
Abstract
Background
Extremely preterm infants have a high mortality and morbidity. Here, we present a statistical analysis plan for secondary Bayesian analyses of the pragmatic, sufficiently powered multinational, trial—SafeBoosC III—evaluating the benefits and harms of cerebral oximetry monitoring plus a treatment guideline versus usual care for such infants.
Methods
The SafeBoosC-III trial is an investigator-initiated, open-label, randomised, multinational, pragmatic, phase III clinical trial with a parallel-group design. The trial randomised 1601 infants, and the frequentist analyses were published in April 2023. The primary outcome is a dichotomous composite outcome of death or severe brain injury. The exploratory outcomes are major neonatal morbidities associated with neurodevelopmental impairment later in life: (1) bronchopulmonary dysplasia; (2) retinopathy of prematurity; (3) late-onset sepsis; (4) necrotising enterocolitis; and (5) number of major neonatal morbidities (count of bronchopulmonary dysplasia, retinopathy of prematurity, and severe brain injury). The primary Bayesian analyses will use non-informed priors including all plausible effects. The models will use a Hamiltonian Monte Carlo sampler with 1 chain, a sampling of 10,000, and at least 25,000 iterations for the burn-in period. In Bayesian statistics, such analyses are referred to as ‘posteriors’ and will be presented as point estimates with 95% credibility intervals (CrIs), encompassing the most probable results based on the data, model, and priors selected. The results will be presented as probability of any benefit or any harm, Bayes factor, and the probability of clinical important benefit or harm. Two statisticians will analyse the blinded data independently following this protocol.
Discussion
This statistical analysis plan presents a secondary Bayesian analysis of the SafeBoosC-III trial. The analysis and the final manuscript will be carried out and written after we publicise the primary frequentist trial report. Thus, we can interpret the findings from both the frequentists and Bayesian perspective. This approach should provide a better foundation for interpreting of our findings.
Trial registration
ClinicalTrials.org, NCT03770741. Registered on 10 December 2018.
Similar content being viewed by others

Introduction
Extremely preterm infants have a high mortality and morbidity [1, 2]. The SafeBoosC-II trial observed that cerebral oximetry monitoring by near-infrared spectroscopy (NIRS), plus a treatment guideline for the first three days of life, could potentially reduce the cerebral hypoxic burden [3]. There were also a trend towards reduced mortality and occurrence of severe brain injury in the intervention group, whereas the occurrence of bronchopulmonary dysplasia and retinopathy of prematurity tended to increase in this group [4]. As the SafeBoosC-II trial was insufficiently powered to detect a difference on these clinical outcomes, a larger trial was needed. Therefore, the pragmatic, multinational trial—the SafeBoosC III trial—evaluating the benefits and harms of cerebral oximetry monitoring plus an accompanying treatment guideline versus usual care—was conducted [5, 6].
The primary analyses of the SafeBoosC-III trial were carried out using frequentist statistical methods [7]. Bayesian statistical analyses are now more commonly used both as a standalone analysis of randomised clinical trials, primarily those of adaptive design but also as a sensitivity analysis of sequentially randomised clinical trials [8,9,10,11]. Previously, Bayesian analyses have nuanced the conventional frequentists statistics interpretation when the p values have been used with a dichotomous threshold of difference and interpreted to prove or disprove similarity between groups [12, 13].
Here, we present a secondary statistical analysis plan for a sensitivity analysis with a pre-defined statistical code of the SafeBoosC-III trial using Bayesian statistical analyses.
Methods
The SafeBoosC-III trial is an investigator-initiated, open-label, randomised, multinational, pragmatic, phase-III superiority clinical trial with a parallel-group design [5]. The trial methodology and design has previously been described in detail elsewhere [5]. The trial aims to evaluate the benefits and harms of cerebral oximetry monitoring by spatially resolved near-infrared spectroscopy (NIRS) plus a treatment guideline versus usual care. A total of 1601 infants were randomised with an allocation ratio of 1:1, stratified by site and gestational age (< 26 weeks compared to ≥ 26 weeks). Randomisation and initiation of cerebral oximetry monitoring should occur within 6 h of birth, and cerebral oximetry monitoring should continue for the first 72 h after birth [5]. The trial was registered on ClinicalTrials.gov (identification no. NCT03770741) before inclusion of the first participant on 10 December 2018. The consent workflow and eligibility criteria are described elsewhere [5]. Overall, all infants born before 28 weeks postmenstrual age with decision to provide full life support and with the possibility to initiate cerebral oximetry monitoring within 6 h after birth were eligible [5].
Trial status
The last participant was included 16 December 2021, and the primary frequentists analyses were carried out on 30 May 2022, and the main article has been published [6].
Outcomes
All outcomes are assessed when the infant is discharged from the hospital, at 36 weeks of postmenstrual age, or when the infant dies, whichever event occurs first. The primary outcome is a dichotomous composite outcome of death or severe brain injury, defined as one of the following: cerebral haemorrhage grade ≥ III (Papile’s classification) [14], cystic periventricular leukomalacia [15], cerebellar haemorrhage, post-haemorrhagic ventricular dilatation, or cerebral atrophy. The exploratory outcomes are (1) major neonatal morbidities associated with neurodevelopmental impairment later in life (count; 0 to 3) [16], (2) bronchopulmonary dysplasia (dichotomous), (3) retinopathy of prematurity stage 3 and above (dichotomous), (4) late-onset sepsis (dichotomous), and (5) necrotising enterocolitis stage 2 and above or focal intestinal perforation (dichotomous).
General analysis principles
Statistical analyses will be performed using Stata (StataCorp LLC, Texas, USA). Analyses in Stata 18 will follow the recommendation from the Stata Bayesian Reference Manual [17]. All randomised participants will be included in all analyses (intention-to-treat principle), and stratification variables will be included in all analyses (site and gestational age).
Rationale for Bayesian analyses
The conventional frequentist analyses of randomised clinical trials are often reported using an effect estimate, a confidence interval, and a p value. Despite advice to the contrary, the results are often interpreted in a dichotomous matter, based on the p-value chosen as threshold for ‘statistical significance’ and ‘no evidence of effect’ is confounded with ‘evidence of no effect’.
Bayesian analysis may provide information of the probability of benefits and harms, which may be more easily interpretable [18] and may be less susceptible to the long-standing tradition of misinterpreting results achieved using frequentist statistics [19].
Priors
The primary Bayesian analyses will use default non-informed priors as defined in Stata—normalprior—with a standard deviation of 10, which will be centred around no difference (i.e. centred around 0) and thus including all plausible effects. These default non-informed priors will also be used for covariates. As secondary Bayesian analyses, we will use an informative prior distribution generated from previous randomised clinical trials [20]. The included trials are based on information obtained through a systematic review [21].
Statistical analyses
The SafeBoosC-III trial has one primary and five exploratory outcomes. The outcomes are dichotomous, apart from one exploratory being a count outcome. The results from the analyses are in Bayesian statistics referred to as ‘posteriors’ and will be presented as point estimates and 95% credible intervals (CrIs), encompassing the most probable results based on the data, model, and priors selected.
Dichotomous outcomes
Dichotomous outcomes will be analysed using Bayesian logistic regression models with gestational age and site as control variables (or covariates). Effects on dichotomous outcomes will be presented as the adjusted relative risks (aRRs), adjusted odds ratios (aORs), and adjusted risk differences (aRDs), by comparing the probability of the outcome in the two intervention groups. We will calculate aRRs by applying exponential transformation to the simulated values and then summarise them [17]. Furthermore, we will estimate the probability of any benefit or harm and the probability of clinically important benefit or harm (see the ‘Interpretation of results’ section) (Table 1).
Count data outcome
The count data outcome, major neonatal morbidity count, ranges from 0 to 3 and will most likely present with a non-normal distribution. We will use Bayesian linear regression model with gestational age and site as covariates, corresponding to the planned primary frequentists analyses [7]. The large sample size is most likely sufficient to account for the non-normally distributed data [22]. Effects on the outcome will be presented as a mean difference (MD), by comparing the two intervention groups. Furthermore, the probability of any harm or benefit, together with the clinically important benefit and harm (see the ‘Interpretation of results’ section), will be presented (Table 1).
Model settings
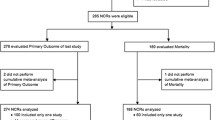
Every analysis will be carried out in accordance with the recommendation described in the Stata manual [17]. The models will use a Hamiltonian Monte Carlo sampler with 1 chain, a sampling of 10,000, and at least 25,000 iterations for the burn-in period [17]. Chain convergence will be evaluated by visual inspection of density, autocorrelation, histograms, and trace plots (Fig. 1) [23]. Trace plot should depict relative homogenous static noise without any visualisable patterns; the density plot illustrates convergence and is interpreted by estimating the similarities between the first and second half. Higher serial correlation typically has the effect of requiring more samples to obtain to a stationary distribution. If upon inspection of the autocorrelation plots looks ‘snake-like’ rather than like a hairy caterpillar, this might indicate that more simulations are required. Furthermore, each analysis will be evaluated in three chains using Gelman-Rubin convergence diagnostics and interpreted using 95 Ru which needs to be below 1.01 in order to accept the model [24,25,26].

Presentation of a model diagnostic plot including a trace plot, histogram, autocorrelation plot, and density plot. Trace plot (upper left) should depict relative homogenous static noise without any visualisable patterns. The histograms (upper light) must depict a normal distribution. The autocorrelation plot (lower left) indicates the degree of convergence and good convergence and thereby autocorrelation becomes negligible if a pattern of decrease and ends below 0.1. The density plot (lower right) also illustrates convergence and is interpreted by estimating the similarities between the first and second half
If convergence issues occur, we will gradually increase the sampling up to 50,000 and the burn-ins gradually up to 100,000. If this does not solve the issues, we will do the analyses by combining sites. Furthermore, if necessary, we will carry out the analysis with and without the problematic covariate(s) and present both analyses [17].
If the initial diagnostic inspection for convergence has proven satisfactory, we plan to assess if changes in the definition of the model result in significant changes in posterior inferences. We therefore plan to compare models with plausible but different priors (including different distributions) and to explore the consequences of inclusion or exclusion of different variables (https://m-clark.github.io/bayesian-basics/diagnostics.html).
Interpretation of results
The results will be presented as probability of any benefit or any harm, Bayes factor, and the probability of clinical important benefit or harm. Benefit will be defined as the probability that the adjusted RR (aRR) is below 1.0. Harm will be defined as the probability that the aRR is above 1.0. The probability of benefit or harm will be interpreted as high probability, if above 99%. Bayes factor will be estimated for all outcomes, and the Bayes factor described by Jakobsen and colleagues above 10 will be interpreted as a high probability of conformation of the null hypothesis [27]. For the primary outcome, clinically important benefit will be defined as the probability that the aRR is below 0.90, and clinically important harm will be defined as the probability that the aRR is above 1.10 for the primary outcome [7]. Sensitivity analyses using 0.97, 0.95, 0.85, 0.80, 0.75, and 0.70 as benefit and 1.03, 1.05, 1.10, 1.15, 1.20, 1.25, and 1.30 as harm will be carried out. For the exploratory outcomes, major neonatal morbidities associated with neurodevelopmental impairment later in life, bronchopulmonary dysplasia, and late-onset sepsis, an RR of 0.80 and 1.20 will be used to assess clinically important benefit and harm, respectively. For retinopathy of prematurity stage 3 and above secondary, an RR of 0.70 and 1.30 will be used. For necrotising enterocolitis stage 2 and above, an RR of 0.83 and 1.17 will be used. All these estimates relate to the primary sample size calculation and power estimations, and the rationale is described in the primary protocol in detail [7].
Handling of missing data
Missing data for each variable will be presented in detail, and decision about potential multiple imputation will follow the recommendations of Jakobsen and colleagues [28]. In brief, if missingness is less than 5%, we will carry out complete case analysis and present results from a best–worst and worst-best analyses as sensitivity analyses. Best–worst analysis assumes all missing data in the experimental group has the best possible outcome and those in the control group have the worst possible outcome, and vice versa for the worst-best analysis [28]. Multiple imputation will only be considered if missingness is more than 5%, less than 40%, and missing mechanism is assessed to be missing at random. If relevant, multiple imputation using all stratification variables (i.e. site and gestational age) and selective baseline variables (i.e. birth weight, gestational age, twin (yes/no), and sex) will be carried out. If multiple imputation is carried out, the posteriors will have similar weight in each imputed dataset.
Statistical reports
The statistical analyses are prepared with predefined coding for Stata (Supplemental material). The report is based on simulated data, which outlines the analyses chosen for the manuscript. Two statisticians will analyse the data independently following this protocol, where ‘A’ and ‘B’ refer to the two intervention groups which is randomly shuffled. The chosen analyses are based on this statistical analysis plan and pre-defined statistical code (Supplemental material). The results from the outcomes will be presented in two independent reports, which will be compared by the coordinating investigator, the two statisticians, and the co-authors. Based on the consensus from this meeting, a final statistical report will be developed, and based on this report, two abstracts will be written by the steering group: one assuming ‘A’ is the experimental group and ‘B’ is the control group and one assuming the opposite. These abstracts will use the results from the blinded final report, and when the blinding is broken, the ‘correct’ abstract will be chosen, and the conclusions in this abstract will not be revised. Furthermore, all three statistical reports will be published as Supplementary material.
Results
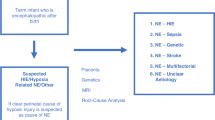
See Table 1 and Fig. 2 with simulated data prepared for the final manuscript.

Presentation of an analysis using simulated data. The vertical black line throughout the two plots represents no difference. The upper plot presents the posterior distribution, with the blue area representing the 95% credibility interval and the blue line showing the median value. The lower plot shows the cumulative posterior distribution
Discussion
This statistical analysis plan presents a pre-planned secondary Bayesian analysis of the SafeBoosC-III trial. The manuscript will be written after acceptance of our manuscript based on the primary frequentist analysis of the trial [6]; thus, we are able to interpret the findings from two perspectives, both the frequentists and the Bayesian perspective. This pre-planned approach will provide us with the best possible foundation for interpretation of the findings.
The previously addressed, often dichotomous interpretation of p values in frequentists statistics does not leave much room for interpretation [19, 29, 30]. Absence of evidence, measured by an insignificant p value, is often interpreted as evidence of absence of effect [19, 31]. This absence of evidence could merely be caused by a smaller effect size than the a priori estimated effect size. Thus, the more easily interpretable probability estimates in Bayesian statistics open for the possibility of clinicians and non-statisticians to interpret the results [32], especially the ability to present the probability of different definitions of benefit and harm may help inform future guidelines.
Strengths
The SafeBoosC-III trial has several strengths, which have previously been described in detail [5, 7]. In brief, the SafeBoosC-III trial is the largest trial in the field [6, 23], has a strict outcome hierarchy [27], and is accompanied by a pre-published design manuscript and frequentist statistical analysis plan [5, 7]. Moreover, the detailed handling of missing data and innovative central data monitoring process further increases the data quality of the trial [33]. The present Bayesian statistical analysis plan describes the analyses in detail, which will minimise the risks of selective reporting bias [34,35,36]. The details provided above are of a level that independent statisticians should be able to reproduce the statistical analyses [37, 38].
Limitations
The primary limitation of the SafeBoosC-III trial is the inherent difficulty to blind the intervention. This limitation has previously been addressed [5], but the potential bias has been mitigated by having blinded statisticians and blinded assessment of the subjective component of the primary outcome, severe brain injury, together with the blinded interpretation of results and formulation of the abstracts. The priors introduced by the Bayesian analyses might introduce bias; however, using weakly informed or uninformed priors as primary and evidence-based and sceptic priors as sensitivity analyses aims to minimise the influence of this potential bias.
Conclusion
This Bayesian statistical analysis plan for the SafeBoosC-III trial includes a detailed predefined description of how data will be analysed and presented for our secondary analyses. We have included detailed descriptions of the statistical considerations aimed to limit selective reporting bias. This statistical analysis plan will likely increase the validity of our results.
Availability of data and materials
The datasets will be made available after reasonable request to the steering committee of SafeBoosC-III, while the scripts for the reports will be made available after reasonable request to the corresponding author.
References
Stoll BJ, Hansen NI, Bell EF, Shankaran S, Laptook AR, Walsh MC, et al. Neonatal outcomes of extremely preterm infants from the NICHD Neonatal Research Network. Pediatrics. 2010;126:443–56.
Adams-Chapman I, Heyne RJ, DeMauro SB, et al. Neurodevelopmental Impairment Among Extremely Preterm Infants in the Neonatal Research Network. Pediatrics. 2018;141(5):e20173091. https://doi.org/10.1542/peds.2017-3091.
Pellicer A, Greisen G, Benders M, Claris O, Dempsey E, Fumagalli M, et al. The SafeBoosC phase II randomised clinical trial: a treatment guideline for targeted near-infrared-derived cerebral tissue oxygenation versus standard treatment in extremely preterm infants. Neonatology. 2013;104:171–8.
Hyttel-Sorensen S, Pellicer A, Alderliesten T, Austin T, Van Bel F, Benders M, et al. Cerebral near infrared spectroscopy oximetry in extremely preterm infants: Phase II randomised clinical trial. BMJ [Internet]. 2015;350:1–11. Available from: https://doi.org/10.1136/bmj.g7635
Hansen ML, Pellicer A, Gluud C, Dempsey E, Mintzer J, Hyttel-Sørensen S, et al. Cerebral near-infrared spectroscopy monitoring versus treatment as usual for extremely preterm infants: a protocol for the SafeBoosC randomised clinical phase III trial. Trials Trials. 2019;20:1–11.
Hansen ML, Pellicer A, Hyttel-Sørensen S, Ergenekon E, Szczapa T, Hagmann C, et al. Cerebral oximetry monitoring in extremely preterm infants. N Engl J Med. 2023;388:1501–11.
Hansen ML, Pellicer A, Gluud C, Dempsey E, Mintzer J, Hyttel-Sorensen S, et al. Detailed statistical analysis plan for the SafeBoosC III trial: a multinational randomised clinical trial assessing treatment guided by cerebral oxygenation monitoring versus treatment as usual in extremely preterm infants. Trials Trials. 2019;20:1–12.
Mølgaard Nielsen F, Lass Klitgaard T, Granholm A, et al. Higher versus lower oxygenation targets in COVID-19 patients with severe hypoxaemia (HOT-COVID) trial: Protocol for a secondary Bayesian analysis. Acta Anaesthesiol Scand. 2022;66(3):408–14. https://doi.org/10.1111/aas.14023.
Angus DC, Derde L, Al-Beidh F, Annane D, Arabi Y, Beane A, et al. Effect of hydrocortisone on mortality and organ support in patients with severe COVID-19: the REMAP-CAP COVID-19 corticosteroid domain randomized clinical trial. JAMA. 2020;324:1317–29.
Angus DC, Berry S, Lewis RJ, Al-Beidh F, Arabi Y, van Bentum-Puijk W, et al. The REMAP-CAP (Randomized Embedded Multifactorial Adaptive Platform for Community-acquired Pneumonia) study. Rationale and Design. Ann Am Thorac Soc. 2020;17:879–91.
Granholm A, Alhazzani W, Derde LPG, Angus DC, Zampieri FG, Hammond NE, et al. Randomised clinical trials in critical care: past, present and future. Intensive Care Med. 2022;48:164–78.
Granholm A, Munch MW, Myatra SN, Vijayaraghavan BKT, Cronhjort M, Wahlin RR, et al. Dexamethasone 12 mg versus 6 mg for patients with COVID-19 and severe hypoxaemia: a pre-planned, secondary Bayesian analysis of the COVID STEROID 2 trial. Intensive Care Med. 2022;48:45–55.
COVID STEROID 2 Trial Group, Munch MW, Myatra SN, Vijayaraghavan BKT, Saseedharan S, Benfield T, et al. Effect of 12 mg vs 6 mg of dexamethasone on the number of days alive without life support in adults with COVID-19 and severe hypoxemia: the COVID STEROID 2 randomized trial. JAMA. 2021;326:1807–17.
Papile LA, Burstein J, Burstein R, Koffler H. Incidence and evolution of subependymal and intraventricular hemorrhage: a study of infants with birth weights less than 1,500 gm. J Pediatr. 1978;92:529–34.
Volpe JJ. Brain injury in the premature infant: overview of clinical aspects, neuropathology, and pathogenesis. Semin Pediatr Neurol. 1998;5:135–51.
Holsti A, Serenius F, Farooqi A. Impact of major neonatal morbidities on adolescents born at 23–25 weeks of gestation. Acta Paediatr. 2018;107:1893–901.
Stata Bayesian Analysis Reference Manual Release 18 [Internet]. 2022 [cited 2023 May 28]. Available from: https://www.stata.com/manuals/bayes.pdf
Hackenberger BK. Bayes or not Bayes, is this the question? Croat Med J. 2019;60:50–2.
Greenland S, Senn SJ, Rothman KJ, Carlin JB, Poole C, Goodman SN, et al. Statistical tests, P values, confidence intervals, and power: a guide to misinterpretations. Eur J Epidemiol. 2016;31:337–50.
Salpeter SR, Cheng J, Thabane L, Buckley NS, Salpeter EE. Bayesian meta-analysis of hormone therapy and mortality in younger postmenopausal women. AJM. 2009;122:1016-1022.e1.
Hansen ML, Hyttel-Sørensen S, Jakobsen JC, Gluud C, Kooi EMW, Mintzer J, et al. Cerebral near-infrared spectroscopy monitoring (NIRS) in children and adults: a systematic review with meta-analysis. Pediatr Res [Internet]. 2022; Available from: http://www.ncbi.nlm.nih.gov/pubmed/35194162
Li X, Wong W, Lamoureux EL, Wong TY. Are linear regression techniques appropriate for analysis when the dependent (outcome) variable is not normally distributed? Invest Ophthalmol Vis Sci. 2012;53:3082–3.
Gelman A, Carlin JB, Stern HS, Dunson DB, Vehtari A, Rubin DB. Bayesian Data Analysis Third edition (with errors fixed as of 15 February 2021). Chapman and Hall/CRC; 2013. http://www.stat.columbia.edu/~gelman/book/BDA3.pdf.
Vehtarh A, Gelman A, Simpson D, Carpenter B, Burkner PC. Rank-normalization, folding, and localization: an improved (formula presented) for assessing convergence of MCMC (with discussion)*†. Bayesian Anal. 2021;16:667–718.
Gelman A, Rubin DB. Inference from iterative simulation using multiple sequences. Stat Sci. 1992;7:457–511.
Brooks SP, Gelman A. General methods for monitoring convergence of iterative simulations. J Comput Graph Stat. 1998;7:434–55.
Jakobsen JC, Gluud C, Winkel P, Lange T, Wetterslev J. The thresholds for statistical and clinical significance - a five-step procedure for evaluation of intervention effects in randomised clinical trials. BMC Med Res Methodol. 2014;14:34.
Jakobsen JC, Gluud C, Wetterslev J, Winkel P. When and how should multiple imputation be used for handling missing data in randomised clinical trials - a practical guide with flowcharts. BMC Med Res Methodol. 2017;17:162.
Greenland S, Poole C. Living with P values: resurrecting a bayesian perspective on frequentist statistics. Epidemiology. 2013;24:62–8.
Gagnier JJ, Morgenstern H. Misconceptions, misuses, and misinterpretations of P values and significance testing. J Bone Joint Surg Am. 2017;99:1598–603.
Altman DG, Bland JM. Absence of evidence is not evidence of absence. BMJ. 1995;311:485.
Amrhein V, Greenland S, McShane B. Scientists rise up against statistical significance. Nature. 2019;567:305–7.
Olsen MH, Hansen ML, Safi S, Jakobsen JC, Greisen G, Gluud C, et al. Central data monitoring in the multicentre randomised SafeBoosC-III trial – a pragmatic approach. BMC Med Res Methodol. 2021;21:1–10.
Dwan K, Altman DG, Clarke M, Gamble C, Higgins JPTT, Sterne JACC, et al. Evidence for the selective reporting of analyses and discrepancies in clinical trials: a systematic review of cohort studies of clinical trials. PLoS Med. 2014;11: e1001666.
Kirkham JJ, Dwan KM, Altman DG, Gamble C, Dodd S, Smyth R, et al. The impact of outcome reporting bias in randomised controlled trials on a cohort of systematic reviews. BMJ. 2010;340:637–40.
Dwan K, Gamble C, Williamson PR, Altman DG. Reporting of clinical trials: a review of research funders’ guidelines. Trials. 2008;9:66.
Gamble C, Krishan A, Stocken D, Lewis S, Juszczak E, Doré C, et al. Guidelines for the content of statistical analysis plans in clinical trials. JAMA. 2017;318:2337–43.
Finfer S, Bellomo R. Why publish statistical analysis plans? Crit Care Resusc. 2009;11:5–6.
Acknowledgements
We thank the investigators and parents of participants globally for making this randomised clinical trial possible.
Collaborators
The SafeBoosC-III trial group consists of (listed in alphabetically order by forename) and should be defined as seen in ‘Collaborator Names’ section in Authorship in MEDLINE (nih.gov):
Adelina Pellicer (La Paz University Hospital, Madrid, Spain);
Afif El-Kuffash (The Rotunda Hospital, Dublin, Ireland);
Agata Bargiel (Warsaw University of Medical Sciences, Warszawa, Poland);
Ana Alarcon (Hospital Sant Joan de Deu, Barcelona, Spain);
Andrew Hopper (Loma Linda University Children’s Hospital, Los Angeles, United States);
Anita Truttmann (University Hospital Center of Lausanne, Lausanne, Switzerland);
Anja Hergenhan (Children's Hospital Lucerne, Lucerne, Switzerland);
Anja Klamer (Odense University Hospital, Odense, Denmark);
Anna Curley (National Maternity Hospital, Holles Street, Dublin, Ireland);
Anne Marie Heuchan (Royal Hospital for Children, Glasgow, United Kingdom);
Anne Smits (University Hospitals Leuven, Leuven, Belgium);
Asli Cinar Memisoglu (Marmara University Research and Educational Hospital, Istanbul, Turkey);
Barbara Krolak-Olejnik (Wroclaw Medical University, Wrocław, Poland);
Beata Rzepecka (Centrum Medycne “Ujastek” Sp. z.o.o, Kraków, Poland);
Begona Loureiro Gonzales (University Hospital Cruces, Barakaldo, Spain);
Beril Yasa (Basaksehir Cam and Sakura City Hospital, Istanbul, Turkey);
Berndt Urlesberger (University Hospital Graz, Graz, Austria);
Catalina Morales-Betancourt (12 de Octubre University Hospital, Madrid, Spain);
Chantal Lecart (Grand Hopital de Charleroi, Belgium);
Claudia Knöepfli (University Hospital Zurich, Switzerland);
Cornelia Hagmann (University Hospital Zürich, Switzerland);
David Healy (University College Cork, Cork, Ireland);
Ebru Ergenekon (Gazi University hospital, Turkey);
Eleftheria Hatzidaki (University Hospital of Heraklion, Greece);
Elena Bergon-Sendin (12 de Octubre University Hospital, Madrid, Spain);
Eleni Skylogianni (University of Patras General Hospital, Patras, Greece);
Elzbieta Rafinska-Wazny (Centrum Medyczne "Ujastek" Sp. z o.o., Krakow, Poland);
Emmanuele Mastretta (Ospedale S.Anna – Cita della Salute e della Scienza di Torino, Turin, Italy);
Eugene Dempsey (University College Cork, Cork, Ireland);
Eva Valverde (La Paz University Hospital, Madrid, Spain);
Evangelina Papathoma (“Alexandra” University and State Maternity Hospital, Athens, Greece);
Fabio Mosca (Fondazione IRCCS Ca’ Granda Ospedale Maggiore Policlinico, Milan, Italy);
Gabriel Dimitriou (University of Patras General Hospital, Patras, Greece);
Gerhard Pichler (University Hospital Graz, Graz, Austria);
Giovanni Vento (Fondazione Policlinico Universitario A. Gemelli IRCCS, Rome, Italy);
Gitte Holst Hahn (Copenhagen University Hospital, Copenhagen, Denmark);
Gunnar Naulaers (University Hospitals Leuven, Leuven, Belgium);
Guoqiang Cheng (Children's Hospital of Fudan University, Shanghai, China);
Hans Fuchs (Medical Center, University of Freiburg, Freiburg, Germany);
Hilal Ozkan (Bursa Uludag University Hospital, Bursa, Turkey);
Isabel De Las Cuevas (Marqués De Valdecilla University Hospital, Santander, Spain);
Itziar Serrano-Vinuales (Miguel Servet University Hospital, Zaragoza, Spain);
Iwona Sadowska-Krawczenko (Collegium Medicum in Bydgoszcz Nicolaus Cupernicus University in Torun, Bydgoszcz, Poland);
Jachym Kucera (The Institute for the Care of Mother and Child, Prague, Czech Republic);
Jakub Tkaczyk (University Hospital Motol, Prague, Czech Republic);
Jan Miletin (Coombe Women and Infant University Hospital, Dublin, Ireland);
Jan Sirc (The Institute for the Care of Mother and Child, Prague, Czech Republic);Jana Baumgartner (Medical Center, University of Freiburg, Freiburg, Germany);
Jonathan Mintzer (Mountainside Medical Center, Montclair, United States);
Julie De Buyst (Tivoli Hospital, La Louviere, Belgium);
Karen McCall (University Hospital Wishaw, Wishaw, United Kingdom);
Konstantina Tsoni (Ippokrateion General Hospital of Thessaloniki, Thessaloniki, Greece);
Kosmas Sarafidis (Ippokrateion General Hospital of Thessaloniki, Thessaloniki, Greece);
Lars Bender (Aalborg University Hospital, Aalborg, Denmark);
Laura Serrano Lopez (Virgen De Las Nieves University Hospital, Granada, Spain);
Le Wang (Children’s Hospital of Fudan University, Shanghai, China);
Liesbeth Thewissen (University Hospitals Leuven, Leuven, Belgium);
Lin Huijia (Children's Hospital of Zheijang, Hangzhou, China);
Lina Chalak (UT Southwestern Medical Center, Dallas, United States);
Ling Yang (Hainan Women and Children’s Medical Center, Hainan, China);
Luc Cornette (AZ St. Jan Bruges, Bruges, Belgium);
Luis Arruza (Hospital Clinico San Carlos, Madrid, Spain);
Maria Wilinska (Centre of Postgraduate Medical Education, Warsaw, Poland);
Mariana Baserga (University of Utah Hospital, Salt Lake City, United States);
Marie Isabel Skov Rasmussen (Copenhagen University Hospital, Copenhagen, Denmark);
Marta Mencia Ybarra (La Paz University Hospital, Madrid, Spain);
Marta Teresa Palacio (Hospital Clínic Barcelona, Barcelona, Spain);
Martin Stocker (Children’s Hospital Lucerne, Lucerne,, Switzerland);
Massimo Agosti (“Fillipo del Ponte” Hospital, Varese, Italy);
Merih Cetinkaya (Kanuni Sultan Süleyman Training and Research Hospital, Istanbul,, Turkey);
Miguel Alsina (Hospital Clinic Barcelona, Barcelona, Spain);
Monica Fumagalli (Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, Milan, Italy);
Munaf M. Kadri (Loma Linda University Children's Hospital, Los Angeles, United States);
Mustafa Senol Akin (Ankara City Hospital, Ankara, Turkey).
Münevver Baş (Gazi University Hospital, Ankara, Turkey);
Nilgun Koksal (Bursa Uludag University Hospital, Bursa, Turkey);
Olalla Otero Vaccarello (Hospital Universitario De Tarragona Juan XXIII, Tarragona, Spain);
Olivier Baud (Children’s University Hospital of Geneva, Geneva, Switzerland);
Pamela Zafra (Puerta Del Mar University Hospital, Cadiz, Spain);
Peter Agergaard (Aarhus University Hospital, Aarhus, Denmark);
Peter Korcek (The Institute for the Care of Mother and Child, Prague, Czech Republic);
Pierre Maton (Clinique CHC Montlegia, Liege, Belgium);
Rebeca Sanchez-Salmador (La Paz University Hospital, Madrid, Spain);
Ruth del Rio Florentino (Hospital De Sant Joan De Deu, Barcelona, Spain);
Ryszard Lauterbach (Jagiellonian University Hospital, Kraków, Poland);
Salvador Piris Borregas (12 De Octubre University Hospital, Madrid, Spain);
Saudamini Nesargi (St Johns Medical College Hospital, Karnataka, India);
Serife Suna (Ankara City Hospital, Ankara, Turkey).
Shashidhar Appaji Rao (St Johns Medical College Hospital, Karnataka, India);
Shujuan Zeng (Longgang district Central Hospital, Shenzhen, China);
Silvia Pisoni (Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, Milan, Italy);
Simon Hyttel-Sørensen (Copenhagen University Hospital, Copenhagen, Denmark);
Sinem Gulcan Kersin (Marmara University Research and Education Hospital, Istanbul, Turkey);
Siv Fredly (Oslo University Hospital, Oslo, Norway);
Suna Oguz (Ankara City Hospital, Ankara, Turkey);
Sylwia Marciniak (Specialist Hospital No.2, Bytom, Poland).
Tanja Karen (University Hospital Zürich, Zürich, Switzerland);
Tomasz Szczapa (Poznan University of Medical Sciences, Poznan, Poland);
Tone Nordvik (Oslo University Hospital, Oslo, Norway);
Veronika Karadyova (University Hospital Motol, Prague, Czech Republic);
Xiaoyan Gao (Maternal and Child Health Hospital of Zhuang Autonomous Region, Guangxi, China);
Xin Xu (Xiamen Children's Hospital, Xiamen, China);
Zachary Vesoulis (St. Louis Children’s Hospital, St. Louis, United States);
Zhang Peng (Children’s Hospital of Fudan University, Shanghai, China);
and Zhaoqing Yin (The People's Hospital of Dehong, Dehong, China).
Funding
Open access funding provided by Royal Library, Copenhagen University Library The Copenhagen Trial Unit, Centre for Clinical Intervention Research, The Capital Region, Copenhagen University Hospital ─ Rigshospitalet, Copenhagen, Denmark.
Author information
Authors and Affiliations
Consortia
Contributions
The study was designed by MHO, MLH, JCJ, GG, and CG. Data was collected by the collaborators (see below). The first version of the manuscript was written by MHO and CG; all authors revised the manuscript; and all authors and collaborators (see below) approved the final version.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Olsen, M.H., Hansen, M.L., Lange, T. et al. Detailed statistical analysis plan for a secondary Bayesian analysis of the SafeBoosC-III trial: a multinational, randomised clinical trial assessing treatment guided by cerebral oximetry monitoring versus usual care in extremely preterm infants. Trials 24, 737 (2023). https://doi.org/10.1186/s13063-023-07720-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13063-023-07720-3