
Abstract
Background
Ventilator-associated pneumonia (VAP) is common in patients with severe SARS-CoV-2 pneumonia. The aim of this ancillary analysis of the coVAPid multicenter observational retrospective study is to assess the relationship between adjuvant corticosteroid use and the incidence of VAP.
Methods
Planned ancillary analysis of a multicenter retrospective European cohort in 36 ICUs. Adult patients receiving invasive mechanical ventilation for more than 48 h for SARS-CoV-2 pneumonia were consecutively included between February and May 2020. VAP diagnosis required strict definition with clinical, radiological and quantitative microbiological confirmation. We assessed the association of VAP with corticosteroid treatment using univariate and multivariate cause-specific Cox’s proportional hazard models with adjustment on pre-specified confounders.
Results
Among the 545 included patients, 191 (35%) received corticosteroids. The proportional hazard assumption for the effect of corticosteroids on the incidence of VAP could not be accepted, indicating that this effect varied during ICU stay. We found a non-significant lower risk of VAP for corticosteroid-treated patients during the first days in the ICU and an increased risk for longer ICU stay. By modeling the effect of corticosteroids with time-dependent coefficients, the association between corticosteroids and the incidence of VAP was not significant (overall effect p = 0.082), with time-dependent hazard ratios (95% confidence interval) of 0.47 (0.17–1.31) at day 2, 0.95 (0.63–1.42) at day 7, 1.48 (1.01–2.16) at day 14 and 1.94 (1.09–3.46) at day 21.
Conclusions
No significant association was found between adjuvant corticosteroid treatment and the incidence of VAP, although a time-varying effect of corticosteroids was identified along the 28-day follow-up.
Similar content being viewed by others

Introduction
The novel severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) can lead to a severe respiratory tract infection (coronavirus disease 2019 (COVID-19)) and hit the world with multiple pandemic waves from December 2020. During the first surge of COVID-19, studies reported that around 80% of patients admitted to hospital for COVID-19 would require oxygen support [1, 2] and a high rate of them an invasive mechanical ventilation (IMV) due to acute respiratory distress syndrome (ARDS) leading to high mortality rates [3, 4]. IMV during ARDS exposes patients to severe complications, such as ventilator-associated pneumonia (VAP).
Several studies have recently described the high incidence of ventilator-associated lower respiratory tract infection (VA-LRTI) in COVID-19 patients ranging from 30 to 84% [4,5,6,7]. Previous studies demonstrated a significantly higher incidence of VA-LRTI and notably VAP in SARS-CoV-2 pneumonia patients versus non-SARS-CoV-2 pneumonia patients [5, 8,9,10]. High rates of ARDS, alveolar inflammation, prolonged IMV, lung microbiota alteration, COVID-19-related specific lesions, neuromuscular blocking and immunosuppressive agent use could explain this high rate of VAP in SARS-CoV-2 pneumonia patients [11, 12].
The positive results of the randomized controlled multicenter trial RECOVERY [13] and its further confirmation in large meta-analysis [14] have placed dexamethasone as the first line agent for treating hospitalized COVID-19 patients with a significantly improved 28-day survival, especially in the subgroup of patients invasively ventilated. Yet, the impact of such treatment on the incidence of VAP in COVID-19 patients is still a matter for debate, as available data are scarce and conflicting [3, 15,16,17,18,19].
Hence, we sought to determine the relationship between adjuvant corticosteroid treatment and the incidence of VAP in a large cohort of COVID-19 patients invasively ventilated for more than 48 h, during the first surge of the SARS-CoV-2 pandemic. Our hypothesis was that VAP incidence would be higher in corticosteroid-treated versus non-treated COVID-19 patients.
The primary objective was to compare the incidence of VAP in patients receiving or not adjuvant corticosteroid treatment. Secondary objectives were to determine the relationship between adjuvant corticosteroid treatment and 28-day mortality, duration of mechanical ventilation and ICU length of stay, based on the occurrence of VAP. We also evaluated microbiology of VAP in both groups of patients.
Methods
Study design and population
This is a planned ancillary analysis of the coVAPid study, which design was previously described [8]. Briefly, it was a multicenter retrospective observational cohort conducted in 36 ICUs in Europe (28 centers in France, 3 in Spain, 3 in Greece, 1 in Portugal and 1 in Ireland) aimed to determine the relationship between SARS-CoV-2 pneumonia as compared to influenza pneumonia or no viral infection and the incidence of VA-LRTI. The present analysis was restricted to the population of SARS-CoV-2 pneumonia. Patients were 18-year-old or above and received IMV for more than 48 h. Patients were excluded if data related to corticosteroid treatment were not available.
Patients were consecutively included in each center starting from the beginning of the COVID-19 pandemic if they had a positive polymerase chain reaction (PCR) test for the SARS-CoV-2 virus on nasopharyngeal swab or respiratory secretions.
The Ethics Committee and Institutional Review Boards approved the coVAPid study protocol (Comité de Protection des Personnes Ouest VI; approved by April 14, 2020; registration number RIPH:20.04.09.60039) as minimal-risk research using data collected for routine clinical practice. The requirement for informed consent was waived, and patients or their relative received information about the study and were given the possibility to refuse the use of their personal data. The coVAPid database was registered into the “Commission Nationale de l’Informatique et des Libertés” in accordance with the French law. The coVAPid study was registered at ClinicalTrials.gov, number NCT04359793.
Demographic characteristics, severity scores and comorbidities, past medical history and ongoing treatments, prior hospitalization and exposition to antibiotics (during the past three months) were collected for each patient at baseline. During hospitalization, clinical, biological and radiological findings were recorded as well as the different treatments received during ICU stay (i.e., prone positioning, extra corporeal membrane oxygenation (ECMO)). Antibiotic and corticosteroid use was recorded as type, time of initiation, duration of exposure before occurrence of VAP, maximum daily dose expressed as prednisone equivalent dose (for corticosteroid treatment).
Objectives and outcomes
Our primary objective was to determine the impact of corticosteroid use on the incidence of VAP in SARS-CoV-2 pneumonia patients. The primary outcome was the occurrence of VAP [8, 20]. Briefly, new or progressive infiltrates on chest X-rays and two of the following criteria were needed for the diagnosis of VAP: (1) leucocyte count greater than 12,000 cells per μL or less than 4000 cells per μL, (2) hyperthermia above 38.5 °C or hypothermia under 36.5 °C, (3) purulent tracheal secretions. Microbiological confirmation was required to confirm the diagnosis, with at least 105 colony-forming units (CFUs) per mL for endotracheal aspirates or 104 CFU per mL for bronchoalveolar lavage. VAP episodes were prospectively recorded and confirmed by two distinct physicians as well as the chest X-rays readings. Only first VAP episodes were taken into account.
The secondary objective was to determine the impact of adjuvant corticosteroid treatment on 28-day mortality, MV duration and ICU length of stay.
Statistical analysis
Categorical variables are reported as absolute number and percentage, whereas continuous variables are expressed as median with interquartile range (25th–75th percentile). Patient characteristics at ICU admission and during ICU stay were described according to the use or not of corticosteroids without statistical comparisons. The 28-day cumulative incidence of VAP, extubation alive and ICU discharge alive were estimated using the Kalbfleisch and Prentice method [21], considering extubation within 28-day (dead or alive), death under MV, or death during ICU as a competing events. The 28-day cumulative incidence of all-cause mortality was estimated using the Kaplan–Meier method.
The association between corticosteroids and VAP was assessed using Cox regression with cause-specific hazard function considering initiation of corticosteroid treatment as a time-varying covariate. In this model, extubation within 28 days (dead or alive) without VAP was considered as a competing event. The corticosteroid time-varying variable was coded 0 during the period before the start of the treatment and 1 from the day of initiation of corticosteroids until the occurrence of VAP or MV withdrawal or death within the 28-day period of follow-up. The cause-specific hazard ratios (cHR) for corticosteroid vs. non-corticosteroid exposure were calculated as effect size. Hazard assumption proportionality of corticosteroids during follow-up was assessed by using the scaled Schoenfeld residuals plots. Since the assumption was not satisfied, the corticosteroids effect was modeled using time-dependent coefficient by including corticosteroids and corticosteroids*time interaction terms as covariates into cause-specific Cox’s models and the overall corticosteroids effect was assessed by the likelihood ratio test.
Similarly, we investigated the association of corticosteroids with patient’s outcomes censored at day-28 (overall survival, MV duration, length of ICU stay) by using a Cox’s regression model with cause-specific hazard for MV duration (considering as event of interest extubation alive and death under MV as competing event) and for length of ICU stay (considering as event of interest ICU discharge alive, and death in ICU as competing event) [22]. Since there was no deviation on proportionality assumption, the corticosteroid effect was only modeled as a time-varying covariate without time-dependent coefficients.
In addition, we investigated the effect of the occurrence of VAP on the association between corticosteroid use and these outcomes by including in the models the VAP covariate and the corticosteroids x VAP interaction (both treated as time-varying covariates).
All associations were further investigated after adjustment for pre-specified confounders already known to be associated with VAP and patients’ outcomes (age, gender, BMI, SAPS II, MacCabe classification, immunosuppression, recent hospitalization, recent antibiotics, shock, ARDS and cardiac arrest). To avoid case-deletion in multivariate analyses due to presence of missing data in covariates, multivariable Cox’s models were performed after handling missing data by using a multiple imputation procedure [23]. Specifically, imputation of missing values was performed using a regression-switching approach (chained equations with m = 20 obtained) under the “missing at random” assumption, using all baseline characteristics (see Table 1) and outcomes, with a predictive mean matching method for quantitative variables and a logistic regression model (binary, ordinal or multinomial) for categorical variables. Estimates obtained in the different imputed data sets were combined using Rubin’s rules [24]. Sensitivity analysis on complete cases (patients without missing data on covariates) was also performed.
Statistical testing was performed with a two-tailed α level of 0.05. Data were analyzed using the SAS software package, release 9.4 (SAS Institute, Cary, NC). Statistical analysis is fully detailed in the online data supplement.
Results
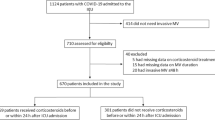
From March 2020 through May 2020, 568 patients receiving IMV > 48 h for SARS-CoV-2 pneumonia were eligible for this study. Twenty-three patients (4%) were excluded due to missing data. Among the 545 included patients, 191 (35%) received corticosteroids (Fig. 1).

Study flowchart
Patient characteristics at ICU admission
At ICU admission, the majority of patients were men with a median age of 64 year-old in corticosteroid and no-corticosteroid groups. Body mass index (BMI), SAPS II and SOFA scores, recent hospitalization (< 3 months) and recent antibiotic use (< 3 months) were comparable between both groups. In the corticosteroid group, the percentage of patients with immunosuppression was higher than in patients who did not receive corticosteroids. The main causes for ICU admission were acute respiratory failure and ARDS in both groups (Table 1).
Patient characteristics during ICU stay
Patient characteristics during ICU stay are presented in Table 2. Over 90% of patients in both groups had an antibiotic treatment during their ICU stay with a slightly longer duration of treatment in the corticosteroid group. Prone positioning was more frequent in patients who received corticosteroids than in those who did not. ECMO use was comparable in the two groups. 28-day mortality was higher in patients who received corticosteroids than in those who did not. Duration of MV and ICU length of stay were longer in the corticosteroid group than in the no-corticosteroid group.
In the corticosteroid group, patients mainly received methylprednisolone (48.1%) for a median time of 6 days (3–8 days) before occurrence of VAP. The highest daily dose of prednisone equivalent was 100 mg (50–133 mg).
Incidence of VAP and corticosteroid use
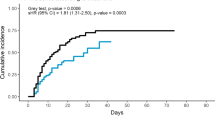
In the corticosteroid group, 74 (38.7%) patients developed at least one episode of VAP versus 138 (38.9%) patients in the no-corticosteroid group. As shown in Additional file 1: e-Fig. 1, the proportional hazard assumption for the effect of corticosteroids on the incidence of VAP, assessed by the scaled Schoenfeld residuals, revealed a time tendency indicating that this effect varied during ICU stay. By modeling the effect of corticosteroids with time-dependent coefficients, the association of corticosteroids with incidence of VAP was not significant before and after pre-specified adjustment (Table 3), with time-dependent adjusted hazard ratios (95% confidence interval) of 0.47 (0.17–1.31) at day 2, 0.95 (0.63–1.42) at day 7, 1.48 (1.01–2.16) at day 14 and 1.94 (1.09–3.46) at day 21. Similar results were found in sensitivity complete case analysis. Additional file 1: e-Table 1 depicts the association of different corticosteroids with VAP in all study patients.
Patient characteristics at the day of VAP and microbiological data
VAP episodes were mainly diagnosed with endotracheal aspirates in both groups. SOFA score, modified CPIS and PaO2/FiO2 ratio did not differ at the day of VAP between the two groups. Thirty-five (25%) patients had at least one VAP recurrence in the no-corticosteroids group versus 8 (11%) in the corticosteroids group. A higher percentage of patients received antibiotic treatment at the day of VAP in the corticosteroid group versus no-corticosteroid group (Table 4).
Gram-negative bacilli were the main bacteria responsible for VAP in the 2 groups (60%). Pseudomonas aeruginosa, Enterobacter spp. and Escherichia coli were the most frequently identified bacteria. A Higher proportion of VAP due to multidrug-resistant bacteria (MDR) was found in the corticosteroid-treated group (Table 5).
Impact of corticosteroid use on patient outcomes
Twenty-eight-day mortality was significantly associated with corticosteroid exposure in unadjusted analysis and after adjusting for pre-specified confounders in complete case analysis, and after multiple imputation analysis. In adjusted analysis, corticosteroid use was associated with prolonged duration of MV after multiple imputation analysis, but not with ICU length of stay (Table 3). Associations between different corticosteroids and VAP, 28-day mortality, MV duration and ICU length of stay are presented in e-Table 1
VAP occurrence did not significantly modify the relationship between corticosteroids and mortality, duration of MV, or length of ICU stay (Table 6). However, a significant association was found between corticosteroids exposure and ICU mortality in the absence of exposure to VAP. Twenty-eight-day cumulative incidence of VAP, all-cause mortality, extubation alive and ICU discharge alive are presented in Additional file 1: e-Fig. 2.
Discussion
In this ancillary study of the coVAPid study, we found no significant association between adjuvant corticosteroid treatment and the incidence of VAP in a population of SARS-CoV-2 patients invasively ventilated for over 48 h. However, we found a time-varying effect of corticosteroid adjuvant therapy on the incidence of VAP over the 28-day period.
The incidence of VAP in the SARS-CoV-2 population was high, nearly half of the patients presenting at least one VAP episode during ICU stay, irrespective of corticosteroid use. This result is in line with several previous studies that reported high incidence of VAP in critically ill COVID-19 patients [3, 8,9,10, 17].
Following the RECOVERY trial, corticosteroid adjuvant use dramatically increased in critically ill COVID-19 patients, although only 15% patients were invasively ventilated in this trial. In invasively ventilated COVID-19 patients, high rates of ARDS, prolonged ICU stay and IMV duration along with immunologic disorders and neuromuscular blocking agent use expose these patients to higher risk of developing VAP and one could question the impact of wide use of corticosteroids on the incidence of hospital-acquired infections (HAI) and VAP in this population, already at higher risk for these infections.
In COVID-19 patients, VAP is a serious complication, as our group and others demonstrated a significant association between VAP and mortality in this population [25, 26]. To date, there is no prospective interventional study that evaluated the impact of corticosteroid use on the incidence of VAP, as the RECOVERY study itself did not include it as an outcome. However, there is a growing body of evidence in the literature pointing out the increased risk of developing VAP in COVID-19 patients treated with corticosteroids [16,17,18,19, 27, 28].
A recent study by Mesland et al. [17]. reported, among 322 COVID-19 patients invasively ventilated, a significantly higher incidence for VA-LRTI in patients receiving corticosteroid adjuvant therapy compared with those who did not. Corticosteroids were found to be an independent factor associated with VA-LRTI in a multivariable adjusted analysis. Another recent study found the same association between corticosteroid use and VA-LRTI [18]. However, other studies suggested no association between corticosteroid exposure and the incidence of VA-LRTI in COVID-19 [15, 29].
In our study, we did not find a significant association between corticosteroid exposure and VAP incidence during the 28-day period of follow-up. However, our results suggest a trend toward a time-varying effect of corticosteroid exposure on the incidence of VAP. This time-varying effect increased all along the 28-day follow-up, and the association between corticosteroid use and VAP became statistically significant after the 14th day of mechanical ventilation. Several explanations could be provided for this time-varying effect. First, corticosteroid-immunosuppressive effect is a time-dependent but also a cumulative-dose-dependent mechanism [30] that may explain the late occurrence of hospital-acquired infections in treated patients. Second, sepsis-associated immunosuppression is a time-dependent process occurring in the late course of ICU stay, resulting in immunoparalysis and ICU-acquired infection [31, 32]. Finally, SARS-CoV-2-mediated immune dysfunction is associated with a progressive lymphopenia [33, 34], and a multifactorial immunosuppression culminating after day 14 [35] that exposes patients to late-onset ICU-acquired infection.
Our study reports higher 28-day mortality and longer MV duration in the group of patients who received adjuvant corticosteroid treatment, as compared to those who did not. The main reason for this discrepancy with results of randomized controlled trials [13, 36] might be the observational design of this study taking place before the RECOVERY era when corticosteroid prescriptions were at the discretion of attending physicians who selected the sickest patients to receive these treatments. Septic shock, non-resolving ARDS and intense systemic inflammation were the main reasons for corticosteroid adjuvant therapy, and this led de facto to a poorer prognosis in the corticosteroid-treated patients. Several other observational studies also failed to demonstrate this benefit from corticosteroids [17, 36].
Microorganisms responsible for VAP in our study did not differ between the corticosteroid treated and non-treated patients. In line with previous results, Gram-negative bacilli were the main bacteria found in respiratory tract samples with a high rate of Enterobacteriaceae and Pseudomonas aeruginosa. Methicillin-sensitive Staphylococcus aureus was the main Gram-positive cocci, and the rate of multidrug-resistant bacteria was also high [3, 15, 17].
To our knowledge, our study is the largest multicenter study to examine the impact of corticosteroid adjuvant therapy on the incidence of VAP in COVID-19 patients, and the first to show a varying association between corticosteroid use and the incidence of VAP. Additional strengths of our study are the large number of patients, the multicenter design and the strict definition of VAP with quantitative microbiological documentation for each event. However, some limitations should be mentioned. First, the observational retrospective design of our study taking place before the RECOVERY era is responsible for possible selection bias with disparate use of corticosteroids among centers that intentionally selected the sickest patients to receive corticosteroids, leading to poorer outcomes. Second, a small proportion of included patients (30%) received corticosteroids, which could also introduce a selection bias. Third, in our study we collected all steroid prescriptions irrespective of variations in molecule, duration and dosage. The impact of this discrepancy on patient outcomes might be real, yet no data support this in the literature.
Conclusions
We found no significant association between corticosteroid adjuvant therapy and the incidence of VAP in the population of invasively ventilated patients for a SARS-CoV-2 pneumonia. However, we found a time-varying effect of corticosteroid adjuvant therapy on the cause-specific estimated risk of developing VAP throughout patient course in ICU. Further studies are needed to clarify the role and effects of adjuvant corticosteroid treatment in the sickest COVID-19 patients. Future research should also investigate the interest of a corticosteroid-use strategy based on patient inflammatory phenotypes.
Availability of data and materials
All data needed to evaluate the conclusions in this article are present and tabulated in the main text or the appendix. This article is the result of an original retrospective cohort. For individual de-identified raw data that underlie the results reported in this article, please contact the corresponding authors.
Abbreviations
- ARDS:
-
Acute respiratory distress syndrome
- BMI:
-
Body mass index
- BSI:
-
Bloodstream infection
- CFU:
-
Colony-forming unit
- CPIS:
-
Clinical pulmonary infection score
- COVID-19:
-
Coronavirus disease 2019
- ECMO:
-
Extra corporeal membrane oxygenation
- HAI:
-
Hospital-acquired infection
- ICU:
-
Intensive care unit
- IMV:
-
Invasive mechanical ventilation
- PCR:
-
Polymerase chain reaction
- SAPS II:
-
Simplified Acute Physiology Score II
- SARS-CoV-2:
-
Severe acute respiratory syndrome coronavirus 2019
- SOFA:
-
Sequential Organ Failure Assessment
- VA-LRTI:
-
Ventilator-associated lower respiratory tract infection
- VAP:
-
Ventilator-associated pneumonia
- VAT:
-
Ventilator-associated tracheobronchitis
References
Wu C, Chen X, Cai Y, Xia J, Zhou X, Xu S, et al. Risk Factors associated with acute respiratory distress syndrome and death in patients with coronavirus disease 2019 pneumonia in Wuhan, China. JAMA Intern Med. 2020;180:934. https://doi.org/10.1001/jamainternmed.2020.0994.
Wang L, Zhou K-H, Chen W, Yu Y, Feng S-F. Epidemiology and risk factors for nosocomial infection in the respiratory intensive care unit of a teaching hospital in China: a prospective surveillance during 2013 and 2015. BMC Infect Dis. 2019;19:145. https://doi.org/10.1186/s12879-019-3772-2.
Grasselli G, Scaravilli V, Mangioni D, Scudeller L, Alagna L, Bartoletti M, et al. Hospital-acquired infections in critically Ill patients with COVID-19. Chest. 2021. https://doi.org/10.1016/j.chest.2021.04.002.
COVID-ICU Group on behalf of the REVA Network and the COVID-ICU Investigators. Clinical characteristics and day-90 outcomes of 4244 critically ill adults with COVID-19: a prospective cohort study. Intensive Care Med 2021;47:60–73. https://doi.org/10.1007/s00134-020-06294-x.
Maes M, Higginson E, Pereira-Dias J, Curran MD, Parmar S, Khokhar F, et al. Ventilator-associated pneumonia in critically ill patients with COVID-19. Crit Care. 2021;25:25. https://doi.org/10.1186/s13054-021-03460-5.
Luyt C-E, Bouadma L, Morris AC, Dhanani JA, Kollef M, Lipman J, et al. Pulmonary infections complicating ARDS. Intensive Care Med. 2020;46:2168–83. https://doi.org/10.1007/s00134-020-06292-z.
Giacobbe DR, Battaglini D, Enrile EM, Dentone C, Vena A, Robba C, et al. Incidence and prognosis of ventilator-associated pneumonia in critically Ill patients with COVID-19: a multicenter study. J Clin Med. 2021;10:555. https://doi.org/10.3390/jcm10040555.
on behalf of the coVAPid study Group, Rouzé A, Martin-Loeches I, Povoa P, Makris D, Artigas A, et al. Relationship between SARS-CoV-2 infection and the incidence of ventilator-associated lower respiratory tract infections: a European multicenter cohort study. Intensive Care Med 2021;47:188–98. https://doi.org/10.1007/s00134-020-06323-9.
Razazi K, Arrestier R, Haudebourg AF, Benelli B, Carteaux G, Decousser J, et al. Risks of ventilator-associated pneumonia and invasive pulmonary aspergillosis in patients with viral acute respiratory distress syndrome related or not to Coronavirus 19 disease. Crit Care. 2020;24:699. https://doi.org/10.1186/s13054-020-03417-0.
Hedberg P, Ternhag A, Giske CG, Strålin K, Özenci V, Johansson N, et al. Ventilator-associated lower respiratory tract bacterial infections in COVID-19 compared with non-COVID-19 patients*. Crit Care Med. 2022;50:825–36. https://doi.org/10.1097/CCM.0000000000005462.
Povoa P, Martin-Loeches I, Nseir S. Secondary pneumonias in critically ill patients with COVID-19: risk factors and outcomes. Curr Opin Crit Care. 2021;27:468–73. https://doi.org/10.1097/MCC.0000000000000860.
Tsitsiklis A, Zha BS, Byrne A, Devoe C, Levan S, Rackaityte E, et al. Impaired antibacterial immune signaling and changes in the lung microbiome precede secondary bacterial pneumonia in COVID-19. Respir Med. 2021. https://doi.org/10.1101/2021.03.23.21253487.
The RECOVERY Collaborative Group. Dexamethasone in hospitalized patients with Covid-19. N Engl J Med. 2021;384:693–704. https://doi.org/10.1056/NEJMoa2021436.
The WHO Rapid Evidence Appraisal for COVID-19 Therapies (REACT) Working Group, Sterne JAC, Murthy S, Diaz JV, Slutsky AS, Villar J, et al. Association Between Administration of Systemic Corticosteroids and Mortality Among Critically Ill Patients With COVID-19: A Meta-analysis. JAMA 2020;324:1330. https://doi.org/10.1001/jama.2020.17023.
Gragueb-Chatti I, Lopez A, Hamidi D, Guervilly C, Loundou A, Daviet F, et al. Impact of dexamethasone on the incidence of ventilator-associated pneumonia and blood stream infections in COVID-19 patients requiring invasive mechanical ventilation: a multicenter retrospective study. Ann Intensive Care. 2021;11:87. https://doi.org/10.1186/s13613-021-00876-8.
Martínez-Martínez M, Plata-Menchaca EP, Nuvials FX, Roca O, Ferrer R. Risk factors and outcomes of ventilator-associated pneumonia in COVID-19 patients: a propensity score matched analysis. Crit Care. 2021;25:235. https://doi.org/10.1186/s13054-021-03654-x.
Mesland J-B, Carlier E, François B, Serck N, Gerard L, Briat C, et al. Early corticosteroid therapy may increase ventilator-associated lower respiratory tract infection in critically Ill patients with COVID-19: a multicenter retrospective cohort study. Microorganisms. 2022;10:984. https://doi.org/10.3390/microorganisms10050984.
Søvik S, Barrat-Due A, Kåsine T, Olasveengen T, Strand MW, Tveita AA, et al. Corticosteroids and superinfections in COVID-19 patients on invasive mechanical ventilation. J Infect. 2022. https://doi.org/10.1016/j.jinf.2022.05.015.
Wolfe CR, Tomashek KM, Patterson TF, Gomez CA, Marconi VC, Jain MK, et al. Baricitinib versus dexamethasone for adults hospitalised with COVID-19 (ACTT-4): a randomised, double-blind, double placebo-controlled trial. Lancet Respir Med. 2022. https://doi.org/10.1016/S2213-2600(22)00088-1.
Martin-Loeches I, Povoa P, Rodríguez A, Curcio D, Suarez D, Mira J-P, et al. Incidence and prognosis of ventilator-associated tracheobronchitis (TAVeM): a multicentre, prospective, observational study. Lancet Respir Med. 2015;3:859–68. https://doi.org/10.1016/S2213-2600(15)00326-4.
Prentice RL, Kalbfleisch JD, Peterson AV, Flournoy N, Farewell VT, Breslow NE. The analysis of failure times in the presence of competing risks. Biometrics. 1978;34:541–54.
Austin PC, Lee DS, Fine JP. Introduction to the analysis of survival data in the presence of competing risks. Circulation. 2016;133:601–9. https://doi.org/10.1161/CIRCULATIONAHA.115.017719.
van Buuren S, Groothuis-Oudshoorn K. Mice: multivariate imputation by chained equations in R. J Stat Softw. 2011. https://doi.org/10.18637/jss.v045.i03.
Gladitz J. Rubin, Donald B.: Multiple Imputation for Nonresponse in Surveys. John Wiley & Sons, Chichester – New York – Brisbane – Toronto – Singapore 1987, xxx, 258 S., 6 Abb., £ 30.25, ISSN 0271-6232. Biom J 1989;31:131–2. https://doi.org/10.1002/bimj.4710310118.
Nseir S, Martin-Loeches I, Povoa P, Metzelard M, Du Cheyron D, Lambiotte F, et al. Relationship between ventilator-associated pneumonia and mortality in COVID-19 patients: a planned ancillary analysis of the coVAPid cohort. Crit Care. 2021;25:177. https://doi.org/10.1186/s13054-021-03588-4.
Vacheron C-H, Lepape A, Savey A, Machut A, Timsit JF, Comparot S, et al. Attributable Mortality of Ventilator-associated Pneumonia Among COVID-19 Patients. Am J Respir Crit Care Med. 2022. https://doi.org/10.1164/rccm.202202-0357OC.
Lamouche-Wilquin P, Souchard J, Pere M, Raymond M, Asfar P, Darreau C, et al. Early steroids and ventilator-associated pneumonia in COVID-19-related ARDS. Crit Care. 2022;26:233. https://doi.org/10.1186/s13054-022-04097-8.
Conway Morris A, Kohler K, De Corte T, Ercole A, De Grooth H-J, Elbers PWG, et al. Co-infection and ICU-acquired infection in COVID-19 ICU patients: a secondary analysis of the UNITE-COVID data set. Crit Care. 2022;26:236. https://doi.org/10.1186/s13054-022-04108-8.
Saade A, Moratelli G, Dumas G, Mabrouki A, Tudesq J-J, Zafrani L, et al. Infectious events in patients with severe COVID-19: results of a cohort of patients with high prevalence of underlying immune defect. Ann Intensive Care. 2021;11:83. https://doi.org/10.1186/s13613-021-00873-x.
Crabtree GR, Gillis S, Smith KA, Munck A. Mechanisms of glucocorticoid-induced immunosuppression: Inhibitory effects on expression of fc receptors and production of T-cell growth factor. J Steroid Biochem. 1980;12:445–9. https://doi.org/10.1016/0022-4731(80)90305-2.
Webster NR, Galley HF. Immunomodulation in the critically ill. Br J Anaesth. 2009;103:70–81. https://doi.org/10.1093/bja/aep128.
Monneret G, Venet F, Pachot A, Lepape A. Monitoring immune dysfunctions in the septic patient: a new skin for the old ceremony. Mol Med. 2008;14:64–78. https://doi.org/10.2119/2007-00102.Monneret.
Qin C, Zhou L, Hu Z, Zhang S, Yang S, Tao Y, et al. Dysregulation of immune response in patients with COVID-19 in Wuhan. China SSRN Electron J. 2020. https://doi.org/10.2139/ssrn.3541136.
Tan L, Wang Q, Zhang D, Ding J, Huang Q, Tang Y-Q, et al. Lymphopenia predicts disease severity of COVID-19: a descriptive and predictive study. Signal Transduct Target Ther. 2020;5:33. https://doi.org/10.1038/s41392-020-0148-4.
López-Collazo E, Avendaño-Ortiz J, Martín-Quirós A, Aguirre LA. Immune response and COVID-19: a mirror image of Sepsis. Int J Biol Sci. 2020;16:2479–89. https://doi.org/10.7150/ijbs.48400.
van Paassen J, Vos JS, Hoekstra EM, Neumann KMI, Boot PC, Arbous SM. Corticosteroid use in COVID-19 patients: a systematic review and meta-analysis on clinical outcomes. Crit Care. 2020;24:696. https://doi.org/10.1186/s13054-020-03400-9.
Acknowledgments
coVAPid Study Group
Mathilde Bouchereau (CHU de Lille, Centre de Réanimation, F-59000 Lille, France), Sean Boyd (Department of Intensive Care Medicine, Multidisciplinary Intensive Care Research Organization (MICRO), St.’James's Hospital, Dublin, Ireland), Luis Coelho (Polyvalent Intensive Care Unit, Hospital de São Francisco Xavier, CHLO, Lisbon, Portugal and NOVA Medical School, CHRC, New University of Lisbon, Portugal), Julien Maizel (Service de médecine intensive réanimation, CHU Amiens Picardie, 80000 Amiens, France), Pierre Cuchet (Department of Medical Intensive Care, Caen University Hospital, F-14000 Caen, France), Wafa Zarrougui (Service de réanimation polyvalente, Centre hospitalier de Valenciennes, Valenciennes, France), Déborah Boyer (Medical Intensive Care Unit, Rouen University Hospital, 76000 Rouen, France), Jean-Pierre Quenot (Department of Intensive Care, François Mitterrand University Hospital, Dijon, France), Mehdi Imouloudene (Service de réanimation et de soins intensifs, Centre hospitalier de Douai, France), Marc Pineton de Chambrun (Service de Médecine Intensive Réanimation, Institut de Cardiologie, Groupe Hospitalier Pitié-Salpêtrière, Assistance Publique – Hôpitaux de Paris Cedex 13, France), Thierry Van der Linden (Service de médecine intensive réanimation, Hôpital Saint Philibert GHICL, université catholique, Lille, France), François Arrive (CHU de Poitiers, Médecine Intensive Réanimation, CIC 1402 ALIVE France université de Poitiers, Poitiers, France), Sebastian Voicu (Department of Medical and Toxicological Critical Care, Lariboisière Hospital, INSERM UMRS-1144, Paris University, Paris, France), Elie Azoulay (Service de médecine intensive réanimation, Hôpital Saint-Louis, 75010 Paris, France), Edgard Moglia (Critical Care Department, Hospital Universitari Parc Taulí, Sabadell, Spain), Frédéric Pene (Medical Intensive Care Unit, Cochin Hospital, Assistance Publique – Hôpitaux de Paris, Paris, France), Catia Cilloniz (Department of Pulmonology, Hospital Clinic of Barcelona, University of Barcelona, IDIBAPS, CIBERES, Barcelona, Spain), Didier Thevenin (Service de réanimation polyvalente, Centre Hospitalier de Lens, Lens, France), Charlotte Larrat (Service de Médecine Intensive Réanimation CHU de Tours, Hôpital Bretonneau, 37044 Tours Cedex 9, France), Laurent Argaud (Service de Médecine Intensive - Réanimation, Hôpital Edouard Herriot, Hospices Civils de Lyon, 69437 Lyon Cedex 03, France), Bertrand Guidet (Service de Médecine Intensive Réanimation, Hôpital Saint-Antoine, Assistance Publique-Hôpitaux de Paris, 75012 Paris, France), Damien Contou (Service de réanimation polyvalente, CH Victor Dupouy, Argenteuil, France), Alexandra Beurton (Service de Médecine Intensive-Réanimation et Pneumologie, Assistance Publique-Hôpitaux de Paris, Hôpital Pitié Salpêtrière, France), David Meguerditchian (Service de médecine intensive réanimation, CHU de Bordeaux, F-33000 Bordeaux, France), Keyvan Razazi (Assistance Publique-Hôpitaux de Paris, Hôpitaux Universitaires Henri-Mondor, Service de Médecine Intensive Réanimation; Université Paris Est Créteil, CARMAS; INSERM U955, Institut Mondor de recherche Biomédicale; F-94010 Créteil, France), Vassiliki Tsolaki (Intensive Care Unit, University Hospital of Larissa, University of Thessaly, Biopolis Larissa, 41110 Greece), Mehdi Marzouk (Intensive Care Unit, Hôpital de Béthune, 62408 Béthune, France), Guillaume Brunin (Service de réanimation, Hôpital Duchenne, 62200 Boulogne-sur-Mer, France), Clémence Marois (Sorbonne Université, Assistance Publique-Hôpitaux de Paris, Sorbonne Université Hôpital de la Pitié-Salpêtrière, Département de Neurologie, Unité de Médecine Intensive Réanimation Neurologique, Paris, France), Luis Morales (Intensive Care Unit, Hospital Unive rsitari Sagrat Cor, Barcelona, Spain)
Funding
This study was supported in part by a grant from the French government through the « Programme Investissement d’Avenir» (I-SITE ULNE) managed by the Agence Nationale de la Recherche (coVAPid project). Prof. Ignacio Martin-Loeches has been supported by SFI (Science Foundation Ireland), Grant number 20/COV/0038. The funders of the study had no role in the study design, data collection, analysis or interpretation, writing of the report or decision to submit for publication.
Author information
Authors and Affiliations
Consortia
Contributions
OS, AR, IML, PP, AD, JL and SN contributed to conception and design of the study. All authors were involved in data acquisition. OS, AR, IML, PP, AT, LK, AD, JL and SN contributed to data analysis and interpretation. All authors were involved in manuscript drafting or critical revision for important intellectual content. All authors contributed to final approval of the submitted version. SN was guarantor of the paper.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The Ethics Committee and Institutional Review Boards approved the study protocol (Comité de Protection des Personnes Ouest VI; approved by April 14, 2020; registration number RIPH:20.04.09.60039) as minimal-risk research using data collected for routine clinical practice and waived the requirement for informed consent.
Competing interests
AR received personal fees from Maat Pharma, and IML received personal fees from MSD and Gilead. AA received personal fees from Lilly Foundation and grants from Grifols and Fisher & Paykel. CEL received personal fees from Bayer, Merck, Aerogen, bioMérieux, ThermoFisher Brahms and Carmat. SN received personal fees from MSD, Bio Rad, bioMérieux, Gilead, Fisher & Paykel and Pfizer. All other authors declare no competing interests.
Consent for publication
Not applicable.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Supplementary e-figures and e-tables.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Saura, O., Rouzé, A., Martin-Loeches, I. et al. Relationship between corticosteroid use and incidence of ventilator-associated pneumonia in COVID-19 patients: a retrospective multicenter study. Crit Care 26, 292 (2022). https://doi.org/10.1186/s13054-022-04170-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13054-022-04170-2