
Abstract
Background
Subacute thyroiditis (SAT) is the most common cause of thyroid pain. Several clinical guidelines recommend that patients who fail to respond to full doses of non-steroidal anti-inflammatory drugs (NSAIDs) should be treated instead with oral corticosteroid therapy. However, albeit strong recommendations, the treatment protocol is based on low-quality evidence and high-quality clinical trials are lacking with respect to the optimal initiation dosage and usage of corticosteroid. We aimed to evaluate whether 15 mg/day of prednisolone (PSL) as the initial dosage could provide non-inferiority effectiveness but with lower risk and more safety compared with 30 mg/day of PSL as the initial dosage.
Methods/design
This is a multicenter, open-label, randomized, parallel trial that will be conducted at five academic hospitals in China. A total of 90 adult patients diagnosed with SAT who present moderate to severe pain or fail to respond to full doses of NSAIDs will be randomly assigned with a 1:1 ratio to the low initial PSL dosage group (15 mg daily) and standard initial PSL dosage group (30 mg daily). The primary endpoint is the time period (days) required for PSL treatment (including PSL treatment for recurrence).
Discussion
Our randomized controlled trial will try to determine the optimal protocol in the treatment of SAT by providing high-quality evidence.
Trials registration
Chinese Clinical Trial Register, ChiCTR1900023884. Registered on 15 June 2019.
Similar content being viewed by others


Background
Subacute thyroiditis (SAT), also named subacute granulomatous or subacute painful thyroiditis or de Quervain thyroiditis, is a transient inflammatory thyroid disease [1]. SAT is the most common painful thyroid disease and the prevalence of SAT is nearly 5% in the population with abnormal thyroid function [2]. According to the data from the Rochester Epidemiology Project in Olmsted County, Minnesota, the incidence of SAT was reported as 12.1 cases per 100,000/year with a higher incidence in females than in males (19.1 and 4.1 per 100,000/year, respectively) [3, 4]. Over 95% of people with SAT often present with moderate-to-severe pain [3], which may be limited to the region of thyroid or radiate to the upper neck, jaw, throat, upper chest, or ears. The pain may begin focally and spread from one side to the other of the gland over several weeks. Patients may also have fever, fatigue, malaise, anorexia, and myalgia.
SAT is a self-limiting disease and the primary treatment is to relieve thyroid pain. Several clinical guidelines, such as the American Thyroid Association (ATA) [5] and the Chinese Endocrinology Association [6], recommend anti-inflammatory agents based on the severity of symptoms. Non-steroidal anti-inflammatory drugs (NSAIDs) are initially used, particularly for mild cases. Oral glucocorticoids (prednisolone [PSL]) are suggested when patients fail to respond, or present initially with moderate to severe pain and/or thyrotoxic symptoms. ATA and UpToDate Clinical Consultants recommend that patients who fail to respond to full doses of NSAIDs over several days (2–3 days) should be treated instead with oral corticosteroid therapy. PSL of 40 mg daily for 1–2 weeks followed by a gradual taper over 2–4 weeks or longer is the most popular recommendation [5]. According to the Chinese Endocrinology Association, the initial PSL dosage of 20–40 mg daily is recommended [6].
However, albeit strong recommendations, the treatment protocol is based on low-quality evidence [3, 7,8,9,10,11] and high-quality clinical trials are lacking with respect to the optimal initiation dosage and usage of corticosteroids. Considering the short- and long-term adverse effects on many organ systems and that the risk is both dose- and duration-dependent [12,13,14,15,16], it is essential to consider the possibility of starting with a minimal dosage of corticosteroid and stop for a short duration. A recent observational study showed that the treatment protocol of PSL 15 mg daily as the initial dosage with tapering by 5 mg every 2 weeks was effective and safe for Japanese patients [17]. In addition, a retrospective study found that PSL treatment with mean dose of 15.0 mg/day (range = 14–16 mg/day) was superior to NSAIDs with regard to resolution of symptoms [18]. Based on the findings, we hypothesized that a low initial dosage of PSL seemed effective in the treatment of SAT; unfortunately there was a lack of high-quality well-designed clinical trials.
Therefore, in the present randomized controlled trial (RCT), we will use 15 mg/day of PSL as the initial dosage for treatment in patients with SAT who fail to respond to full doses of NSAIDs or present initially with moderate to severe pain, with the aim of evaluating whether 15 mg/day of PSL could provide non-inferiority effectiveness but with lower risk and more safety compared with 30 mg/day of PSL.
Methods
Study design
This is a multicenter, open-label, randomized, parallel non-inferiority trial. The study will be conducted at five academic hospitals in China: (1) Xiangyang Central Hospital, Affiliated Hospital of Hubei University of Arts and Science; (2) No. 1 Hospital of Yulin; (3) 3201 Hospital of Xi’an Jiao tong University Health Science Center; (4) Tangdu Hospital, Air Force Medical University; and (5) The Second Affiliated Hospital of Xi’an Jiaotong University.
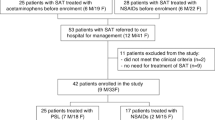
Participants who fulfill the eligibility criteria will be randomly assigned with a 1:1 ratio to any of the following two groups: group 1 = low initial PSL dosage; and group 2 = standard initial PSL dosage. In group 1, 15 mg daily of PSL as the initial dosage for 14 days will be used, followed by a gradual taper by 5 mg every 7–14 days. In group 2, 30 mg daily of PSL as the initial dosage for 5–14 days will be used, followed by a gradual taper of 5–10 mg every 5–7 days (Figure 1).

Study flow chart. SAT subacute thyroiditis, PSL prednisolone
Study population
Individuals should fulfil the following criteria:
- 1.
Age ≥ 18 years at screening;
- 2.
Diagnosis of SAT and presenting with moderate to severe pain (sore > 7/10) or failing to respond to full doses of NSAIDs;
- 3.
Provide informed consent before any study-specific procedures and not involved in another clinical study in the previous 3 months.
Exclusion criteria
Individuals should not enter the study if any of the following exclusion criteria are fulfilled:
- 1.
Women who are pregnant, intending to become pregnant during the study period, currently lactating women, or women of childbearing potential not using highly effective, medically approved methods of birth control;
- 2.
Suspicion or diagnosis of acute suppurative thyroiditis, Graves’ disease, Hashimoto thyroiditis, or thyroid carcinoma;
- 3.
Glucocorticoids allergy or intolerance (e.g. systemic allergic reaction, induced asthma, bleeding, ulcer and perforation of stomach or intestine);
- 4.
Previous treatment with PSLs in the last 6 months before screening;
- 5.
Adrenocortical hyperfunction, uncontrolled hypertension, or diabetes;
- 6.
Patients with clinically apparent liver disease characterized by any of the following:
- a.
ALT or AST > 3× upper limit of normal confirmed on two consecutive measurements (by local laboratory) within 4 weeks before the screening period;
- b.
Impaired excretory (e.g. hyperbilirubinemia) and/or synthetic function, or other conditions of decompensated liver disease such as coagulopathy, hepatic encephalopathy, hypoalbuminemia, ascites, or bleeding from esophageal varices;
- c.
Acute viral or active autoimmune, alcoholic, or other types of hepatitis.
- a.
- 7.
Patients with moderate /severe renal impairment or end-stage renal disease (estimated glomerular filtration rate ≤ 60 mL/min calculated by using the abbreviated equation developed by the Modification of Diet in Renal Disease study with modification for the Chinese population) at screening or within 4 weeks before screening (by local laboratory);
- 8.
Congestive heart failure defined as New York Heart Association class III or IV;
- 9.
Significant cardiovascular history within the past 3 months before screening defined as myocardial infarction, coronary angioplasty or bypass graft(s), valvular disease or repair, unstable angina pectoris, transient ischemic attack, or cerebrovascular accident;
- 10.
History of mental illness;
- 11.
History of corneal ulcer;
- 12.
History of gastrointestinal disease including gastroenterostomy, enterectomy, Roemheld syndrome, severe hernia, and intestinal obstruction;
- 13.
Postoperative patients with unhealing wound;
- 14.
Diagnosed and/or treated malignancy (except for basal cell skin cancer, in situ carcinoma of the cervix, or in situ prostate cancer) within the past 5 years;
- 15.
History of organ transplant or acquired immunodeficiency syndrome;
- 16.
History of alcohol abuse or illegal drug abuse within the past 12 months;
- 17.
Potentially unreliable patients and those judged by the investigator to be unsuitable for the study.
Randomization methods and concealment mechanism
The stratified block randomization method will be used. Participants will be stratified by research center and the appropriate segment lengths will be selected. Based on the number of seeds, a random coding table of 92 participants will be generated using the statistical software SAS8.2 PROC PLAN. The randomized numbers will be segmented, retained, and managed by the third party who will not be involved in the data collection (Lei Shang). The investigators in research centers will enroll the participants. When needed, the investigators will ask for numbers from the third party by telephone, using the order in which the participants will be treated, and the intervention scheme with that serial number will be provided.
Methods for ensuring blinding
The aim of the present study is to explore the effects of different dosages of PSL and a definite blindness is deemed worthless for investigators or for the patients. Therefore, an open-label study is conducted in which only laboratory personnel and data analysts (the third party) will be blinded; unblinding will not occur.
Screening period
In the screening period, patients’ data on demographical information, physical examination, current medical conditions, and history of concomitant diseases will be collected. Laboratory examination including hematology panel, urinalysis, liver function, kidney function, thyroid function, erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) will be conducted. Thyroid ultrasound and radioactive iodine uptake rate of thyroid (thyroid scintigraphy or fine-needle aspiration cytology as alternatives) will be performed. The thyroid pain will be evaluated based on visual analog scales (VAS) and thyroid tenderness will be categorized by no (–), mild (+), moderate (++), and severe (+++) degrees. Heart rates and temperatures will be monitored. Since eligible patients will be randomized within 1–2 days after screening, laboratory results from the screening period will be considered as baseline data and there will be no need to repeat. However, other data such as thyroid pain, heart rate, and blood pressure should be assessed after randomization and considered as baseline data.
Treatment period
Patients who fulfill the eligible criteria will be randomly assigned with a 1:1 ratio to treatment groups and drugs will be dispensed accordingly.
Group 1 is the low initial PSL dosage, in which 15 mg daily of PSL will be provided as the initial dosage for 2 weeks; the dosage will then taper by 5 mg every 7–14 days over 2–4 weeks or longer. Group 2 is the standard initial PSL dosage group, in which 30 mg daily of PSL will be provided as the initial dosage. The dosage will begin to taper 3–7 days after the complete resolve of thyroid pain and then taper by 5–10 mg every 5–7 days over 2–4 weeks or longer. Because most patients will receive complete resolve of thyroid pain within 5–10 days, 30 mg daily of PSL will be provided for around 5–14 days in the standard initial PSL dosage group. However, in the low initial PSL dosage group, 15 mg daily of PSL will be provided for 14 days regardless of the time period of complete pain resolve.
According to the clinical experience and the results of the pre-experiment, the pain of most patients will disappear completely within 5–10 days after receiving PSL treatment, no matter the low initial dose or the standard initial dose. Therefore, if the test group still has pain at 2 weeks, consider termination, adjust to the standard initial dose for treatment and specify the reason (with the exception of the situation that the pain completely disappears but the symptoms recur subsequently). In addition, whether in the low initial dose or in the standard initial dose group, if the pain does not relieve significantly 3 days after PSL is given, it is necessary to re-evaluate the diagnosis of SAT, eliminate other causes (such as acute thyroiditis), and give corresponding treatment if confirmed; if other causes are excluded, the study can be considered to be terminated, and the low initial dose can be adjusted to the standard initial dose for treatment and the reasons recorded in detail; the standard initial dose can be increased to a higher dose (such as 40 mg/day) and the reason specified.
The laboratory parameters that will be measured to assess efficacy and safety at each visit are shown in Table 1. The patients will receive face-to-face daily visit within the first week in research centers; thyroid pain, temperature, and adverse events (AE) will be assessed at each visit. Time periods required for the relief and complete resolution of thyroid pain will be recorded. Blood samples will be taken for the measurement of CRP and ESR in the first week. The patients will then receive telephone visits every 7–10 days. During each telephone visit, thyroid pain, temperature, and AEs will be investigated, medicine usage will be directed and recorded. If patients complain of pain in the tapering period, the tapering of the dosage will be delayed. In some cases with severe pain, the dosage will even increased; the dosage will then be tapered until the thyroid pain disappears. If PSL is tapered to a minimum dosage (i.e. 5 mg) for several days (3–7 days) with no thyroid pain, discontinuation of PSL will be considered and patients will receive a face-to-face visit. During the visit, physical examination (e.g. blood pressure and body weight) will be conducted and a blood sample will be taken for the measurement of thyroid function, liver function, kidney function, glucose level, CRP, and ESR. In addition, AEs will be collected. If SAT recurs after discontinuation of PSL, PSL will be administered again. During the treatment period, anti-ulcer drugs will be administered to some patients with a history of intestinal ulcer or who feel abdominal discomfort during treatment. A hepatologist will be consulted for possible antiviral therapy in patients with inactive hepatitis.
About 50% of patients have an initial thyrotoxic phase due to unregulated release of performed thyroid hormones from damaged thyroid follicular cells [3]. The thyrotoxic phase usually lasts 3–6 weeks, ending when the thyroid stores of preformed hormones are depleted. About 30% of patients subsequently enter a hypothyroid phase that can last up to 6 months. In the present study, anti-thyroid drugs will have no role and beta-blockers will be used as needed to control thyrotoxic symptoms. Levothyroxine will be employed when patients have a TSH level above 10 mIU/L or symptoms during the hypothyroid stage. In addition, although viral infection is regarded as the possible cause of SAT, antiviral medications will not be suggested in the study.
After the discontinuation of PSL, patients will be invited to participate in the following observational study in which a 3-month face-to-face visit will be planed. The details of the follow-up study will be described elsewhere.
Outcomes
The primary endpoint is the time period (days) required for PSL treatment (including PSL treatment for recurrence).
Secondary outcomes include time periods (days) required for complete resolution of thyroid pain (defined as no thyroid pain and no tenderness), time periods required for the relief of thyroid pain (defined as at least 50% decline of VAS scores), percentage of relapse during treatment, and the total dosage of PSL. Safety outcomes include all the AEs, vital signs, and collection of clinical chemistry parameters.
Statistical methods
The primary and secondary outcomes will be analyzed based on the full analysis set. All outcomes will also be analyzed based on the per-protocol set. The security endpoint will be analyzed based on the safety analysis set. Supportive sensitivity analysis will be carried out based on the per-protocol set and safety analysis set, using the method of last observation carried forward. Descriptive analysis will be conducted for continuous variables such as time period required for PSL treatment, total dosage of PSL, body weight, blood glucose, blood lipids, and blood pressure. Indexes such as the percentage of relapse will be summarized using frequencies and percentages. The AEs and their incidence will be summarized. The mid-term analysis will be carried out at the end of the PSL treatment, before the follow-up study.
Sample size estimate
The present study is a non-inferiority trial. The primary endpoint is the time period (days) required for PSL treatment (including PSL treatment for recurrence). PASS 11.0 software (NCSS, LLC, Kaysville, UT, USA.) was used to estimate sample size.
According to the previous literature [17, 18], the mean time was around 36 days with a standard deviation of 12 days. With a one-sided alpha level of 0.05, group sample sizes of 38 and 38 will achieve the power of 81% to detect non-inferiority with the margin of 7 days and the standard deviation of 12 days. Considering a drop-out rate of 20%, a sample size of 90 patients with a 1:1 allocation rate (45 patients per group) was finally determined.
Data management
Investigators will collect and record data on the case report form and input the data to the electric database. All data will be stored in the database and inspected by a third party who is not involved in this study. The doctors and statisticians will not have access to these data until patient evaluations are completed.
The steering committee consists of the principal investigators, the local investigators at participating study sites, the statisticians, and the trial coordinators. The steering committee remains responsible for the interpretation of the data and drafts the final report that will be approved by all investigators.
The Data Monitoring Committee (DMC) will comprise representatives from the School of Public Health, Air Force Medical University of PLA. The DMC will be formed independently from the funders. The DMC will be responsible for the independent assessment of the validity and integrity of the randomized parallel control study. The DMC will meet twice a year or more if needed. A monitor will conduct monitoring visits once every 3 months and the auditing trial conduct will be independent from investigators and the sponsor.
Discussion
Corticosteroids are important in the treatment of subacute thyroiditis; however, numerous adverse effects have been attributed to corticosteroids. Several retrospective reports have shown that long-term use of corticosteroids, even in low doses, is a significant independent predictor of adverse effects [12,13,14,15,16]. For example, a study found that the average daily prednisone dose was the strongest predictor of an adverse effect potentially attributable to glucocorticoid therapy (odds ratio = 4.5 for 5–10 mg and 32.3 for 10–15 mg) [12]. Studies also suggest that even short-term use of glucocorticoids may be associated with serious adverse effects. For example, a retrospective cohort study included 327,452 adults aged < 65 who received at least one short-term prescription over a 3-year period; results showed that there was an increase in the rates of sepsis, venous thromboembolism, and fracture [16]. Adverse effects may be not necessarily serious but displeasing to patients (e.g. Cushingoid appearance), life-threatening (e.g. serious infections), symptomatic (e.g. gastrointestinal ulcer), or largely asymptomatic until a later manifestation develops that requires medical attention (e.g. acute vertebral collapse). However, due to the relative short-term study period in the present trial, some long-term AEs cannot be collected and we may have difficulty in comparing adverse effects between groups, which is the limitation of the study. Meanwhile, because the risk is both dose- and duration-dependent, the time period of PSL usage was chosen as the primary endpoint; if non-inferior results are obtained, a lower initial dosage of PSL with a non-inferior time period will theoretically indicate reduced adverse effects.
This article presents the rationale and design of a RCT to test the effectiveness and safety of 15 mg daily of PSL versus 30 mg daily of PSL as the initial dosage in patients with SAT. This is the first RCT on this topic in Chinese people; by providing high-quality evidence, the present study will try to address the question of whether a lower initial dosage of PSL could provide non-inferiority effectiveness but with lower risk and more safety. If confirmed, our clinical practice may be modified to some extent, and patients may ultimately benefit.
Trial status
The trial is currently recruiting participants. The recruitment began in June 2019 and is anticipated to end in March 2021. Trial registration number: ChiCTR1900023884. Registration date: 15 June 2019. The name of the registry is Chinese Clinical Trial Registry and the URL of the trial registry record is https://www.chictr.org.cn/.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- SAT:
-
Subacute thyroiditis
- NSAIDs:
-
Non-steroidal anti-inflammatory drugs
- PSL:
-
Prednisolone
- ATA:
-
American Thyroid Association
- ESR:
-
Erythrocyte sedimentation rate
- CRP:
-
C-reactive protein
- VAS:
-
Visual analog scales
References
Farwell AP. Subacute thyroiditis and acute infectious thyroiditis. In: Braverman LE, Utiger RD, editors. The Thyroid. A Fundamental and Clinical Text. 9th ed. Philadelphia: Lippincott Williams & Wilkins; 2005. p. 536–47.
Bahn Chair RS, Burch HB, Cooper DS, Garber JR, Greenlee MC, Klein I, et al. Hyperthyroidism and other causes of thyrotoxicosis: management guidelines of the American Thyroid Association and American Association of Clinical Endocrinologists. Thyroid. 2011;21:593–646.
Fatourechi V, Aniszewski JP, Fatourechi GZ, Atkinson EJ, Jacobsen SJ. Clinical features and outcome of subacute thyroiditis in an incidence cohort: Olmsted County, Minnesota, study. J Clin Endocrinol Metab. 2003;88:2100–5.
Golden SH, Robinson KA, Saldanha I, Anton B, Ladenson PW. Clinical review: Prevalence and incidence of endocrine and metabolic disorders in the United States: a comprehensive review. J Clin Endocrinol Metab. 2009;94:1853–78.
Ross DS, Burch HB, Cooper DS, Greenlee MC, Laurberg P, Maia AL, et al. 2016 American Thyroid Association Guidelines for Diagnosis and Management of Hyperthyroidism and Other Causes of Thyrotoxicosis. Thyroid. 2016;26:1343–421.
Chinese Society of Endocrinology. Thyroiditis: a guide to diagnosis and treatment of thyroid diseases in China. Chin J Intern Med. 2008;47:784–8 (in Chinese).
Vagenakis AG, Abreau CM, Braverman LE. Prevention of recurrence in acute thyoiditis following corticosteroid withdrawal. J Clin Endocrinol Metab. 1970;31:705–8.
Yamada T, Sato A, Aizawa T. Dissociation between serum interleukin-6 rise and other parameters of disease activity in subacute thyroiditis during treatment with corticosteroid. J Clin Endocrinol Metab. 1996;81:577–9.
Bennedbaek FN, Hegedus L. The value of ultrasonography in the diagnosis and follow-up of subacute thyroiditis. Thyroid. 1997;7:45–50.
Topuzovic N, Smoje J, Karner I. The therapeutic approach in subacute (de Quervain's) thyroiditis. J Nucl Med. 1997;38:1665.
Mizukoshi T, Noguchi S, Murakami T, Futata T, Yamashita H. Evaluation of recurrence in 36 subacute thyroiditis patients managed with prednisolone. Intern Med. 2001;40:292–5.
Huscher D, Thiele K, Gromnica-Ihle E, Hein G, Demary W, Dreher R, et al. Dose-related patterns of glucocorticoid-induced side effects. Ann Rheum Dis. 2009;68:1119–24.
Saag KG, Koehnke R, Caldwell JR, Brasington R, Burmeister LF, Zimmerman B, et al. Low dose long-term corticosteroid therapy in rheumatoid arthritis: an analysis of serious adverse events. Am J Med. 1994;96:115–23.
McDougall R, Sibley J, Haga M, Russell A. Outcome in patients with rheumatoid arthritis receiving prednisone compared to matched controls. J Rheumatol. 1994;21:1207–13.
Curtis JR, Westfall AO, Allison J, Bijlsma JW, Freeman A, George V, et al. Population-based assessment of adverse events associated with long-term glucocorticoid use. Arthritis Rheum. 2006;55:420–6.
Waljee AK, Rogers MA, Lin P, Singal AG, Stein JD, Marks RM, et al. Short term use of oral corticosteroids and related harms among adults in the United States: population based cohort study. BMJ. 2017;357:j1415.
Kubota S, Nishihara E, Kudo T, Ito M, Amino N, Miyauchi A. Initial treatment with 15 mg of prednisolone daily is sufficient for most patients with subacute thyroiditis in Japan. Thyroid. 2013;23:269–72.
Sato J, Uchida T, Komiya K, Goto H, Takeno K, Suzuki R, et al. Comparison of the therapeutic effects of prednisolone and nonsteroidal anti-inflammatory drugs in patients with subacute thyroiditis. Endocrine. 2017;55:209–14.
Acknowledgments
None.
Funding
This study is an investigator-initiated trial and is sponsored by SX. The sponsor has the role in the design of the study and interpretation of the data and in writing the manuscript. The study is funded by Research Foundation for 2019 Talented Scholars of Xiangyang Central Hospital (No. 2019YC04). SX is also supported by the China Postdoctoral Science Foundation (No. 2018 M643837) and partly supported by special grade of the financial support from the China Postdoctoral Science Foundation (No. 2019 T120986). The funding bodies have no role in the design of the study and collection, analysis and interpretation of data, and in writing the manuscript.
Author information
Authors and Affiliations
Contributions
SX and YJ contributed equally to this work. SX, LS, and LG were involved in study concept and design. SX and YJ wrote the first draft; AJ, JZ, BG, JX, XJ, JY, WX, and RC contributed to the revision of the final report. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This protocol (version: 2.0, date: 30 September, 2019) was approved by the independent Ethics Committee of Xiangyang Central Hospital, the Affiliated Hospital of Hubei University of Art and Science (ID: XYSZXYY-LLDD-PJ-2019 − 032) and registered (registration date: 15 June 2019) at Chinese Clinical Trial Registry (www.chictr.org.cn, identifier: ChiCTR1900023884). Research staff will get informed consent from the participants before the study. On the consent form, participants will be asked if they agree to the use of their data should they choose to withdraw from the trial. Participants will also be asked for permission for the research team to share relevant data with people from the Universities taking part in the research or from regulatory authorities, where relevant. This trial does not involve collecting biological specimens for storage. The informed consent form is available from the corresponding author on request. There is no anticipated harm and compensation for trial participation. Post-trial care will be provided and participants will be followed up for at least 6 months.
Consent for publication
Written informed consent for publication of their clinical details and/or clinical images will be obtained from the participants. A copy of the consent form is available for review at any stage if required. Participation in this study is strictly confidential. Any information that is published will not reveal the identity of the participants. The findings of this trial will be submitted to a peer-reviewed journal. Abstracts will be submitted to relevant national and international conferences.
Competing interests
The authors declare that they have no conflict of interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Xu, S., Jiang, Y., Jia, A. et al. Comparison of the therapeutic effects of 15 mg and 30 mg initial dosage of prednisolone daily in patients with subacute thyroiditis: protocol for a multicenter, randomized, open, parallel control study. Trials 21, 418 (2020). https://doi.org/10.1186/s13063-020-04337-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13063-020-04337-8