
Abstract
Purpose
Veno-arterial (VA) extracorporeal membrane oxygenation (ECMO) can be used to restore organ perfusion in patients with cardiogenic shock until native heart recovery occurs. It may be challenging, however, to determine when patients can be weaned successfully from ECMO—surviving without requiring further mechanical support or heart transplant. We aimed to systematically review the medical literature to determine the biomarkers, hemodynamic and echocardiographic parameters associated with successful weaning of VA-ECMO in adults with cardiogenic shock and to present an evidence-based weaning algorithm incorporating key findings.
Method
We systematically searched PubMed, Embase, ProQuest, Google Scholars, Web of Science and the Grey literature for pertinent original research reports. We excluded studies limited to extracorporeal cardiopulmonary resuscitation (ECPR) as the neurological prognosis may significantly alter the decision-making process surrounding the device removal in this patient population. Studies with a mixed population of VA-ECMO for cardiogenic shock or cardiac arrest were included. We excluded studies limited to patients in which ECMO was only used as a bridge to VAD or heart transplant, as such patients are, by definition, never “successfully weaned.” We used the Risk of Bias Assessment tool for Non-Randomized Studies. The study was registered on the International prospective register of systematic reviews (PROSPERO CRD42020178641).
Results
We screened 14,578 records and included 47 that met our pre-specified criteria. Signs of lower initial severity of shock and myocardial injury, early recovery of systemic perfusion, left and right ventricular recovery, hemodynamic and echocardiographic stability during flow reduction trial and/or pump-controlled retrograde trial off predicted successful weaning. The most widely used parameter was the left ventricular outflow tract velocity time integral, an indicator of stroke volume. Most studies had a moderate or high risk of bias. Heterogeneity in methods, timing, and conditions of measurements precluded any meta-analysis.
Conclusions
In adult patients on VA-ECMO for cardiogenic shock, multiple biomarkers, hemodynamic and echocardiographic parameters may be used to track resolution of systemic hypoperfusion and myocardial recovery in order to identify patients that can be successfully weaned.
Graphical Abstract

Similar content being viewed by others

Take-home message
In adult patients on VA-ECMO for cardiogenic shock, the following indices predicted successful weaning from VA-ECMO (survival after removal of ECMO without requirement for further mechanical support or heart transplant):
-
Lower severity of initial shock (MAP, lactates) and myocardial injury (Troponins).
-
Early recovery of systemic perfusion (lactate, liver enzymes, microcirculation).
-
Left ventricular recovery (LVEF > 20–25%, LVOT VTI > 10 cm, Mitral TDSa > 10 cm/s).
-
Right ventricular recovery (TAPSE ≥ 19 mm, RVEF ≥ 25%, Low RA/PCWP, High PAPi).
-
Stable MAP, CI, SBP without significant increase in inotropic support and stable or improved LV/RV function during flow reduction trial and PCRTO.
Most studies were observational, unblinded, retrospective and had small sample size and a moderate or high risk of bias.
Introduction
Veno-arterial (VA) extracorporeal membrane oxygenation (ECMO) can be used to restore organ perfusion in patients with cardiogenic shock [1, 2]. The device drains deoxygenated blood from a venous inflow cannula, drives it through a membrane lung and returns oxygenated blood in an arterial outflow cannula, providing both respiratory and cardiac support [3]. VA-ECMO can be used as a bridge to recovery, restoring and maintaining systemic perfusion while cardiac recovery occurs. In the absence of myocardial recovery, VA-ECMO may act as a bridge to durable ventricular assist device (VAD) implantation or heart transplant [4]. Successful weaning of VA-ECMO is generally defined as survival after complete removal of the extracorporeal circuit without requirement for further mechanical support or heart transplant [5,6,7,8]. Reported success rates range from 30 to 75% [5,6,7,8,9]. The timing of weaning is crucial as premature withdrawal may lead to recurrence of shock and cause secondary injury on barely recuperating organs. Conversely, longer duration of ECMO is associated with higher complications and in-hospital mortality [10, 11]. Identifying patients who are ready to be weaned off VA-ECMO may be challenging. The Extracorporeal Life Support Organization (ELSO) recommends that weaning be attempted in hemodynamically stable patients on low vasoactive support with the use of echocardiography to assess myocardial recovery [12,13,14]. Echocardiographic indices [15] are widely used to assess readiness to be weaned. Other parameters, such as biomarkers [16] or hemodynamic parameters [17] may also be used. Despite numerous descriptions of weaning protocols based on expert opinion in the literature [7, 18, 19], there has been no systematic reviews to provide more robust guidance. We aimed to systematically review the medical literature to determine the biomarkers, hemodynamic and echocardiographic parameters associated with successful weaning of VA-ECMO in adults with cardiogenic shock. Secondarily, we aimed to present an evidence-based weaning algorithm incorporating key findings to guide clinicians in the weaning process.
Methods
The protocol for this systematic review was registered on the International Prospective Register of Systematic Reviews (CRD42020178641). The results are reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis Guidelines [20].
Study characteristics
As we did not expect randomized controlled trials to be available on the subject, we elected to include both interventional and observational studies, including cohort studies and case-series ≥ 10 patients. We included records in all languages, both in full text or abstract-only formats, published from database inception to April 10, 2022. Studies had to report on the association between biomarkers, hemodynamic and echocardiographic parameters and VA-ECMO weaning success. Studies evaluating the association between therapies and weaning success were excluded. Studies evaluating exclusively the association of baseline parameters (before ECMO initiation) and weaning success were excluded. The PICO strategy is detailed in Fig. 1.

Search strategy. NP brain natriuretic peptide, C comparison, I intervention, LVOT VTI left ventricular outflow tract velocity–time integral, O outcome, P population
Participants
We selected studies that included adults with cardiogenic shock secondary to potentially reversible etiologies treated with VA-ECMO. We excluded studies limited to extracorporeal cardiopulmonary resuscitation (ECPR) as the neurological prognosis may significantly alter the decision-making process surrounding the device removal in this patient population. Studies with a mixed population of VA-ECMO for cardiogenic shock or cardiac arrest were included. We excluded studies limited to patients in which ECMO was only used as a bridge to VAD or heart transplant, as such patients are, by definition, never “successfully weaned.”
Search strategy
The search strategy is detailed in Additional file 1: Table S2. We searched Medline and Embase for studies including the following concepts: VA-ECMO, ECMO, extracorporeal life support (ECLS), ECPR, cardiogenic shock, weaning, success, decannulation. ProQuest, Google Scholar and Grey literature (OpenGrey, GreyLit, GreyNet) were also searched using key search terms. Backward and forward citation tracking was performed using Web of Science. Conference abstracts indexed in Embase and these other sources were eligible for inclusion. The searches were rerun prior to the final analyses (April 10, 2022) and further studies retrieved for inclusion.
Study selection process
Covidence systematic review software (Veritas Health Innovation, Melbourne, Australia) was used for the selection process. Two independent members of the review team (FC and EB or OL or KC) first screened the citations using only titles and abstracts and assessed the full texts for eligibility. Conflicts were resolved by consensus by the corresponding author (YAC).
Data extraction and synthesis
Study design, setting, country, period, sample size, funding source, VA-ECMO indication, weaning protocol, successful weaning definition and reported value, biomarkers, hemodynamic and echocardiographic data as well as effect measures between exposition and outcome were extracted independently by authors on electronic data collection forms (Covidence software). Missing data were presented as not reported in Table 1. The primary outcome was weaning success, defined as survival after complete removal of the extracorporeal circuit without requirement for further mechanical support or heart transplant. We planned to present a narrative synthesis of findings and a meta-analysis of the diagnostic accuracy of parameters to predict a successful weaning if they had been studied by multiple groups under similar conditions.
Quality assessment and risk of bias
The quality assessment of all retained articles was performed by two independent reviewers (FC and EB or OL or KC), with conflicts resolved by consensus by the corresponding author (YAC), using the Cochrane’s Risk of Bias Assessment tool for Non-randomized Studies [21].
Results
Study selection and characteristics
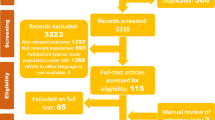
The search strategy yielded a total of 14,578 records, including 2742 duplicates that were removed. The remaining 11,830 were screened by title and abstract. We reviewed the full text of 130 records to assess eligibility, 47 of which studies were finally selected (Fig. 2 and Table 1). Study sample size ranged from 12 to 258 patients. The main indications for ECMO were cardiogenic shock secondary to acute myocardial infarction (AMI), fulminant myocarditis, other acute cardiomyopathies, post-cardiotomy shock and cardiac arrest. Eight studies included some cardiac arrest patients in their case-mix [9, 22,23,24,25,26,27,28]. Specific etiology of cardiac arrest was not specified in most studies. The risk of bias of the included records can be found in Table 2. Fifteen studies were published conference abstracts that did not provide detailed protocols, greatly limiting our methodological assessment. Most studies presented a high risk of bias overall.

PRISMA flowchart. ECPR Extracorporeal cardiopulmonary resuscitation
Main findings: parameters to predict weaning success
Selected records reported on the use of various parameters to predict successful weaning, including biomarkers, microcirculation indices, hemodynamic, respiratory and echocardiographic parameters. Individual study findings are detailed in Table 1 and summarized below. Heterogeneity in methods, timing and conditions of measurements precluded any meta-analysis.
Biomarkers
Cardiac injury
Elevation in biomarkers reflecting the severity of myocardial injury was associated with adverse weaning outcomes in most studies. Lower peak CK-MB was associated with higher weaning success and better initial systolic function in patients with myocarditis or cardiac arrest [5, 29, 30]. Peak CK-MB < 183 U/L predicted weaning success with a sensitivity of 86%, a specificity of 71% and an area under the receiving operator characteristic curve (AUROC) of 0.89 [CI95: 0.77–1.00] [30]. Peak troponins were associated with weaning success in AMI patients (p = 0.003) [31], but not in a cohort of patients with refractory CS of mixed etiologies where AMI represented only 27% of the cohort [23]. Several other biomarkers including NT-proBNP failed to demonstrate any predictive value for successful weaning [23].
Oxygen delivery
Early correction of biomarkers reflecting tissue hypoperfusion appeared to predict successful weaning. Blood lactate levels at 24 h of support were independently associated with successful weaning in patients with cardiac arrest caused by AMI cannulated during or after the arrest (OR 0.52, p = 0.018) [32,33,34]. Lactate clearance in the first 12 h similarly predicted weaning outcomes in post-cardiotomy VA-ECMO (AUROC 0.72; OR 0.3; p = 0.023) [16, 34]. However, initial [5, 16, 26, 30, 32, 33, 35,36,37,38] and pre-weaning [23, 39,40,41] lactate values were inconsistently associated with weaning success. We also found conflicting data concerning the association between mixed venous oxygen saturation (SvO2) and VA-ECMO weaning success. Hsu et al. found a higher pre-weaning SvO2 in patients that survived compared to those that died following weaning [39]. Yoshida et al. found no difference in the mean SvO2 while on VA-ECMO in weaned vs non-weaned patients [26]. Finally, Naruke et al. reported that patients with sustained SvO2 < 75% during VA-ECMO had a higher rate of weaning success (88 vs 47% p < 0.01) compared to patients that experienced periods of SvO2 > 75% [42].
Organ damage
Similarly, signs of persistent organ damage are adversely linked to weaning outcomes. Higher aspartate aminotransferase at 48 h and 72 h after initiation of ECMO was associated with weaning failure [5, 43].
Microcirculation
Multiple studies evaluated the use of microcirculatory parameters in VA-ECMO. During the first 48 h of support, successfully weaned patients showed a significantly higher perfused small vessel density (p = 0.002), small vessel density (p = 0.008) and percent perfused vessels (p = 0.02) [44]. Before first weaning attempt, higher skin blood flow (≥ 34 perfusion units) measured by skin laser Doppler was also found to accurately predict weaning success (AUROC = 0.93 [CI95: 0.81–1]; sensitivity 83%; and specificity 92%) [36]. During an extracorporeal blood flow (ECBF) reduction trial (50% of initial ECBF), total vessel density and perfused vessel density displayed an AUROC of 0.99 and 0.91, respectively, for the prediction of successful weaning. In two of these studies, microcirculatory indices outperformed commonly used echocardiographic parameters such as left ventricular ejection fraction (LVEF) and left ventricular outflow tract (LVOT) velocity time integral (VTI) [36, 45].
Macrocirculation
Better early hemodynamic parameters as well as their maintenance during the weaning phase appear to predict weaning success [46]. Higher mean arterial pressure (MAP) and MAP to pulmonary artery pressure ratio at 24 h were associated with successful weaning [32, 47]. Over the first 6 h of extracorporeal support, a pulse pressure (PP) < 30 mmHg, reflecting reduced residual LV ejection, was found to be independently associated with weaning failure (OR: 0.95, Log rank p < 0.001) [17]. MAP at time of weaning was independently associated with weaning success (OR: 1.05, p = 0.009) [41, 48]. In a cohort of weaned patients, MAP, cardiac index and PP increased significantly from pre-ECMO to weaning despite a reduction in inotropic support. Moreover, compared to patients who died after weaning, patients who survived to ICU discharge had a higher systolic blood pressure (120 [112–140] vs 103 [99–125] mmHg, p = 0.04) despite a lower inotropic score [9] and a lower central venous pressure (CVP) [39]. Successfully weaned patients also presented more favorable right ventricular (RV) hemodynamic parameters at 48 and 72 h: lower right atrial to pulmonary capillary wedge pressure (PCWP), lower transpulmonary gradient and higher pulmonary artery pulsatility index [49].
End-tidal CO2
In patients on VA-ECMO, end-tidal CO2 (EtCO2) is primarily determined by transpulmonary blood flow generated by the native heart. It may thus be used to monitor native cardiac output in this context (Table 3). In a cohort of 37 patients on VA-ECMO, an increase in EtCO2 of 5 mmHg or more above previous mean values during two consecutive 12-h periods occurred in all successfully weaned patients and in none of the patients that could not be successfully weaned [50]. This inflection point in EtCO2 preceded cardiac index increase. Weaned patients were also found to have a higher absolute EtCO2 value at 24 h of extracorporeal support. Their average EtCO2 increased from 9 mmHg immediately post-cannulation to 21 mmHg at 24 h (p = 0.04) [26].
Echocardiographic assessment
LV function
Early recovery of LVEF after VA-ECMO initiation has been associated with improved weaning outcomes. LVEF significantly increased after cannulation in weaned patients (from baseline to 24 h: + 8.5%, p = 0.012; from 24 to 48 h, + 9.0%, p = 0.001) [32]. At 48 h of support, both the absolute LVEF (OR 1.11 [1.01–1.22]; p = 0.03) and LVEF change from baseline (OR 1.15 [1.01–1.31]; p = 0.03) were independently associated with weaning success [43]. Multiple studies similarly showed a higher LVEF and fractional shortening (FS) [29, 31, 41] as well as lower LV chamber sizes in successfully weaned patients compared to non-weaned patients [39, 51, 52]. Others found LVEF improvement from cannulation to weaning, without significant absolute differences in LVEF values in weaned vs non-weaned patients [9, 22, 53, 54].
LVOT VTI is the most widely used parameter to track LV recovery in patients on VA-ECMO [15, 22, 27, 36, 40, 41, 48, 52, 54,55,56,57]. Successfully weaned patients tend to have a higher VTI at the time of weaning, reflecting a better stroke volume. The most commonly reported threshold to predict successful weaning is > 9.5 cm. The threshold itself and the conditions under which it is measured, especially the timing and the ECBF, vary significantly across studies, making comparisons difficult [15, 22, 36, 40, 48, 52, 54,55,56,57]. Two studies reported on the accuracy of the LVOT VTI to predict weaning success. Mongkolpun et al. found an AUROC of 0.85 [CI95: 0.65–1] [36] and Sawada et al. an AUROC of 0.74, with a sensitivity of 75% and a specificity of 72% at an optimal VTI threshold of > 8.6 cm [40]. The ratio of VTI from cannulation to weaning has also shown a strong association with successful weaning (OR, 2.80, p = 0.01) [27, 41, 48]. In two different studies, Aissaoui and colleagues reported a higher VTI in the group of successfully weaned patients compared to those who were not, both at maximal (10.5 vs 6.2 cm, p < 0.001) and minimal ECBF during weaning trials (12.8 vs 9.5 cm, p = 0.010 and 16.4 vs 8.5 cm, p < 0.0001) [15, 52]. The main limitation, Aissaoui found, is the load dependence of most LV function parameters, including LVEF, LVOT VTI, LV systolic velocity, strain and strain rate [52].
Tissue Doppler systolic velocities, which were also found to be higher in successfully weaned patients, are probably less load-dependent [15, 41, 52, 54]. Improvements in lateral e′ velocity and tricuspid annular S′ velocity during a flow reduction trial predicted weaning success with a better performance (AUROC for the presence of both parameters = 0.93 [CI95: 0.863–0.996]; p < 0.001) than conventional parameters, such as LVEF > 20–25%, LVOT VTI ≥ 10 cm and mitral annulus S′ ≥ 6 cm/s [58]. Total isovolumic time (t-IVT, Additional file 1: Table S1) improvement in the first 48 h of support was the strongest predictor of successful VA-ECMO weaning in another study [22]. Measured at an ECBF of 1.5 L/min, a corrected LV ejection time (LVETc) to PCWP ratio > 15.9 s/mmHg was a robust predictor of weaning success (AUROC = 0.82; sensitivity = 88%; specificity = 69%) [40].
RV function
Improvement in RV function during ECMO also appears to be associated with weaning success [59]. Pappalardo and colleagues observed a decrease in the prevalence of RV failure from 52% pre-ECMO to 36% during weaning in successfully weaned patients [9]. Successfully weaned patients exhibited a higher tricuspid plane systolic excursion at full ECBF (16 vs 8 mm, p = 0.02) [25, 56]. Tricuspid lateral annular S′/right ventricular systolic pressure > 0.33 was associated with successful weaning at full and minimal ECMO flow, performing better than conventional LV indexes, reflecting better RV coupling to pulmonary circulation [60]. Huang et al. also found the three-dimensional RV ejection fraction to be the strongest predictor of successful decannulation at first attempt (AUROC 0.90; CI95: 0.80–0.99) [61].
Biventricular function
In an unblinded study, qualitative echocardiographic assessment of biventricular recovery during a weaning trial had a positive predictive value of 100% [CI95: 73–100%] for successful weaning [7]. Interestingly, absence of ventricular interdependence was found to be a robust predictor of successful weaning, with sensitivity of 94% and specificity of 95% [55].
Weaning trial
Weaning protocols varied significantly across studies, as detailed in Table 1. Our main findings concerning weaning protocols reported in the literature are summarized below.
Criteria used to decide to submit patients to a weaning trial were not always explicitly reported and varied significantly. Most commonly used criteria included a MAP ≥ 60 mmHg and systemic arterial pulsatility on minimal inotropic and vasopressor support [5, 9, 15, 16, 23, 25, 32, 35, 40, 45, 47, 52, 54, 58, 61]. Another commonly stated condition was the resolution of shock as indicated, for instance, by lactate normalization [25, 40, 45, 58, 61], SVO2 > 65% [40, 45] or end-organ dysfunction recovery [7, 16, 40, 44]. Most authors used some form of myocardial improvement, globally [47] or a specific parameter such as LV FS [40], LVEF ≥ 20% and S′ > 6 cm/s [25], LVETc > 200 ms [29, 30, 40], LVOT VTI ≥ 10 cm [25, 56, 57] or TAPSE > 10 mm [25]. Other conditions included the absence of ventricular arrhythmia [47], optimized fluid balance [7, 25, 51] with a low CVP [51, 58, 61] and adequate native lung oxygenation capacity [7, 15, 23, 25, 32, 50, 52, 54] with resolution of pulmonary edema and an inspired oxygen fraction < 50% [7, 25].
In patients who met these criteria, a gradual ECBF reduction was usually advocated with close monitoring of hemodynamic, vasopressor needs and biventricular response to load variation. Even with a minimal ECBF, VA-ECMO still provides significant cardiorespiratory support. As such, some centers reported clamping the circuit in patients who remained stable at 0.5–1.5 L/min of ECBF. Others used a pump-controlled retrograde trial off (PCRTO) to challenge the native heart without the increased risk of thrombus formation associated with circuit clamping [62]. Pump speed was reduced in a controlled fashion until the flow became retrograde (− 0.5 to − 1 L/min). This was maintained for up to an hour, after which the test was considered successful if hemodynamic parameters, vasopressors needs and oxygen requirements remained stable. Ling and colleagues compared the outcomes of seven patients weaned after a successful PCRTO, to 23 patients weaned without PCRTO. The reported number of deaths due to cardiac failure in the PCRTO and conventional groups was 0 and 3, respectively (0 vs 13%, p = 0.99) [63]. Lower initial heart rate and PCWP measured by Swan-Ganz catheter at the start of PCRTO were associated with weaning success during this procedure [28].
Discussion
In this systematic review of the literature, we found multiple studies reporting on biomarkers, hemodynamic and echocardiographic parameters associated with successful weaning of VA-ECMO in adults. These were mainly small observational studies with a relatively high risk of bias. They nevertheless allowed to draw some important points to guide the weaning process. First, the initial severity of shock and myocardial injury may help establish baseline prognosis. Second, rapid recovery of systemic perfusion is associated with weaning success. Third, signs of native heart recovery are strongly associated with weaning success. Finally, in patients that show signs of native heart recovery, readiness to be weaned can be further assessed with a flow reduction trial, with or without a PCRTO (Fig. 3).

VA-ECMO weaning algorithm. CK-MB creatine kinase MB, CI cardiac index, CVP central venous pressure, ECMO extracorporeal membrane oxygenation, ETCO2 end-tidal CO2, e′ early diastolic peak myocardial velocities, LV left ventricle, LVAD left ventricular assist device, LVEF left ventricular ejection fraction, LVOT VTI left ventricular outflow tract velocity time integral, MAP mean arterial pressure, MPAP mean pulmonary arterial pressure, MFI microvascular flow index, PAPi pulmonary artery pulsatility index, PCWP pulmonary capillary wedge pressure, PH pulmonary hypertension, PP pulse pressure, PPV percent perfused vessels, PSVD perfused small vessel density, RA right atrial, RV right ventricle, RVEF right ventricular ejection fraction, SBP systolic blood pressure, SVD small vessel density, S′ velocity systolic peak myocardial velocities, TAPSE tricuspid annular plane systolic excursion, TDSa systolic tissue Doppler imaging septal mitral annulus, TPG transpulmonary gradient, VV veno-venous, V-A-V veno-arterio-venous, *Investigational markers
Proposed evidenced-based algorithm for VA-ECMO weaning
Step 1: establishing initial illness severity
Initial severity of illness greatly impacts the odds of being weaned successfully from VA-ECMO. Although this may not directly help determine if a patient is ready to be weaned, it may help set expectations. For instance, a patient with very severe initial myocardial injury and limited organ dysfunction may be considered early for durable left ventricular assist device implantation or heart transplantation. Greater initial myocardial injury, reflected by higher CK-MB, troponins and lower initial systolic function are associated with weaning failure in multiple studies [5, 29,30,31]. At the time of ECMO initiation, parameters of shock severity such as lactate, end-organ perfusion markers, hemodynamics and extent of myocardial injury predict subsequent weaning and survival. In the first 24 h of support, weaned patients have a higher MAP and PP [17, 32, 47]. Microcirculation indices could also help refine prognostication in the future as they appear to strongly predict weaning outcomes early [36, 44] and independently of hemodynamic parameters, lactates and inotropic support [44, 64, 65].
Step 2: monitoring recovery of tissue and organ perfusion
If flow is adequately restored through VA-ECMO, one should expect rapid normalization of markers of hypoperfusion and end-organ damage. Studies showed increased rates of successful weaning with higher lactate clearance and AST normalization in the first 72 h [5, 24, 26, 32,33,34,35, 37, 38, 43]. Microcirculatory improvement in the first 48 h has also been associated with successful weaning [36, 44]. Persistence of markers of hypoperfusion should prompt clinicians to try to further improve blood flow by increasing extracorporeal circuit or native heart output, decreasing venous congestion, and seeking local causes of hypoperfusion that could be addressed (such as mesenteric ischemia). In the absence of adequate restoration of tissue perfusion under maximal support, irreversible organ injury usually ensues.
Step 3: assessing recovery of native heart function
Once tissue perfusion is restored, the next step is to assess native heart recovery. Under constant minute ventilation, an increase in EtCO2 reflects an increase in transpulmonary flow, a reliable marker of native cardiac output recovery that may be observed earlier than changes in hemodynamics [26, 50]. Higher LVOT VTI, both at minimal and maximal ECBF, is a widely used parameter of LV recovery with good predictive performance for weaning success [27, 48]. Weaned patients also tend to display higher LVEF, t-IVT, FS, MAPSE and mitral S′ velocity [25, 29, 40, 43, 53]. Echocardiographic (RV ejection fraction and TAPSE) [25, 59, 61] and hemodynamic (RA/PCWP ratio, TPG and PAPi) parameters of RV function are also strongly associated with weaning success [47, 49]. On full extracorporeal support, LV indices tend to underestimate true LV performance, while RV indices tend to overestimate true RV performance. Tissue Doppler systolic velocities are relatively load-independent [15, 52, 54, 58, 66, 67], making them interesting parameters to follow when patients are still supported with high ECBF.
Step 4: performing flow reduction trials
In stable patients with evidence of myocardial recovery, a trial of ECBF reduction is generally attempted prior to decannulation to assess the net hemodynamic effect of reducing the support provided by VA-ECMO. The effect of flow reduction on MAP, CVP and vasopressor-inotropic support is observed. If tolerated, echocardiographic evaluation may be performed. Better indices of LV systolic and diastolic function [7, 15, 51, 52, 55, 57], ventricular interdependence [55] and RV function [58] during flow reduction trials predict favorable weaning outcomes. Importantly, flow reduction may unmask significant underlying hypoxemic respiratory failure that may be associated with increased pulmonary vascular resistance [19].
Step 5: pump-controlled retrograde trial off (PCRTO)
Finally, PCRTO may be performed by reducing the centrifugal pump rotation speed until a retrograde flow occurs through the circuit. This creates a controlled arterio-venous fistula, with the blood being pumped through the ECMO circuit by the native heart, returning in the venous system. This significantly challenges the RV which has to accommodate a substantial preload increase. Thereby, it may simulate VA-ECMO decannulation more accurately than flow reduction and may last longer than circuit clamping, which is limited by the risk of clot formation. During retrograde flow, the sweep gas should be turned off to uncover any residual gas exchange impairment [63]. By reversing the flow, there is a theoretical risk of pulmonary embolism through clot detachment from the venous side of the oxygenator. More studies are needed to validate this method.
Strengths and limitations
This is the first systematic review on VA-ECMO weaning providing an exhaustive and detailed summary of the literature for clinicians and researchers. Our conclusions, however, are limited by the quality of the available literature. We included mostly unblinded observational retrospective studies with small sample sizes and a high risk of bias. Many of the reported parameters, including ETCO2, were studied in small cohorts of patients. This warrants cautious interpretation about their role in clinical practice. Also, the microcirculatory parameters are still in the investigative stage and deserve more validation before drawing conclusions that will influence VA-ECMO weaning guidance. Variability in weaning protocols and in the definition of successful weaning make interpretation and comparison between studies difficult. Most studies did not provide formal assessments of predictive accuracy of the proposed indices and only reported on associations. Selection bias was often present as patients who were not considered for weaning because of complications or futility were often not included. There was often significant residual confounding. These limitations underline the need for high-quality research in this area, more robust data on investigational markers and standardization of weaning protocols and successful VA-ECMO weaning definition.
Conclusion
We found a large number of studies, of generally low quality, reporting on parameters associated with successful weaning of VA-ECMO in adults. We propose a stepwise approach to weaning based on our findings. First, the initial severity of shock and myocardial injury may help establish baseline prognosis. Then, signs of reversal of tissue hypoperfusion and native heart recovery may help determine readiness to be weaned. Finally, careful assessment of the physiological response to extracorporeal blood flow reduction and/or reversal may allow identification of patients who are ready to be safely decannulated.
Availability of data and materials
All data generated or analyzed during this study are included in this published article and its supplementary information file.
Abbreviations
- ABG:
-
Arterial blood gas
- ACHF:
-
Acute on chronic heart failure
- AMI:
-
Acute myocardial infarction
- ALT:
-
Alanine aminotransferase
- AST:
-
Aspartate aminotransferase
- AUROC:
-
Area under the receiving operator characteristic curve
- BIC:
-
Bicarbonate
- BE:
-
Base excess
- Bili:
-
Bilirubin
- BP:
-
Blood pressure
- BNP:
-
Brain natriuretic peptide
- BUN:
-
Blood urea nitrogen
- CBC:
-
Complete blood count
- CE-CT:
-
Contrast enhanced computed tomodensitometry
- CI:
-
Cardiac index
- CK-MB:
-
Creatine kinase MB
- CI95 :
-
95% confidence interval
- CMP:
-
Cardiomyopathy
- CO:
-
Cardiac output
- CREAT:
-
Creatinine
- CS:
-
Cardiogenic shock
- CSt:
-
Circumferential strain
- CRP:
-
C-reactive protein
- CPR:
-
Cardiopulmonary resuscitation
- CV:
-
Cardiovascular
- CVP:
-
Central venous pressure
- DBP:
-
Diastolic blood pressure
- ECBF:
-
Extracorporeal blood flow
- ECLS:
-
Extracorporeal life support
- ECMO:
-
Extracorporeal membranous oxygenation
- ECPR:
-
Extracorporeal cardiopulmonary resuscitation
- ELSO:
-
Extracorporeal Life Support Organization
- ETCO2 :
-
End-tidal CO2
- e′:
-
Early diastolic peak mitral velocities
- FAC:
-
Fractional area change
- FM:
-
Fulminant myocarditis
- FS:
-
Fractional shortening
- [FWLS]:
-
Absolute value of free-wall longitudinal strain
- GLS:
-
Global longitudinal strain
- HB:
-
Hemoglobin
- HD:
-
Hemodynamic
- HI:
-
Heterogeneity index
- hTEE:
-
Hemodynamic transesophageal echocardiography
- HR:
-
Heart rate
- INR:
-
International normalized ratio
- L:
-
Liter
- Lact:
-
Lactates
- LDH:
-
Lactate dehydrogenase
- LS:
-
Longitudinal strain
- LV:
-
Left ventricle
- LVAD:
-
Left ventricular assist device
- LVEDV:
-
Left ventricular end-diastolic volume
- LVEF:
-
Left ventricular ejection fraction
- LVEDD:
-
Left ventricular end-diastolic volume
- LVESD:
-
Left ventricular end systolic volume
- LVETc:
-
Left ventricle ejection time corrected
- LVOT VTI:
-
Left ventricular outflow tract velocity time integral
- LVPWT:
-
Left ventricle posterior wall thickness
- LVWT:
-
Left ventricle wall thickness
- MAP:
-
Mean arterial pressure
- MAPSE:
-
Mitral annular plane systolic excursion
- MCS:
-
Mechanical cardiac support
- MFI:
-
Microvascular flow index
- MPAP:
-
Mean pulmonary arterial pressure
- MR:
-
Mitral regurgitation
- NR:
-
Not reported
- PA:
-
Pulmonary artery
- PAP:
-
Pulmonary artery pressure
- PAPi:
-
Pulmonary artery pulsatility index
- PCRTO:
-
Pump-controlled retrograde trial off
- PCWP:
-
Pulmonary capillary wedge pressure
- PDB:
-
Pulmonary diastolic pressure
- PE:
-
Pulmonary embolism
- PH:
-
Pulmonary hypertension
- PP:
-
Pulse pressure
- PPV:
-
Percent perfused vessels
- PSP:
-
Pulmonary systolic pressure
- PSVD:
-
Perfused small vessel density
- PVD:
-
Perfused vessel density
- RA:
-
Right atrial
- RAP:
-
Right atrial pressure
- RV:
-
Right ventricle
- RVEDD:
-
Right ventricle end-diastolic volume
- RVEF:
-
Right ventricular ejection fraction
- RVSP:
-
Right ventricular systolic pressure
- SBF:
-
Skin blood flow
- SBP:
-
Systolic blood pressure
- S/L:
-
Sublingual
- SV:
-
Stroke volume
- SVD:
-
Small vessel density
- SVO2 :
-
Mixed venous oxygen saturation
- S′:
-
Systolic peak myocardial velocities
- TAPSE:
-
Tricuspid annular plane systolic excursion
- TD:
-
Tissue Doppler
- a′:
-
Late diastolic atrial contraction velocities
- E:
-
Transmitral early peak velocities
- Ea/e′:
-
Lateral mitral annulus early diastolic velocities
- Sa:
-
Lateral mitral annulus peak systolic velocities
- Sv:
-
Systolic peak velocity
- t-IVT:
-
Total isovolumic time
- TNI:
-
Troponin I
- TPG:
-
Transpulmonary gradient
- TR:
-
Tricuspid regurgitation
- VV:
-
Veno-venous
- TVD:
-
Total vessel density
- V-A-V:
-
Veno-arterio-venous
- VAD:
-
Ventricular assist device
- VTI:
-
Velocity time integral
- VVI:
-
Velocity vector imaging
- WBC:
-
White blood count
References
Abrams D, Garan AR, Abdelbary A, et al. Position paper for the organization of ECMO programs for cardiac failure in adults. Intensive Care Med. 2018;44:717–29. https://doi.org/10.1007/s00134-018-5064-5.
Fiser SM, Tribble CG, Kaza AK, et al. When to discontinue extracorporeal membrane oxygenation for postcardiotomy support. Ann Thorac Surg. 2001. https://doi.org/10.1016/S0003-4975(00)02340-7.
Mebazaa A, Combes A, van Diepen S, et al. Management of cardiogenic shock complicating myocardial infarction. Intensive Care Med. 2018;44:760–73. https://doi.org/10.1007/s00134-018-5214-9.
Rousse N, Juthier F, Pinçon C, et al. ECMO as a bridge to decision: recovery, VAD, or heart transplantation? Int J Cardiol. 2015;187:620–7. https://doi.org/10.1016/j.ijcard.2015.03.283.
Chen Y-S, Chao A, Yu H-Y, et al. Analysis and results of prolonged resuscitation in cardiac arrest patients rescued by extracorporeal membrane oxygenation. J Am Coll Cardiol. 2003;41:197–203. https://doi.org/10.1016/S0735-1097(02)02716-X.
Chang W-W, Tsai F-C, Tsai T-Y, et al. Predictors of mortality in patients successfully weaned from extracorporeal membrane oxygenation. PLoS ONE. 2012. https://doi.org/10.1371/journal.pone.0042687.
Cavarocchi NC, Pitcher HT, Yang Q, et al. Weaning of extracorporeal membrane oxygenation using continuous hemodynamic transesophageal echocardiography. J Thorac Cardiovasc Surg. 2013;146:1474–9. https://doi.org/10.1016/j.jtcvs.2013.06.055.
Aso S, Matsui H, Fushimi K, Yasunaga H. In-hospital mortality and successful weaning from venoarterial extracorporeal membrane oxygenation: analysis of 5,263 patients using a national inpatient database in Japan. Crit Care Lond Engl. 2016;20:80–80. https://doi.org/10.1186/s13054-016-1261-1.
Pappalardo F, Pieri M, Arnaez Corada B, et al. Timing and strategy for weaning from venoarterial ECMO are complex issues. J Cardiothorac Vasc Anesth. 2015;29:906–11. https://doi.org/10.1053/j.jvca.2014.12.011.
Zangrillo A. A meta-analysis of complications and mortality of extracorporeal membrane oxygenation. Crit Care Resusc. 2013;15:7.
Omar HR, Mirsaeidi M, Mangar D, Camporesi EM. Duration of ECMO is an independent predictor of intracranial hemorrhage occurring during ECMO support. ASAIO J. 2016;62:634–6. https://doi.org/10.1097/MAT.0000000000000368.
Extracorporal Life Support Organisation (ELSO). Guidelines for adult cardiac failure. https://www.elso.org/Portals/0/IGD/Archive/FileManager/e76ef78eabcusersshyerdocumentselsoguidelinesforadultcardiacfailure1.3.pdf. Accessed 19 Aug 2019
Extracorporal Life Support Organisation (ELSO). Guidelines for ECPR cases. https://www.elso.org/Portals/0/IGD/Archive/FileManager/6713186745cusersshyerdocumentselsoguidelinesforecprcases1.3.pdf. Accessed 19 Aug 2019
Lorusso R, Shekar K, MacLaren G, et al. ELSO interim guidelines for venoarterial extracorporeal membrane oxygenation in adult cardiac patients. ASAIO J. 2021;67:827–44. https://doi.org/10.1097/MAT.0000000000001510.
Aissaoui N, Luyt C-E, Leprince P, et al. Predictors of successful extracorporeal membrane oxygenation (ECMO) weaning after assistance for refractory cardiogenic shock. Intensive Care Med. 2011;37:1738–45. https://doi.org/10.1007/s00134-011-2358-2.
Li C-L, Wang H, Jia M, et al. The early dynamic behavior of lactate is linked to mortality in postcardiotomy patients with extracorporeal membrane oxygenation support: a retrospective observational study. J Thorac Cardiovasc Surg. 2015;149:1445–50. https://doi.org/10.1016/j.jtcvs.2014.11.052.
Park B-W, Seo D-C, Moon I-K, et al. Pulse pressure as a prognostic marker in patients receiving extracorporeal life support. Resuscitation. 2013;84:1404–8. https://doi.org/10.1016/j.resuscitation.2013.04.009.
Ortuno S, Delmas C, Diehl J-L, et al. Weaning from veno-arterial extra-corporeal membrane oxygenation: which strategy to use? Ann Cardiothorac Surg. 2019;8:E1–8. https://doi.org/10.21037/acs.2018.08.05.
Aissaoui N, El-Banayosy A, Combes A. How to wean a patient from veno-arterial extracorporeal membrane oxygenation. Intensive Care Med. 2015;41:902–5. https://doi.org/10.1007/s00134-015-3663-y.
Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021. https://doi.org/10.1136/bmj.n71.
Risk of Bias Assessment tool for Non-randomized Studies (RoBANS). Development and validation of a new instrument|Colloquium Abstracts. https://abstracts.cochrane.org/2011-madrid/risk-bias-assessment-tool-non-randomized-studies-robans-development-and-validation-new. Accessed 6 Sept 2021
Colombo CNJ, Dammassa V, Pozzi M, et al. Echocardiographic predictors of VA ECMO weaning in patients with cardiogenic shock. Eur Heart J Acute Cardiovasc Care. 2019;8(Supplement 1):144–5. https://doi.org/10.1177/2048872619829424.
Luyt C-E, Landivier A, Leprince P, et al. Usefulness of cardiac biomarkers to predict cardiac recovery in patients on extracorporeal membrane oxygenation support for refractory cardiogenic shock. J Crit Care. 2012;27:524.e7-524.e14. https://doi.org/10.1016/j.jcrc.2011.12.009.
Mazet C, Conil JM, Georges B, et al. How to predict weaning success during ECLS support? Ann Intensive Care. 2017;7(1 Supplement 1):160. https://doi.org/10.1186/s13613-016-0224-7.
Mork SR, Frederiksen CA, Nielsen RR, et al. A systematic approach to weaning from extracorporeal membrane oxygenation in patients with refractory cardiac failure. Acta Anaesthesiol Scand. 2021;17:17. https://doi.org/10.1111/aas.13814.
Yoshida T, Watanabe M, Murakami M, et al. End-tidal carbon dioxide monitoring indicates recovery from cardiogenic shock in patients receiving percutaneous cardiopulmonary support. J Artif Organs. 2005;8:63–6. https://doi.org/10.1007/s10047-004-0279-3.
Gonzalez Martin J, Alonso-Fernandez-Gatta M, Merchan Gomez S, et al. Echocardiographic recovery changes in patients supported with veno-arterial extracorporeal membrane oxygenator and weaning success. Eur Heart J. 2021;42:ehab724 1060. https://doi.org/10.1093/eurheartj/ehab724.1060.
Xu Y, Liu N, Dong D, et al. Pulmonary artery flotation catheter (PAFC) combined with pump-controlled retrograde trial off (PCRTO) as a trial for weaning VA-ECMO patients: a retrospective study. Perfusion. 2022. https://doi.org/10.1177/02676591211054976.
Asaumi Y, Yasuda S, Morii I, et al. Favourable clinical outcome in patients with cardiogenic shock due to fulminant myocarditis supported by percutaneous extracorporeal membrane oxygenation. Eur Heart J. 2005;26:2185–92. https://doi.org/10.1093/eurheartj/ehi411.
Matsumoto M, Asaumi Y, Nakamura Y, et al. Clinical determinants of successful weaning from extracorporeal membrane oxygenation in patients with fulminant myocarditis. ESC Heart Fail. 2018;5:675–84. https://doi.org/10.1002/ehf2.12291.
North M, Eckman P, Samara M, et al. Peak troponin predicts successful weaning from VA ECMO in patients with acute myocardial infarction complicated by cardiogenic shock. Int J Artif Organs. 2022;45:68–74. https://doi.org/10.1177/0391398821991155.
Sugiura A, Abe R, Nakayama T, et al. Predictors of successful weaning from veno-arterial extracorporeal membrane oxygenation after coronary revascularization for acute myocardial infarction complicated by cardiac arrest: a retrospective multicenter study. Shock. 2019;51:690–7. https://doi.org/10.1097/SHK.0000000000001220.
Omar HR, Handshoe JW, Tribble T, Guglin M. Survival on venoarterial extracorporeal membrane oxygenation in cardiogenic shock: which lactate is most useful? ASAIO J. 2022;68:41–5. https://doi.org/10.1097/MAT.0000000000001413.
Suhr L, Djordjevic I, Ivanov B, et al. Concomitant IABP Improves ECMO Weaning: A Single-Center Experience. Thorac Cardiovasc Surg. 2022;70(S 01):S1–61. https://doi.org/10.1055/s-0042-1742931.
Oshima K, Morishita Y, Hinohara H, et al. Factors for weaning from a percutaneous cardiopulmonary support system (PCPS) in patients with severe cardiac failure: a comparative study in weaned and nonweaned patients. Int Heart J. 2006;47:575–84. https://doi.org/10.1536/ihj.47.575.
Mongkolpun W, Bakos P, Peluso L, et al. Cutaneous blood flow as a predictor of successful weaning from VA-ECMO. Crit Care. 2019. https://doi.org/10.1186/s13054-019-2358-0.
Fried JA, Griffin JM, Masoumi A, et al. Predictors of survival and ventricular recovery following acute myocardial infarction requiring extracorporeal membrane oxygenation therapy. ASAIO J. 2022;68:800–7. https://doi.org/10.1097/MAT.0000000000001570.
Morisawa D, Higuchi Y, Iwakura K, et al. Predictive factors for successful weaning from percutaneous cardiopulmonary support in patients with cardiogenic shock complicating acute myocardial infarction. J Cardiol. 2012;60:350–4. https://doi.org/10.1016/j.jjcc.2012.06.005.
Hsu J. Clinical parameters for successful weaning from venous-arterial extracorporeal membrane oxygenation after cardiogenic shock. J Am Coll Cardiol. 2012;59:E1022. https://doi.org/10.1016/S0735-1097%2812%2961023-7.
Sawada K, Kawakami S, Murata S, et al. Predicting parameters for successful weaning from veno-arterial extracorporeal membrane oxygenation in cardiogenic shock. ESC Heart Fail. 2021;8:471–80. https://doi.org/10.1002/ehf2.13097.
Yi R, Guo J, Zhou Q, et al. Effect evaluation of bedside ultrasound monitoring of left ventricular functional parameters combined with clinical indicators on veno-arterial extracorporeal membrane oxygenation. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2021;33:329–33. https://doi.org/10.3760/cma.j.cn121430-20201023-00684.
Naruke T, Inomata T, Kawaguchi T, et al. Prognostic impact of dramatic alteration of mixed venous oxygen saturation on the hemodynamic recovery from veno-arterial extracorporeal membrane oxygenation. Eur Heart J. 2012;33:69. https://doi.org/10.1093/eurheartj/ehs281.
Sawamura A, Okumura T, Hirakawa A, et al. Early prediction model for successful bridge to recovery in patients with fulminant myocarditis supported with percutaneous venoarterial extracorporeal membrane oxygenation—insights from the change pump study. Circ J. 2018;82:699–707. https://doi.org/10.1253/circj.CJ-17-0549.
Chommeloux J, Montero S, Franchineau G, et al. Microcirculation evolution in patients on venoarterial extracorporeal membrane oxygenation for refractory cardiogenic shock. Crit Care Med. 2020;48:e9–17. https://doi.org/10.1097/CCM.0000000000004072.
Akin S, dos Reis MD, Caliskan K, et al. Functional evaluation of sublingual microcirculation indicates successful weaning from VA-ECMO in cardiogenic shock. Crit Care. 2017;21:265. https://doi.org/10.1186/s13054-017-1855-2.
North M, Wilson K, Hryniewicz K. Swan-Ganz catheter guided VA ECMO wean leads to successful decannulation. ASAIO J. 2018;64(Supplement 2):44. https://doi.org/10.1097/MAT.0000000000000882.
Wu MY, Lin PJ, Tsai FC, et al. (2009) Postcardiotomy extracorporeal life support in adults: the optimal duration of bridging to recovery. ASAIO J Am Soc Artif Intern Organs. 1992;55:608–13. https://doi.org/10.1097/mat.0b013e3181b899c0.
Lim JY, Jung JS. Predictors of successful weaning from veno-arterial extracorporeal membrane oxygenation support. Perfus Ger. 2019;34(1 Supplement):88–9. https://doi.org/10.1177/0267659119829686.
Joseph A, Venturini J, Blair JEA, et al. Prognostic value of right ventricular function in percutaneous veno-arterial extracorporeal membrane oxygenation. BMC Cardiovasc Disord. 2019;19:1–16. https://doi.org/10.1186/s12872-018-0978-y.
Naruke T, Inomata T, Imai H, et al. End-tidal carbon dioxide concentration can estimate the appropriate timing for weaning off from extracorporeal membrane oxygenation for refractory circulatory failure. Int Heart J. 2010;51:116–20. https://doi.org/10.1536/ihj.51.116.
Heaney C, Vuthoori R, Lima B, et al. Assessment of cardiac recovery using a formal stepwise weaning protocol in patients supported with venoarterial extracorporeal membrane oxygenation. Artif Organs. 2020;44(3):E97. https://doi.org/10.1111/aor.13651.
Aissaoui N, Guerot E, Combes A, et al. Two-dimensional strain rate and doppler tissue myocardial velocities: analysis by echocardiography of hemodynamic and functional changes of the failed left ventricle during different degrees of extracorporeal life support. J Am Soc Echocardiogr. 2012;25:632–40. https://doi.org/10.1016/j.echo.2012.02.009.
Colombo CNJ, Dammassa V, Pozzi M, et al. Echocardiographic predictors of VA-ECMO weaning in patients with cardiogenic shock. Intensive Care Med Exp. 2019. https://doi.org/10.1186/s40635-019-0265-y.
Ouazani N, Shudo Y, Hill C, et al. The interest of tissue doppler imaging in the weaning of venoarterial extracorporeal membrane oxygenation. BMC Cardiovasc Disord. 2019;19:1–16. https://doi.org/10.1186/s12872-018-0978-y.
Aissaoui N, Caudron J, Leprince P, et al. Right–left ventricular interdependence: a promising predictor of successful extracorporeal membrane oxygenation (ECMO) weaning after assistance for refractory cardiogenic shock. Intensive Care Med. 2017;43:592–4. https://doi.org/10.1007/s00134-016-4657-0.
Frederiksen CA, Nielsen R, Frederiksen AS, et al. Echocardiographic predictors for successful weaning from veno-arterial extracorporeal membrane oxygenation. Eur Heart J. 2018;39(Supplement 1):1200. https://doi.org/10.1093/eurheartj/ehy566.P5689.
Gambaro A, Vazir A, Galiatsou E, et al. Can speckle tracking help to guide VA-ECMO weaning? Provisional results of a pilot study. Perfusion. 2020;35(1 SUPPL):110. https://doi.org/10.1177/0267659120909723.
Kim D, Jang WJ, Park TK, et al. Echocardiographic predictors of successful extracorporeal membrane oxygenation weaning after refractory cardiogenic shock. J Am Soc Echocardiogr. 2021. https://doi.org/10.1016/j.echo.2020.12.002.
Elena Puerto E, Guido Tavazzi G, Alessia Gambaro A, et al. Interaction between veno-arterial extracorporeal membrane oxygenation and the right ventricle. Eur Heart J Acute Cardiovasc Care. 2021;10(zuab020):173. https://doi.org/10.1093/ehjacc/zuab020.173.
Kim D, Park Y, Choi KH, et al. Prognostic implication of RV coupling to pulmonary circulation for successful weaning from extracorporeal membrane oxygenation. JACC Cardiovasc Imaging. 2021;14:1523–31. https://doi.org/10.1016/j.jcmg.2021.02.018.
Huang K-C, Lin L-Y, Chen Y-S, et al. Three-dimensional echocardiography-derived right ventricular ejection fraction correlates with success of decannulation and prognosis in patients stabilized by venoarterial extracorporeal life support. J Am Soc Echocardiogr. 2018;31:169–79. https://doi.org/10.1016/j.echo.2017.09.004.
Westrope C, Harvey C, Robinson S, et al. Pump controlled retrograde trial off from VA-ECMO. ASAIO J. 2013;59:517–9. https://doi.org/10.1097/MAT.0b013e31829f5e9f.
Ling L, Chan KM. Weaning adult patients with cardiogenic shock on veno-arterial extracorporeal membrane oxygenation by pump-controlled retrograde trial off. Perfusion. 2018;33:339–45. https://doi.org/10.1177/0267659118755888.
Yeh Y-C, Lee C-T, Wang C-H, et al. Investigation of microcirculation in patients with venoarterial extracorporeal membrane oxygenation life support. Crit Care Lond Engl. 2018;22:200. https://doi.org/10.1186/s13054-018-2081-2.
Kara A, Akin S, dos Reis MD, et al. Microcirculatory assessment of patients under VA-ECMO. Crit Care. 2016. https://doi.org/10.1186/s13054-016-1519-7.
Abali G, Tokgözoğlu L, Özcebe OI, et al. Which Doppler parameters are load independent? A study in normal volunteers after blood donation. J Am Soc Echocardiogr. 2005;18:1260–5. https://doi.org/10.1016/j.echo.2005.06.012.
Yalçin F, Kaftan A, Muderrisoğlu H, et al. Is Doppler tissue velocity during early left ventricular filling preload independent? Heart. 2002;87:336–9. https://doi.org/10.1136/heart.87.4.336.
Moury PH, Zunarelli R, Bailly S, et al. Diaphragm Thickening during venoarterial extracorporeal membrane oxygenation weaning: an observational prospective study. J Cardiothorac Vasc Anesth. 2021;35:1981–8. https://doi.org/10.1053/j.jvca.2020.10.047.
Acknowledgements
We would like to thank Monique Clar, librarian at Université de Montréal, for her help with the search strategy.
Funding
Dr Cavayas’ work is supported by the Fonds de Recherche du Québec – Santé. Dr Cournoyer’s work is supported by the Département de Médecine Familiale et de Médecine d’Urgence de l’Université de Montréal, as well as the Fonds des Urgentistes de l’Hôpital du Sacré-Cœur de Montréal.
Author information
Authors and Affiliations
Contributions
FC and YAC contributed to study design, data analysis and interpretation and quality and risk of bias assessment and drafted the manuscript. FC, KC, EB, OL and YAC were involved in data acquisition and extraction. FC, EL, YL, KS, MA, PEN, AC and YAC contributed to revision of content. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
No details, images or videos relating to an individual person were collected. Thus, consent for publication was not sought.
Competing interests
On behalf of all authors, the corresponding authors state that there are no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Supplementary tables.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Charbonneau, F., Chahinian, K., Bebawi, E. et al. Parameters associated with successful weaning of veno-arterial extracorporeal membrane oxygenation: a systematic review. Crit Care 26, 375 (2022). https://doi.org/10.1186/s13054-022-04249-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13054-022-04249-w