceived the paper and drafted the manuscript. VS, KJ, SF and AL developed the INCLUDE Impaired Capacity to Consent Framework in collaboration with the Inclusivity subgroup of the Trial Conduct Working Group from the MRC-NIHR Trial Methodology Research Partnership. VS led the implementation project with ST, BN, JS and members of the development group (KJ, SF and AL). All authors critically revised the manuscript and approved the final version.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
No research data were collected for this paper.
Consent for publication
Not applicable.
Competing interests
ST is an Editor-in-Chief of Trials. The other authors all declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
INCLUDE Framework User Guide.
Additional file 2.
INCLUDE Framework FAQs.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Shepherd, V., Joyce, K., Lewis, A. et al. Improving the inclusion of an under-served group in trials: development and implementation of the INCLUDE Impaired Capacity to Consent Framework. Trials 25, 83 (2024). https://doi.org/10.1186/s13063-024-07944-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13063-024-07944-x