
Abstract
Background
Allergic rhinitis (AR) is one of the most common allergic diseases. The conventional treatments of allergic rhinitis are oral anti-histamines, the use of intranasal corticosteroids, and immunotherapy. Dissatisfied with the ineffectiveness and side effects of these treatments, substantial numbers of patients are turning to alternative treatments like Chinese herbal medicine, particularly Tian Jiu (TJ). TJ is a form of moxibustion in which herbal patches are applied to specific acupoints on the skin. This study aims to investigate the efficacy and safety of TJ in the treatment of allergic rhinitis.
Methods/design
This will be a prospective, randomized, single-blinded, controlled trial in patients with AR. After a 1-week run-in period, eligible subjects will be randomly assigned to the TJ group, placebo-control group or waitlist-control group. The TJ and placebo-control groups will undergo a 4-week treatment with one session per week and one 4-week post-treatment follow-up. Participants in the waitlist-control group will not receive any treatment during the first 4 weeks but will be required to be assessed. The primary outcome will be the change in the weekly average of the Total Nasal Symptom Score recorded from baseline to the end of treatment. The secondary outcomes will be change in symptoms and change in need for medication between baseline and the end of treatment by using the Rhinitis Quality of Life Questionnaire. Rescue medication (RM) needs will be measured using an RM score, comprising the weekly sum of daily assessments and any form of systemic steroids for allergic rhinitis.
Discussion
This study will be the first study to compare TJ treatment for allergic rhinitis with a placebo-control group, and a waitlist-control group. The investigation of TJ for allergic rhinitis will also suggest recommendations for clinical practice. The results of this study are expected to provide consolidated evidence for the effectiveness and safety of TJ for the treatment of patients with allergic rhinitis.
Trial registration
NCT02470845 (17 May 2015).
Similar content being viewed by others


Background
Allergic rhinitis (AR), which can be acute or chronic, is one of the most common allergic diseases. A number of surveys have documented the high prevalence of AR and the substantial burden to patients and the health care system [1–3]. In the United States, the prevalence of AR was shown to vary from 10 to 30 % [4]. In Europe, the prevalence was around 23 % [5]. In 11 cities in China, the prevalence of AR was shown to vary from 8 to 24.1 % [6]. The conventional treatment of AR symptoms, such as nasal obstruction, rhinorrhea, sneezing, and itching, includes the use of intranasal corticosteroids, oral anti-histamines with or without decongestants, immunotherapy, and education [7]. Substantial numbers of patients with AR are dissatisfied with conventional medical treatment and repeatedly experience side effects. As a result, many AR sufferers are turning to complementary and alternative treatments [8, 9]. Among them, Chinese medicine, including herbal medicine, acupuncture and Tian Jiu (TJ), are frequently used to manage AR in East Asia [10].
In China, traditional Chinese medicine (TCM) has a long history of using TJ as a measure to prevent asthmatic attacks [11]. TJ as an external application is also known as “drug moxibustion” or “vesiculating moxibustion.” Herbal patches are applied on the selected acupoints or the diseased part. In TCM, this treatment regulates the functions of channels and zang-fu organs. It can warm the channels and disperse coldness. It is also able to invigorate qi movement, harmonize nutrient absorption and defense mechanisms, and resolve stagnation in the body and stasis of the blood. The mechanisms of TJ, which have been studied in recent years, show that it can inhibit the release of mast cell mediators and modulate serum IgE levels, lymphocyte and/or macrophage activity [12].
Currently, some clinical studies have showed that TJ therapy is effective in treating AR. They have found that TJ therapy is better than placebo for treating clinical symptoms and signs as well as improving quality of life [13, 14]. One previous study has also shown that the TJ group had lower scores for sneezing, rhinorrhea and nasal stuffiness after finishing therapy when compared with the control group and also showed significant improvement in the scores for the 36-item Short Form Health Survey (SF-36), which measures patients’ quality of life [15]. A study using the Rhinitis Quality of Life Questionnaire (RQLQ) to assess quality of life also demonstrated that TJ therapy can improve quality of life when compared with a placebo group [16].
In recent years, clinical and basic researchers have found that TJ acts as a modulator of anti-inflammatory cytokines [17] and affects neuro-immunological mechanisms, e.g., lowering plasma levels of vasoactive intestinal peptides and substance P [18]. However, these studies were done on a relatively small scale and did not use a randomized control design.
In order to further investigate the efficacy of TJ in the treatment of AR, a rigorous randomized controlled trial will be conducted in our clinical centers. The evidence from this rigorous clinical research, if successful, will become the basis for a large multi-center study. The overall goal is to develop evidence-based clinical guidelines for the use of TJ therapy in treating AR.
The research was supported by the Marcoda Co. Ltd. Research Fund and was registered with the identifier NCT02470845 (17 May 2015) at ClinicalTrials.gov. The funding agency had no role in the development of the study design, data collection, or manuscript preparation for publication.
Objective
The aim of this study is to investigate the efficacy of TJ in the treatment of AR, by comparing it with a placebo-control group and a waitlist-control group, in Hong Kong.
Methods/design
Study design
This will be a prospective, randomized, single-blinded, controlled trial in patients with AR. After a 1-week run-in period, eligible subjects will be randomly assigned to the TJ group, placebo-control group or waitlist-control group. Except for rescue medication (RM) drugs, no other routine medication use for AR symptom control will be permitted in the entire study.
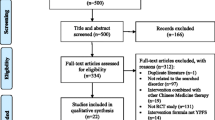
The TJ group will undergo a 4-week treatment with herbal patches for one session per week, and a 4-week post-treatment follow-up of one assessment session per week. The placebo-control group will undergo a 4-week treatment with placebo patches for one session per week, and a 4-week post-treatment follow-up of one assessment session per week. The waitlist-control group will receive no treatment during the first 4 weeks but, beginning at the fifth week, this group will receive TJ treatment for 4 weeks as compensatory. All groups will be assessed in the same way throughout the study period. The total study period will be 9 weeks. The participant flowchart is listed in Fig. 1 and participant timeline is listed in Fig. 2.

Participant flowchart

Schedule of enrollment, intervention and assessment
The study protocol has been approved by the Hong Kong Baptist University Ethics Committee on the Use of Human Subjects for Teaching and Research (Approval number HASC/13-14/0241), and informed consent was obtained from each participant.
Participants
Setting
The study will be conducted in the research and clinical centers, School of Chinese Medicine, Hong Kong Baptist University (HKBU). All participants will be recruited from the general public via daily outpatient services and advertisements in newspapers and on a website.
Inclusion criteria
Patients who have intermittent or persistent AR, who are 18 years of age or older, regardless of gender, race or educational and economic status will be included. The diagnostic criteria for AR for inclusion will be as follows according to the ARIA criteria [19]: (1) positive skin prick tests, (2) high circulating levels of allergen-specific IgE antibody detected by a specific blood test for allergy called a radioallergosorbent (RAST) test, (3) clinical history or identified allergen, (4) nasal provocation (test). The lowest score of the Total Nasal Symptom Score (TNSS) should be 8 or above.
Exclusion criteria
Exclusion criteria will be allergic asthma, moderate to severe atopic dermatitis, any autoimmune disorder, any severe chronic inflammatory disease, history of anaphylactic reactions and hypersensitivity to cetirizine or related drugs, specific immunotherapy during the past 3 years or planned in the next 2 years, and pregnancy or breastfeeding.
Interventions
Medications
Participants in the TJ group will be treated with herbal patches on five acupoints on the back. The formula of the herbal patch consists of Bai Jie Zi (Sinapis semen), Yan Hu Suo (Corydulis rhizoma), Zhi Gan Sui (Kansui radix), Xi Xin (Asari radix et rhizama) and Rengong She Xiang (Moschus artifactus). The first four of these herbs will be ground into a powder, mixed thoroughly with 20 % Bai Jie Zi (Sinapis semen), 25 % Yan Hu Suo (Corydulis rhizoma), 15 % Zhi Gan Sui (Kansui radix), and 40 % Xi Xin (Asari radix et rhizama), and the resulting powder will then be mixed with fresh ginger juice in a ratio of 20 g to 25 ml. The mixture will be made in to a 1 cm2 round patch weighing 2 g. Artificial Rengong She Xiang (Moschus artifactus), 0.02 g, will then be placed on top of each patch. Participants in the placebo-control group will be treated with placebo patches on the same acupoints as the TJ group. The placebo patch consists of flour and edible pigments. These two ingredients will be mixed with water and made in to 1 cm2 round patches weighing 2 g. Participants in the waitlist-control group will wait for 4 weeks and will not receive any treatment material. The composition and the action of each herb in the TJ herbal patches are listed in Table 1.
Acupoints
The choice of acupoints was based on a literature review and clinical practice. A survey conducted in 2010 by the School of Chinese Medicine at HKBU revealed that 60 % of patients who were suffering from AR or asthma found their symptoms were alleviated after receiving TJ therapy. Amongst the 812 people receiving TJ therapy, 558 (approximately 70 %) were suffering from AR or asthma. The survey covered 224 AR patients and 57 asthma patients, and found that 60 % of each group reported that their symptoms were relieved [20]. The latest clinical study conducted in 2014 revealed that more than 50 % of patients suffering from AR obtained benefit after receiving TJ therapy. The study found that, among the 3438 patients included in the survey, 52–67 % of the patients with AR found that their symptoms were alleviated and 32–50 % of those surveyed reported that their body constitution had been improved [21].
Five acupoints will be used: Dazhui (GV 14), Feishu (UB 13) and Shenshu (UB 23), on both sides of the body. A TJ patch will be applied to each acupoint, and left on for 2 hours. A 4 cm2 piece of hypoallergenic tape will be used to stick one patch on one acupoint. After 2 hours the patches will be removed by our Chinese medicine practitioner (CMP). If a participant cannot tolerate the stimulation or suffers a allergic reaction, the patching time can be appropriately shortened. Names and details of acupoints are listed in Table 2.
Outcomes
The primary outcome will be the change in the weekly average of the Total Nasal Symptom Score (TNSS) recorded in participants’ diaries from baseline to the end of treatment [22]. The TNSS consists of four nasal symptoms (rhinorrhea, nasal itching, nasal obstruction, and sneezing) using a five-point scale from 0 to 4 (0 = no symptom, 1 = mild, 2 = moderate, 3 = severe, 4 = very severe). The TNSS will be obtained from the sum of all four individual symptom scores, with a total possible score ranging from 0 (no symptoms) to 16 (maximum symptom intensity). This scoring system has been validated [23, 24].
The secondary outcomes will be changes in symptoms and changes in need for medication between baseline and the end of treatment. Symptoms will be assessed by using the RQLQ, which has 28 questions in seven domains (activity limitation, sleep problems, nasal symptoms, ocular symptoms, other symptoms, practical problems, and emotional function) ranked from 0 (no impairment) to 6 (severe impairment) [25]. Rescue medication need will be measured using an RM score (RMS), comprising the weekly sum of daily assessments. Rescue medicine usage will be scored daily on a four-point scale (0 = no rhinitis medicine; 1 = cetirizine, 10 mg/d, or equivalent; 2 = cetirizine, 20 mg/d, or equivalent; 3 = systemic or topical corticosteroids for AR) (daily range; 0 to 3; weekly range: 0 to 21). If more than one RM is used on the same day, only the maximal score medication will be recorded [26].
For safety concern, we will record every adverse event during the treatment and follow-up, and make statistical comparisons. Treatment will be suspended immediately should serious adverse events occur. Further assessment will be needed to decide whether the trial should be suspended.
Randomization assignment
This study is designed as a randomized, waitlist-control trial. Eligible participants will be randomly and equally allocated to one of the three groups: T (TJ) group, P (placebo) group, and W (waitlist-control) group. Random Allocation Software (version 1.0.0, Isfahan, Iran) will be used to generate a randomization scheme. The principal investigator (PI) will generate the random allocation sequence, and will not share it with other investigators. After the run-in stage, a research assistant (RA) will assign treatments according to the codes which are kept in opaque sealed envelopes with consecutive randomization numbers. Emergency unblinding can only happen when the intervention information is compulsory for the participant’s future management.
Sample size
Sample size calculations are based on the primary outcome measurement. Since this is a pilot clinical study, the improvement rate of group W would obviously be 0. Subsequently, we assume that there will be 30 % improvement of TNSS symptoms in group T and 15 % in group P. Considering a power of 80 %, and a alpha value of 2.5 % (two-tailed), the sample size will be calculated using the following formula:
The λ is the cut-off value. Pt is 30 % and Pw is 0. Then each group will need at least 38 subjects for significance to be detected [27]. Allowing for a 20 % dropout, we plan to recruit 46 subjects in each group, making a total of 138.
Data processing and analysis
All efficacy and safety analyses will be conducted according to the intention-to-treat (ITT) principle. Missing values will be imputed by the last-observation-carried-forward method. The statistical analysis will be performed using the Statistical Packages for the Social Sciences (SPSS) for Windows, version 21.0. Statistical significance is defined as a two-sided P value of <0.05. Baseline characteristics will be reported as mean (SD). Comparisons between groups will be conducted by using an analysis of covariance (ANCOVA) with baseline as covariate. All items and subscales will be compared between groups for each 4-week period using ANCOVA, with treatment group as a factor in the model and baseline as the covariate. The changes in scores from baseline to the end-point of treatment will be tested using repeated measure analysis of variance (ANOVA). Within-group differences will be assessed using a paired t test for normally distributed data and a Wilcoxon signed-rank test for non-normally distributed data.
Data collection and handling of withdrawal and dropout
This is a 9-week clinical trial, in which subjects must take TJ for 8 weeks, attend five assessment visits, complete a set of questionnaires, and stop taking other medications for symptom control. All collected information will be input into a computer by a RA. In the meantime, all the files will be stored in numerical order. Participant files will keep in storage for 5 years.
Considering maximization of participants’ compliance, we will firstly run a thorough consent process for all subjects by interpreting the details of the trial schedule, potential adverse events, and the responsibilities of researchers and participants. In addition, before every visit, a RA will contact the subject to re-confirm the schedule. If a participant shows signs of wanting to withdraw, we would try to understand the possible reasons and aim to find the best option for encouraging the participant to remain in the study.
Discussion
TJ, also known as natural moxibustion is a conventional method of treating respiratory allergic diseases in TCM. The procedure is convenient and inexpensive. Thousands of people accept this treatment in China every year. Laboratory study has found that natural moxibustion treatment can reduce IgE and interleukin (IL)-4 levels in the plasma of asthmatic rats, as well as airway inflammation [28]. Clinical studies have found that TJ can modulate anti-inflammatory cytokines [17], and that it appears to work by neuro-immunological mechanisms. However, there have been no methodologically controlled clinical studies confirming the efficacy of TJ therapy.
Therefore, our team has designed this randomized, single-blinded, controlled trial to evaluate the effectiveness of TJ therapy for AR. To our knowledge, this will be the first study to compare TJ therapy with a placebo-control group, as well as a waitlist-control group.
We use pigmented flour mixed with water to make the sham TJ treatment. However, some articles mention that in many studies, sham acupuncture is equally effective as acupuncture [29, 30]. Although the sham TJ does not have the pharmacological effects, the operating procedures still causes a pressing sensation to the skin. Because we use the same acupoints for both groups, pressing these acupoints may create an effect like the acupressure. Therefore, we have designed the study with three groups. One group (group T) will receive traditional TJ therapy, which means the application of herbal patches to specific acupoints on the skin. A second group (group P) will receive sham TJ therapy, which means the application of patches with an inert, similar appearance to the TJ patch on the same acupoints. A third group (group W) will not receive any treatment material in order to examine the influence of sham TJ on the study results.
The trial protocol is the foundation of every clinical study. To facilitate appropriate reference standards for scientific, ethical and safety issues before the trial begins, the protocol of this study has been developed according to Consolidated Standards of Reporting Trials (CONSORT) statement [31], the Standard Protocol Items: Standards for Reporting Interventions in Controlled Trials of Acupuncture (STRICTA) statement 2010 [32], and Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) statement 2013 [33].
The results of this study are expected to provide consolidated evidence for the effectiveness and safety of TJ for the treatment of patients with AR.
Trial status
At the time of manuscript submission the study is preparing to enroll participants; no patient has yet begun treatment.
Abbreviations
- AR:
-
allergic rhinitis
- ANCOVA:
-
analysis of covariance
- CONSORT:
-
Consolidated Standards of Reporting Trials
- CMP:
-
Chinese medicine practitioner
- ITT:
-
intention-to-treat principle
- PI:
-
principal investigator
- RA:
-
research assistant
- RMS:
-
rescue medication score
- RQLQ:
-
Rhinitis Quality of Life Questionnaire
- SD:
-
standard deviation
- SPIRIT:
-
Standard Protocol Items: Recommendations for Interventional Trials
- SPSS:
-
Statistical Packages for the Social Sciences
- STRICTA:
-
STandards for Reporting Interventions in Controlled Trials of Acupuncture
- TNSS:
-
Total Nasal Symptom Score
References
Anonymous. Worldwide variation in prevalence of symptoms of asthma, allergic rhino conjunctivitis, and atopic eczema: ISAAC. The International Study of Asthma and Allergies in Childhood (ISAAC) Steering Committee. Lancet. 1998;351:1225–32.
Weiss KB, Sullivan SD. The health economics of asthma and rhinitis. I. Assessing the economic impact. J Allergy Clin Immunol. 2001;107:3–8.
Van Cauwenberge P, Bachert C, Passalacqua G, Bousquet J, Canonica GW, Durham SR, et al. Consensus statement on the treatment of allergic rhinitis. European Academy of Allergology and Clinical Immunology. Allergy. 2000;55:116–34.
Schoenwetter WF, Dupclay L, Appajosyula S, Botteman MF, Pashos CL. Economic impact and quality-of-life burden of allergic rhinitis. Curr Med Res Opin. 2004;20:305–17.
Bauchau V, Durham SR. Prevalence and rate of diagnosis of allergic rhinitis in Europe. Eur Respir J. 2004;24:758–64.
Zhang L, Han DM, Huang D, Wu YF, Dong Z, Xu G, et al. Self-reported prevalence of allergic rhinitis in eleven cities in China. Int Arch Allergy Immunol. 2009;149(1):47–57.
Dykewicz MS, Fineman S, Skoner DP, Nicklas R, Lee R, Blessing-Moore J, et al. Diagnosis and management of rhinitis: complete guidelines of the Joint Task Force on Practice Parameters in Allergy, Asthma and Immunology. American Academy of Allergy, Asthma, and Immunology. Ann Allergy Asthma Immunol. 1998;81:478–518.
Passalacqua G, Bousquet PJ, Carlsen KH, Kemp J, Lockey RF, Niggemann B, et al. ARIA update: I – Systematic review of complementary and alternative medicine for rhinitis and asthma. J Allergy Clin Immunol. 2006;117:1054–62.
Schafer T, Riehle A, Wichmann HE, Ring J. Alternative medicine in allergies – prevalence, patterns of use, and costs. Allergy. 2002;57:694–700.
Le MS, Pittler MH, Shin BC, Kim JI, Ernst E. Acupuncture for allergic rhinitis: a systematic review. Ann Allergy Asthma Immunol. 2009;102(4):269–79.
Zhu XM. Application of intensive moxibustion with ginger paste. Zhongguo Zhen Jiu. 2013;33(3):233–5. Chinese.
Xue CCL, Hugel H, Li CG, Story DF. Efficacy, chemistry and pharmacology of Chinese herbal medicine for allergic rhinitis. Curr Med Chem. 2004;11:1403–21.
Dai MY, Wang Y, Tao ZZ. Meta analysis of therapy effect of acupoint application in treatments of patients with allergic rhinitis. Xiandai Sheng Wu Yi Xue Jin Zhan. 2014;14(25):4895–8. Chinese.
Shen X, Fu LX, Zhu Y, Zuo XH, Bian XK. Meta analysis of efficacy of sanfu patching in treatments of patients with allergic rhinitis. Henan Zhong Yi. 2013;33(3):449–52. Chinese.
Hsu WH, Ho TJ, Huang CY, Ho HC, Liu YL, Liu HJ, et al. Chinese medicine acupoint herbal patching for allergic rhinitis: a randomized controlled clinical trial. Am J Chin Med. 2010;38(4):661–73.
Hu N, Deng G, Xian PF. Effect of point application therapy on the life quality of patients with perennial allergic rhinitis. Shanghai J of Acupunct and Mox. 2012;31:100–2. Chinese.
Brinkhaus B, Hummelsberger J, Kohnen R, Seufert J, Hempen CH, Leonhardy H, et al. Acupuncture and Chinese herbal medicine in the treatment of patients with seasonal allergic rhinitis: a randomized-controlled clinical trial. Allergy. 2004;59:953–60.
Li YM, Zhuang LX, Lai XS, Jiang GH. Effects of electroacupuncture on plasma vasoactive intestinal peptide and substance P in perennial allergic rhinitis patients. Zhen Ci Yan Jiu. 2007;32(2):136–8. Chinese.
Lin J, Su N, Liu G, Yin K, Zhou X, Shen H, et al. The impact of concomitant allergic rhinitis on asthma control: a cross-sectional nationwide survey in China. J Asthma. 2014;51(1):34–43.
HKBU eNews. Chinese medicine research finds “Tianjiu” helpful in alleviating asthma. http://enews.hkbu.edu.hk/view_article.php?id=11539. Accessed 21 Dec 2012.
HKBU eNews. HKBU clinical study finds Tian Jiu treatment helps relieve allergic rhinitis and bronchial asthma. http://hkbuenews.hkbu.edu.hk/?t=enews_details/689. Accessed 30 June 2014.
Park Y, Jo J, Hong K, Kang W, Choi S. Effect of acupuncture on nasal obstruction in patients with persistent allergic rhinitis: a randomized controlled trial. J Kor Acu Mox. 2005;22:229–39.
Xue CC, An X, Cheung TP, Da Costa C, Lenon GB, Thien FC, et al. Acupuncture for persistent allergic rhinitis: a randomised, sham-controlled trial. Med J Aust. 2007;187:337–41.
Ng DK, Chow PY, Ming SP, Hong SH, Lau S, Tse D, et al. A double-blind, randomized, placebo-controlled trial of acupuncture for the treatment of childhood persistent allergic rhinitis. Pediatrics. 2004;114(5):1242–7.
Juniper EF, Guyatt GH, Griffith LE, Ferrie PJ. Interpretation of rhino conjunctivitis quality of life questionnaire data. J Allergy Clin Immunol. 1996;98:843–5.
Kuehr J, Brauburger J, Zielen S, Schauer U, Kamin W, Von Berg A, et al. Efficacy of combination treatment with anti-IgE plus specific immunotherapy in polysensitized children and adolescents with seasonal allergic rhinitis. J Allergy Clin Immunol. 2002;109:274–80.
Yan H, editor. Medical statistics. 2nd ed. Beijing: People’s Medical Publishing House; 2010.
Li YM, Ling CM. Effects of natural moxibustion on cytokines and specific transcription factors in asthma rats. Zhongguo Zhen Jiu. 2014;34(4):379–83. Chinese.
Birch S, Hesselink JK, Jonkman FA, Hekker TA, Bos A. Clinical research on acupuncture. Part 1. What have reviews of the efficacy and safety of acupuncture told us so far? J Altern Complement Med. 2004;10:468–80.
Lund I, Lundeberg T. Are minimal, superficial or sham acupuncture procedures acceptable as inert placebo controls? Acupunct Med. 2006;24:13–5.
Schulz KF, Altman DG, Moher D, CONSORT Group. CONSORT 2010 statement: updated guidelines for reporting parallel group randomized trials. Ann Intern Med. 2010;152(11):726–32.
MacPherson H, Altman DG, Hammerschlag R, Youping L, Taixiang W, White A, et al. Revised STandards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA): extending the CONSORT statement. J Altern Complement Med. 2010;16(10):ST1–14.
Chan AW, Tetzlaff JM, Altman DG, Laupacis A, Gøtzsche PC, Krleža-Jerić K, et al. Statement: defining standard protocol items for clinical trials. Ann Intern Med. 2013;2013(158):200–7.
Acknowledgements
The researchers gratefully acknowledge the financial support provided by the Marcoda Co. Ltd. Research Fund. The funding agency had no role in the development of the study design, data collection, or manuscript preparation for publication.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
All authors participated in the design of the study and will perform the trial. KW and LZ drafted the manuscript. ZB will supervise and coordinate the clinical trial. KW and LZ are responsible for recruiting subjects. AL gave critical review and advice on the manuscript. LD will participate in assessing the subjects. CC will participate in randomization and statistical analysis. All authors read and approved the final manuscript.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Kun, W., Zhong, L.L.D., Dai, L. et al. Tian Jiu therapy for allergic rhinitis: study protocol for a randomized controlled trial. Trials 17, 248 (2016). https://doi.org/10.1186/s13063-016-1374-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13063-016-1374-5