
Abstract
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) causes virus-induced-senescence. There is an association between shorter telomere length (TL) in coronavirus disease 2019 (COVID-19) patients and hospitalization, severity, or even death. However, it remains unknown whether virus-induced-senescence is reversible. We aim to evaluate the dynamics of TL in COVID-19 patients 1 year after recovery from intensive care units (ICU). Longitudinal study enrolling 49 patients admitted to ICU due to COVID-19 (August 2020 to April 2021). Relative telomere length (RTL) quantification was carried out in whole blood by monochromatic multiplex real-time quantitative PCR (MMqPCR) assay at hospitalization (baseline) and 1 year after discharge (1-year visit). The association between RTL and ICU length of stay (LOS), invasive mechanical ventilation (IMV), prone position, and pulmonary fibrosis development at 1-year visit was evaluated. The median age was 60 years, 71.4% were males, median ICU-LOS was 12 days, 73.5% required IMV, and 38.8% required a prone position. Patients with longer ICU-LOS or who required IMV showed greater RTL shortening during follow-up. Patients who required pronation had a greater RTL shortening during follow-up. IMV patients who developed pulmonary fibrosis showed greater RTL reduction and shorter RTL at the 1-year visit. Patients with longer ICU-LOS and those who required IMV had a shorter RTL in peripheral blood, as observed 1 year after hospital discharge. Additionally, patients who required IMV and developed pulmonary fibrosis had greater telomere shortening, showing shorter telomeres at the 1-year visit. These patients may be more prone to develop cellular senescence and lung-related complications; therefore, closer monitoring may be needed.
Similar content being viewed by others


Introduction
Coronavirus disease 2019 (COVID-19) has been declared a pandemic and global emergency by the World Health Organization (WHO). It is an airborne disease caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), leading to a range of respiratory infections from mild symptoms to severe conditions such as pneumonia or acute respiratory distress syndrome (ARDS) [1].
Around 20% of severe cases are transferred to the intensive care unit (ICU) where invasive mechanical ventilation (IMV) is often required for approximately 10 days [2, 3]. While these vital methods are crucial for patient survival, they can cause lung injury, oxidative stress and a reduction of antioxidant enzymes, leading to accelerated telomere shortening and immune senescence [4,5,6]. This accelerated oxidative stress, in combination with normal aging and other health conditions, leads to telomere shortening. When telomeres reach a critical threshold in length, it can trigger senescence and apoptosis depending on the cell type. These factors also contribute to immune senescence, altering the function of the immune cells and increasing the risk of infection and age-related diseases [7].
Moreover, virus-induced senescence directly affects the length of lymphocyte telomeres, mostly impacting older adults who are at a higher risk of severe COVID-19-related complications [8, 9]. There is an association between shorter telomere length and the need for hospitalization, greater severity of COVID-19, and even mortality [10,11,12]. Schneider et al. recently linked telomere shortening to an increased mortality risk in respiratory diseases, with a Hazard Ratio of 1.4 [13]. A recent study also found that individuals who recovered from SARS-CoV-2 infection had shorter telomeres around one year after recovery, and this shortening was associated with higher severity of the disease [14]. However, while telomere shortening during ICU stay has been observed due to reasons other than COVID-19 [15], to date, there are no longitudinal studies evaluating telomere shortening or recovery in patients admitted to the ICU. Therefore, this study aimed to assess the change in telomere length in patients admitted to the ICU at least one year after hospital discharge.
Materials and methods
Design and study population
We performed a longitudinal study of COVID-19 patients admitted to the ICU at the Tajo University Hospital (Aranjuez, Madrid) and Infanta Cristina University Hospital (Parla, Madrid) from August 2020 to April 2021, who were followed for at least 12 months from hospital discharge. Patients were diagnosed by laboratory confirmation (RNA detection by PCR or serology-based methodology) or by consideration of clinical manifestations compatible with COVID-19. The strengthening the reporting of observational studies in epidemiology (STROBE-ID) checklist was followed (Supplemental File 1). The study protocol was approved by the Ethics Committee of the Institute of Health Carlos III (PI 33_2020-v3) and the Investigation Committee of both hospitals.
Clinical data and samples
Epidemiological and clinical variables were collected from medical records with research electronic data capture (REDCap) [16]. Peripheral blood samples were obtained in ethylenediaminetetraacetic acid (EDTA) tubes upon admission to the ICU and at least one year after discharge. DNA was isolated with the commercial kit “ReliaPrep™ Blood gDNA Miniprep System” from PROMEGA, according to the manufacturer’s instructions. DNA concentration and quality were determined using NanoDrop™ One/OneC (Thermo Scientific™). All samples were then diluted into 10 ng/uL working aliquots.
Telomere relative quantification
Relative telomere length (RTL) quantification was carried out by monochromatic multiplex real-time quantitative PCR (MMqPCR) assay as previously described [12]. Each MMqPCR plate included a standard curve generated by serial dilution (1:3) of a pool of DNA extracted from plasma samples of 20 healthy individuals. The standard curve was run in duplicate for each run, along with a duplicated negative control. Every experimental sample was tested in triplicate. Any samples with a coefficient of variation (CV) greater than 0.15 were reanalyzed, and samples that still had a CV greater than 0.15 were discarded (see Supplemental File 2 for extended information).
Study variables
The outcome variable was the change of RTL from baseline to one-year visit. This change was analyzed using the RTL ratio (one-year RTL / baseline RTL). The secondary outcome was the RTL at one-year visit.
The study factors included were: (a) Hospitalization variables: (i) ICU length of stay (ICU-LOS); (ii) need for IMV and its duration; (iii) prone position during the first 7 days of ICU stay. (b) Radiologic alterations in the one-year visit for the subgroup of patients who required IMV: presence of fibrosis on the X-ray image.
Statistical analysis
For the descriptive analysis, the McNemar test for categorical variables and the Wilcoxon test for continuous variables were used.
Regarding RTL measurement, outlier identification was performed using the interquartile range (IQR) method. Correlation between RTL and age was performed using Spearman correlation.
For telomere size differential analysis, we performed the Mann–Whitney test for transversal analysis and the Wilcoxon test for longitudinal analysis between paired samples. We used Generalized Linear Models (GLMs) with gamma distribution to study the association between the baseline RTL, RTL ratio, and one-year RTL values (y, dependent variables) with the need for IMV, IMV duration, ICU-LOS, prone position, and pulmonary fibrosis development at the end of the follow-up (x, independent variables). This test provides the arithmetic means (AMR) ratio and its significance level. GLMs were adjusted by the most relevant covariates by using a stepwise method (forward), where at each step, the covariates were considered to enter according to the lowest Akaike information criteria (AIC) for that specific model. The covariates included were age, gender, body mass index (BMI), sequential organ failure assessment (SOFA) score at admission, PCR plate, and follow-up time (months) when GLMs included variables from the one-year visit. For the association analysis with radiological alterations, we analyzed the differences in epidemiological and clinical variables between groups (no alterations and fibrosis), and significant variables were included as covariables in the model.
Statistical software R (v.4.2.2) was used to perform the statistical analysis. All p-values were two-tailed, and the statistical significance was p ≤ 0.05.
Results
Patient characteristics
Clinical and epidemiological characteristics of the 49 patients according to the baseline and one-year time (after a median of 13.8 months) are shown in Table 1.
Overall, the median age was 60 years; 71.4% were male, and more than 80% were Caucasian. In addition, 42.9% had hypertension, 55.1% obesity, and 37.4% diabetes. Regarding hospitalization variables, 73.5% required IMV, patients had a median ICU-LOS of 12 days and IMV duration of 14 days, and 38.8% needed a prone position (first 7 days). At baseline, no patient was vaccinated but received the first dose before the one-year visit.
In addition, we found a negative but not significant physiological correlation between RTL and age at baseline (r = − 0.242; p = 0.094) and significant at one-year visit (r = − 0.310; p = 0.030) (Supplemental File 3).
Evolution of RTL according to hospitalization variables
Firstly, we analyzed the epidemiological and clinical differences between patients who experienced an increase in RTL and those who had a decrease from baseline to one year. We found that patients who shortened their RTL showed significantly higher body temperature (p = 0.036), longer ICU LOS (p = 0.008), a greater need for IMV (p = 0.002), and all of them developed pulmonary fibrosis by the end of the follow-up period (p = 0.019). It's worth noting that there were no differences in terms of age or the presence of comorbidities (Supplemental File 4).
ICU-LOS While no differences were found at baseline, prolonged ICU-LOS was related to RTL differently. Thus, we observed that only those patients with ICU-LOS > 12 days showed significantly shortened telomeres size (p < 0.001), while patients with an ICU-LOS < 12 days showed similar RTL (p = 0.380) during follow-up (Fig. 1A).

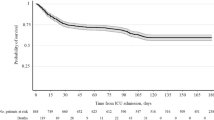
A Evolution of relative telomere length (RTL) in COVID-19 patients, stratified by length of stay (LOS) in the intensive care unit (ICU), need for invasive mechanical ventilation (IMV), and need for prone position, from baseline to one-year visit (12 months since hospital discharged). B Differences in RTL, one-year visit, in COVID-19 patients who required IMV and had X-ray images, comparing patients without radiological alterations and with fibrosis. Statistics: Data represent the crude means and 95% confidence interval for each group of patients. P-values were calculated using the Mann–Whitney test for transversal analysis and the Wilcoxon test for longitudinal analysis between paired samples. R and p-value in the scatter plot were calculated by a Spearman’s correlation. Statistical significance was determined as p ≤ 0.05. Abbreviations: RTL, Relative telomere length; ICU, Intensive care unit; IMV, Invasive mechanical ventilation
Need for IMV and its duration No differences in RTL were found at baseline, but those patients who required IMV significantly reduced their RTL during follow-up (p < 0.001). So, those patients admitted to the ICU but who did not receive IMV significantly increased their RTL during follow-up (p = 0.012) (Fig. 1A) (Supplemental File 5). Besides, one year after discharge, patients without IMV showed higher RTL than those with IMV, although this difference did not reach significance p = 0.068).
Need for a prone position The requirement for a prone position suggests a more severe and worse evolution of ARDS. Therefore, we analyzed the RTL between patients with and without needing a prone position during the first 7 days. While no differences were observed at baseline, those patients who required a prone position significantly reduced their RTL during follow-up (p = 0.005). On the other hand, patients who were not placed in the prone position did not modify their RTL during follow-up (Fig. 1A).
Radiologic abnormalities at one-year visit
For the subgroup of patients who required IMV and had an X-ray image at the one-year visit (n = 33), 63.3% had no radiological alterations, 9.1% had interstitial infiltrates, and 27.3% had fibrosis. Regarding the clinical and epidemiological characteristics of extreme phenotypes (fibrosis and no radiological alterations), we only observed significant differences in the presence of arterial hypertension at baseline (p = 0.035) and IMV days during ICU stay (p = 0.043), so both variables were included in the model (Supplemental File 6).
Regarding the association analysis, patients with fibrosis showed a higher RTL shortening at the one-year visit (p = 0.007) than those without radiological abnormalities. Additionally, these differences remained significant at the one-year visit, where patients who developed pulmonary fibrosis showed significantly lower RTL (p = 0.040) (Fig. 1B).
All the significant results for each comparison were confirmed by multivariate GLMs adjusted by the covariates selected by a stepwise method (Supplemental File 5).
Discussion
In this longitudinal study, we found that patients with longer ICU-LOS and those who required IMV had a greater shortening of the RTL during the first year after hospital discharge. In addition, patients who developed pulmonary fibrosis showed a deep reduction of RTL during the first year after hospital discharge, showing lower RTL at the one-year visit than those who did not have pulmonary fibrosis. To our knowledge, our study is the first one showing an association between RTL shortening and clinical variables of hospitalization after more than one year of follow-up in COVID-19 patients admitted to the ICU.
Telomere length shortens with each cell division and, when it reaches a critical length (dysfunctional telomeres), senescence and apoptosis are elicited [17]. Telomere shortening has been associated with numerous diseases, including age-related diseases, stress-related conditions, cancer, and bacterial and viral infections [18, 19]. In the context of these diseases, inflammation or oxidative stress induces accelerated telomere shortening [20]. However, this molecular process can be reversed in some cell types due to the presence of telomerase enzyme, which is responsible for maintaining telomere length [21]. In our study, we could not measure telomerase, so we could not evaluate the cells’ capacity to reverse telomere shortening.
In the context of COVID-19, complications of the disease are more likely to occur in older individuals, suggesting that age-related molecular pathways contribute to its severity [22]. In this regard, several studies have shown a link between shorter telomeres and an increased need for hospitalization, greater disease severity, and even mortality in COVID-19 patients [10,11,12]. However, few studies have investigated the changes in telomere length after patients are discharged from the hospital. Retuerto et al. found that, after a median of 14 months of follow-up, 35% of study participants experienced telomere shortening. Although they did not find an association between RTL and clinical outcomes in the hospital, this might be due to the heterogeneous nature of their study population, which included varying levels of disease severity. However, the patients who had a more severe disease also exhibed the greatest telomere shortening [14]. The impact and, consequently, the implications of telomere shortening in COVID-19 patients admitted to the ICU remain unknown.
In this study, patients with longer ICU-LOS experienced a shortening of RTL during follow-up. This could be attributed to the critical exhaustion of the immune system after an extended ICU stay, where telomeres would reach a critical size, compromising the capacity of telomerase to restore telomere length. Previous studies have demonstrated significant changes in leukocyte telomere size in critically ill patients during the ICU stay [15, 23]. However, to our knowledge, no studies have investigated the impact of ICU-LOS on RTL after hospital discharge. Our findings highlight the importance of follow-up for patients with prolonged ICU-LOS to monitor for future senescence-related complications.
Patients requiring IMV had a longer ICU-LOS and a worse prognosis [24]. Overall, we found that, in critically ill COVID-19 patients, the need for IMV was associated with telomere shortening during follow-up, possibly reflecting lung damage and loss of functionality. To our knowledge, few studies have addressed this issue. Only Liang et al. observed telomere shortening in ICU patients requiring IMV, but their evaluation was conducted only two days after ICU discharge [23]. Therefore, additional studies with longer follow-up periods are needed to elucidate the impact of IMV on RTL reduction and its association with post-COVID syndrome in patients admitted to the ICU.
In severe patients with worse evolution of ARDS, a prone position is recommended to improve oxygen saturation and reduce lung damage [25, 26]. A prone position significantly reduces the rate of tracheal intubation and mortality [27], although there are also studies with contradictory results [28]. Moreover, among intubated patients, those who respond to the prone position in terms of oxygenation show better survival than non-responders [29]. Regarding evolution after discharge, our study revealed that COVID-19 patients who required a prone position experienced telomere shortening during follow-up. To our knowledge, these findings are the first to associate the prone position with reduced telomere size in COVID-19 patients during the first year after hospital discharge. Further studies with a longer follow-up are needed to determine whether telomere size evolves to more critical levels in this subgroup of patients.
COVID-19 patients often develop fibrotic pulmonary sequelae [30,31,32]. There is also an association between telomere shortening in immune cells and the development of lung diseases, such as idiopathic pulmonary fibrosis [7, 33,34,35]. In our study, while no significant differences in RTL were observed at baseline, patients who experienced RTL shortening during follow-up developed lung fibrosis. Similarly, patients with fibrotic pulmonary sequelae had shorter RTL at the one-year visit than those without radiological abnormalities. To our knowledge, this is the first study assessing the RTL and fibrosis development during follow-up in ICU patients. Still, these findings are in concordance with previous studies in hospitalized patients. McGroder et al. showed that patients with shorter telomere size at hospitalization were more prone to develop fibrotic abnormalities in the lung four months later, but the telomere length dynamics were not addressed [36]. Using a different approach (Quantitative telomere Fluorescence in situ Hybridization Q-FISH), Martínez et al. found loss of alveolar type II (ATII) cellularity and shorter telomeres in these cells in post-COVID-19 lung cancer patients. Authors suggested that ATII cell telomere reduction may trigger lung fibrosis development in post-COVID-19 patients [37], although these results were obtained in a cancer background, and studies on non-lung cancer COVID-19 patients are needed. Similarly, Mulet et al., in a recent prospective study [38], described that this attrition could also be evaluated on peripheral blood cells, as COVID-19 patients with radiological signs of fibrosis had significant telomere shortening one year after leaving the hospital. However, this study involved only 19 patients, and the authors did not specify how they measured telomere length. Retuerto et al. also observed that patients who experienced peripheral blood leukocyte telomere shortening after discharge were more prone to show persistent radiographic abnormalities. However, this study was conducted during the first pandemic wave, when the hospital admission criteria were exceptional.
Our study is the first to confirm these findings in ICU patients, with a homogeneous group characterized by similar severity and clinical strategies. However, further studies with longer follow-up periods are needed to establish the role of RTL shortening on fibrotic pulmonary sequelae and vice versa.
Limitations
Several issues must be considered to interpret our data correctly. The sample size was limited as only patients with the one-year visit were included in the study. This may have limited the statistical power of the analysis, and some significant associations may not have been detected. However, despite its preliminary nature, the statistical analyses correctly addressed this issue. It is important to note that other potential factors potentially impacting telomere shortening, like telomerase activity, could not be measured. Additionally, it is unclear whether the viral genotype or the viral inoculum, which may impact the disease severity, could have also played a role in influencing telomere attrition. This study also has several strengths, such as the fact that all patients were recruited during the second and third pandemic waves, where the ICU admission criteria were similar, and the selected method of measuring telomere length. We measured RTL in whole blood, and its determination could be transferred to routine clinical practice. This study addressed a topic that has been scarcely studied until now in critical patients because the recruitment and follow-up of these patients are arduous. In addition, it should be noted that we analyzed RTL before initiating any mechanical ventilation.
Conclusions
In conclusion, we found that patients with longer ICU stays, need for IMV, and fibrosis development shortened telomere size in the first year after hospital discharge. In addition, patients who required IMV and developed pulmonary fibrosis showed shorter telomeres at the one-year visit. The findings of this preliminary study suggest that these patients need extensive monitoring as they are at higher risk of developing cellular senescence-related and chronic respiratory complications.
Availability of data and materials
All data are available upon request to the corresponding authors.
Abbreviations
- ARDS:
-
Acute respiratory distress syndrome
- ACE:
-
Angiotensin-converting-enzyme inhibitors
- AIIRA:
-
Angiotensin II receptor antagonists
- AIC:
-
Akaike information criteria
- ATII:
-
Alveolar type II
- AMR:
-
Arithmetic mean ratio
- BMI:
-
Body mass index
- CV:
-
Coeficient of variation
- CI:
-
Confidence interval
- COVID-19:
-
Coronavirus disease 2019
- EDTA:
-
Ethylenediaminetetraacetic acid
- GLMs:
-
Generalized linear models
- ICU:
-
Intensive care unit
- ICU-LOS:
-
ICU length of stay
- IMV:
-
Invasive mechanical ventilation
- IQR:
-
Interquartile range
- MMqPCR:
-
Monochromatic multiplex real-time quantitative PCR
- PCR:
-
Polymerase chain reaction
- Q-FISH:
-
Quantitative telomere fluorescence in situ hybridization
- RTL:
-
Relative telomere length
- REDCap:
-
Research electronic data capture
- SOFA:
-
Sequential organ failure assessment
- SARS-CoV-2:
-
Severe acute respiratory syndrome coronavirus 2
- STROBE:
-
Strengthening the reporting of observational studies in epidemiology
- TL:
-
Telomere length
- WHO:
-
World health organization
References
Anka AU, Tahir MI, Abubakar SD, Alsabbagh M, Zian Z, Hamedifar H, et al. Coronavirus disease 2019 (COVID-19): an overview of the immunopathology, serological diagnosis and management. Scand J Immunol. 2021;93: e12998.
Chang R, Elhusseiny KM, Yeh YC, Sun WZ. COVID-19 ICU and mechanical ventilation patient characteristics and outcomes-A systematic review and meta-analysis. PLoS ONE. 2021;16: e0246318.
Wolff D, Nee S, Hickey NS, Marschollek M. Risk factors for Covid-19 severity and fatality: a structured literature review. Infection. 2021;49:15–28.
Joelsson JP, Asbjarnarson A, Sigurdsson S, Kricker J, Valdimarsdottir B, Thorarinsdottir H, et al. Ventilator-induced lung injury results in oxidative stress response and mitochondrial swelling in a mouse model. Lab Anim Res. 2022;38:23.
Sun ZT, Yang CY, Miao LJ, Zhang SF, Han XP, Ren SE, et al. Effects of mechanical ventilation with different tidal volume on oxidative stress and antioxidant in lung. J Anesth. 2015;29:346–51.
Mazullo Filho JB, Bona S, Rosa DP, Silva FG, Forgiarini Junior LA, Dias AS, et al. The effects of mechanical ventilation on oxidative stress. Rev Bras Ter Intensiva. 2012;24:23–9.
Ruiz A, Flores-Gonzalez J, Buendia-Roldan I, Chavez-Galan L. Telomere shortening and its association with cell dysfunction in lung diseases. Int J Mol Sci. 2021;23(1):425.
Bellon M, Nicot C. Telomere dynamics in immune senescence and exhaustion triggered by chronic viral infection. Viruses. 2017;9(10):289.
Reyes A, Ortiz G, Duarte LF, Fernandez C, Hernandez-Armengol R, Palacios PA, et al. Contribution of viral and bacterial infections to senescence and immunosenescence. Front Cell Infect Microbiol. 2023;13:1229098.
Froidure A, Mahieu M, Hoton D, Laterre PF, Yombi JC, Koenig S, et al. Short telomeres increase the risk of severe COVID-19. Aging (Albany NY). 2020;12:19911–22.
Haridoss M, Ayyasamy L, Bagepally BS. Is COVID-19 severity associated with telomere length? A systematic review and meta-analysis. Virus Genes. 2023;59:489–98.
Virseda-Berdices A, Concostrina-Martinez L, Martinez-Gonzalez O, Blancas R, Resino S, Ryan P, et al. Relative telomere length impact on mortality of COVID-19: Sex differences. J Med Virol. 2023;95: e28368.
Schneider CV, Schneider KM, Teumer A, Rudolph KL, Hartmann D, Rader DJ, et al. Association of telomere length with risk of disease and mortality. JAMA Intern Med. 2022;182:291–300.
Retuerto M, Lledo A, Fernandez-Varas B, Guerrero-Lopez R, Usategui A, Lalueza A, et al. Shorter telomere length is associated with COVID-19 hospitalization and with persistence of radiographic lung abnormalities. Immun Ageing. 2022;19:38.
Zribi B, Uziel O, Lahav M, Mesilati Stahy R, Singer P. Telomere length changes during critical illness: a prospective, observational study. Genes. 2019;10(10):761.
Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)–a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42:377–81.
Lin J, Epel E. Stress and telomere shortening: Insights from cellular mechanisms. Ageing Res Rev. 2022;73: 101507.
Bar C, Blasco MA (2016). Telomeres and telomerase as therapeutic targets to prevent and treat age-related diseases. F1000Res, 5.
Rossiello F, Jurk D, Passos JF, d’Adda di Fagagna F. Telomere dysfunction in ageing and age-related diseases. Nat Cell Biol. 2022;24:135–47.
Barnes RP, Fouquerel E, Opresko PL. The impact of oxidative DNA damage and stress on telomere homeostasis. Mech Ageing Dev. 2019;177:37–45.
de Punder K, Heim C, Wadhwa PD, Entringer S. Stress and immunosenescence: The role of telomerase. Psychoneuroendocrinology. 2019;101:87–100.
Becerra-Munoz VM, Nunez-Gil IJ, Eid CM, Garcia Aguado M, Romero R, Huang J, et al. Clinical profile and predictors of in-hospital mortality among older patients hospitalised for COVID-19. Age Ageing. 2021;50:326–34.
Liang Z, Saugar EE, Alamian A, Ferreira T, Downs CA. Changes in telomere length and indicators of oxidative stress in critically ill mechanically ventilated adults - A pilot study. Biol Res Nurs. 2023;25:282–8.
Wang CH, Lin HC, Chang YC, Maa SH, Wang JS, Tang WR. Predictive factors of in-hospital mortality in ventilated intensive care unit: a prospective cohort study. Medicine (Baltimore). 2017;96: e9165.
Chua EX, Zahir S, Ng KT, Teoh WY, Hasan MS, Ruslan SRB, et al. Effect of prone versus supine position in COVID-19 patients: a systematic review and meta-analysis. J Clin Anesth. 2021;74: 110406.
Guerin C, Albert RK, Beitler J, Gattinoni L, Jaber S, Marini JJ, et al. Prone position in ARDS patients: why, when, how and for whom. Intensive Care Med. 2020;46:2385–96.
Tekantapeh ST, Nader ND, Ghojazadeh M, Fereidouni F, Soleimanpour H. Prone positioning effect on tracheal intubation rate, mortality and oxygenation parameters in awake non-intubated severe COVID-19-induced respiratory failure: a review of reviews. Eur J Med Res. 2024;29:63.
Nay MA, Hindre R, Perrin C, Clement J, Plantier L, Seve A, et al. Prone position versus usual care in hypoxemic COVID-19 patients in medical wards: a randomised controlled trial. Crit Care. 2023;27:240.
Kharat A, Simon M, Guerin C. Prone position in COVID 19-associated acute respiratory failure. Curr Opin Crit Care. 2022;28:57–65.
Safont B, Tarraso J, Rodriguez-Borja E, Fernandez-Fabrellas E, Sancho-Chust JN, Molina V, et al. Lung function, radiological findings and biomarkers of fibrogenesis in a cohort of COVID-19 patients six months after hospital discharge. Arch Bronconeumol. 2022;58:142–9.
Giacomelli C, Piccarducci R, Marchetti L, Romei C, Martini C. Pulmonary fibrosis from molecular mechanisms to therapeutic interventions: lessons from post-COVID-19 patients. Biochem Pharmacol. 2021;193: 114812.
Hirawat R, Jain N, Aslam Saifi M, Rachamalla M, Godugu C. Lung fibrosis: Post-COVID-19 complications and evidences. Int Immunopharmacol. 2023;116: 109418.
Planas-Cerezales L, Arias-Salgado EG, Buendia-Roldan I, Montes-Worboys A, Lopez CE, Vicens-Zygmunt V, et al. Predictive factors and prognostic effect of telomere shortening in pulmonary fibrosis. Respirology. 2019;24:146–53.
Qian Y, Ding T, Wei L, Cao S, Yang L. Shorter telomere length of T-cells in peripheral blood of patients with lung cancer. Onco Targets Ther. 2016;9:2675–82.
Luppi F, Kalluri M, Faverio P, Kreuter M, Ferrara G. Idiopathic pulmonary fibrosis beyond the lung: understanding disease mechanisms to improve diagnosis and management. Respir Res. 2021;22:109.
McGroder CF, Zhang D, Choudhury MA, Salvatore MM, D’Souza BM, Hoffman EA, et al. Pulmonary fibrosis 4 months after COVID-19 is associated with severity of illness and blood leucocyte telomere length. Thorax. 2021;76:1242–5.
Martinez P, Sanchez-Vazquez R, Saha A, Rodriguez-Duque MS, Naranjo-Gonzalo S, Osorio-Chavez JS, et al. Short telomeres in alveolar type II cells associate with lung fibrosis in post COVID-19 patients with cancer. Aging (Albany NY). 2023;15:4625–41.
Mulet A, Gonzalez-Cabo P, Pallardo FV, Signes-Costa J. Persistent pulmonary fibrotic sequelae in patients with telomere shortening one year after severe COVID-19. Arch Bronconeumol. 2024;60:62–4.
Acknowledgements
This study would not have been possible without the collaboration of all the patients, their families, medical and nursery staff, and data managers who participated in the project.
Funding
This study was supported by grants from Instituto de Salud Carlos III (ISCIII; grant number COV20/1144 [MPY224/20] to AFR/MAJS) and Fundación Universidad Alfonso X el Sabio (FUAX) – Santander (1.013.005). The study was also supported by CIBER – Consorcio Centro de Investigación Biomédica en Red-(CB 2021), Instituo de Salud Carlos III, Ministerio de Ciencia e Innovación and Unión Europea – NextGenerationEU (CB21/13/00044).
Author information
Authors and Affiliations
Contributions
Funding body: MAJS, AFR and RB. Study concept and design: AFR, MAJS, AVB, OMG and RB. Patients’ selection and clinical data acquisition: AVB, OMG, RB, EM, MJMP, BLM, CMP. Sample preparation and analysis: AVB, SBB, RBL. Statistical analysis and interpretation of data: AVB, SBB, RBL, AFR, and MAJS. Writing of the manuscript: AVB, AFR, and MAJS. Critical revision of the manuscript for relevant intellectual content: SR, RB, OMG. Supervision and visualization: AFR and MAJS. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The study protocol was approved by the Ethics Committee of the Institute of Health Carlos III (PI 33_2020-v3) and the Investigation Committee of both hospitals.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Virseda-Berdices, A., Behar-Lagares, R., Martínez-González, O. et al. Longer ICU stay and invasive mechanical ventilation accelerate telomere shortening in COVID-19 patients 1 year after recovery. Crit Care 28, 267 (2024). https://doi.org/10.1186/s13054-024-05051-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13054-024-05051-6