
Abstract
Background
Operative repair of a rotator cuff tear requires up to 12 weeks of post-operative (post-op) home-based rehabilitation. Maintaining patients’ compliance in the post-op rehabilitation program is a pivotal component for generating successful outcomes. By developing a post-op rehabilitation-oriented digital healthcare system and applying it in patients who had undergone rotator cuff repair, we aim to increase the efficacy of the rehabilitation program and raise patients’ compliance levels. Here, we present a protocol developed for comparing the efficacy of rehabilitation using a newly developed augmented reality (AR)-based digital healthcare system with that of conventional rehabilitation for post-op rehabilitation of rotator cuff repair.
Methods
This study will recruit a total of 115 patients who had undergone rotator cuff repair within 3 days after surgery. Patients will be randomly allocated to rehabilitation using an AR-based digital healthcare system (digital group) or conventional rehabilitation (conventional group). Patients in both groups will perform brochure-based exercises from the immediate post-op period to post-op 6 weeks. From post-op 6 weeks to 12 weeks, patients in the digital group will use the AR-based system for post-op exercises, whereas patients in the conventional group will continue brochure-based rehabilitation exercises. The primary outcome will be scores on the Simple Shoulder Test at post-op 12 weeks. Secondary outcomes include numeric rating scale scores for pain, measures of range of motion and muscle strength of the affected shoulder, grip strength of the affected arm, scores on the Disabilities of the Arm, Shoulder and Hand test, the Shoulder Pain and Disability Index, and the EuroQoL-5D-5L quality-of-life measure. Analyses will be conducted using an intention-to-treat approach.
Discussion
This study will examine the effectiveness of an AR-based digital healthcare system for post-op rehabilitation in the patients after rotator cuff repair. The study will add evidence for the application of digital healthcare systems in post-op rehabilitation.
Trial registration
ClinicalTrials.gov NCT04511377. Registered on 10 August 2020.
Similar content being viewed by others


Introduction
Rotator cuff tears result in pain and dysfunction of the shoulder and are one of the most common causes of shoulder disability [1, 2]. Previous studies have estimated the prevalence of rotator cuff tears among the general population at 20% [3] to 23% [4], with a higher prevalence associated with an older age [5]. Treatment of rotator cuff tears can be divided into operative and non-operative treatments. Operative repair of the rotator cuff, which is mainly performed in patients who are unresponsive to conservative management, has demonstrated good results, with reduced pain and good functional recovery of the shoulder [6, 7].
Post-operative (post-op) rehabilitation is a pivotal component of successful rotator cuff repair. The current consensus on rehabilitation after rotator cuff repair suggests 4–6 weeks of immobilization followed by another 4–6 weeks of rehabilitation directed at recovery of range of motion (ROM) and rotator cuff muscle strengthening [8, 9]. Post-op rehabilitation thus takes up to 12 weeks after surgery and is usually performed with outpatient-based or home-based rehabilitation programs. Enhancing the efficacy of the rehabilitation program and improving patient compliance in post-op rehabilitation are important factors for achieving successful outcomes [10]. Thus, various forms of rehabilitation programs, including video instructions [11] and individualized supervision [12], have been attempted to raise patient compliance levels and increase the efficacy of rehabilitation programs.
Recent developments in information and communication technologies have led to attempts to implement virtual reality (VR)- or augmented reality (AR)-based healthcare systems in musculoskeletal post-op rehabilitation [13,14,15]. These VR- or AR-based rehabilitation programs have shown advantages in terms of increasing patients’ compliance levels and documenting their progress [16, 17], essential factors for successful post-op rehabilitation. However, most previous studies have used commercial healthcare applications or devices providing generalized fitness exercise programs rather than rehabilitation-oriented programs. Developing and applying an AR-based digital healthcare system with post-op rehabilitation-oriented programs for patients who had undergone rotator cuff repair would increase the efficacy of rehabilitation and improve patient compliance. In this report, we present a protocol for evaluating the efficacy of an AR-based digital healthcare system for post-op rehabilitation of rotator cuff repair by comparing it with that of a conventional rehabilitation program in an assessor-blinded 1:1 randomized controlled single-center trial.
Methods
Study design
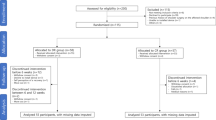
This protocol was developed for an assessor-blinded superiority randomized controlled trial. The eligible participants are recruited 1–3 days after surgery at the orthopedic ward of Seoul National University Bundang Hospital (Seongnam-si, Gyeonggi-do, Korea). The participants are then randomized based on 1:1 allocation to two groups: the digital group will undergo a rehabilitation program using a digital healthcare system, whereas the conventional group will undergo a conventional rehabilitation program. Patients will be discharged home a few days after the surgery with a shoulder brace on the affected shoulder and will immediately begin the rehabilitation program, including early mobilization of the shoulder girdle. Until post-op 6 weeks, when they will remove their braces, both groups will use brochures received at the time of discharge that provide instructions on mobilizing the affected shoulder girdle. From post-op 6 to 12 weeks, participants in the digital group will perform exercises using an AR-based digital healthcare system (UINCARE Home+; UINCARE Corp., Seoul, Korea), whereas participants in the conventional group will perform exercises using only the brochures provided by the hospital. Participants in both groups will be allowed hospital visits for exercise education by physical therapists, up to three sessions (30 min per session) over 12 weeks. The primary and secondary outcomes will be measured at baseline and at post-op 6, 12, and 24 weeks. An overview of the study design and process is given in Fig. 1.

Study flow diagram
Participants and recruitment
In the protocol, the aim is to enroll 115 adult participants over 50 years of age who had undergone rotator cuff repair surgery. Patients who had undergone biceps tenotomy, acromioplasty, or labral repair along with the rotator cuff repair can be included. Patients who had undergone reverse total shoulder arthroplasty or total shoulder arthroplasty will be excluded. Patients who are not discharged home or who cannot understand or read Korean will also be excluded. Other major inclusion and exclusion criteria are described in Table 1. Participants will be recruited from the orthopedic surgery ward at 1–3 days after surgery by research therapists from the study team. The research team will screen the medical records of the post-op patients for eligibility, and the eligible patients will receive written and verbal information about the trial from the research therapists, along with a request to participate.
Randomization and blinding
Participants will be randomized after the baseline evaluation and allocated to either the Digital or conventional group at a 1:1 ratio. Randomization sequences will be computer-generated blocks, without stratification, by the institution’s biostatistician, who is independent of the study team. The randomized allocation information was sealed in a numbered opaque envelope. The envelope seals will be checked monthly by the principle investigator to make sure the future participants’ allocation is kept blinded. Participant allocation and follow-up arrangements will be managed by the study coordinator, who will not be blinded to the participants’ group assignments. Assessments will be performed by two research therapists from the study team, who will be blinded to the participants’ intervention groups.
Intervention
Conventional group
Participants in this group will undergo a brochure-based home rehabilitation program, which is the standard protocol for patients who had undergone rotator cuff repair surgery in our hospital. The rehabilitation program can be divided into three phases: on-brace, off-brace, and active mobilization. The on-brace phase (immediate post-op period to post-op 6 weeks) mainly consists of low-intensity whole-body exercises with shoulder girdle, elbow, and hand mobilization exercises on the affected side. Participants in this phase are instructed to perform three sets of exercises with 10 repetitions of each set per day. The off-brace phase (post-op 6–9 weeks) consists of passive shoulder ROM exercises using an exercise stick and an early scapular stabilization exercise. The active mobilization phase (post-op 9–12 weeks) consists of both active and passive shoulder ROM and scapular stabilization exercises. During the off-brace and active mobilization phases, patients are instructed to perform 3–5 sets of exercises with 10 repetitions of each set per day. A detailed exercise protocol is described in Table 2.
Participants in the conventional group will be educated by a physical therapist, and a brochure with illustrations of the exercises will be provided before they are discharged home. Additional exercise education sessions will be allowed (up to three times, 30 min per session) at the participants’ request.
Digital group
The rehabilitation program for participants in this group employs a digital healthcare system. During the on-brace phase, participants in this group will use the same brochure as the conventional group participants for home-based rehabilitation. Participants in the digital group will also be educated by a physical therapist before being discharged home. During the off-brace and active mobilization phases, participants will use the digital healthcare system for home-based rehabilitation. The digital healthcare system consists of four components: software for the rehabilitation program, a three-dimensional (3D)-depth camera (Xbox One Kinect for Windows®, Microsoft, USA), a computer, and a display (TV or monitor). The software consists of an AR-based program for post-op rotator cuff tear rehabilitation, and the 3D camera tracks the participant’s motion until it reaches a pre-determined angle or position. The rehabilitation program and prescribed exercises will be matched with those for the conventional group. Participants in the digital group will use this system at home during post-op 6–12 weeks. The daily exercise amount and progression will be logged by the system, and physicians will review the data at the outpatient clinic. Up to three additional exercise education sessions (30 min each) will also be allowed in this group upon participants’ request.
Outcomes
Primary outcome measure
The primary outcome will be scores on the Simple Shoulder Test (SST), which range from 0 (worst) to 12 (best). The SST is a self-reported questionnaire consisting of 12 dichotomous (yes/no) questions that measure functional limitations [18]. It is a widely used outcome measure for assessing functional improvement in patients who had undergone rotator cuff repair [19, 20].
Secondary outcome measures
A number of secondary outcome measures will be employed (Table 3). Pain at rest and during activity will be measured using a numeric rating scale (0–10), and the ROM of the affected shoulder will be measured manually by a research therapist. The shoulder ROM will be measured in degrees in four directions: forward flexion (0–180°), abduction (0–180°), external rotation (0–90°), and internal rotation (0–70°). Muscle strength of the affected shoulder in four directions will be measured by the research therapist using a manual muscle test and rating scale (0–5). Hand grip strength on the affected side will be measured using a Takei handgrip dynamometer (Takei Scientific Instruments Co., Ltd., Tokyo, Japan). Shoulder function will be assessed using the Disabilities of Arm, Shoulder and Hand (DASH) questionnaire and the Shoulder Pain and Disability Index (SPADI). DASH is a 30-item questionnaire that measures the ability of a patient to perform certain upper extremity activities. Scores range from 0 to 100, with a score of 0 indicating no disability and 100 indicating the most severe disability. The SPADI (0–100) consists of a pain scale and a disability scale; higher scores indicate more pain and greater disability. Quality of life will be measured using the European Quality of Life Index (EQ-5D-5L).
Sample size
A minimal clinically important difference (MCID) in scores on the SST in patients with rotator cuff tear was reported to be 4.3 [21], and the average score on the SST at post-op 3 months in a previous study was 6.34 (SD = 3.7) [22]. The minimum sample size for the present study was calculated t-test based on a 2.15-point difference in SST score (50% of the MCID) and an SD of 3.7, while allowing a 5% probability of two-sided type 1 error and applying 80% statistical power. Forty-nine subjects will be required in each group to allow 15% attrition per group; thus, a total of 115 subjects will be required for the study.
Data management and sharing
All participant data will be collected by research team members and will be stored in the secured network of Seoul National University Bundang Hospital. Backup database will be updated regularly and only the research team will have access to the database. The case report forms will be stored in the locked cabinet of the research team. The coordinating investigator will have access to the final study dataset and the anonymized dataset will be available on request to the corresponding author. Final results will be published in peer-reviewed journals and presented at conferences, both nationally and internationally after completion of the study.
Primary hypothesis and data analysis
The primary hypothesis is that participants in the rehabilitation program using a digital healthcare system will demonstrate better shoulder function compared to those in the conventional rehabilitation group. Analyses will be performed using both intention-to-treat and per-protocol approach. The primary outcome measure for this study will be SST scores at post-op 12 weeks. A two-way repeated-measures ANOVA will be used to explore the effects of intervention, time, and intervention by time interaction on SST scores. The results will be presented with a mean difference with 95% confidence interval at each follow-up time point. Continuous secondary outcomes will be analyzed using repeated-measures ANOVA at each post-op 12 weeks and 24 weeks. Subgroup analysis based on the size of the tear will be performed only if there are sufficient participants in all four subgroups (small, <1 cm; medium, 1–3 cm; large, 3–5 cm; massive, ≥5 cm tear or more than two tendons involved) [23]. Statistical analysis will be performed after the 24-week follow-up measurement of the last enrolled participant is done and no inter-rim analysis will be performed during the trial. All tests will use a 5% level of significance (P < 0.05).
Participant safety and withdrawal
The potential risks for participants in this study are minimal. There is no independent oversight committee and adverse events (AEs) will be monitored by the research team at the scheduled follow-ups. Possible AEs include increased pain due to exercise and re-tear of the repaired rotator cuff tendons. Pain will be managed at the orthopedic outpatient clinic with pain medications or steroid injections, if needed. Surveillance of re-tear of repaired tendon will be routinely performed in post-op 12 weeks; however, if the re-tear is clinically suspected at any time during the follow-up periods, appropriate examinations and treatments will be provided. Participants in both groups can report AEs to the research team via direct telephone contact. Participants in the digital group will also receive a telephone number of the manufacturer for technical support.
Participants are allowed to leave the trial at any time. Participants can withdraw from the trial by informing the research team. Participants will be encouraged to visit the pre-scheduled follow-ups even if they withdraw from the study for data collection. Participants in both groups will be regularly reminded with phone calls and text messages to minimize loss of follow-ups and maximize the adherence to the trial.
Discussion
The prevalence of rotator cuff tears is increasing as the general population ages, which will eventually lead to an increased incidence of rotator cuff repair surgery. Because post-op rehabilitation is a crucial element in restoring function and reducing pain after rotator cuff repair [24], the need for an effective method of post-op rehabilitation is emerging. Post-op rehabilitation of musculoskeletal disorders using VR and AR systems is at an early stage, with only a few published studies showing its feasibility [14, 15, 25, 26].
In this trial, a digital healthcare system will be implemented only during the off-brace (post-op 6–9 weeks) and active mobilization (post-op 9–12 weeks) phases. It will not be applied during the on-brace phase (immediate post-op period to 6 weeks) because exercise programs in this phase are mainly focused on low-intensity whole-body movements under support by a post-operative brace. Also from the previous literatures, patients at this phase have good compliance with seldom having difficulty following the exercise program [27, 28]. The cost of the digital healthcare system (170 USD per week) was also considered. To maximize the cost-effectiveness of rehabilitation using the digital system, we decided that it would only be applied during the off-brace and the active mobilization phases.
This trial would have several strengths. First, to our knowledge, this would be the first randomized controlled trial to compare the effectiveness of post-op rehabilitation using a digital healthcare system with that of conventional rehabilitation in patients who had undergone rotator cuff repair. Second, this trial will implement an AR-based digital healthcare system dedicated to post-op rehabilitation. Some previous studies have used commercial fitness programs such as the Nintendo Wii FitTM [14, 15], which comprises fitness programs for the general population. However, in this trial, the digital healthcare system is tailor-made for patients who have undergone rotator cuff repair surgery and provides specific exercise programs according to the patient’s rehabilitation phase and daily progress. With this rehabilitation-oriented program, we anticipate that the effectiveness of AR-based post-op rehabilitation will be amplified.
In conclusion, this study will examine the effectiveness of an AR-based digital healthcare system for post-op rehabilitation in the patients after rotator cuff repair. The study will add evidence for the application of digital healthcare systems in post-op rehabilitation.
Trial status
Protocol ver 3.0 (approved on 2021-08-03)
The study protocol is registered in ClinicalTrials.gov (Identifier: NCT04511377).
Participant recruitment started on 2020-07-30 and is anticipated to be completed by 2022-12-31.
Availability of data and materials
All relevant data from this study will be made available upon study completion.
Abbreviations
- post-op:
-
Post-operative
- ROM:
-
Range of motion
- VR:
-
Virtual reality
- AR:
-
Augmented reality
- 3D:
-
Three-dimensional
- SST:
-
Simple Shoulder Test
- DASH:
-
Disabilities of Arm, Shoulder and Hand
- SPADI:
-
Shoulder Pain and Disability Index
- EQ-5D-5L:
-
European Quality of Life Index
- MCID:
-
Minimal clinically important difference
- AEs:
-
Adverse events
References
Tashjian RZ. Epidemiology, natural history, and indications for treatment of rotator cuff tears. Clin Sports Med. 2012;31:589–604.
Yamamoto A, Takagishi K, Osawa T, Yanagawa T, Nakajima D, Shitara H, et al. Prevalence and risk factors of a rotator cuff tear in the general population. J Shoulder Elbow Surg. 2010;19:116–20. Journal of Shoulder and Elbow Surgery Board of Trustees. https://doi.org/10.1016/j.jse.2009.04.006.
Fukuda H. Partial-thickness rotator cuff tears: a modern view on Codman’s classic. J Shoulder Elbow Surg. 2000;9:163–8.
Tempelhof S, Rupp S, Seil R. Age-related prevalence of rotator cuff tears in asymptomatic shoulders. J Shoulder Elbow Surg. 1999;8:296–9.
Boykin RE, Heuer HJD, Vaishnav S, Millett PJ. Rotator cuff disease? Basics of diagnosis and treatment. Rheumatol Rep. 2010;2:1–12.
Cofield RH, Parvizi J, Hoffmeyer PJ, Lanzer WL, Ilstrup DM, Rowland CM. Surgical repair of chronic rotator cuff tears: a prospective long-term study. J Bone Joint Surg Am. 2001;83:71–7.
Lapner PL, Sabri E, Rakhra K, McRae S, Leiter J, Bell K, et al. A Multicenter randomized controlled trial comparing single-row with double-row fixation in arthroscopic rotator cuff repair. J Bone Joint Surg Am. 2012;94:1249–57 Available from: http://journals.lww.com/00004623-201207180-00001.
van der Meijden OA, Westgard P, Chandler Z, Gaskill TR, Kokmeyer D, Millett PJ. Rehabilitation after arthroscopic rotator cuff repair: current concepts review and evidence-based guidelines. Int J Sports Phys Ther. 2012;7:197–218 Available from: http://www.ncbi.nlm.nih.gov/pubmed/3325631.
Ross D, Maerz T, Lynch J, Norris S, Baker K, Anderson K. Rehabilitation following arthroscopic rotator cuff repair: a review of current literature. J Am Acad Orthop Surg. 2014;22:1–9 Available from: http://www.ncbi.nlm.nih.gov/pubmed/24382874.
Ahmad S, Haber M, Bokor DJ. The influence of intraoperative factors and postoperative rehabilitation compliance on the integrity of the rotator cuff after arthroscopic repair. J Shoulder Elbow Surg. 2015;24:229–35. Elsevier Ltd. https://doi.org/10.1016/j.jse.2014.06.050.
Roddey T, Olson SL, Gartsman GM, Hanten WP, Cook KF. Exercise instruction following arthroscopic. J Orthop Sports Phys Ther. 2002;32:548–59.
Hayes K, Ginn KA, Walton JR, Szomor ZL, Murrell GAC. A randomised clinical trial evaluating the efficacy of physiotherapy after rotator cuff repair. Aust J Physiother. 2004;50:77–83. Australian Physiotherapy Association. https://doi.org/10.1016/S0004-9514(14)60099-4.
Gumaa M, Youssef AR. Is virtual reality effective in orthopedic rehabilitation? A systematic review and meta-analysis. Phys Ther. 2019;99:1304–25.
Fung V, Ho A, Shaffer J, Chung E, Gomez M. Use of Nintendo Wii FitTM in the rehabilitation of outpatients following total knee replacement: a preliminary randomised controlled trial. Physiotherapy (United Kingdom). 2012;98:183–8. The Chartered Society of Physiotherapy. https://doi.org/10.1016/j.physio.2012.04.001.
Baltaci G, Harput G, Haksever B, Ulusoy B, Ozer H. Comparison between Nintendo Wii Fit and conventional rehabilitation on functional performance outcomes after hamstring anterior cruciate ligament reconstruction: prospective, randomized, controlled, double-blind clinical trial. Knee Surg Sports Traumatol Arthrosc. 2013;21:880–7.
Sveistrup H. Motor rehabilitation using virtual reality. J NeuroEng Rehabil. 2004;1:1–8.
Schultheis MT, Rizzo AA. The application of virtual reality technology in rehabilitation. Rehabil Psychol. 2001;46:296–311.
Angst F, Schwyzer HK, Aeschlimann A, Simmen BR, Goldhahn J. Measures of adult shoulder function: Disabilities of the Arm, Shoulder, and Hand Questionnaire (DASH) and Its Short Version (QuickDASH), Shoulder Pain and Disability Index (SPADI), American Shoulder and Elbow Surgeons (ASES) Society Standardized Shoulder. Arthritis Care Res. 2011;63:174–88.
Cole BJ, McCarty LP, Kang RW, Alford W, Lewis PB, Hayden JK. Arthroscopic rotator cuff repair: prospective functional outcome and repair integrity at minimum 2-year follow-up. J Shoulder Elbow Surg. 2007;16:579–85.
Tashjian RZ, Deloach J, Green A, Porucznik CA, Powell AP. Minimal clinically important differences in ASES and simple shoulder test scores after nonoperative treatment of rotator cuff disease. J Bone Joint Surg Am. 2010;92:296–303.
Tashjian RZ, Shin J, Broschinsky K, Yeh CC, Martin B, Chalmers PN, et al. Minimal clinically important differences in the American Shoulder and Elbow Surgeons, Simple Shoulder Test, and visual analog scale pain scores after arthroscopic rotator cuff repair. J Shoulder Elbow Surg. 2020;29:1406–11. Elsevier Inc. https://doi.org/10.1016/j.jse.2019.11.018.
Kim YS, Chung SW, Kim JY, Ok JH, Park I, Oh JH. Is early passive motion exercise necessary after arthroscopic rotator cuff repair? Am J Sports Med. 2012;40:815–21.
DeOrio JK, Cofield RH. Results of a second attempt at surgical repair of a failed initial rotator-cuff repair. J Bone Joint Surg Am. 1984;66:563–7.
Sgroi TA, Cilenti M. ROTATOR CUFF REPAIR (M TAO AND M TEUSINK, SECTION EDITORS) Rotator cuff repair: post-operative rehabilitation concepts. Curr Rev Musculoskelet Med. 2018:86–91. https://doi.org/10.1007/s12178-018-9462-7.
Jin C, Feng Y, Ni YSZ. Virtual reality intervention in postoperative rehabilitation after total knee arthroplasty: a prospective and randomized controlled clinical trial. Int J Clin Exp Med. 2018;11:6119–24.
Koo KI, Park DK, Youm YS, do Cho S, Hwang CH. Enhanced reality showing long-lasting analgesia after total knee arthroplasty: prospective, randomized clinical trial. Sci Rep. 2018;8:1–9. Springer US. https://doi.org/10.1038/s41598-018-20260-0.
Sgroi TA, Cilenti M. Rotator cuff repair: post-operative rehabilitation concepts. Curr Rev Musculoskelet Med. 2018;11(1):86–91. https://doi.org/10.1007/s12178-018-9462-7.
Silverio LM, Cheung EV. Patient adherence with postoperative restrictions after rotator cuff repair. J Shoulder Elbow Surg. 2014;23:508–13 Mosby Inc.
Acknowledgements
The authors are grateful to the study participants, hospital staff, and study staff.
Funding
This research is supported by a grant of the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (grant number : HI19C0781). The funding source has no role in the design of this study and its execution, analyses, interpretation of the data, or decision to submit results.
Author information
Authors and Affiliations
Contributions
Conceptualization: WKC, JIL, JHH, and JYL. Design/methodology: WKC, JIL, JHH, and JYL. Investigation: WKC and JYL. Project administration: JHH and JYL. Funding acquisition: JIL, JHH, and JYL. Writing—original draft: WKC. Writing—review and editing: WKC, JIL, JHH, and JYL. Jay-Young Lim and Ji Hye Hwang will share the corresponding authorship of the publications arising from this study. The author(s) read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The study protocol was first reviewed by the institutional review board of Seoul National University Bundang Hospital in May 2020 and was approved with version 1.1 in July 2020 (reference number: B-2005/612-001). Protocol has been modified from version 1.1 to 2.0 in February 2021 for the modification of terminology in the case report form (from Visit 1/2/3/4 to visit 0/1/2/3) and to 3.0 in August 2021 for the extension of the trial period. Modification of the study protocol will be reported to the institutional review board of Seoul National University Bundang Hospital. The latest protocol version is 3.0. Participants will receive written and oral information about the study, and written consent forms will be collected by the research team members prior to baseline data collection. The trial is registered on the ClinicalTrials.gov website.
Consent for publication
Not applicable.
Competing interests
The authors have declared that no competing interests exist.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Informed Consent Form (Korean).
Additional file 2: Supplementary Table 1.
Trial registration data.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Chang, W.K., Lee, J.I., Hwang, J.H. et al. Post-operative rehabilitation using a digital healthcare system in patients who had undergone rotator cuff repair: protocol for a single-center randomized controlled trial. Trials 23, 667 (2022). https://doi.org/10.1186/s13063-022-06648-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13063-022-06648-4