
Abstract
Background
Healthcare systems data (HSD) has the potential to optimise the efficiency of randomised controlled trials (RCTs), by decreasing trial-specific data demands. Therefore, the use of HSD in trials is expected to increase. In 2019, it was estimated that 47% of NIHR-funded trials were planning to use HSD. We aim to understand the extent and nature of its current use and its evolution over time.
Methods
We identified a cohort of RCTs within the NIHR Journals Library that commenced after 2019 and were described as being in progress on 6 June 2022. Details on the source and use of HSD were extracted from eligible RCTs. The use of HSD was categorised according to whether it was used as the sole data source for outcomes and whether the outcomes were primary or secondary. HSD is often insufficient for patient-reported outcomes (PROs). We aimed to determine methods used by trialists for collecting PRO data alongside HSD.
Results
Of the 84 eligible studies, 52 (62%) planned to use HSD and 79 (94%) planned to collect PROs. The number of RCTs planning to use HSD for at least one outcome was 28 (54%) with 24 of these planning to use HSD as the sole data source for at least one outcome.
The number of studies planning to use HSD for primary and secondary outcomes was 10 (20%) and 21 (40%) respectively. The sources of HSD were National Health Service (NHS) Digital (n = 37, 79%), patient registries (n = 7, 29%), primary care (n = 5, 21%), The Office for National Statistics (ONS) (n = 3, 13%) and other (n = 2, 8%).
PROs were collected for 92% of the trials planning to use HSD. Methods for collection of PROs included in-person (n = 26, 54%), online (n = 22, 46%), postal (n = 18, 38%), phone (n = 14, 29%) and app (n = 2, 4%).
Conclusions
HSD is being used in around two thirds of the studies but cannot yet be used to support PRO data collection within the cohort we examined. Comparison with an earlier cohort demonstrates an increase in the number of RCTs planning to use HSD.
Similar content being viewed by others


Background
Randomised controlled trials (RCTs) are the gold standard for evaluating healthcare interventions [1]. RCTs usually require a lot of personnel, bespoke data collection and lengthy follow-up, thus resulting in high costs. In 2017 [2], the price of an RCT in the USA was between $40,000 and $100,000 per patient recruited.
The traditional methods of collecting data for RCTs typically involve requesting patients to provide information about their treatment by going to the trial-specific medical site and undergoing medical assessments or tests and through self-reported questionnaires, as necessary, according to the trial design, at predetermined time-points.
The use of health data collected as part of routine care, instead of, or in combination with bespoke trial data collection, may reduce the burden on participants, both patients and site staff, with an associated reduction in cost. Healthcare systems data (HSD) refers to medical information collected without having a specific research question formulated in advance. Such data can be gathered from different sources, including National Health Services (NHS) Digital, the Office for National Statistics (ONS) and disease-specific patient registries. These databases contain a large amount of information, for example, the NHS which holds comprehensive medical records for more than 65 million people that contain data recorded over 10 years. Given the resources required to undertake participant follow-up and collect bespoke clinical trial data, the efficiency that may be gained with HSD is of heightened interest.
The use of HSD in research is increasing [3] and its benefits and limitations in RCTs are being explored worldwide [4,5,6]. It has been argued that many common RCT limitations can be resolved by using healthcare systems data, including recruitment challenges, randomised allocation to interventions and missing data due to loss to follow-up of participants [4].
Only 3% of all UK RCTs were estimated to have successfully accessed HSD from UK-based registries between 2013 and 2018 [7]. Over half of the studies accessed this data (91/160) within the final 2 years of the cohort (2017–2018), demonstrating increasing trends in demand and availability of HSD. In 2019, a cohort of 216 ongoing trials funded by the National Institute for Health and Care Research (NIHR) were examined for their use of HSD [8]. Nearly half (47% 102/216) planned to use healthcare systems data, of which 46 (45%) aimed to use HSD as the sole source of data for one or more outcomes.
The importance of patient-reported outcome (PRO) data has been recognised [9]. However, it is as yet unknown the extent to which PRO data can be obtained from HSD, and if not, how trialists plan to collect and integrate the two sources of information. Two organisations, MRC-NIHR TMRP (https://www.methodologyhubs.mrc.ac.uk/about/tmrp/) and HDR UK (https://www.hdruk.ac.uk/), recently hosted a workshop on “What do we need to do to make Patient-Reported Outcomes (PROs) part of routinely collected health data?” [10]. Speakers at the workshop presented current research related to PRO data collection, including technical issues encountered, and patient and healthcare professional engagement, and highlighted, through open discussions, the need to embed PROs into healthcare systems data, as well as the associated opportunities and challenges.
Given the continuing focus and advances in accessing and utilising HSD, the aim of this study was to ascertain current practice amongst a United Kingdom (UK) cohort of recently funded and ongoing RCTs in relation to sources and use of healthcare systems outcome and PRO data.
Methods
A similar study was previously undertaken which identified NIHR HTA-funded investigator-led studies in progress in 2019. We aimed to reexamine this cohort and establish a new cohort of ongoing studies added to the Journals Library after October 25, 2019. The NIHR HTA programme was selected as a major source of publicly funded clinical trials within the UK due to its use within the previous cohort for comparison. The search of the NIHR library was undertaken on June 6, 2022; search criteria are shown in Additional file 1.
NIHR HTA-funded randomised trials were eligible for the cohort if they were in progress, were described as primary research and provided access to an available protocol. Where multiple versions of the protocol were available, only the most recently published version was considered.
The following data items were extracted from all available protocols:
-
1.
Type of trial to be conducted (randomised controlled trial, feasibility study, etc.)
-
2.
Whether the trial involved the use of any HSD
-
3.
The source of the HSD, where relevant
-
4.
Whether there were PROs collected in the trial, and if so, the means of recording the PRO data.
A trial was classified as planning to use HSD if the protocol mentioned a link with any healthcare systems for any purpose. These excluded trials asking for participant consent to use this data for the purpose of future studies that are subject to further funding which has not yet been awarded. The categories for analysis were based on those used by McKay et al. [8], with amendments made as necessary (see Additional file 2).
A trial was classified as planning to use HSD as the sole data source for at least one outcome of interest if it was mentioned that data for any of the primary or secondary outcomes would be accessed using a healthcare systems data source only. Trials that aimed to use healthcare systems data to validate the results collected using bespoke data collection were not included in this category.
The use of PROs and the data collection method were recorded for each trial. The following categories were used: in-person, postal, by telephone, via text message, video conferencing, web-based and app collection. Based on their planned use, the collection methods were further categorised as either primary or secondary (for back-up reasons, e.g. if a participant did not return their postal questionnaires, members of the team would contact them by telephone). Any study within a trial (SWAT), feasibility assessment or internal pilot that related to the collection of PROs was noted. Additionally, the protocols identified in McKay’s study were reviewed to extract PRO use, not previously undertaken [8].
During the process of extracting PRO data from the protocols, both PROs and proxy-reported outcomes (i.e. those recorded by a non-medical representative on behalf of the patient) were considered, as several trials included patients who were not capable of completing outcomes on their own. However, outcomes reported by medical professionals, including nurses and professional caregivers, were excluded as they represent a professional rather than a patient-centred interpretation of the results.
Results
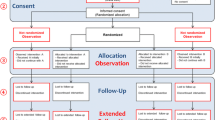
There were 183 trials identified as being in progress at the time of the search (Fig. 1). Of these, 89 (48%) had no protocols and were therefore excluded. An additional 10 (5%) were not RCTs, leaving 84 (46%) protocols to be reviewed.

PRISMA flow diagram
Fifty-two (62%) of the 84 protocols reviewed detailed plans to use healthcare systems data. Of these, 24 trials (46%) described aiming to use HSD as the sole source for at least one outcome of interest (Table 1).
There has been an increase in the proportion of trials planning to use healthcare systems data since the original review, while the percentage of trials planning to use HSD as the only source of data for at least one outcome remains relatively similar (Table 1). There are three protocols that mention using only HSD and PROs, without any bespoke clinical data collection (Table 2).
Table 3 defines the sources when outcome data are obtained solely from HSD, demonstrating that many of the RCTs use multiple sources of HSD. In the current cohort of trials, 46% of the trials planning to use HSD solely for at least one outcome plan to use more than one source of healthcare systems data, while in McKay et al. [8], this percentage is 61%. The main source of HSD in both cohorts is NHS Digital; indeed, there is an increase in the proportion of trials planning to use data from NHS Digital since the original review, alongside a decrease in the use of sources like ONS and registries.
Table 4 illustrates the most common outcomes that were collected fully from HSD (in the current cohort only). Other outcomes mentioned include treatment failure, specific events (e.g. asthma attacks) and specific drug measurements (e.g. cumulative dose of treatment).
Table 5 describes the proportion of trials planning to collect PROs, which is similar across the two cohorts regardless of whether HSD is also used. The primary method of collection remains in-person, while postal questionnaire use has decreased. The use of online data collection has increased over time for both web-based and app approaches.
In 23% of the trials collecting both PRO data and HSD, a sub-study using PROs has been included (Table 6). Predominantly, this study assesses the PRO response rate, but the adherence to treatment and patient-reported treatment success are also examined. There were no sub-studies looking at PRO data from HSD.
Discussion
The current research has three key findings, based on the aim of comparing the current trials in progress and the ones identified in McKay et al. [8]. First, there has been an increase in the number of trials planning to use HSD for any reason, from 47% in trials ongoing in 2019 [8] to 62% in trials started between 2019 and 2022. Second, survival and hospital admission were the outcomes most commonly to be collected from HSD alone.
Finally, PROs are measured in nearly all trials, but, within the current cohort, none are collecting PRO data from HSD. The importance of integrating PROs within HSD was recently discussed at the TMRP-HDRUK North workshop [10]. While there is a need to further explore the topic, the online collection of PRO data could be potentially integrated into HSD databases, such as patient registries. Currently, it can be observed that the preference for an online collection method has increased.
There are several strengths and limitations in the current research. The source of the trials and the inclusion/exclusion criteria match the previous study [8] facilitating comparison. However, all the trials included are NIHR funded, which might not completely be representative of all the RCTs currently in progress in the UK, or beyond.
Data up-cycling refers to reusing information already collected. As more trialists begin to access HSD, the amount of data available for research is becoming more widely recognised. There are potential issues to be considered when using healthcare systems data. The recently published COMORANT-UK study [11] has released a prioritised list of challenges to be addressed regarding HSD. The domains of the questions included data access, data collection and outcome selection.
Several recent publications [12, 13] have highlighted issues regarding access to data. Powell et al. [13] described trying to access 14 databases in order to gather information about 98 participants. The results suggested that secondary care data, although challenging in terms of application process, was available to access, whereas primary care data had limited accessibility and non-clinical datasets were not accessible. An update to this review is currently underway [14], aiming to further evaluate the degree of agreement between bespoke and HSD in recent UK clinical trials.
HSD related to adverse effects is being collected in almost a third of trials. Another key point previously discussed [7, 12, 13] is the timeliness of data. Data collected from healthcare systems usually involves a delay between the recording of the data and it being supplied to the trial team; for example, Hospital Episode Statistics (HES) data take approximately 3 months to be provided [12].
The PRIMORANT study sought to address two of the prioritised questions from the COMORANT study: “How should the trials community decide when routinely collected data for outcomes is of sufficient quality and utility to replace bespoke data collection?” and “What are the best methods to communicate and build trust with trial participants (and the public) about how their routinely collected data will be used?”. While the second part was approached through exploring different methods of communicating to the public, the work around the first question resulted in a list of issues to consider (under review). This list explored the necessary changes to the trial structure and highlighted aspects that should be considered before deciding to use HSD. These include terminology, feasibility, internal pilot, onward data sharing and data archiving. Following the publication of the PRIMORANT paper, it will be of interest to explore any resulting changes in the extent and nature of HSD use in trials.
Conclusion
Our research examined a cohort of ongoing RCTs and described their planned use of healthcare systems data and patient-reported outcomes. The proportion of RCTs accessing HSD has increased over time, although the proportion of planning to use it as the sole source of data for at least one outcome of interest has remained similar. This suggests the increased interest in HSD, while being aware of the current barriers of solely relying on this data. Future snapshots of HSD use in trials will be beneficial in relaying its evolution. Further research exploring the reasoning behind choosing whether to use HSD in RCTs, or not, would be useful.
The increase in online data collection for PROs supports the potential for remote data collection. This suggests it may be possible to integrate PRO with clinical data collected from HSD in a single system. Further work is needed to enable this integration, with the benefit of reducing the burden of research participation.
Availability of data and materials
The datasets generated and/or analysed during the current study are available in the “The use of healthcare systems data for RCTs - data” folder, [10.6084/m9.figshare.24158535].
Abbreviations
- HE:
-
Health economic
- HES:
-
Hospital Episode Statistics
- HSD:
-
Healthcare Systems Data
- NHS:
-
National Health Service
- NIHR:
-
National Institute for Health and Care Research
- ONS:
-
Office for National Statistics
- PO:
-
Primary outcome
- PRO:
-
Patient-reported outcome
- RCT:
-
Randomised controlled trial
- SO:
-
Secondary outcome
- SWAT:
-
Study within a trial
References
Harriton E, Locascio J. Randomized controlled trials-the gold standard for effective research. BJOG. 2018;125(13)
Speich B, von Niederhäusern B, Schur N, Hemkens LG, Fürst T, Bhatnagar N, et al. Systematic review on costs and resource use of randomized clinical trials shows a lack of transparent and comprehensive data. J Clin Epidemiol. 2018;96:1–11.
Hemkens LG, Contopoulos-Ioannidis DG, Ioannidis JP. Routinely collected data and comparative effectiveness evidence: promises and limitations. Cmaj. 2016;188(8):E158–E64.
Mc Cord KA, Al-Shahi Salman R, Treweek S, Gardner H, Strech D, Whiteley W, et al. Routinely collected data for randomized trials: promises, barriers, and implications. Trials. 2018;19(1):1–9.
Mathes T, Buehn S, Prengel P, Pieper D. Registry-based randomized controlled trials merged the strength of randomized controlled trails and observational studies and give rise to more pragmatic trials. J Clin Epidemiol. 2018;93:120–7.
Li G, Sajobi TT, Menon BK, Korngut L, Lowerison M, James M, et al. Registry-based randomized controlled trials-what are the advantages, challenges, and areas for future research? J Clin Epidemiol. 2016;80:16–24.
Lensen S, Macnair A, Love SB, Yorke-Edwards V, Noor NM, Martyn M, et al. Access to routinely collected health data for clinical trials–review of successful data requests to UK registries. Trials. 2020;21(1):1–11.
McKay AJ, Jones AP, Gamble CL, Farmer AJ, Williamson PR. Use of routinely collected data in a UK cohort of publicly funded randomised clinical trials. F1000Research. 2021;9:323.
Mercieca-Bebber R, King MT, Calvert MJ, Stockler MR, Friedlander M. The importance of patient-reported outcomes in clinical trials and strategies for future optimization. Patient Relat Outcome Meas. 2018:353–67.
TMRP-HDRUK North Workshop: What do we need to do to make Patient-Reported Outcomes (PROs) part of routinely collected health data? [Available from: http://www.methodologyhubs.mrc.ac.uk/about/tmrp-workshops-and-meetings/tmrp-hdr-uk-north-pros-workshop/.
Williams AD, Davies G, Farrin AJ, Mafham M, Robling M, Sydes MR, et al. A DELPHI study priority setting the remaining challenges for the use of routinely collected data in trials: COMORANT-UK. Trials. 2023;24(1):1–8.
Sydes MR, Barbachano Y, Bowman L, Denwood T, Farmer A, Garfield-Birkbeck S, et al. Realising the full potential of data-enabled trials in the UK: a call for action. BMJ Open. 2021;11(6):e043906.
Powell G, Bonnett L, Tudur-Smith C, Hughes D, Williamson P, Marson A. Using routinely recorded data in the UK to assess outcomes in a randomised controlled trial: the trials of access. Trials. 2017;18(1):1–11.
Ahmed S, Sydes MR, Love SB, James ND. PS8C-01 Agreement and completeness of routine versus trial-specific patient outcome data: a systematic review; 2023.
Acknowledgements
We want to thank the reviewers for their helpful comments.
Funding
Alice-Maria Toader is funded by MRC Trials Methodology Research Partnership (TMRP) Doctoral Training Partnership (DTP). Grant Number MR/W006049/1.
Author information
Authors and Affiliations
Contributions
A-MT conducted the search, analysed the results and wrote the first draft of the manuscript. CLG, SD and PRW supervised the work and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Search Criteria. Presents the search criteria used in the NIHR Journals Library.
Additional file 2.
Changes in categories for the data collected in 2022 compared to the previous review in 2019. Presents the changes made in categories for the data collected in 2022 compared to the previous review.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Toader, AM., Gamble, C.L., Dodd, S. et al. The use of healthcare systems data for RCTs. Trials 25, 95 (2024). https://doi.org/10.1186/s13063-023-07846-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13063-023-07846-4