
Abstract
Background
Medial knee osteoarthritis (OA) is a common health problem resulting in knee pain and limiting patients’ physical activity. After failed conservative treatment, unicompartmental knee arthroplasty (UKA) and high tibial osteotomy (HTO) are possible surgical treatment options for this condition. There is a paucity of high-quality evidence in the literature comparing objective and subjective outcomes of these procedures. Also, there is no common agreement on whether these procedures provide comparable results in late-stage medial knee OA patients.
Methods
We will perform a prospective randomized controlled trial comparing HTO and UKA in patients with late-stage medial knee OA. 100 patients with isolated medial knee OA (KL III–IV) are assigned to either UKA (n = 50) or HTO (n = 50) procedure in patients 45–65 years of age. Our primary outcome will be KOOS5 at one year postoperatively. Secondary outcomes include OARSI physical assessment, length of stay, wearable activity watch, radiographs (OA progression according to Kellgren-Lawrence classification), patient-reported outcomes (KOOS subscales, pain visual analog scale [VAS], Lysholm, and Oxford knee scores), and adverse events (conversion to total knee arthroplasty, surgery-related complications, need for revision surgery) outcomes. Our hypothesis is that neither of the interventions is superior as measured with KOOS5 at 12 months.
Ethics and dissemination
The institutional review board of the Helsinki and Uusimaa Hospital District has approved the protocol. We will disseminate the findings through peer-reviewed publications.
Trial registration
ClinicalTrials.gov/TooloH NCT05442242. Registered on 7/1/2022.
Similar content being viewed by others


Introduction
Knee osteoarthritis (OA) is a common medical condition negatively affecting patients’ everyday lives and creating economic burden to societies [1,2,3]. Knee OA is often related to varus deformity and has various treatment options [4]. After failed nonsurgical care, total knee arthroplasty (TKA) has been the gold-standard treatment. Although TKA has proven superiority over nonsurgical care, [5] around 20% of patients are not satisfied with TKA [6,7,8]. In addition to TKA, unicompartmental knee arthroplasty (UKA) and high tibial osteotomy (HTO) are widely accepted treatment options in isolated unicompartmental OA [9]. Also, after failed UKA or HTO there is a possibility to convert to TKA.
In UKA, the damaged cartilage of the affected compartment is replaced by intra-articular implants. In a recent multicenter randomized controlled trial (RCT), UKA resulted in similar clinical outcomes and similar number of reoperations and complications compared with TKA. The cost-effectiveness of UKA was superior to TKA [10]. It has been estimated that 25–48% of knee OA patients would be suitable for UKA [4, 11]. However, the UKA rate has varied between 8 and 12.2% in different countries [12]. This suggests that UKA should be considered more often in patients with isolated medial compartment OA.
In HTO, the mechanical axis of the lower limb is corrected using an extra-articular osteotomy to shift weight towards the healthy lateral compartment in patients with medial knee OA and varus malalignment. The osteotomy can be performed with open or closed wedge technique [13]. While different complication profiles have been described, similar outcomes of these two methods have been reported [14]. Traditionally, HTO has been considered an option for younger active patients with a less severe OA. However, there is a paucity of high-quality evidence in the literature to support this assumption and in recent studies, HTO has been used in late-stage OA with good long-term results [15].
Recently, Jin et al. reported the first long-term follow-up results comparing HTO with UKA [16]. They found that WOMAC scores were superior in the UKA group but found no other significant differences between the groups in survival rates, complication rates, or OA progression. This study was performed using Propensity score matching (PSM) from a retrospective data.
To our knowledge, there are no previous RCTs comparing UKA with HTO in the treatment of late-stage medial knee OA. To fill this evidence gap, we designed this RCT to compare HTO and UKA in patients with medial late-stage OA of the knee with the following hypotheses.
-
1.
Null hypothesis is that there is no clinically significant difference between HTO and UKA in the primary outcome measure (The Knee Injury and Osteoarthritis Outcome Score composite, KOOS5) at 12 months postoperatively.
-
2.
There is no significant difference in rehabilitation time after surgery between HTO and UKA as measured with KOOS5 at follow-up timepoints.
-
3.
We expect no progression in lateral compartment OA in imaging studies during follow-up.
Methods and analyses
Study setting
This study is a randomized controlled, pragmatic single-center, parallel-group, 1:1 superiority trial. Our goal is to compare the effect of HTO and UKA in patients with late-stage medial knee OA. The study will take place in Helsinki University Hospital. Approximately 50 UKAs and 50 HTOs are performed in our hospital every year.
Eligibility criteria
Orthopedic surgeons identify potential study participants from the referrals to outpatient clinics. Patients are scheduled for an outpatient visit to a surgeon member of the study group. Patients aged between 45 and 65 years with primary medial unicompartmental knee OA (Kellgren-Lawrence [KL] III–IV) [17] with varus deformity of 4 degrees or more can participate in the study. The patients are diagnosed according to clinical and radiologic examinations including MRI, weight-bearing knee, and mechanical axis radiographs. The patients meeting the inclusion criteria are asked to participate in the study. Written information and a consent form are given to the patient at the outpatient clinic. If the patient is willing to participate in the trial, they are scheduled for an appointment to the outpatient clinic once more for randomization and baseline measures. The detailed inclusion and exclusion criteria are shown in Table 1.
Interventions
After recruitment, the patients are scheduled an appointment with a physical therapist and an individual training program is introduced. Patients are randomized to either HTO or UKA in 1:1 ratio. If the patients’ symptoms are reduced markedly before the operative treatment (1–4 months post randomization) a possibility for drop-out is offered. Both UKA and HTO operations are performed by experienced surgeons with at least 50 operations of UKA or HTO in total.
Surgical technique
HTO — high tibial osteotomy (open wedge)
An open wedge HTO is a standard approach in our clinic and thus used as the surgical technique in this study. Weight-bearing mechanical axis radiograph is used to plan the desired correction. An arthroscopy of the knee is performed first to determine the degree of OA. Arthrosis of the lateral and medial TF joint is graded by the modified Outerbridge classification [18, 19]. Patients with lateral OA grade II or greater are excluded from the study at this point. Cruciate ligaments and menisci are also evaluated in the arthroscopy.
A medial high tibial open wedge osteotomy is performed using a diagonal incision just cranial to pes anserinus tendons or a medial longitudinal incision. Pes anserinus tendons are retracted distally and the superficial medial collateral ligament is exposed and incised at the level of the planned osteotomy. Two parallel K-wires are inserted under image intensifier to mark the osteotomy level. Patellar tendon is protected and a biplanar osteotomy line is created using an oscillating saw and osteotomes leaving the lateral cortex intact and the tibial tubercle to the distal side of the osteotomy. Thin osteotomes are used to open the osteotomy after sawing to achieve the desired correction (Fujisawa point) [20]. The osteotomy site is secured using a medial locking plate (TomoFix®, DePuy Synthes, Raynham, MA, USA). The wound is closed in a standard manner. Local infiltration analgesia is used for all patients. An elastic bandage is applied. Weight-bearing as tolerated is allowed immediately after the surgery.
UKA — unicompartmental knee arthroplasty
Oxford® Partial Knee (Zimmer Biomet, Warsaw, IN, USA) arthroplasty (PKA) is performed from medial parapatellar arthrotomy without dislocating the patella. Tourniquet is used for every patient if no contraindications exist. Retropatellar fat pad is partially resected if necessary, to ensure adequate surgical visualization. The anterior cruciate ligament is inspected for possible ligament rupture and fibrillation, and lateral and patellofemoral joint compartments are inspected for possible cartilage damage. Patients with lateral OA grade II or greater are excluded from the study at this point. Grade of medial femoral and tibial cartilage loss is verified. All osteophytes are removed from the intercondylar notch, medial margin of the medial condyle, tibial plateau, and patella. PKA instrumentation and implantation are performed according to the cementless Oxford® PKA Microplasty® (Zimmer Biomet, Warsaw, IN, USA) instrumentation system technique. Local infiltration analgesia is used for all patients. The wound is closed in a standard manner. An elastic bandage is applied. Full weight-bearing is allowed immediately after the surgery [21].
Outcomes
The outcomes of this study consist of objective and patient-reported outcomes. The outcomes will be collected at randomization, preoperative visit, and postoperatively 3, 6, and 12 months. We will follow up the participants thereafter at 2, 5, and 10 years via letter survey.
Baseline data
Baseline data is collected at the time of randomization at the outpatient clinic. These include radiographs of the affected knee, weight-bearing mechanical axis, MRI, KOOS5, Lysholm, Oxford knee score, and Osteoarthritis Research Society International (OARSI) performance-based measures. The patients receive an activity watch (Withings Move®, Issy-les-Moulineaux, France), which they are asked to use day and night throughout the trial.
Primary outcome measure
The Knee Injury and Osteoarthritis Outcome Score (KOOS) is a validated patient-reported outcome measure (PROM) assessing the outcomes of various knee conditions [22]. The tool consists of five subscales: pain, other symptoms, activities of daily living, function in sports or recreational activities, and quality of life. We will use the KOOS5 composite score as the primary outcome measure. Based on clinical experience and literature, there will be only minimal change in pain and PROM scores after 1 year postoperatively [23]. Thus, the primary outcome measure, KOOS5 score for HTO vs. UKA is analyzed 12 months postoperatively. A minimal clinically important difference (MCID) of 10 points will be used [24].
Secondary outcome measures
Secondary outcome measures are divided into objective (OARSI, length of stay, Withings activity measures, Radiographs [KL and OA progression]), patient-reported (KOOS subscales, pain visual analog scale [VAS], Lysholm, and Oxford knee scores), and adverse events (conversion to TKA, complications [peri- and postoperative], need for revision surgery) outcomes.
In addition to KOOS5, additional PROMs are gathered from the Lysholm score (MCID, 4.2 points) [25] and Oxford knee score (MCID, 5 points) [26]. We will also report KOOS subscales individually (ADL, Pain, Symptoms, Quality of life, Sport/Rec) [27].
Average pain for the previous 2 weeks is measured using VAS, which is validated to knee OA pain (MCID, 17 mm) [28, 29].
The OARSI performance-based tests are performed by a physical therapist at baseline and at follow-up visits as shown in the participant timeline in Table 2. This includes 30-s chair stand test (MCID, 2 repetitions), 40-m fast-paced walk test (MCID, 0.2 m/s), stair climb test (MCID, 5.5 s), the timed up and go test (MCID: reduction of 0.8 s), and 6-min walk test (MCID, 20 m increase) [30].
After the surgery, the days spent in the hospital will be recorded to follow the early recovery. Early readmissions within 90 days after surgery for any reason are reported for the analysis of possible complications. See safety considerations for the list of complications monitored.
The OA progression is monitored at the follow-up visits using radiographs of the knee at 3, 6, and 12 months after surgery, and the mechanical axis is re-evaluated at 12 months post-randomization. Patients not satisfied with the results of operative treatment (HTO or UKA) can be converted to TKA at any time during the follow-up.
For later determining the MCID of KOOS5 in this study, we will include an anchor question to the trial: “If you think about your pain level and daily activities this week, would it be acceptable that your knee would be like this for the rest of your life?”. The answer options are “Yes” or “No.” The proportion of patients reaching the Patient Acceptable Symptom State (PASS) be analyzed from the answers to this question.
We will use the Withings Move electronic watch as an activity tracker. The watches are given to patients right after randomization and the patients are asked to wear them for 24 h per day until the primary time-point of 12 months. The following data are recorded: ID number, date, time, number of steps per day, and sleeping hours. The watch is connected to a secured database and the data is wirelessly transferred and stored.
Cost-effectiveness
The consumption of healthcare and social services, used implants, pain medication, and alternative medical services and all related costs will be included in the cost-effectiveness analysis. The costs and benefits will be evaluated against the difference in our primary outcome and in the results of the KOOS quality of life subscale. Used implants, pain medication, and consumption of alternative therapies (i.e., osteopath, chiropractor, naprapath, healer) will be recorded.
The outcome measures are summarized in Table 3.
Safety considerations
Adverse surgical complications (deep wound infection, deep venous thrombosis, mechanical failure, post-operative fracture, neurologic complication) and minor complications (superficial wound infection, pain) are collected and reported in the results.
Sample size
The sample size calculation was performed using G*Power 3.1 and was based on KOOS5 as the primary outcome measure in this trial. For the sample size calculation, we used a two-sided α level of 0.05. We assumed the MCID of the KOOS5 to be 10 points, [27, 31] with an SD of 15 points. Using these assumptions, the required sample size is 36 per group with 80% power to show a clinically important difference between the treatment methods with a two-sided type I error rate of 5%. With the assumption of 36% lost to follow-up, we decided to include 50 participants per group.
Allocation
Block randomization will be used in this study. A person not involved in the execution of the trial generates the randomization list using block randomization. The same person prepares sealed envelopes containing the treatment allocation information (HTO/UKA). The block size is not revealed to the study group before analyses. The envelopes are stored in a secure place at the study center. After receiving the informed consent, a surgeon member of the study gives a sealed envelope to the patient containing the treatment allocation information, and the surgery is arranged accordingly.
Blinding
The physical therapist will be blinded from the treatment allocation when collecting the objective measurements. The patient will be wearing long trousers during the follow-up visits and asked not to reveal the given treatment. The blinding of operative treatment is not possible for the personnel executing the operative treatment nor the patients.
Statistical analyses
We will conduct all primary and secondary analyses according to the intention-to-treat principle. The Consolidated Standards of Reporting Trials statement will be used in the reporting of the trial results [32].
We will conduct the primary comparison (KOOS5 composite score) between the study groups using a mixed-model repeated-measures analysis of variance (MMRM ANOVA) allowing possible data missingness. We will assume data missing at random. Study group and time of assessment will be used as fixed factors and patients will be used as random factors. We are using the model to quantify the treatment effect as the absolute difference between the groups in KOOS5 (mean and 95% confidence interval [CI]) and p-value at 12 months postoperatively. A two-sided p-value of 0.05 will be used to indicate statistical significance.
We will compare secondary outcomes using a similar model where applicable (e.g., KOOS subscales, pain-VAS, Lysholm, Oxford knee score, OARSI). Radiological classification (KL- classification) is used for covariate in post hoc analysis. For categorical response variables, we will analyze the effects using the generalized estimating equations model with the unstructured correlation structure. Secondary outcomes will be considered explanatory and/or exploratory. Thus, multiplicity is not considered a problem. We will report adverse events descriptively.
We plan to perform a sensitivity analysis according to as-treated principle where the patients are analyzed according to their definitive treatment method irrespective of the randomization.
Data monitoring
Data monitoring committee, interim analyses, or stopping guidelines are not included in this study because both operative treatment options are already in daily practice and the results have been acceptable.
Harms
All complications and harms are reported in the results section of this study. Major and minor complications are listed in the safety consideration section.
Protocol amendments
In the case of modification of the study protocol, all changes will be updated to ClinicalTrials.gov.
Confidentiality
Trial data will be stored in a secure storage at the study center for 10 years after the completion of the study. All data will be handled according to the principles of the GDPR.
Participant timeline
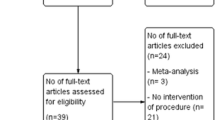
The participant timeline is represented in Table 2 and the flow chart is in Fig. 1.

Study flow chart
Implementation
The recruitment is done by the surgeon member of the study. After receiving the written consent, the surgeon member opens the envelope, and the patient is then randomized to one of the study groups. A physical therapist does the baseline measures, and the patient receives a written guide for exercise therapy.
Secondary cohort study
Eligible patients declining randomization are offered to participate in a concurrent observational cohort (“declined cohort”). In addition, patients who are ineligible for the RCT but are treated with either UKA or HTO are asked to take part in a second cohort study (“ineligible cohort”). Those consenting to these cohorts can choose their preferred treatment method after information on both treatment methods is given. Both cohorts are followed up according to the same principles as the participants of the RCT. The results of the declined and ineligible cohorts will be analyzed separately from the RCT.
Data collection and management
The data is collected by the physical therapist and research nurse using paper forms. The original paper forms are evaluated visually, and missing data is acquired if possible. From the paper forms the data is secured in an electronic archive. Only the research nurse is allowed to access the data during data gathering. In case of missing items in the master data, the original paper forms are reassessed and if needed the patient is contacted.
Blinded data interpretation
All data collected are interpreted by a blinded scheme. A statistician provides results from each arm of the study labeled A and B. The writing committee then analyzes the results and a consensus on all alternative interpretations is agreed. After a common agreement has been reached, the statistician reveals the randomization code, the correct interpretation is chosen, and the manuscript is finalized [33].
Ancillary and post-trial care
Patients will be treated during and after the trial with best intention. If malpractice has taken place, patients will not receive any compensation beyond those from the Finnish Patient Insurance Centre.
Discussion
Both UKA and HTO have been used in clinical practice for treating late-stage unicompartmental knee OA but to our knowledge, there are no previous RCTs comparing UKA with HTO in patients with this condition. In general, HTO has been recommended for younger more active adults with a low-grade unicompartmental OA [9, 15]. However, HTO has been used also in OA patients with higher grade OA [34, 35] and is considered to share indications with UKA in some cases [36]. Thus, we chose to study patients with KL grade III–IV OA.
We will use KOOS5 as the primary outcome as we feel that the outcome should be primarily analyzed by the subjective feeling of the patient. A Finnish version of the KOOS score has been appropriately translated and culturally adapted and it has demonstrated good validity and reliability [22]. Additionally, most of our secondary outcomes will be patient-reported as we feel that the most important result of the intervention is the patient’s subjective feeling rather than any objective measure.
As a novel objective measure, a Withings Move activity watch is used for counting the number of steps and hours of sleep per day. This watch has been validated for counting steps and also for analyzing the hours of sleep [37]. We will use the same device in every group for all patients. These objective measures will add to the OARSI performance-based tests used in various OA studies.
Generalizability
Although OA of the knee is very common, not every OA patient meets the inclusion criteria. The surgical options in this study are very different from the ideological point of view and participants might have a strong preference for one of the treatment modalities, causing participation bias. Therefore, we decided to have a secondary cohort for the declined patients.
Expectations
We expect that KOOS scores improve significantly after operative treatment during the follow-up. We expect that there is no clinically relevant difference between HTO and UKA treatment in late-stage medial knee OA. Our results will provide high-quality evidence on the surgical treatment options for patients suffering from late-stage medial knee OA.
Trial status
The present protocol is version 1.2 (2022–12-27). The trial will start in the first half of 2023. We assume to complete the recruitment by the end of 2025.
Availability of data and materials
The datasets generated during and/or analyzed during the current study are not publicly available but are available from the corresponding author on reasonable request.
References
Cross M, Smith E, Hoy D, Nolte S, Ackerman I, Fransen M, et al. The global burden of hip and knee osteoarthritis: estimates from the global burden of disease 2010 study. Ann Rheum Dis. 2014;73:1323–30.
Sharma L. Osteoarthritis of the knee. N Engl J Med. 2021;384:51–9.
Katz JN, Arant KR, Loeser RF. Diagnosis and treatment of hip and knee osteoarthritis: a review. JAMA. 2021;325:568–78.
Willis-Owen CA, Brust K, Alsop H, Miraldo M, Cobb JP. Unicondylar knee arthroplasty in the UK national health service: an analysis of candidacy, outcome and cost efficacy. Knee. 2009;16:473–8.
Skou ST, Roos EM, Laursen MB, Rathleff MS, Arendt-Nielsen L, Simonsen O, et al. A randomized, controlled trial of total knee replacement. N Engl J Med. 2015;373:1597–606.
Shannak O, Palan J, Esler C. A regional registry study of 216 patients investigating if patient satisfaction after total knee arthroplasty changes over a time period of five to 20years. Knee. 2017;24:824–8.
Baker PN, van der Meulen JH, Lewsey J, Gregg PJ, National Joint Registry for E, Wales. The role of pain and function in determining patient satisfaction after total knee replacement. Data from the National Joint Registry for England and Wales. J Bone Joint Surg Br. 2007;89:893–900.
Robertsson O, Dunbar M, Pehrsson T, Knutson K, Lidgren L. Patient satisfaction after knee arthroplasty: a report on 27,372 knees operated on between 1981 and 1995 in Sweden. Acta Orthop Scand. 2000;71:262–7.
McCormack DJ, Puttock D, Godsiff SP. Medial compartment osteoarthritis of the knee: a review of surgical options. EFORT Open Rev. 2021;6:113–7.
Beard DJ, Davies LJ, Cook JA, MacLennan G, Price A, Kent S, et al. The clinical and cost-effectiveness of total versus partial knee replacement in patients with medial compartment osteoarthritis (TOPKAT): 5-year outcomes of a randomised controlled trial. Lancet. 2019;394:746–56.
Maredupaka S, Meshram P, Chatte M, Kim WH, Kim TK. Minimal clinically important difference of commonly used patient-reported outcome measures in total knee arthroplasty: review of terminologies, methods and proposed values. Knee Surg Relat Res. 2020;32:19.
Riddle DL, Jiranek WA, McGlynn FJ. Yearly incidence of unicompartmental knee arthroplasty in the United States. J Arthroplasty. 2008;23:408–12.
Wang Z, Zeng Y, She W, Luo X, Cai L. Is opening-wedge high tibial osteotomy superior to closing-wedge high tibial osteotomy in treatment of unicompartmental osteoarthritis? A meta-analysis of randomized controlled trials. Int J Surg. 2018;60:153–63.
Nerhus TK, Ekeland A, Solberg G, Olsen BH, Madsen JE, Heir S. No difference in time-dependent improvement in functional outcome following closing wedge versus opening wedge high tibial osteotomy: a randomised controlled trial with two-year follow-up. Bone Joint J. 2017;99-B:1157–66.
Cao Z, Mai X, Wang J, Feng E, Huang Y. Unicompartmental knee arthroplasty vs high tibial osteotomy for knee osteoarthritis: a systematic review and meta-analysis. J Arthroplasty. 2018;33:952–9.
Jin QH, Lee WG, Song EK, Jin C, Seon JK. Comparison of long-term survival analysis between open-wedge high tibial osteotomy and unicompartmental knee arthroplasty. J Arthroplasty. 2021;36:1562-7 e1.
Kellgren JH, Lawrence JS. Radiological assessment of osteo-arthrosis. Ann Rheum Dis. 1957;16:494–502.
Curl WW, Krome J, Gordon ES, Rushing J, Smith BP, Poehling GG. Cartilage injuries: a review of 31,516 knee arthroscopies. Arthroscopy. 1997;13:456–60.
Jungius KP, Schmid MR, Zanetti M, Hodler J, Koch P, Pfirrmann CW. Cartilaginous defects of the femorotibial joint: accuracy of coronal short inversion time inversion-recovery MR sequence. Radiology. 2006;240:482–8.
Fujisawa Y, Masuhara K, Shiomi S. The effect of high tibial osteotomy on osteoarthritis of the knee. An arthroscopic study of 54 knee joints. Orthop Clin North Am. 1979;10:585–608.
Kerr DR, Kohan L. Local infiltration analgesia: a technique for the control of acute postoperative pain following knee and hip surgery: a case study of 325 patients. Acta Orthop. 2008;79:174–83.
Multanen J, Honkanen M, Hakkinen A, Kiviranta I. Construct validity and reliability of the Finnish version of the Knee Injury and Osteoarthritis Outcome Score. BMC Musculoskelet Disord. 2018;19:155.
Nerhus TK, Heir S, Svege I, Skramm I, Jervidalo T, Madsen JE, et al. Time-dependent improvement in functional outcome following Oxford medial unicompartmental knee arthroplasty. A prospective longitudinal multicenter study involving 96 patients. Acta Orthop. 2012;83:46–52.
Berliner JL, Brodke DJ, Chan V, SooHoo NF, Bozic KJ. Can preoperative patient-reported outcome measures be used to predict meaningful improvement in function after TKA? Clin Orthop Relat Res. 2017;475:149–57.
Ogura T, Ackermann J, Barbieri Mestriner A, Merkely G, Gomoll AH. Minimal clinically important differences and substantial clinical benefit in patient-reported outcome measures after autologous chondrocyte implantation. Cartilage. 2020;11:412–22.
Clement ND, MacDonald D, Simpson AH. The minimal clinically important difference in the Oxford knee score and Short Form 12 score after total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc. 2014;22:1933–9.
Roos EM, Lohmander LS. The Knee injury and Osteoarthritis Outcome Score (KOOS): from joint injury to osteoarthritis. Health Qual Life Outcomes. 2003;1:64.
Alghadir AH, Anwer S, Iqbal A, Iqbal ZA. Test-retest reliability, validity, and minimum detectable change of visual analog, numerical rating, and verbal rating scales for measurement of osteoarthritic knee pain. J Pain Res. 2018;11:851–6.
Olsen MF, Bjerre E, Hansen MD, Hilden J, Landler NE, Tendal B, et al. Pain relief that matters to patients: systematic review of empirical studies assessing the minimum clinically important difference in acute pain. BMC Med. 2017;15:35.
Dobson F, Hinman RS, Roos EM, Abbott JH, Stratford P, Davis AM, et al. OARSI recommended performance-based tests to assess physical function in people diagnosed with hip or knee osteoarthritis. Osteoarthritis Cartilage. 2013;21:1042–52.
Frobell RB, Roos EM, Roos HP, Ranstam J, Lohmander LS. A randomized trial of treatment for acute anterior cruciate ligament tears. N Engl J Med. 2010;363:331–42.
Schulz KF, Altman DG, Moher D, Group C. CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. BMJ. 2010;340:c332.
Jarvinen TL, Sihvonen R, Bhandari M, Sprague S, Malmivaara A, Paavola M, et al. Blinded interpretation of study results can feasibly and effectively diminish interpretation bias. J Clin Epidemiol. 2014;67:769–72.
Nha KW, Oh SM, Ha YW, Patel MK, Seo JH, Lee BH. Radiological grading of osteoarthritis on Rosenberg view has a significant correlation with clinical outcomes after medial open-wedge high-tibial osteotomy. Knee Surg Sports Traumatol Arthrosc. 2019;27:2021–9.
Shon OJ, Park SJ, Shim BJ, Lee DY. Comparative study of clinical and radiographic outcomes of high tibial osteotomy in patients with kissing lesions and non-kissing lesions. Knee Surg Relat Res. 2017;29:288–94.
Dettoni F, Bonasia DE, Castoldi F, Bruzzone M, Blonna D, Rossi R. High tibial osteotomy versus unicompartmental knee arthroplasty for medial compartment arthrosis of the knee: a review of the literature. Iowa Orthop J. 2010;30:131–40.
Au-Yeung WM, Kaye JA, Beattie Z. Step count standardization: validation of step counts from the withings activite using PiezoRxD and wGT3X-BT. Annu Int Conf IEEE Eng Med Biol Soc. 2020;2020:4608–11.
World Medical A. World medical association declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310:2191–4.
Acknowledgements
Not applicable.
Authorship agreement
The authorships for the primary results publication will follow the International Committee of Medical Journal Editors’ guidelines. Those who (1) have substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work, AND (2) participate in the drafting of the manuscript or revise it critically for important intellectual content, AND (3) approve the final version to be published, AND (4) agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved will be listed as authors. Also, those fulfilling the first criteria, will be offered an opportunity to participate in the review, drafting, and final approval of the manuscript.
In case the trial is extended to other centers, authorships will be granted to these recruiting centers after the first patient has completed the 12-month follow-up.
This is an investigator-initiated trial and we do not plan to use external professional medical writers.
Funding
Open Access funding provided by University of Helsinki including Helsinki University Central Hospital. This work is supported by the University of Helsinki and the Academy of Finland funds. The sponsors do not participate in study design, writing of the report, or decision to submit the report for publication. No direct or indirect funding will be acquired from industry related to this study setting.
Author information
Authors and Affiliations
Contributions
JS is the primary investigator in the trial. JK, LR, AR, MR, OK, NS, and JL participated in the conception, design, and drafting of the primary trial protocol. JS, JK, LR, and AR discuss the design and description of the statistical analysis plan. All authors were involved in drafting, reading, and approving the final version.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The trial will be conducted according to the Declaration of Helsinki [38]. The institutional review board of Helsinki and Uusimaa Hospital District has approved the protocol (HUS/1259/2019). The trial is registered to ClinicalTrials.gov (NCT05442242). A written consent from each patient is mandatory for the participation of this study. The consent will be obtained by the recruiting members of the study. The consent will be obtained from the declined cohort also.
Consent for publication
A written, informed consent to participate will be requested from all participants. The findings of this study will be disseminated through peer-reviewed publications and conference presentations and sent to participants.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Siren, J., Rämö, L., Rantasalo, M. et al. Unicompartmental knee arthroplasty vs. high tibial osteotomy for medial knee osteoarthritis (UNIKORN): a study protocol of a randomized controlled trial. Trials 24, 256 (2023). https://doi.org/10.1186/s13063-023-07263-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13063-023-07263-7