
Abstract
Background
Extracorporeal cardiopulmonary resuscitation (ECPR) has been proposed as a rescue therapy for patients with refractory cardiac arrest. This study aimed to evaluate the association between ECPR and clinical outcomes among patients with out-of-hospital cardiac arrest (OHCA) using risk-set matching with a time-dependent propensity score.
Methods
This was a secondary analysis of the JAAM-OHCA registry data, a nationwide multicenter prospective study of patients with OHCA, from June 2014 and December 2019, that included adults (≥ 18 years) with OHCA. Initial cardiac rhythm was classified as shockable and non-shockable. Patients who received ECPR were sequentially matched with the control, within the same time (minutes) based on time-dependent propensity scores calculated from potential confounders. The odds ratios with 95% confidence intervals (CI) for 30-day survival and 30-day favorable neurological outcomes were estimated for ECPR cases using a conditional logistic model.
Results
Of 57,754 patients in the JAAM-OHCA registry, we selected 1826 patients with an initial shockable rhythm (treated with ECPR, n = 913 and control, n = 913) and a cohort of 740 patients with an initial non-shockable rhythm (treated with ECPR, n = 370 and control, n = 370). In these matched cohorts, the odds ratio for 30-day survival in the ECPR group was 1.76 [95%CI 1.38–2.25] for shockable rhythm and 5.37 [95%CI 2.53–11.43] for non-shockable rhythm, compared to controls. For favorable neurological outcomes, the odds ratio in the ECPR group was 1.11 [95%CI 0.82–1.49] for shockable rhythm and 4.25 [95%CI 1.43–12.63] for non-shockable rhythm, compared to controls.
Conclusion
ECPR was associated with increased 30-day survival in patients with OHCA with initial shockable and even non-shockable rhythms. Further research is warranted to investigate the reproducibility of the results and who is the best candidate for ECPR.
Graphical Abstract

Similar content being viewed by others


Background
Extracorporeal cardiopulmonary resuscitation (ECPR) is an advanced procedure used in addition to standard resuscitation in patients with refractory out-of-hospital cardiac arrest (OHCA). It involves the implementation of an extracorporeal circuit through emergent percutaneous cannulation of the femoral vein and artery to supply oxygenated blood and remove carbon dioxide from the brain and other vital organs [1, 2]. Currently, three randomized controlled trials (RCTs) and observational studies have been published, and their meta-analysis showed that ECPR potentially improves clinical outcomes of patients with OHCA; however, the effect on clinical outcomes and who is the best candidate of ECPR is still under discussion [3,4,5,6,7,8,9,10,11]. Hence, further investigation is needed to consider the effect of ECPR and who is the best candidate for ECPR.
While further research on the effects of ECPR is indeed necessary, conducting an RCT is challenging due to the practical burdens in clinical settings, costs, and ethical issues [12]. High-quality observational studies are therefore required to compensate for the limitations of conducting RCTs. However, prior observational studies on ECPR have raised concerns about the risk of bias, particularly with regard to the resuscitation time bias [10, 13]. To address this bias, some studies related to resuscitation used sequential risk-set matching with time-dependent propensity scores to evaluate interventions such as advanced airway management and adrenaline administration [14,15,16]. Previously, one study investigated the association between ECPR and outcomes using this time-dependent propensity score; however, this study did not divide the patients based on the initial cardiac rhythm, which is crucial for discussing the effectiveness of ECPR, because the patients with initial non-shockable rhythm have totally different clinical features, such as potential causes, resuscitation algorithm, risk factors, predictors and their outcomes among patients with OHCA treated with ECPR [17,18,19,20,21,22]. However, no studies have evaluated the association between ECPR and clinical outcomes considering these issues. This study aimed to investigate the association between ECPR and clinical outcomes among patients with OHCA using sequential risk-set matching analysis with a time-dependent propensity score to address resuscitation time bias.
Methods
The study protocol and retrospective analysis was approved by the Ethics Committees of Kyoto University (approval ID: R1045), Osaka University (approval ID: 21304), and each participating institution, and the requirement for written informed consent was waived for this observational study.
Data source and management
This study was a retrospective analysis of the JAAM-OHCA registry, a prospective, multicenter, nationwide database established by the steering committee of the Japanese Association of Acute Medicine. Details of the registry have been previously published [23, 24]. This database combines pre-hospital and in-hospital information and outcomes of patients with OHCA transported to the emergency departments of 93 institutions (69 university hospitals and/or tertiary critical care centers). Tertiary critical care centers are certified by the Ministry of Health, Labor, and Welfare in Japan and are required to provide highly specialized treatments such as ECPR, percutaneous coronary intervention, and intensive care 24 h a day. The other 24 hospitals were not critical care centers or university hospitals; they provided emergency medical services to the community. Pre-hospital information based on the standardized Utstein format was collected by paramedics [25] and verified by the Fire and Disaster Management Agency in Japan. In-hospital information, such as treatment in the emergency department and after admission to the ICU, was registered by clinicians or clinical data administrators using an electronic data capture system with a standardized reporting form [23, 24]. The JAAM-OHCA registry committee checked the logic and quality of the data, and anonymized data were provided to the researchers by the committee.
Participants
This study included all consecutive patients with OHCA registered in the JAAM-OHCA registry between June 2014 and December 2019 based on the following inclusion criteria, adult with OHCA aged ≥ 18 years due to medical causes, resuscitation attempted by paramedics at the scene, and cardiac arrest sustained and confirmed upon hospital arrival. The exclusion criteria were opting out of the study, absence of a pre-hospital record, not receiving resuscitation attempts, age less than 18 years, cardiac arrest due to external causes (such as trauma, drowning, and choking), absence of cardiac arrest at the time of initial evaluation by paramedics, and ROSC before/on hospital arrival, which means that we excluded ECMO implementation for cardiogenic shock after ROSC. ROSC was defined as the presence of palpable pulses for more than 30 s [26]. Further, we also excluded those who were transferred to a hospital in which the ECPR cases were not registered in the database because those hospitals were assumed to lack the capacity to provide ECPR, those whose final disposition in the emergency department (ROSC, termination of resuscitation, or ECPR) was missing, and those whose time to final disposition, such as time from hospital arrival to termination of resuscitation, was zero. The study participants were stratified by initial cardiac rhythm into shockable and non-shockable groups as confirmed by paramedics at the scene, as the current international guidelines propose two different algorithms according to the initial rhythm [27, 28]. A shockable rhythm was defined as VF or pulseless ventricular tachycardia, and a non-shockable rhythm was defined as pulseless electrical activity or asystole.
Exposure
ECPR is defined as emergency cannulation and veno-arterial extracorporeal membrane oxygenation for patients with OHCA who sustained cardiac arrest upon arrival at the hospital. The decision to perform ECPR was determined by the individual physicians attending to each patient. Generally, pre-hospital ECPR was not available during the study period in Japan.
Outcome
The primary outcome was 30-day survival. The secondary outcome was 30-day survival with favorable neurological outcomes, defined as Cerebral Performance Category (CPC) 1 or 2. It is commonly used to evaluate the neurological status after OHCA as follows: category 1, good cerebral performance; category 2, moderate cerebral disability; category 3, severe cerebral disability; category 4, coma or vegetative state; and category 5, death/brain death [25]. The CPC was evaluated by clinicians or research assistants in each hospital and registered to the database.
Data measurement, collection, and handling of missing data
The following clinical information was obtained from the database: sex, age, witnessed status, CPR performed by a bystander, pre-hospital initial cardiac rhythm, cardiac rhythm on hospital arrival, resuscitation time course, final disposition in the emergency department (ED), and outcome. Final disposition in the ED is defined as the situation on termination of chest compression which can be classified as ROSC, death (terminate the resuscitation effort), or the start of ECPR. The details of the other variables are provided in the Additional file (Additional file 1: Method S1). Missing data were imputed by a random forest-based imputation procedure using the “missForest” package for eligible study participants [29]. We describe the details of this imputation method in the Additional file (Additional file 1: Method S2).
Statistical analysis
Patient and hospital characteristics
We described the patients’ characteristics and hospital information. Data are shown as median and interquartile range (IQR) for continuous variables and as numbers and percentages for categorical variables. We used standardized mean differences to describe the data in both the original and matched cohorts.
Time-dependent propensity scores and sequential risk-set matching
We performed time-dependent propensity score and risk-set matching analysis in each cohort of the initial cardiac rhythm to evaluate the association between ECPR and outcomes. The details of the time-dependent propensity scores and sequential risk-set matching are explained in the Additional file (Additional file 1: Method 3). To estimate the time-dependent propensity score of receiving ECPR after hospital arrival, we applied the fine-gray regression model in the presence of competing risk with time-dependent covariates [30]. In this model, we dealt with ROSC and death (termination of resuscitation) before ECPR as the competing risk. We also set 120 min after arrival at the hospital as censoring in the model. Time-dependent covariates were defibrillation, intubation, and adrenaline administration in the hospital. The time-independent covariates in the calculation of the propensity score were as follows: patient characteristics (sex and age), pre-hospital information (witness, bystander CPR, initial cardiac rhythm, defibrillation by bystander, physician-staffed ambulance or helicopter, defibrillation by paramedics, type of advanced airway, number of administrations of adrenaline, pre-hospital ROSC, and time from call to hospital), and hospital capability of ECPR. Hospital capability for ECPR was defined as “high,” “middle,” or “low,” according to the tertiles of the number of patients who received ECPR in the last two years. Although we adopted the same variables to calculate the time-dependent propensity score for both shockable and non-shockable cohorts, the scores were calculated separately for each rhythm cohort.
Based on the time-dependent propensity scores, we performed 1:1 sequential matching of the patients who received ECPR at any given minute from minute 0 to minute 120 (patients treated with ECPR) to a patient who was at risk of receiving ECPR within the same minute (control) with replacement. In this sequential matching, at-risk patients (controls) included those who were still undergoing resuscitation at the emergency department and had not received ECPR before or within the same minute. Matching with replacements of unexposed patients meant that matched controls with no ECPR at each time were allowed to match again later until they received ECPR. Therefore, at-risk patients also included those who received ECPR later, as matching was not dependent on future events. In sequential matching, we set the caliper width for nearest-neighbor matching at 0.2 standard deviations of the propensity score, as recommended in previous literature [31]. We calculated standardized differences to evaluate the balance of variables in each propensity score-matched cohort. We considered a standardized mean difference of < 0.25, as suggested in the literature [31].
Estimation of association between ECPR and outcomes
To evaluate the association between ECPR and each outcome, we fitted a conditional logistic regression model to estimate odds ratios (ORs) with 95% confidence intervals (CIs) to compare to those at risk of receiving ECPR (control). All tests were two-sided; we regarded p < 0.05 as statistically significant. Data analysis was conducted from March 2022 to July 2022. All statistical analyses were performed using R software, version 4.1.2 (R Foundation for Statistical Computing).
Results
Study flowchart and original cohort
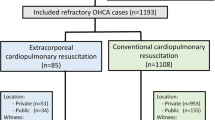
Of the 57,754 patients registered in the JAAM-OHCA registry, 3,050 patients with OHCA with initial shockable rhythm (942 patients treated with ECPR and 2,108 cases without ECPR) and 30,231 patients with OHCA with initial non-shockable rhythm (376 cases treated with ECPR and 29,855 cases without ECPR) were included in the analysis (Fig. 1). Details of the missing variables are described in the Additional file (Additional file 1: Table S1). The characteristics before matching are described in Table 1 and the Additional file (Additional file 1: Table S2).

Study flowchart. ECPR, Extracorporeal cardiopulmonary resuscitation, ROSC, Return of spontaneous circulation
Matched cohort
Through matching using a time-dependent propensity score, 1,826 initially shockable cases (913 cases treated with ECPR and 913 controls) and 740 initially non-shockable cases (370 cases treated with ECPR and 370 controls) were included in the primary analysis. In the matched cohort with initial shockable rhythm, ECPR versus control, median (IQR) ages were 59 [48–68] and 59 [48–70] years and males were 86% (784/913) and 85% (778/913), respectively. In the non-shockable matched cohort, ECPR versus control, median (IQR) ages were 60 [47–69] and 58 [45–69] years and males were 77% (284/370) and 75% (278/370), respectively. In the ECPR group, the median (IQR) time to ECPR initiation was 25 [6, 18] minutes in patients with initial shockable rhythm and 28 [3, 20] minutes in patients with initial non-shockable rhythm. Among the control groups, ECPR was performed in 389 (43%) and 60 (16%) patients in the initial shockable and non-shockable groups, respectively. Additional details of the characteristics are described in Table 2 and the Additional file (Additional file 1: Tables S3-S5). Overall, patient characteristics were well-balanced.
Outcomes in the initially shockable rhythm matched cohort
The 30-day survival rate in the cohort with initial shockable rhythm was 24.6% (225/913) in the ECPR group and 16.3% (149/913) in the control group (Fig. 2). The OR by the conditional logistic regression model for 30-day survival with ECPR was 1.76 [95%CI 1.38–2.25] compared with the control. However, in the matched cohort with initial shockable rhythm, 30-day favorable neurological outcomes accounted for 11.9% (109/913) in the ECPR group and 11.0% (100/913) in the control group. The OR for 30-day favorable neurological outcome was 1.11 [95%CI 0.82–1.49] for ECPR compared with the control (Fig. 2).

Main results of the matched cohorts. ECPR, Extracorporeal cardiopulmonary resuscitation, Survival, 30-day survival, Good Neuro, 30-day good neurological outcome. Left: Percentage of 30-day survival and good neurological outcome in the matched cohorts (initial shockable and initial non-shockable rhythm). Right: Odds ratio of the ECPR group for 30-day survival and good neurological outcome in the matched cohorts (initial shockable and initial non-shockable rhythm)
Outcomes in the initially non-shockable rhythm matched cohort
The 30-day survival rate in the matched cohort with initial non-shockable rhythm was 11.9% (44/370) for the ECPR group and 2.4% (9/370) for controls. The OR for 30-day survival was 5.37 [95%CI 2.53–11.43] for ECPR compared with the control (Fig. 2). The 30-day favorable neurological outcomes in the matched cohort with initial non-shockable rhythm accounted for 4.6% (17/370) in the ECPR group and 1.1% (4/370) in the control group. The OR for 30-day favorable neurological outcome was 4.25 [95%CI 1.43–12.63] for ECPR compared with the control (Fig. 2).
Discussion
Key observations and strengths
This observational study using risk-set matching by time-dependent propensity score indicated that ECPR was associated with higher survival rates among adult patients with OHCA with both initial shockable and non-shockable rhythms. Furthermore, ECPR was associated with favorable neurological outcomes in patients with OHCA with non-shockable rhythm. Although some previous observational studies investigated the association between ECPR and clinical outcomes, they did not adequately address resuscitation time bias and time-dependent confounding [10]. The strength of this study is to show the association between ECPR and outcomes using the robust methodology to address resuscitation time bias among patients with OHCA with and without initial shockable rhythm.
Interpretation and clinical implications
ECPR was associated with improved survival and favorable neurological outcomes among patients with OHCA with an initial non-shockable rhythm. The potential mechanism explaining this finding may be that ECPR allows time to address the treatable causes of non-shockable rhythms, such as dialysis for hyperkalemia or anticoagulation therapy for pulmonary embolization, which may improve outcomes in selected patients with OHCA with initial non-shockable rhythms [19]. Accordingly, the appropriate selection of ECPR candidates can lead to better outcomes even the patients with OHCA initially had non-shockable rhythms.
In contrast, although patients with OHCA with shockable rhythm are recognized as the target population for ECPR, this study indicated that ECPR was not associated with favorable neurological outcomes among patients with OHCA with an initial shockable rhythm. We guess the reason that ECPR was administered to some of these patients even if their brains had already been hypoxically injured. These patients may have had better survival with ECPR but not improved neurological outcomes. In Japan, ECPR is commonly implemented according to the criteria suggested by the SAVE-J study; [7] however, the final decision of using ECPR is made by the physician in charge of the patient, and the indications for ECPR vary between institutions [32]. This study included patients from a wide range of institutions and time periods, including cases where the time from call to hospital arrival was longer than 40 min or the time from hospital arrival to start of ECPR was more than 60 min. Worse neurological outcomes have been reported with longer durations to ECPR initiation [21]. We opine that some of the patients received ECPR after the “golden period”; hence, the effect of ECPR might has been diluted. The RCT recently published investigating the effect of ECPR among patients with OHCA with an initial shockable rhythm also did not show the favorable effect of ECPR on the neurological outcome, and in this trial, the duration between the emergency call and the start of ECPR in most cases was more than 60 min (median 74 [IQR: 63–87] minutes) [5]. We did not analyze the time to hospital or time to start ECPR because of the limited sample size; however, future studies should investigate the heterogeneity of the effect of ECPR based on the time to determine the optimal timing for ECPR.
However, we believe that it is not appropriate to conclude that ECPR is not suitable for patients with OHCA with an initial shockable rhythm based on our results that ECPR was not associated with good neurological outcomes. A previous RCT (the ARREST trial) and meta-analysis of some RCTs had already indicated a favorable effect of ECPR on neurological outcomes of selected OHCA patients with initial shockable rhythm [3, 6, 33]. Rather, the results in this study suggested that all the patients with OHCA with an initially shockable rhythm treated with ECPR in this database may not be the best target population for ECPR in terms of neurological outcomes and it might be better to reconsider the current criteria among the institutions included in this database. We previously developed a clinical score for predicting the probability of favorable outcomes among patients with OHCA with a shockable rhythm treated with ECPR [34, 35] based on the following criteria: age less than 65 years, shockable rhythm at hospital arrival, time from call to hospital shorter than 25 min, and pH higher than 7.0 in the initial blood gas assessment. If the score is more than three, the probability of a favorable neurological outcome is predicted as approximately 20–30%. Therefore, ECPR may be more effective in the selected population. Here, we were unable to perform a subgroup analysis to investigate the population that may benefit from ECPR because risk-set matching would have been disturbed if the study population was divided by these factors. However, further observational research is needed to suggest the appropriate patients with OHCA for ECPR to inform further RCTs.
Limitations
This study has some limitations: first, it has a potential risk of selection bias. The indication to perform ECPR was decided not based on unified criteria but on each clinician’s judgment. Most patients in this study were reasonable candidates for ECPR based on their characteristics; however, imperfect inclusion criteria may lead to concerns about generalizability. The estimated association was the average treatment effect on the treatment group, and the results may be influenced by patient selection. Second, the JAAM-OHCA database did not include complete clinical details, such as the clinical course after admission or details of the ECPR procedures. Third, although we addressed potential confounding factors, there may be a risk of unmeasured confounding factors, such as patients’ comorbidities or the quality of care in each facility. Fourth, since the control group was a combination of patients who never had undergone ECPR or who had ECPR performed later than the ECPR group, the effect estimate would more likely be closer to null (dilution of the effect) compared to that of a randomized trial that would strictly compare ECPR treatment policy to no ECPR. This corresponds to an intention-to-treat analysis with several protocol deviations that patients end up having ECPR later in the “no ECPR” group. In the initial shockable group, the magnitude of this dilution effect might be larger because the proportion of patients who underwent ECPR later in the control group was high (43%). Furthermore, favorable neurological outcomes in the control group were relatively high (11%) compared to those in a previous study in Japan (SAVE-J study), where it was approximately 2% among patients with OHCA who had an initial shockable rhythm, did not obtain ROSC, and ECPR was not performed [36]. Dilution of effect might be caused by sequential matching. Fifth, although evaluating CPC was reported to have substantial inter-rater reliability, there might be a risk of bias of misclassification in outcome assessment [4]. Sixth, we set survival as the primary outcome of this study, when planning our analysis, we observed that several pivotal studies on ECPR mainly considered survival as their primary outcome [3, 37]. Nonetheless, from a patient’s perspective, neurological outcomes hold greater significance. Therefore, we recommend a cautious interpretation and application of our findings. Seventh, this study was not conducted based on the pre-registered analysis plan or protocol; thus, this study may be assessed as having some risk of bias, especially in the domain of selection of the reported results [38]. Finally, although this study included study participants from nationwide data in Japan, there are some concerns about generalizability to other settings such as countries that have different emergency medical systems. The reproducibility of the results should be confirmed in other settings to address these issues.
Conclusion
Although there are several limitations, this observational study using risk-set matching by time-dependent propensity score suggested that ECPR was associated with a higher 30-day survival among patients with OHCA with both initial shockable and even non-shockable rhythms. Furthermore, this study indicated ECPR was also associated with favorable neurological outcomes among patients with OHCA with initial non-shockable rhythms; however, not among patients with OHCA with initial shockable. Further research is warranted to investigate the reproducibility of the results and who is the best candidate for ECPR.
Availability of data and materials
The datasets and/or analyses in this study are not publicly available because the ethics committee did not permit them.
Abbreviations
- ECPR:
-
Extracorporeal cardiopulmonary resuscitation
- OHCA:
-
Out-of-hospital cardiac arrest
- RCTs:
-
Randomized controlled trials
- VF:
-
Ventricular fibrillation
- ROSC:
-
Return of spontaneous circulation
- CPC:
-
Cerebral Performance Category
- IQR:
-
Interquartile range
- ORs:
-
Odds ratios
- CIs:
-
Confidence intervals
References
Inoue A, Hifumi T, Sakamoto T, Kuroda Y. Extracorporeal cardiopulmonary resuscitation for out-of-hospital cardiac arrest in adult patients. J Am Heart Assoc. 2020;9: e015291. https://doi.org/10.1161/JAHA.119.015291.
Abrams D, MacLaren G, Lorusso R, Price S, Yannopoulos D, Vercaemst L, et al. Extracorporeal cardiopulmonary resuscitation in adults: evidence and implications. Intensive Care Med. 2022;48:1–15. https://doi.org/10.1007/s00134-021-06514-y.
Yannopoulos D, Bartos J, Raveendran G, Walser E, Connett J, Murray TA, et al. Advanced reperfusion strategies for patients with out-of-hospital cardiac arrest and refractory ventricular fibrillation (ARREST): a phase 2, single centre, open-label, randomised controlled trial. Lancet. 2020;396:1807–16. https://doi.org/10.1016/S0140-6736(20)32338-2.
Belohlavek J, Smalcova J, Rob D, Franek O, Smid O, Pokorna M, et al. Effect of intra-arrest transport, extracorporeal cardiopulmonary resuscitation, and immediate invasive assessment and treatment on functional neurologic outcome in refractory out-of-hospital cardiac arrest: a randomized clinical trial. JAMA. 2022;327:737–47. https://doi.org/10.1001/jama.2022.1025.
Suverein MM, Delnoij TSR, Lorusso R, Brandon Bravo Bruinsma GJ, Otterspoor L, Elzo Kraemer CV, Vlaar APJ, van der Heijden JJ, Scholten E, den Uil C, Jansen T, van den Bogaard B, Kuijpers M, Lam KY, Montero Cabezas JM, Driessen AHG, Rittersma SZH, Heijnen BG, Dos Reis MD, Bleeker G, de Metz J, Hermanides RS, Lopez Matta J, Eberl S, Donker DW, van Thiel RJ, Akin S, van Meer O, Henriques J, Bokhoven KC, Mandigers L, Bunge JJH, Bol ME, Winkens B, Essers B, Weerwind PW, Maessen JG, van de Poll MCG. Early extracorporeal CPR for refractory out-of-hospital cardiac arrest. N Engl J Med. 2023;388:299–309.
Scquizzato T, Bonaccorso A, Swol J, Gamberini L, Scandroglio AM, Landoni G, et al. Refractory out-of-hospital cardiac arrest and extracorporeal cardiopulmonary resuscitation: a meta-analysis of randomized trials. Artif Organs. 2023;47:806–16. https://doi.org/10.1111/aor.14516.
Sakamoto T, Asai Y, Nagao K, Yokota H, Morimura N, Tahara Y, et al., group S-Js. Multicenter non-randomized prospective cohort study of extracorporeal cardiopulmonary resuscitation for out-of hospital cardiac arrest: study of advanced life support for ventricular fibrillation with extracorporeal circulation in Japan (SAVE-J). In: Book Multicenter non-randomized prospective cohort study of extracorporeal cardiopulmonary resuscitation for out-of hospital cardiac arrest: study of Advanced Life Support for Ventricular Fibrillation with Extracorporeal Circulation in Japan (SAVE-J). Am. Heart Association; 2011
Nakashima T, Noguchi T, Tahara Y, Nishimura K, Ogata S, Yasuda S, et al. Patients with refractory out-of-cardiac arrest and sustained ventricular fibrillation as candidates for extracorporeal cardiopulmonary resuscitation- prospective multi-center observational study. Circ J. 2019;83:1011–8. https://doi.org/10.1253/circj.CJ-18-1257.
Miraglia D, Miguel LA, Alonso W. Extracorporeal cardiopulmonary resuscitation for in- and out-of-hospital cardiac arrest: systematic review and meta-analysis of propensity score-matched cohort studies. J Am Coll Emerg Physicians Open. 2020;1:342–61. https://doi.org/10.1002/emp2.12091.
Holmberg MJ, Geri G, Wiberg S, Guerguerian AM, Donnino MW, Nolan JP, et al. Extracorporeal cardiopulmonary resuscitation for cardiac arrest: A systematic review. Resuscitation. 2018;131:91–100. https://doi.org/10.1016/j.resuscitation.2018.07.029.
Choi Y, Park JH, Jeong J, Kim YJ, Song KJ, Shin SD. Extracorporeal cardiopulmonary resuscitation for adult out-of-hospital cardiac arrest patients: time-dependent propensity score-sequential matching analysis from a nationwide population-based registry. Crit Care. 2023;27:87. https://doi.org/10.1186/s13054-023-04384-y.
Tonna JE, Keenan HT, Weir C. A qualitative analysis of physician decision making in the use of extracorporeal cardiopulmonary resuscitation for refractory cardiac arrest. Resusc Plus. 2022;11: 100278. https://doi.org/10.1016/j.resplu.2022.100278.
Andersen LW, Grossestreuer AV, Donnino MW. "Resuscitation time bias”-A unique challenge for observational cardiac arrest research. Resuscitation. 2018;125:79–82. https://doi.org/10.1016/j.resuscitation.2018.02.006.
Izawa J, Komukai S, Gibo K, Okubo M, Kiyohara K, Nishiyama C, et al. Pre-hospital advanced airway management for adults with out-of-hospital cardiac arrest: nationwide cohort study. BMJ. 2019;364: l430. https://doi.org/10.1136/bmj.l430.
Okubo M, Komukai S, Callaway CW, Izawa J. Association of timing of epinephrine administration with outcomes in adults with out-of-hospital cardiac arrest. JAMA Netw Open. 2021;4: e2120176. https://doi.org/10.1001/jamanetworkopen.2021.20176.
Andersen LW, Granfeldt A, Callaway CW, Bradley SM, Soar J, Nolan JP, et al. Association between tracheal intubation during adult in-hospital cardiac arrest and survival. JAMA. 2017;317:494–506. https://doi.org/10.1001/jama.2016.20165.
Okada Y, Irisawa T, Yamada T, Yoshiya K, Park C, Nishimura T, et al. Clinical outcomes among out-of-hospital cardiac arrest patients treated by extracorporeal cardiopulmonary resuscitation: the CRITICAL study in OsakaResuscitation. ©2022 Elsevier BV. Ireland; 2022
Okada A, Okada Y, Kandori K, Nakajima S, Matsuyama T, Kitamura T, et al. Application of the TiPS65 score for out-of-hospital cardiac arrest patients with initial non-shockable rhythm treated with ECPR. Resusc Plus. 2023;16: 100458. https://doi.org/10.1016/j.resplu.2023.100458.
Hyman MC, Deo R. Post-cardiac arrest evaluation: understanding non-shockable rhythms. Eur Heart J. 2019;40:3835–7. https://doi.org/10.1093/eurheartj/ehz504.
Kandori K, Okada Y, Okada A, Nakajima S, Okada N, Matsuyama T, et al. Association between cardiac rhythm conversion and neurological outcome among cardiac arrest patients with initial shockable rhythm: a nationwide prospective study in Japan. Eur Heart J Acute Cardiovasc Care. 2021;10:119–26. https://doi.org/10.1093/ehjacc/zuaa018.
Matsuyama T, Irisawa T, Yamada T, Hayakawa K, Yoshiya K, Noguchi K, et al. Impact of low-flow duration on favorable neurological outcomes of extracorporeal cardiopulmonary resuscitation after out-of-hospital cardiac arrest: a multicenter prospective study. Circulation. 2020;141:1031–3. https://doi.org/10.1161/CIRCULATIONAHA.119.044285.
Pabst D, Brehm CE. Is pulseless electrical activity a reason to refuse cardiopulmonary resuscitation with ECMO support? Am J Emerg Med. 2018;36:637–40. https://doi.org/10.1016/j.ajem.2017.09.057.
Kitamura T, Iwami T, Atsumi T, Endo T, Kanna T, Kuroda Y, et al. The profile of Japanese Association for Acute Medicine—out-of-hospital cardiac arrest registry in 2014–2015. Acute Med Surg. 2018;5:249–58. https://doi.org/10.1002/ams2.340.
Irisawa T, Matsuyama T, Iwami T, Yamada T, Hayakawa K, Yoshiya K, et al. The effect of different target temperatures in targeted temperature management on neurologically favorable outcome after out-of-hospital cardiac arrest: a nationwide multicenter observational study in Japan (the JAAM-OHCA registry) Resuscitation. 2018. Ireland: Elsevier BV, p. 82–7; 2018
Cummins RO, Chamberlain DA, Abramson NS, Allen M, Baskett PJ, Becker L, et al. Recommended guidelines for uniform reporting of data from out-of-hospital cardiac arrest: the Utstein Style. A statement for health professionals from a task force of the American Heart Association, the European Resuscitation Council, the Heart and Stroke Foundation of Canada, and the Australian Resuscitation Council. Circulation. 1991;84:960–75. https://doi.org/10.1161/01.cir.84.2.960
Jacobs I, Nadkarni V, Bahr J, Berg RA, Billi JE, Bossaert L, et al. Cardiac arrest and cardiopulmonary resuscitation outcome reports: update and simplification of the Utstein templates for resuscitation registries: a statement for healthcare professionals from a task force of the International Liaison Committee on Resuscitation (American Heart Association, European Resuscitation Council, Australian Resuscitation Council, New Zealand Resuscitation Council, Heart and Stroke Foundation of Canada, InterAmerican Heart Foundation, Resuscitation Councils of Southern Africa). Circulation. 2004;110:3385–97. https://doi.org/10.1161/01.CIR.0000147236.85306.15.
Perkins GD, Graesner JT, Semeraro F, Olasveengen T, Soar J, Lott C, et al. European Resuscitation Council Guidelines 2021: executive summary. Resuscitation. 2021;161:1–60. https://doi.org/10.1016/j.resuscitation.2021.02.003.
Panchal AR, Bartos JA, Cabañas JG, Donnino MW, Drennan IR, Hirsch KG, et al. Part 3: adult basic and advanced life support: 2020 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2020;142:S366–468. https://doi.org/10.1161/CIR.0000000000000916.
Stekhoven DJ, Bühlmann P. MissForest—non-parametric missing value imputation for mixed-type data. Bioinformatics. 2012;28:112–8. https://doi.org/10.1093/bioinformatics/btr597.
Beyersmann J, Schumacher M. Time-dependent covariates in the proportional subdistribution hazards model for competing risks. Biostatistics. 2008;9:765–76. https://doi.org/10.1093/biostatistics/kxn009.
Stuart EA. Matching methods for causal inference: a review and a look forward. Stat Sci. 2010;25:1–21. https://doi.org/10.1214/09-STS313.
Hifumi T, Inoue A, Takiguchi T, Watanabe K, Ogura T, Okazaki T, et al. Variability of extracorporeal cardiopulmonary resuscitation practice in patients with out-of-hospital cardiac arrest from the emergency department to intensive care unit in Japan. Acute Med Surg. 2021;8: e647. https://doi.org/10.1002/ams2.647.
Low CJW, Ramanathan K, Ling RR, Ho MJC, Chen Y, Lorusso R, et al. Extracorporeal cardiopulmonary resuscitation versus conventional cardiopulmonary resuscitation in adults with cardiac arrest: a comparative meta-analysis and trial sequential analysis. Lancet Respir Med. 2023;11:883–93. https://doi.org/10.1016/S2213-2600(23)00137-6.
Okada Y, Kiguchi T, Irisawa T, Yamada T, Yoshiya K, Park C, et al. Development and validation of a clinical score to predict neurological outcomes in patients with out-of-hospital cardiac arrest treated with extracorporeal cardiopulmonary resuscitation. JAMA Netw Open. 2020;3: e2022920. https://doi.org/10.1001/jamanetworkopen.2020.22920.
Makino Y, Okada Y, Irisawa T, Yamada T, Yoshiya K, Park C, et al. External validation of the TiPS65 score for predicting good neurological outcomes in patients with out-of-hospital cardiac arrest treated with extracorporeal cardiopulmonary resuscitation. Resuscitation. 2023;182: 109652. https://doi.org/10.1016/j.resuscitation.2022.11.018.
Sakamoto T, Morimura N, Nagao K, Asai Y, Yokota H, Nara S, et al. Extracorporeal cardiopulmonary resuscitation versus conventional cardiopulmonary resuscitation in adults with out-of-hospital cardiac arrest: a prospective observational study. Resuscitation. 2014;85:762–8. https://doi.org/10.1016/j.resuscitation.2014.01.031.
Bougouin W, Dumas F, Lamhaut L, Marijon E, Carli P, Combes A, et al. Extracorporeal cardiopulmonary resuscitation in out-of-hospital cardiac arrest: a registry study. Eur Heart J. 2020;41:1961–71. https://doi.org/10.1093/eurheartj/ehz753.
Sterne JA, Hernán MA, Reeves BC, Savović J, Berkman ND, Viswanathan M, et al. Robins-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ. 2016;355: i4919. https://doi.org/10.1136/bmj.i4919.
Acknowledgements
We are deeply grateful to all EMS personnel for collecting the Utstein data and to Ms. Ikuko Nakamura and Yumiko Murai for supporting this study. YO appreciates the ZOLL Foundation and an overseas scholarship from the FUKUDA Foundation for Medical Technology and the International Medical Research Foundation for their support.
Funding
This study was supported by a scientific research Grant from JSPS KAKENHI of Japan (JP22K21143 to YO, JP22H03313 to TI, and JP22K09139 to TK), a research Grant from the ZOLL Foundation, and the Advanced Clinical Epidemiology Investigator’s Research Project at Osaka University Graduate School of Medicine.
Author information
Authors and Affiliations
Contributions
Conception and design of the work were done by YO, SK, and TK. Data acquisition was done by TI, TY, KY, CP, TN, TI HK, TK, MK, SK, YI, TS, TM, HS, KS, AO, TM, NN, SM SY, SK, SK, YM KK, and LZ. Analysis was done by YO and SK. Draft was written by YO. Review and revision of the draft were done by SK, MO, TI, and TK. All authors have approved the final manuscript and have agreed both to be personally accountable for the author’s own contributions and to ensure that questions related to the accuracy or integrity of any part of the work, even ones in which the author was not personally involved, are appropriately investigated, resolved, and the resolution documented in the literature.
Corresponding author
Ethics declarations
Ethical approval and consent to participate
This study was conducted in accordance with the Declaration of Helsinki. The Ethics Committees of Kyoto University (Approval ID: R1045), Osaka University (Approval ID: 21304), and each participating institution approved this study protocol and retrospective analysis, and the need for written informed consent was waived.
Consent for publication
Not applicable.
Competing interests
YO received a research grant from the ZOLL Foundation and an overseas scholarship from the FUKUDA Foundation for Medical Technology and the International Medical Research Foundation. These organizations have no role in the conceptualization, data curation, analysis, and interpretation of this research.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1:
Supplemental Methods 1–3. Tables S1–S5.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Okada, Y., Komukai, S., Irisawa, T. et al. In-hospital extracorporeal cardiopulmonary resuscitation for patients with out-of-hospital cardiac arrest: an analysis by time-dependent propensity score matching using a nationwide database in Japan. Crit Care 27, 442 (2023). https://doi.org/10.1186/s13054-023-04732-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13054-023-04732-y