
Abstract
Background
Evidence that home telemonitoring for patients with chronic heart failure (CHF) offers clinical benefit over usual care is controversial as is evidence of a health economic advantage.
Methods
Between January 2010 and June 2013, patients with a confirmed diagnosis of CHF were enrolled and randomly assigned to 2 study groups comprising usual care with and without an interactive bi-directional remote monitoring system (Motiva®). The primary endpoint in CardioBBEAT is the Incremental Cost-Effectiveness Ratio (ICER) established by the groups’ difference in total cost and in the combined clinical endpoint “days alive and not in hospital nor inpatient care per potential days in study” within the follow-up of 12 months.
Results
A total of 621 predominantly male patients were enrolled, whereof 302 patients were assigned to the intervention group and 319 to the control group. Ischemic cardiomyopathy was the leading cause of heart failure. Despite randomization, subjects of the control group were more often in NYHA functional class III–IV, and exhibited peripheral edema and renal dysfunction more often. Additionally, the control and intervention groups differed in heart rhythm disorders. No differences existed regarding risk factor profile, comorbidities, echocardiographic parameters, especially left ventricular and diastolic diameter and ejection fraction, as well as functional test results, medication and quality of life. While the observed baseline differences may well be a play of chance, they are of clinical relevance. Therefore, the statistical analysis plan was extended to include adjusted analyses with respect to the baseline imbalances.
Conclusions
CardioBBEAT provides prospective outcome data on both, clinical and health economic impact of home telemonitoring in CHF. The study differs by the use of a high evidence level randomized controlled trial (RCT) design along with actual cost data obtained from health insurance companies. Its results are conducive to informed political and economic decision-making with regard to home telemonitoring solutions as an option for health care. Overall, it contributes to developing advanced health economic evaluation instruments to be deployed within the specific context of the German Health Care System.
Trial registration
ClinicalTrials.gov NCT02293252; date of registration: 10 November 2014
Similar content being viewed by others

Background
Chronic heart failure (CHF) is one of the most frequently diagnosed diseases causing disability and death in the Western hemisphere. It is characterized by a prevalence that increases with age [1]. In Germany, heart failure is the most common reason for hospitalization with about 396,000 cases in 2013 [2]. Direct medical costs related to heart failure account for 1–2 % of total health care expenditure [3].
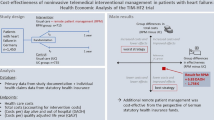
In the majority of cases, home telemonitoring solutions in health care delivery to patients with CHF show advantages over usual care in terms of clinical outcomes. Several meta-analyses reveal that total mortality and number of hospitalizations tend to decrease, while patients’ quality of life improves [4–6]. Two subsequently published trials (Telemedical Interventional Management in Heart Failure trial (TIM-HF) [7], Telemonitoring in patients with Heart Failure trial (TELE-HF) [8]) show neutral findings in general. However, the health economic impact has not been clearly demonstrated so far [9]. A meta-analysis by Klersy et al. (2011) states that the difference in costs between remote patient monitoring and usual care ranges from Euro300 to Euro1000, favoring remote patient monitoring because of a lower hospitalization rate. Thus, direct costs for hospitalization were approximated by diagnosis-related group tariffs [10]. A more detailed evaluation of efficiency and economic feasibility could help to determine cost-effectiveness and to avoid misallocation of resources [11].
The CardioBBEAT trial was designed to assess the health economic impact of a dedicated home telemonitoring system for patients with CHF based on actual costs directly obtained from patients’ health care providers. The present report provides details on the outline of the study and an analysis of the study population’s baseline data.
Methods
Study design
CardioBBEAT represents a randomized, controlled, open, multicenter trial with two prospective study arms. Patients were recruited at ten study sites from five areas of varying economic status in Germany: namely, Berlin, Brandenburg, Bavaria, Hamburg and North Rhine-Westphalia. This diversity allows for investigating the impact of regional differences in medical care, with general medical care predominating in rural districts compared to predominantly specialist care in urban areas. Each site was responsible for recruiting as well as following-up on their patients. Specified information about inclusion and exclusion criteria is displayed in Table 1.
The study has been conducted in accordance with the principles stated in the Declaration of Helsinki, the Good Clinical Practice (International Conference on Harmonization), and national as well as local regulations. The research protocol was approved by the responsible ethics committees (Table 2), and written informed consent was obtained from all patients prior to any study-related procedures. The study is monitored by an independent external institute to ensure that every participating site abides by the study protocol and to perform external quality control of the data.
Setting
During the trial, all patients receive best medical treatment according to the current guidelines of the European Society of Cardiology (ESC) [12, 13].
Patients in the control group only receive best medical treatment as stated above, whereas patients in the intervention group additionally receive home telemonitoring-supported care that connects them to the participating care providers by individual guideline-compliant care plans using the telemedicine-system Motiva® (Philips Medical Systems GmbH, Hamburg, Germany).
Motiva® is an interactive bi-directional home telemonitoring system that provides remote monitoring, empowers patients to manage their disease state more effectively and enables physicians to keep in contact with the patient at home on a daily basis. Patients measure their vital signs (blood pressure, heart rate, and weight) every day and Motiva® transfers the data to the relevant telemonitoring center. In doing so, signals of decompensation regarding their heart function can be detected at an early stage and counteractive measures can be taken. In addition, patients receive information via Motiva®, i.e. coaching material, evaluations, reminders, and feedback regarding their health status as well as references to potentially necessary CHF treatment adaptations. If questionnaires reveal any problems, patients receive a phone call from the study site. Additionally, patients receive standardized questionnaires related to symptoms of cardiac decompensation, hypotension or hypertension or abnormal pulse rates. A call from the telemedicine center is made if patients gain more than 2 kg within 3 days, if their systolic blood pressure exceeds 140 mmHg or is lower than 90 mmHg, or their resting heart rate exceeds 80 bpm or is lower than 50 bpm.
A secured broadband connection (Digital Subscriber Line (DSL) or Universal Mobile Telecommunications System (UMTS)) and a set-top box turn the patient’s television into their center of personalized care protected by a patient-specific password. Thus, patients can transfer all information about their health status to their attending physician safely.
Motiva® is been provided by Philips Medical Systems GmbH, Hamburg, Germany. The telecommunication infrastructure to transfer patients’ data is made available by T-Systems International GmbH, Frankfurt, Germany. Both are provided without any obligations that could influence the study.
Randomization
To assign patients to one of the two study arms, CardioBBEAT used a centralized stacked randomization technique. Patients at home who were managed in cardiologic practices were randomized patient-individually. Patients primarily managed by their general practitioner (GP), on the other hand, were cluster-randomized by their GP’s medical practices, to minimize carry-over effects and to keep the organizational effort manageable. The results of the randomization process with regard to the patients were displayed via the study’s electronic Case Report Form (eCRF) directly after inclusion into the trial. The study center in charge did inform the patients’ attending physicians whether their respective patients were enrolled in the trial and to which study arm they were assigned.
Treatment patterns
After patients are discharged from inpatient care, their GPs or outpatient medical specialists will provide their ambulatory care. These physicians have access to individual patient care plans and are authorized to complete or modify them.
Subjects enrolled in the control group receive best medical treatment according to the current guidelines of the European Society of Cardiology (ESC). Subjects enrolled in the intervention group are additionally supported by the telemedicine system Motiva® installed at the patients’ home usually within 2 weeks.
All trial participants maintain a patient diary and are urged to document any health disturbances at least once a week, such as hospitalizations (date of hospitalization, reason for admission, and length of stay), consultations by any physician, and change in medication or dose rate as well as adverse effects. In addition, every patient has to participate in 3 trial-specific examinations (Table 3) at their relevant study site, that take place at the time of enrollment and after 6 as well as 12 months.
Clinical outcome measures
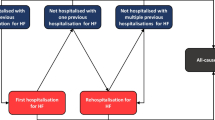
The primary outcome measure to assess the benefit of home telemonitoring is the combined clinical endpoint “days alive and not in hospital nor inpatient care per potential days in study.” For deceased patients, the loss in lifetime is taken into account by setting the denominator to 360 days, for patients lost to follow-up, time to last contact is used. Secondary outcome measures are total mortality, number of inpatient treatments, length of stay in hospital or nursing home, functional state of health and health-related quality of life. These will be determined by the following parameters: days survived in the study, number of hospitalizations for any reason during the study (especially cardiac and heart failure-related reasons), number of days in hospital or nursing home per study month, generic (short form health survey with 36 questions using norm-based scoring (SF-36v2), World Health Organization Five, well-being index (WHO-5)) and disease-specific (Kansas City Cardiomyopathy Questionnaire, (KCCQ)) health-related quality of life as well as medical condition and capacity of each patient.
CardioBBEAT may also be able to differentiate between particular sub-groups (e.g. gender-specific, NYHA-specific, urban/rural, diabetes mellitus) while analyzing the effectiveness of the intervention. The expectation is that several patient groups can be identified which are particularly suited for home telemonitoring with regard to clinical and/or economic outcome.
Cost data
CardioBBEAT aims to reflect the impact of home telemonitoring within an actual health care setting based on originally obtained cost data subdivided into cost of intervention, cost of inpatient and outpatient care, rehabilitation, nursing, and life-saving appliances. To this end, cost data are obtained from patients’ health insurance companies and later on validated using the records of the telemonitoring centers, GPs and medical specialists as well as patients’ diaries. Health insurance data will be obtained similarly for both, patients in the intervention group as well as the control group to avoid ascertainment bias.
All data are analyzed with appropriate statistical methods to determine the economic effectiveness of home telemonitoring for patients with CHF. Common approaches for the analysis of cost data such as t tests, analysis of covariance, bootstrap techniques or permutation tests will be compared regarding their feasibility, the validity of underlying assumptions and their stability and robustness in particular if missing values have to be taken into account.
Especially when analyzing cost data or determining the Incremental Cost-Effectiveness Ratio (ICER), assumptions are made regarding discount rate, utilities, projections or estimation of costs, which are based on uncertain hypotheses. To better understand the outcomes of these analyses, CardioBBEAT uses sensitivity analyses considering best-case and worst-case scenarios to demonstrate in which way the outcomes depend on these assumptions and how they affect their assessment.
Statistical analysis
The primary endpoint ICER, consisting of the group’s difference in total cost and the combined clinical endpoint “days alive and not in hospital nor inpatient care per potential days in study”, is calculated with confidence intervals obtained by resampling methods. The comparative conventional endpoint “event-free survival” to measure the intervention’s effectiveness is evaluated using the Kaplan-Meier analysis and log rank tests. To incorporate possible repeated hospitalizations of a patient, additional analyses will be performed, e.g. comparison of quarterly data and recurrent event analysis.
Secondary outcome measures such as number of stays in hospital per quarter, health-related quality of life or time of survival are analyzed via permutation test, covariance analysis or log rank test as part of the Kaplan-Meier analysis.
Furthermore, the trial uses a cluster-randomization technique and, therefore, correlation effects can evolve due to the collective treatment of patients in a cardiology center, medical practice, or by a single study nurse. Such effects can result in incorrect p values. CardioBBEAT uses frailty and multi-level models to assess if and where such correlations occur. The magnitude of these correlations will be measured and the p values will be rectified.
Since at planning stage neither an established statistical method to directly compare costs and ICERs nor sufficient data to estimate the variability of cost estimates was available, the sample size was determined based on literature data. With respect to clinical endpoints, the figures were rather stable and converged to a minimum of 300 patients per group. Since the primary endpoint was expected to be mainly driven by clinical events, it was assumed that the sample size will also be sufficient for the continuously distributed ICER.
Results
The study group comprised 621 patients, predominantly men. Four hundred and seventy-two (76 %) patients were treated by 449 GPs and 149 (24 %) were treated in 119 cardiologic practices. Three hundred and two patients were randomized into the intervention group and 319 patients into the control group. Ischemic cardiomyopathy was the leading cause of heart failure (59 %). Although randomly assigned, subjects of the control group were significantly more often in NYHA functional classes III or IV and exhibited peripheral edema or renal dysfunction, respectively, more frequently (Table 4). Additionally, the control and intervention group differed in heart rhythm disturbances (Table 5). No differences were detected regarding risk factor profile, comorbidities, echocardiographic parameters, especially left ventricular and diastolic diameter and ejection fraction, as well as functional test (6 MWD) results, medication and quality of life (Tables 4, 5, 6 and 7).
In comparison with recently published German trials (TIM-HF [7], Interdisciplinary Network for Heart failure study (INH) [14]) the CardioBBEAT target population was slightly younger and comprised more male patients with fewer in NYHA classes III and IV. Nevertheless, all patients were either categorized in AHA stages C or D and every fifth patient of the given cohort was diagnosed with peripheral edema; this suggests that the study population had a comparable degree of heart failure. Regarding comorbidities and risk factor profile, the study population was very similar, particularly for diabetes or renal dysfunction. Remarkably, it revealed a left bundle branch block in approximately 25 % of the population, a rhythm disorder with a known worse prognosis [15]. Furthermore, detailed information on prognostic relevant therapies was documented. Besides a high proportion of guideline-based pharmacotherapy including beta blockers and ACE inhibitors/ARB inhibitors, the study population was treated with mineralocorticoid receptor blockers in 71 % of all cases. A cardioverter-defibrillator or a resynchronization system was implanted in two thirds of our patients (comparable to TIM-HF study [7]) with a considerable prognostic impact on primary and secondary endpoints. Table 8 compares the most important baseline characteristics with TIM-HF [7] and INH [14].
Discussion
Several recent randomized controlled trials (RCTs), including TIM-HF [7, 16] and INH [14], have proven the positive clinical effects of home telemonitoring on several groups of patients diagnosed with CHF. The meta-analyses of Clark et al. [4], Klersy et al. [5] and Inglis et al. [6] also showed its potential to improve several clinical outcomes such as quality of life. However, many results were not statistically significant mostly due to the fact that effects were too small despite adequately sized studies.
Another meta-analysis by Klersy et al. [10] focused on the economic impact of remote patient monitoring. It showed that management of HF patients by remote monitoring is cost-saving due to a substantial reduction in health care resource utilization, mostly driven by a reduction in the number of HF hospitalizations. However, cost data in this meta-analysis was estimated using 3 diagnosis-related group reimbursements (minimum, median, maximum over countries) and 3 different incidence rates and their lower and upper 95 % CI (confidence interval). These facts reflect the requirement for additional study-derived and reliable evidence based on originally obtained cost data unlike previously negotiated prices.
In CardioBBEAT, the follow-up care of patients was more diverse than expected: the number of participating practices was higher whereas the number of patients per practice was lower than expected, resulting in an incomplete use of the random blocks implemented in the eCRF and slightly unequal sample sizes between the random groups. However, slight differences in group sizes are of no concern with respect to unbiasedness of results.
At first glance, an imbalance in baseline variables stands out. But, even with perfect randomization the expected number of statistically significant differences between baseline variables is 5 % or 2.45 of the 49 baseline comparisons in Tables 4, 5, 6 and 7, on average. In case of independence of the baseline variables, the observed number of significances will thus follow a binomial distribution with p = 0.05. In CardioBBEAT, 4 out of 49 baseline comparisons (8.2 %) were significant. In case of independence, 4 or more significant comparisons would occur in 23 % of the cases even in perfect randomization. The observed baseline differences could thus well be a play of chance. However, NYHA functional class, peripheral edema, heart rhythm, and renal dysfunction were clinically highly relevant variables that might bias the conclusions even if evoked by chance. Therefore, the statistical analysis plan was extended to include adjusted analyses with respect to the baseline imbalances.
Conclusions
CardioBBEAT is a RCT that adds a comprehensive cost assessment to the clinical component of the study including actual costs generated by patients, health services and health products. The corresponding data have been obtained directly from patients’ health insurances including statutory sickness funds and private insurances. This will provide more reliable information about the cost-effectiveness of home telemonitoring in CHF patients based on the actual health care setting. CardioBBEAT may also be able to differentiate between particular sub-groups (gender-specific, NYHA-specific, urban/rural, diabetes mellitus) while analyzing the effectiveness of the intervention. The expectation is that important patient groups, which are better suited for the input of telemedicine with regard to the clinical and/or economic outcome, can be identified. The study results, reflecting a guideline-compliant, highly accurate treatment of the whole CardioBBEAT study population shown above, will significantly contribute to the existing data basis on home telemonitoring in CHF. Therefore, it adds to informed political and economic decision-making within the specific context of the German Health Care System.
Individual gratitude
Abbreviations
- ACE:
-
angiotensin converting enzyme
- AE:
-
adverse event
- AHA:
-
American Heart Association, staging of heart failure
- ARB:
-
angiotensin receptor blocker
- BMI:
-
body mass index
- CHF:
-
chronic heart failure
- CI:
-
confidence interval
- CM:
-
cardiomyopathy
- COPD:
-
chronic obstructive pulmonary disease
- CRT-D:
-
cardiac resynchronization therapy combined with defibrillation
- DSL:
-
Digital Subscriber Line (broadband connection)
- ECG:
-
electrocardiogram
- eCRF:
-
electronic Case Report Form
- ESC:
-
European Society of Cardiology
- GFR:
-
glomerular filtration rate
- GP:
-
general practitioner
- HF:
-
heart failure
- ICD:
-
implantable cardioverter defibrillator
- ICER:
-
Incremental Cost-Effectiveness Ratio
- INH:
-
Interdisciplinary Network for Heart failure study
- KCCQ:
-
Kansas City Cardiomyopathy Questionnaire with 23 items for measuring disease-specific domains in CHF
- LBBB:
-
left bundle branch block
- LVEDD:
-
left ventricular end-diastolic dimension
- LVEF:
-
left ventricular ejection fraction
- MR:
-
mineralocorticoid receptor
- MWD:
-
minute walking distance
- n.a.:
-
not available
- NYHA:
-
New York Heart Association, classification of heart failure
- PAD:
-
peripheral arterial disease
- RBBB:
-
right bundle branch block
- RCT:
-
randomized controlled trial
- SAE:
-
serious adverse event
- SF-36v2:
-
short form health survey with 36 questions using norm-based scoring
- TELE-HF:
-
Telemonitoring in patients with Heart Failure trial
- TIA:
-
transient ischemic attack
- TIM-HF:
-
Telemedical Interventional Management in Heart Failure trial
- UMTS:
-
Universal Mobile Telecommunications System (mobile cellular system)
- WHO-5:
-
World Health Organization Five, well-being index
References
Cleland JGF, Swedberg K, Follath F, Komajda M, Cohen-Solal A, Aguilar JC, et al. The EuroHeart Failure survey programme – a survey on the quality of care among patients with heart failure in Europe: Part 1: patient characteristics and diagnosis. Eur Heart J. 2003;24:442–63.
Federal Statistical Office – Destatis. Gesundheit: Fallpauschalenbezogene Krankenhausstatistik. https://www.destatis.de/DE/Publikationen/Thematisch/Gesundheit/Krankenhaeuser/FallpauschalenKrankenhaus2120640137004.pdf?__blob=publicationFile. 2013. Accessed 24 Sep 2014.
Federal Statistical Office – Destatis. Gesundheitsberichterstattung des Bundes: Krankheitskosten in Mio. €. http://www.gbe-bund.de. 2014. Accessed 24 Sep 2014.
Clark RA, Inglis SC, McAlister FA, Cleland JGF, Stewart S. Telemonitoring or structured telephone support programmes for patients with chronic heart failure: systematic review and meta-analysis. BMJ. 2007;334:942.
Klersy C, de Silvestri A, Gabutti G, Regoli F, Auricchio A. A meta-analysis of remote monitoring of heart failure patients. J Am Coll Cardiol. 2009;54:1683–94.
Inglis SC, Clark RA, McAlister FA, Stewart S, Cleland JGF. Which components of heart failure programmes are effective? A systematic review and meta-analysis of the outcomes of structured telephone support or telemonitoring as the primary component of chronic heart failure management in 8323 patients: Abridged Cochrane Review. Eur J Heart Fail. 2011;13:1028–40.
Koehler F, Winkler S, Schieber M, Sechtem U, Stangl K, Böhm M, et al. Impact of remote telemedical management on mortality and hospitalizations in ambulatory patients with chronic heart failure: the Telemedical Interventional Monitoring in Heart Failure Study. Circulation. 2011;123:1873–80.
Chaudry SI, Mattera JA, Curts JP, Spertus JA, Herrin J, Zhenqiu L, et al. Telemonitoring in patients with heart failure. N Engl J Med. 2010;363:2301–9.
Heinen-Kammerer T, Wiosna W, Nelles S, Rychlik R. Monitoring von Herzfunktionen mit Telemetrie. Cologne, Germany: DAHTA@DIMDI. 2006;30.
Klersy C, de Silvestri A, Gabutti G, Raisaro A, Curti M, Regoli F, et al. Economic impact of remote patient monitoring: an integrated economic model derived from a meta-analysis of randomized controlled trials in heart failure. Eur J Heart Fail. 2011;13:450–9.
von der Schulenburg JM G, Greiner W, Jost F, Klusen N, Kubin M, Leidl R, et al. German recommendations on health economic evaluation: third and updated version of the Hanover Consensus. Value Health. 2008;11:539–44.
Dickstein K, Cohen-Solal A, Filippatos G, McMurray JJV, Ponikowski P, et al. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2008: the Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2008 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association of the ESC (HFA) and endorsed by the European Society of Intensive Care Medicine (ESICM). Eur Heart J. 2008;29:2388–442.
McMurray JJV, Adamopoulos S, Anker SD, Auricchio A, Böhm M, Dickstein K, et al. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2012. The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2012;33:1787–847.
Angermann CE, Störk S, Gelbrich G, Faller H, Jahns R, Frantz S, et al. Mode of action and effects of standardized collaborative disease management on mortality and morbidity in patients with systolic heart failure: the Interdisciplinary Network for Heart Failure (INH) study. Circ Heart Fail. 2012;5:25–35.
Dissmann R, Kamke W, Reibis R, Herbstleb J, Wegscheider K, Völler H. Prognostic impact of left bundle-branch block in the early stable phase after acute myocardial infarction. Int J Cardiol. 2008;130:438–43.
Koehler F, Winkler S, Schieber M, Sechtem U, Stangl K, Böhm M, et al. Telemedicine in heart failure: pre-specified and exploratory subgroup analyses from the TIM-HF trial. Int J Cardiol. 2012;161:143–50.
Funding
The CardioBBEAT trial is supported by the Federal Ministry of Education and Research in cooperation with (and managed by) the German Aerospace Center (grant number 01KX0805). The home telemonitoring system Motiva® is provided by Philips Medical Systems GmbH, the electronic infrastructure by T-Systems International GmbH.
Author information
Authors and Affiliations
Consortia
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
RH made substantial contributions to the development, implementation and management of the study, drafted the manuscript and will perform the economic analysis and interpretation of data. HV made substantial contributions to conception and design of the study, is principal investigator and head of clinical trial, member of steering committee, revised the manuscript critically and will perform the clinical interpretation of data. KN made substantial contributions to the development and coordination of the study, is head of health economics evaluation, member of steering committee, sponsor, and revised the manuscript critically. DB made substantial contributions to the development and management of the study, drafted the manuscript, is corresponding author and will perform the economic analysis and interpretation of data. EV made substantial contributions to conception and design of the study, drafted the manuscript and will perform the biometry and statistical analysis and interpretation of data. RD made substantial contributions to conception, design, implementation and management of the study and revised the manuscript critically. WW made substantial contributions to conception, design and implementation of the study and revised the manuscript critically. TN made substantial contributions to acquisition of data, is principal investigator and revised the manuscript critically. SS made substantial contributions to acquisition of data, is principal investigator and revised the manuscript critically. OB made substantial contributions to acquisition of data, is principal investigator and revised the manuscript critically. KW made substantial contributions to conception and design of the study, is head of biometry and statistical analysis, member of steering committee and revised the manuscript critically. EN made substantial contributions to conception and design of the study, is head of health economics evaluation, member of steering committee, sponsor, and revised the manuscript critically. EF made substantial contributions to conception and design of the study, is principal investigator and head of clinical trial, member of steering committee, revised the manuscript critically and will perform the clinical interpretation of data. All authors read and approved the final manuscript.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Hofmann, R., Völler, H., Nagels, K. et al. First outline and baseline data of a randomized, controlled multicenter trial to evaluate the health economic impact of home telemonitoring in chronic heart failure – CardioBBEAT. Trials 16, 343 (2015). https://doi.org/10.1186/s13063-015-0886-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13063-015-0886-8