
Abstract
Background
A quantitative assessment of pulmonary edema is important because the clinical severity can range from mild impairment to life threatening. A quantitative surrogate measure, although invasive, for pulmonary edema is the extravascular lung water index (EVLWI) extracted from the transpulmonary thermodilution (TPTD). Severity of edema from chest X-rays, to date is based on the subjective classification of radiologists. In this work, we use machine learning to quantitatively predict the severity of pulmonary edema from chest radiography.
Methods
We retrospectively included 471 X-rays from 431 patients who underwent chest radiography and TPTD measurement within 24 h at our intensive care unit. The EVLWI extracted from the TPTD was used as a quantitative measure for pulmonary edema. We used a deep learning approach and binned the data into two, three, four and five classes increasing the resolution of the EVLWI prediction from the X-rays.
Results
The accuracy, area under the receiver operating characteristic curve (AUROC) and Mathews correlation coefficient (MCC) in the binary classification models (EVLWI < 15, ≥ 15) were 0.93 (accuracy), 0.98 (AUROC) and 0.86(MCC). In the three multiclass models, the accuracy ranged between 0.90 and 0.95, the AUROC between 0.97 and 0.99 and the MCC between 0.86 and 0.92.
Conclusion
Deep learning can quantify pulmonary edema as measured by EVLWI with high accuracy.
Similar content being viewed by others


Introduction
Pulmonary edema is one of the most common findings in chest radiographs [1] and has important clinical consequences. By impeding the gas exchange and reducing lung compliance, severe pulmonary edema is potentially life threatening [2]. Measuring and monitoring pulmonary edema is useful in many, but especially important in critically ill patients.
Technically, the attenuation of X-rays should be proportional to the amount of lung water, and thus, a chest radiograph should be a valuable tool in monitoring the amount of pulmonary edema. Commonly, radiologists rate the severity on a categorical scale. A quantitative measure for pulmonary edema widely used for critically ill patients is the extravascular lung water (EVLW) which is defined as the amount of water accumulating in the lungs outside of the pulmonary vasculature [2]. Measurement of EVLW by transpulmonary thermodilution (TPTD), although invasive, shows good correlation with the gold standard ex vivo method of gravimetry [3]. However, mixed results have been reported in the literature with the grade of correlation of clinicians’ chest X-ray reports or clinicians’ scores to extravascular lung water (EVLW), ranging from good [4, 5] over modest [6, 7] to poor [8, 9].
Recently Horng et al. used a radiologist-based categorical four grade severity score to train a deep learning classification system on chest radiographs and report a high performance [10]. To our knowledge, our present study is the first to explore the usefulness of deep learning in predicting the quantitative pulmonary edema measure EVLW from chest radiographs.
Acquisition of the chest radiographs and classification
A total of 471 images from 431 patients were acquired between 06/2014 and 09/2022 on two Carestream Health DRX-Revolution X-ray machines (120 kV, 0.6 mAs). The images were extracted in the jpg format. We used the 374 images acquired between 06/2014 and 12/2020 as the training set and 97 images from 01/2021 to 09/2022 for the test set with no patient overlap. We included patients who underwent chest radiography and a TPTD measurement within a maximum of 24 h. TPTD measurement was performed as previously reported [11, 12] and the extravascular lung water was indexed as previously reported (EVLWI, [6]).
Deep learning model
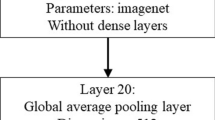
We developed a convolutional neural network for the image classification task. For preprocessing, all images were resized to 300 × 300 pixels and the pixel values were normalized. Data were augmented using cutmix [13]. A transfer learning approach with an EfficientNet B5 backbone [14] with pretrained weights on ImageNet was used. Fine-tuning of the last feature layer was implemented in FastAI [15] using the Adam optimizer and the cross-entropy loss function. Training and testing were performed on a Nvidia Tesla K80 or T4. A result between 0 to 0.5 and 0.5 to 1 was used for the binary classification of each image. We report the accuracy, micro-averaged area under the receiver operator curve in “one vs rest” (AUROC) with confidence Interval (CI) and the Mathews correlation coefficient (MCC) as outcome measures [16].
Patient characteristics
The patients mean age was 64.1 years, ranging from 23 to 92 years. There were slightly less females than males (37.4%). The patients stayed from 1 to 103 days on the intensive care unit (ICU), and the average time on ICU was 21.3 days. The mean EVLWI was 14.9 ranging from 5 to 42.
Results
For the split of the test set with an EVLWI smaller than 15 and larger or equal to 15 the model reached an accuracy of 0.93, the AUROC was 0.98 (CI: [0.98, 1.00]) and an MCC of 0.86 (Fig. 1a). For the three class model we split the data into bins with an EVLWI from 5 to 11 (interval notation: [5, 12[), from 12 to 19 ([12, 20[) and from 20 to 42 ([20, 42]). The corresponding accuracy on the test set was 0.95 (Fig. 1b), the AUROC 0.99 (CI: [0.92;0.99]) and MCC was 0.92. For the four-class model we choose to split the data randomly into the following bins: [5, 8[, [9, 13[, [13, 22[, [22, 44]. The trained model reached an accuracy of ACC 0.90 (CI: [0.89; 0.97]), an AUROC of 0.99 and an MCC of 0.86 (Fig. 1c). We next split the data into five classes in the following manner: EVLWI [5, 8[, [8, 12[, [12, 16[, [16, 20[, [20,44]. The accuracy by the model was 0.90, the AUROC 0.97 (CI: [0.94; 0.98]) and the MCC was 0.87 (Fig. 1d). Splitting into six or more classes resulted in comparably diminished performance (data not shown), most likely due to the lack of training data (On average 63 images in 6 bins).

Precise prediction in the test set split into two, three, four or five classes. a EVLWI 0: < 15, 1: ≥ 15; ACC 0.93, AUROC 0.98, MCC 0.86; b EVLWI 0:[5, 12[, 1:[12, 20[, 2:[20, 44]; ACC 0.95, MCC 0.92, c EVLWI 0:[5, 8[, 1:[9, 13[, 2:[13, 22[, 3:[22, 44]; ACC 0.90, MCC 0.86; d EVLWI 0:[5, 8[, 1:[8, 12[, 2:[12, 16[, 3:[16, 20[,4:[20,44]; ACC 0.90; MCC 0.87
Discussion
In this study, we sequentially developed a deep learning model that accurately quantifies pulmonary edema from chest X-ray images. We use the EVLWI measured invasively by TPTD [2] as ground truth. Our models show very good to excellent performances when binning the available data up to five classes for the clinically most relevant EVLWI range from 6 to 20.
Deep learning has been used in the literature to classify various pathologies from chest radiographs. For example, Majkowska et al. use a machine learning approach to automatically detect four abnormal findings in X-ray images [17]. For the detection of airspace opacity, which includes pulmonary edema, an AUROC of 0.91 to 0.94 is reported. Jarrel et al. use a deep learning approach to diagnose the presence of absence of congestive heart failure (CHF) from chest X-rays. The authors use a cutoff of 100 ng/L BNP as a marker for CHF and find an AUROC of 0.82 [18]. Horng et al. not only diagnose the presence but also quantify lung edema with deep learning [10]. However, the authors use radiology reports as ground truth to categorize training/test data into 4 classes ranging from “0: no edema” to “3: alveolar edema” and an AUC of 0.88 in 2vs0 and only 0.69 in 2vs1.
We see our study as an expansion of these previous works. In our opinion, there are several strong points in our approach. Pulmonary edema presents as a continuous value. We could further increase the resolution of the classification in a clinically relevant range in comparison to Horng et al.’s.
More importantly, our study uses invasively measured EVLWI values as the ground truth instead of subjectively classified radiological estimations of pulmonary edema. While there generally is a good correlation between the gold standard of gravimetry and EVLWI [3] for measuring extravascular lung water, there are mixed results in the literature for correlating classical qualitative or semi-quantitative radiological scores and EVLWI. Chrysopoulo et al. find a good correlation between a 5 scale severity score and EVLW [19]. Brown et al. report a modest positive correlation of clinician-based chest X-ray severity score and EVLW [9]. Halperin et al. describe a modest to poor correlation between a clinical edema score and an EVLW measurement [7].
There are also strong points from a conceptual view. While measuring lung water by TPTD needs a dedicated catheter and equipment, our method uses chest X-rays, which is a widely available tool. On the one hand, this could allow using EVLWI guided fluid therapy on intensive care units where TPTD is not available. On the other hand, this approach could enable access to EVLWI surrogate measurement for a much larger patient cohort. One could speculate for example guiding the diuretics dose by EVLWI in patients with heart failure.
There are limitations to our study too. While Jarrel et al. use 103,489 and Horng et al. 369,071 X-rays to test and train their models we could only use 471 images. This is due to the fact, that thermodilution is an invasive modality, feasible almost only in intensive care units. Furthermore, we tested our model only on a single institution’s critically ill patients. Thus, our results need external confirmation, despite promising results of the above-mentioned studies and the prediction of semi-quantitative scores. Finally, only imaging data acquired on our in-house portable X-ray systems was used in this study. Therefore, model generalization may require not only external imaging data but also additional training with imaging data acquired on standard up right X-ray systems.
Despite these limitations our study demonstrates, that deep learning is a useful tool for the quantification of pulmonary edema with a meaningful resolution with high accuracy.
Availability of data and materials
Dataset is private and is available upon request.
References
Barile M. Pulmonary edema: a pictorial review of imaging manifestations and current understanding of mechanisms of disease (2352-0477 (Print)).
Jozwiak M, Teboul J-L, Monnet X. Extravascular lung water in critical care: recent advances and clinical applications. Ann Intensive Care. 2015;5(1):38.
Tagami T, Kushimoto S, Yamamoto Y, Atsumi T, Tosa R, Matsuda K, et al. Validation of extravascular lung water measurement by single transpulmonary thermodilution: human autopsy study. Critical Care (London, England). 2010;14(5):R162.
Sibbald WJ, Warshawski FJ, Short AK, Harris J, Lefcoe MS, Holliday RL. Clinical studies of measuring extravascular lung water by the thermal dye technique in critically ill patients. Chest. 1983;83(5):725–31.
Pistolesi M, Giuntini C. Assessment of extravascular lung water. Radiol Clin N Am. 1978;16(3):551–74.
Brown LM, Calfee CS, Howard JP, Craig TR, Matthay MA, McAuley DF. Comparison of thermodilution measured extravascular lung water with chest radiographic assessment of pulmonary oedema in patients with acute lung injury. Ann Intensive Care. 2013;3(1):25.
Halperin BD, Feeley TW, Mihm FG, Chiles C, Guthaner DF, Blank NE. Evaluation of the portable chest roentgenogram for quantitating extravascular lung water in critically ill adults. Chest. 1985;88(5):649–52.
Lemson J, van Die LE, Hemelaar AEA, van der Hoeven JG. Extravascular lung water index measurement in critically ill children does not correlate with a chest x-ray score of pulmonary edema. Crit Care. 2010;14(3):R105.
Hammon M, Dankerl P, Voit-Höhne HL, Sandmair M, Kammerer FJ, Uder M, et al. Improving diagnostic accuracy in assessing pulmonary edema on bedside chest radiographs using a standardized scoring approach (1471-2253 (Print)).
Horng S, Liao R, Wang X, Dalal S, Golland P, Berkowitz SJ. Deep learning to quantify pulmonary edema in chest radiographs. Radiol Artif Intell. 2021;3(2):e190228.
Huber W, Umgelter A, Reindl W, Franzen M, Schmidt C, von Delius S, et al. Volume assessment in patients with necrotizing pancreatitis: a comparison of intrathoracic blood volume index, central venous pressure, and hematocrit, and their correlation to cardiac index and extravascular lung water index. Crit Care Med. 2008;36(8):2348–54.
Huber W, Mair S, Götz SQ, Tschirdewahn J, Siegel J, Schmid RM, et al. Extravascular lung water and its association with weight, height, age, and gender: a study in intensive care unit patients. Intensive Care Med. 2013;39(1):146–50.
Yun S, Han D, Oh SJ, Chun S, Choe J, Yoo Y, editors. Cutmix: regularization strategy to train strong classifiers with localizable features. Proceedings of the IEEE/CVF International Conference on Computer Vision; 2019.
Tan M, Le Q, editors. Efficientnet: rethinking model scaling for convolutional neural networks. International Conference on Machine Learning; 2019: PMLR.
Howard J, Gugger S. Fastai: a layered API for deep learning. Information. 2020;11(2):108.
Chicco D, Jurman G. The advantages of the Matthews correlation coefficient (MCC) over F1 score and accuracy in binary classification evaluation. BMC Genomics. 2020;21(1):6.
Majkowska A, Mittal S, Steiner DF, Reicher JJ, McKinney SM, Duggan GE, et al. Chest radiograph interpretation with deep learning models: assessment with radiologist-adjudicated reference standards and population-adjusted evaluation. Radiology. 2019;294(2):421–31.
Seah JCY, Tang JSN, Kitchen A, Gaillard F, Dixon AF. Chest radiographs in congestive heart failure: visualizing neural network learning. Radiology. 2018;290(2):514–22.
Chrysopoulo MT, Barrow RE, Muller M, Rubin S, Barrow LN, Herndon DN. Chest radiographic appearances in severely burned adults. A comparison of early radiographic and extravascular lung thermal volume changes. J Burn Care Rehabil. 2001;22(2):104–10.
Acknowledgements
We dedicate this paper in memoriam of Prof. Dr. med. Wolfgang Huber who inspired this work and contributed valuable input in the early stage of this study. Prof. Huber sadly passed away on the 08th of May 2020 after a short sudden disease. We are still in deep sorrow for the loss of such a one of a kind thorough clinician, impactful scientist, patient and joyful teacher and wonderful colleague.
Funding
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
DS contributed to the data acquisition, did the programming, data evaluation and wrote the main manuscript text. SR, MH, RA, AP, JU, MS contributed to the data acquisition. RMS and TL provided funding. GAK, RFB and TL contributed valuable input to the idea and the final manuscript. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Ethical approval and consent to participate
It was approved by the ethical review board of our institution (Protocol number 87/18 S) and was performed in accordance with the Declaration of Helsinki.
Competing interests
Sebastian Rasch received lecture fees and from CytoSorbents.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Schulz, D., Rasch, S., Heilmaier, M. et al. A deep learning model enables accurate prediction and quantification of pulmonary edema from chest X-rays. Crit Care 27, 201 (2023). https://doi.org/10.1186/s13054-023-04426-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13054-023-04426-5