
Abstract
Background
Treatment and the clinical course during Emergency Department (ED) stay before Intensive Care Unit (ICU) admission may affect predicted mortality risk calculated by the Acute Physiology and Chronic Health Evaluation (APACHE)-IV, causing lead-time bias. As a result, comparing standardized mortality ratios (SMRs) among hospitals may be difficult if they differ in the location where initial stabilization takes place. The aim of this study was to assess to what extent predicted mortality risk would be affected if the APACHE-IV score was recalculated with the initial physiological variables from the ED. Secondly, to evaluate whether ED Length of Stay (LOS) was associated with a change (delta) in these APACHE-IV scores.
Methods
An observational multicenter cohort study including ICU patients admitted from the ED. Data from two Dutch quality registries were linked: the Netherlands Emergency department Evaluation Database (NEED) and the National Intensive Care Evaluation (NICE) registry. The ICU APACHE-IV, predicted mortality, and SMR based on data of the first 24 h of ICU admission were compared with an ED APACHE-IV model, using the most deviating physiological variables from the ED or ICU.
Results
A total of 1398 patients were included. The predicted mortality from the ICU APACHE-IV (median 0.10; IQR 0.03–0.30) was significantly lower compared to the ED APACHE-IV model (median 0.13; 0.04–0.36; p < 0.01). The SMR changed from 0.63 (95%CI 0.54–0.72) to 0.55 (95%CI 0.47–0.63) based on ED APACHE-IV. Predicted mortality risk changed more than 5% in 321 (23.2%) patients by using the ED APACHE-IV. ED LOS > 3.9 h was associated with a slight increase in delta APACHE-IV of 1.6 (95% CI 0.4–2.8) compared to ED LOS < 1.7 h.
Conclusion
Predicted mortality risks and SMRs calculated by the APACHE IV scores are not directly comparable in patients admitted from the ED if hospitals differ in their policy to stabilize patients in the ED before ICU admission. Future research should focus on developing models to adjust for these differences.
Similar content being viewed by others
Background
The Acute Physiology and Chronic Health Evaluation (APACHE)-IV is a scoring system used for risk stratification of Intensive Care Unit (ICU)-patients [1, 2]. The APACHE-IV is also used for case-mix correction when comparing outcomes of patients in national and international research or quality improvement projects.
The acute physiology score (APS), part of the APACHE-IV model, uses the most deviated vital signs and laboratory results measured in the first 24 h after ICU admission [1, 3]. However, physiological parameters may improve or deteriorate in the hours before ICU admission [4,5,6,7], e.g., during initial treatment in the emergency department (ED) or because of deterioration in the clinical course. These data measured prior to ICU admission are not included in the original APACHE-IV scores [1, 3]. Consequently, the calculated severity of illness and predicted mortality risk may differ when for a given patient the same initial treatment is given before or after ICU admission or if the ED stay is shorter resulting in a different clinical course, a phenomenon called lead-time bias in the literature [8, 9]. For appropriate risk stratification and case-mix correction, it is essential to understand whether there is an effect of ED treatment on the APACHE-IV scores.
The present study assessed if, and to what extent, the APACHE-IV score and predicted mortality risk change if the APACHE-IV is recalculated, including data from both the pre-ICU ED period and the first 24 h of ICU treatment. In this way we evaluated if earlier findings from a very small sample could be confirmed [9]. Our second aim was to assess whether ED treatments (e.g., the amount of fluid administered) and clinical course during ED stay were associated with changes in the APACHE-IV score, predicted mortality risk, and standardized mortality ratio (SMR).
Methods
Study design and setting
This was an observational multicenter cohort study using the Netherlands Emergency department Evaluation Database ((NEED), http://www.stichting-need.nl) and the National Intensive Care Evaluation (NICE) registry [10]. Data were available from two urban teaching hospitals (Medical Center Leeuwarden, 14 October 2017–31 July 2020 and Catharina Hospital Eindhoven, 01 January 2019–01 July 2020). In both hospitals, patients were treated and stabilized in the ED before ICU admission by emergency physicians with or without consultation of an intensivist. If necessary, mechanical ventilation was started in the ED. Patients were almost never intubated prehospital because hospitals can be reached within 15 min by ambulance in both regions in the Netherlands. The medical ethical committee of Máxima MC reviewed the research proposal and concluded that the anonymized data were not subject to the Dutch Research on Humans Subjects Act (in Dutch “WMO”) and waived the need for informed consent (registration number N20.117).
Patient selection
All ICU patients who were directly admitted from the ED in the mentioned study period were included. Patients transferred to other hospitals and patients without any registered vital signs or laboratory results (9 patients) in the NEED were excluded.
Data collection
Data from the NICE
The NICE is the national quality registry founded in 1996 in which all ICUs in the Netherlands have participated since 2016 [11]. Data available from NICE were: Age, sex, date of admission, ICU length of stay, ICU mortality, hospital mortality, and all data to calculate the APACHE-IV score [1, 12]. Additional file 1 shows which variables were extracted from the NICE and from the NEED to calculate the APACHE-IV score. Only the lowest and the highest values of vital signs and laboratory tests in the first 24 h of ICU admission were registered in the NICE. The NICE registry uses strict definitions and specifications of the data collected, described in a data dictionary (https://www.stichting-nice.nl/dd/). The NICE provides participants a mandatory training and performs automated checks on data entry and regular on-site quality audits [11, 13].
Data from the NEED
The NEED is the quality registry for EDs in the Netherlands (http://www.stichting-need.nl), founded in 2016. For the present study, data were available from two hospitals. Only the first set of vital signs and laboratory results were registered in the NEED, measured before ED treatment, described in detail previously [14]. Except for variables to calculate the APACHE-IV score (Additional file 1), patient characteristics (e.g., triage category according to the Dutch Triage System or Manchester Triage Standard, presenting complaints, diagnostics (Y/N), fluid administration), and ED- length of stay (LOS) were extracted.
Linking of NEED and NICE databases
Both NEED and NICE have unique identifying patient numbers that are not identical. In the NICE, patients were selected who were admitted from the ED. In the NEED, patients were selected who were admitted to a high dependency care unit. If the following variables were identical between both databases, patient variables were linked: Date of ED admission (in the NEED) and the date of ICU admission (in the NICE), hospital location, sex, and age of the patient. In addition, for records in NICE with ED as resource but without linkage to a NEED record, the date of ED admission could be one day earlier than the date of ICU admission. These patients were linked by changing the data of ED presentation to one day earlier.
Outcome measures
Outcome measures were the original ICU APACHE-IV score (Formally the APACHE III score used in the APACHE IV model [1, 3]) and predicted mortality using the most deviated physiological variables from the first 24 h after ICU admission, and the ED APACHE-IV score using the most deviated values from ED admission until 24 h after ICU admission. The SMR is the ratio between the observed number of deaths and the expected deaths in the ICU using the original (ICU model) or modified (ED model) predicted mortality risks. The delta APACHE-IV was calculated as the ED APACHE-IV score–ICU APACHE-IV score.
Data and data analyses
Descriptive statistics
Data are presented as mean with standard deviation (SD) if normally distributed and as median with interquartile range (IQR) if skewed. Categorical data are presented as frequencies (%).
Main statistical analyses
In our study, the ICU APACHE-IV score was compared with a recalculated APACHE IV score, called the ED APACHE-IV. According to the original model, the ICU APACHE-IV score was calculated with the most deviating vital signs or blood tests in the first 24 h of ICU admission [3]. Points were assigned for the value that was furthest from a reference value. For example, for heart rate the reference value was 75 bpm. Reference values for all other variables are shown in Additional file 2. According to the APACHE IV definitions [3], more deviating vital signs or laboratory results do not necessarily result in a higher score (see Additional file 2). Based on rules of the original APACHE-IV model, missing physiological variables were considered normal. The ED APACHE-IV included the most deviating vital signs and blood tests from ED admission until 24 h after ICU admission. The data available from the NEED registry to calculate the ED APACHE-IV are described in Additional file 1. The acute physiological variables were recalculated, all other variables in the ED APACHE-IV remained identical to the ICU APACHE-IV (e.g., the Chronic Health Conditions). Urine output and mechanical ventilation (Y/N) were not registered in the NEED. Patients were considered not to be intubated at ED arrival. In the ED, venous blood gas is often obtained instead of an arterial blood gas. If no arterial blood gas was available, the pH from the venous blood gas analysis was used with a correction of 0.03, and the pCO2 was used with a correction of − 4.8 mmHg [15]. PaO2 is not well correlated between venous and arterial blood gas and was therefore considered missing if not available as arterial value. Predicted mortality risks were calculated for the ED APACHE-IV using the Beta’s of the ICU APACHE-IV logistic model. The APACHE-IV scores, Acute Physiology Score (APS), and predicted mortality risks were compared between the ICU and ED model with a Wilcoxon Signed Rank test. In addition, we assessed the discriminative performance of both the ICU and ED APACHE-IV model using a receiver operator characteristic (ROC) curve with area under the curve (AUC) analysis and in-hospital mortality as outcome. Calibration plots for both models were presented.
For our second aim, delta APACHE-IV was calculated (e.g., ED APACHE-IV–ICU APACHE-IV). Delta APACHE-IV was normally distributed, and therefore, univariable and multivariable linear regression analyses were performed to assess the association between ED LOS, fluid administration (0 ml, 0-500 ml, > 500 ml) as independent variables, and a delta APACHE-IV as dependent variable. ED-LOS was divided into quartiles (0–1.7 h, 1.7–2.7 h, 2.7–3.9 h, > 3.9 h). Because of a strong correlation between ED LOS and fluid administration, separate models were used. The following potential confounders were included in both multivariable models: Age, gender, hospital, and the ED APACHE-IV score. Although age is one of the variables included in the APACHE-IV, age may still be an independent predictor for delta APACHE-IV. Fluid administration and ED LOS were included as dummy variables to overcome nonlinear associations. The unstandardized coefficients (Beta's) were presented with 95% Confidence Intervals (95%-CI).
To study whether the ED APACHE-IV was significantly different per quartile ED-LOS, a Kruskal Wallis Test was used.
A p value < 0.05 was considered statistically significant. SPSS version 25.0 was used for all data analyses.
Results
Patient characteristics
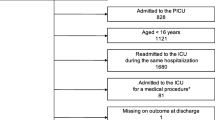
During the study period, 1730 patients were admitted from the ED to the ICU. In total, 1398 (80.8%) patients were included after linking both databases (see Fig. 1). The median age was 64 years (50-74 years), a total of 1046 (60.5%) were male patients. Patient characteristics, including all APS variables, are described in Table 1. Characteristics of patients who could not be linked between both databases (N = 323) are comparable with the included patients and are described in Additional file 3. The median laboratory values in the ED were comparable with the lowest and highest values from the ICU. Additional file 4 describes other patient characteristics, such as the triage category in the ED, and the most common presenting complaints in the ED and reasons for ICU admissions.

Patient flow diagram throughout the study. Patients from the National Intensive Care Evaluation (NICE) registry were linked with patients from the Netherlands Emergency department Evaluation Database (NEED)
The ED APACHE-IV score
Including the most deviating vital signs and blood tests from ED admission until 24 h after ICU admission, the median ED APACHE-IV score (63; IQR 47–90) was calculated and differed significantly from the median ICU APACHE-IV score (56; IQR 39–80) (p value < 0.01). The median predicted mortality for the total population was higher for the ED APACHE-IV system, 0.13 (IQR 0.04–0.36) versus 0.10 (IQR 0.03–0.30) (see Table 2). Observed in-hospital mortality was 13.4% (N = 188). The SMR decreased from 0.63 (95% CI 0.54–0.72) for the ICU APACHE-IV model to 0.55 (95% CI 0.47–0.63) for the ED APACHE-IV model, a relative difference of 12.7%.
Both APACHE-IV models had an identical AUROC of 0.91 (95% CI 0.89–0.93) and 0.91 (95% CI 0.89–0.93). Calibration plots for both models were comparable (Additional file 5). The ED APACHE-IV score increased in 1075 (77.2%) patients, decreased in 33 (2.4%) patients, and remained unaltered in 284 (20.4%) patients. Predicted mortality increased ≥ 5.0% in 320 (23.1%) patients and decreased ≥ 5.0% in 1 (0.1%) patient (see Additional file 6). Higher ICU APACHE-IV scores had larger changes in predicted mortality risks if modified with ED variables.
ED Length of stay and delta APACHE-IV score
To study whether the ED LOS was associated with a delta APACHE-IV score (= ED APACHE-IV–ICU APACHE-IV), the ED APACHE-IV score and the delta APACHE-IV are presented per ED LOS quartile (Fig. 2). As assessed with a multivariable linear model, more fluid administration in the ED was associated with a significant adjusted increase in delta APACHE-IV (p value = 0.04) (see Table 3). Compared to those with an ED LOS < 1.7 h, among patients with ED LOS > 3.9 h the delta-APACHE was on average 1.6 points (95% CI 0.4–2.8) higher.

In panel A the median Emergency Department Acute Physiology and Chronic Health Evaluation (ED APACHE-IV) score is presented per quartile Emergency Department Length of Stay (ED-LOS), with 95% Confidence intervals. The ED APACHE-IV score uses the most deviated physiological variables from ED admission until 24 h after ICU admission, which differs from the ICU APACHE-IV score which only contains the most deviated physiological variables from the first 24 h of ICU admission. Panel B shows the mean delta APACHE-IV per quartile ED-LOS. The delta APACHE-IV is calculated as follows: ED APACHE-IV score—ICU APACHE-IV score
The median APACHE-IV score differed per quartile ED LOS (p < 0.01) calculated with the Kruskal Wallis Test.
Discussion
The present study shows that in ICU patients admitted from the ED, the average calculated severity of illness and predicted mortality risks are substantially higher, and the SMR is lower if not only data from the first 24 h of ICU stay are used to calculate the APACHE-IV score, but also the data from the ED. In our population, the mean increase in APACHE IV score was 13%, with a mean increase in predicted mortality risk of 30% and a decrease in SMR of 13%.
Our results are in accordance with an earlier study of 76 ICU patients admitted from the ED and operating rooms [9]. In this study, higher APACHE II, APACHE III, and SAPS II scores were found if calculated with data from 6 h before ICU referral to 24 h after ICU admission compared with the standard period from ICU admission to 24 h after ICU admission. Consequently, including pre-ICU data leads to higher severity of illness scores. This can be explained by the fact that the period to choose the most deviating physiological variables becomes longer.
It may be argued that this influence of pre-ICU data on the assessment of severity of illness and predicted mortality has no major consequences, because the 24 h time period for data collection is clearly defined and similar for ICUs all over the world. Thus, APACHE scores and mortality predictions would be well comparable for describing case-mix and outcomes between ICUs (benchmarking). However, the true importance of our findings lies in the fact that major differences exist in the location where initial stabilization of patients takes place. For example, patients with septic shock are stabilized in the ED in some hospitals [16], whereas they would be transferred immediately to the ICU in other hospitals [8, 17, 18]. Especially in the early phase of stabilization, physiological parameters may be very disturbed leading to high APACHE scores. Because the APACHE prognostic scores are calculated from data exclusively from the first 24 h after ICU admission, this would contribute to higher APACHE scores and predicted mortality if stabilization took place in the ICU, but not if performed in the ED. Calculated severity of illness with the APACHE-IV score and predicted mortality risk will be lower in hospitals where patients are routinely stabilized in the ED before transfer to the ICU, compared to hospitals where patients are immediately transferred from the ED to the ICU and stabilized there [18]. As a result, the higher calculated SMRs may be falsely interpreted as a difference in the quality of care, while they can be fully explained by the fact that only data from the ICU are used for scoring. In our population, we found a substantial difference in SMR of 0.63 versus 0.55 depending on using or not using the ED data. In ICU literature this occurrence is referred to as lead-time bias [8, 9].
Our findings imply that whenever the quality of care among ICUs is compared using the SMR, a correction should be applied, or a margin of error of approximately 13% should be used if hospitals differ in their policy to stabilize patients. Our study was performed only in patients admitted to the ICU from the ED. However, in patients admitted from the operating rooms, wards, or in patients transferred from other hospitals, comparable differences in measured severity of illness and SMRs may be found if policies in stabilizing patients differ [8].
In the ICU APACHE-IV model, the calculated predicted mortality risk is already adjusted for the source of admission, e.g., from the ED. However, this adjustment does not correct for the influence of initial stabilization in either the emergency department or the ICU. In both situations, the patient is admitted from the ED with identical adjustment for source of admission. Future studies should investigate whether the APACHE-IV model could be improved to account for differences in hospital policy to stabilize patients.
We show that patients with higher ICU APACHE-IV scores had a larger absolute difference in predicted mortality compared to patients with a lower ICU APACHE-IV score. This may be explained by more intense resuscitative treatments in the ED. Unfortunately, the data available about therapies started in the ED were limited to only fluid therapy.
Small increases in delta APACHE-IV were found with more fluid administration in the ED and with an ED LOS of > 3.9 h. We can only speculate why a longer ED LOS led to a larger difference in APACHE-IV. Likely, patients with a prolonged ED LOS got more treatments in the ED, such as fluid administration, but also unregistered resuscitative therapies, which caused bigger changes in physiological signs than in patients who had a short ED LOS. However, we expected to find larger differences between the ICU APACHE-IV and ED APACHE-IV with more intensive ED treatment and a longer ED LOS. Nonetheless, this study analyzed a selective group of patients from the ED who may not have responded sufficiently to therapy and therefore may have been admitted to the ICU. This selection of ED patients may explain why we found only small increases in delta APACHE-IV in patients with a prolonged ED LOS.
Despite several strengths like the sample size and the multicenter design, our study also has some limitations. First, in approximately 18% of patients admitted from the ED to the ICU, no ED data were available. Patients could not be linked between databases for various reasons: i.e., transfers to other hospitals, patients who first went for surgery and not directly to the ICU, patients who bypassed the ED and went for coronary intervention, and possible registration problems. We cannot exclude that this may lead to some selection bias. Nonetheless, patient characteristics and mortality of patients who could not be linked between both databases were comparable with characteristics of included patients. Also, in our ED database, only initial values from ED admission were present. It may well be that even more deviating values could have been measured during ED treatment. Therefore, our findings likely underestimate the actual so-called lead-time bias in our patients. Furthermore, in our study, we did not include patients admitted to the ICU from an ED in another hospital. In those cases, the period between ED admission and ICU admission is prolonged, which potentially leads to more considerable differences in calculated APACHE IV scores and thus more lead-time bias [8].
Conclusions
In summary, including the initial vital signs and laboratory results from the ED in the APACHE-IV score changed the predicted mortality risk and SMR, highlighting the influence of treatment given at the ED prior to IC admission. In addition, a longer ED LOS was associated with an increase in delta APACHE IV score, leading to a spuriously high SMR when this is not considered. Our findings are essential when comparing hospitals regarding quality of care and case-mix adjusted outcomes. APACHE IV scores and SMRs are not directly comparable in patients admitted from the ED if hospitals differ in their policy to stabilize patients in the ED before ICU admission. Future research should focus on refining models to adjust for these differences.
Take home message
-
The average calculated severity of illness and predicted mortality risks are substantially higher, and the SMR is 13% lower if not only data from the first 24 h of ICU stay are used to calculate the APACHE-IV score, but also the data from the ED.
-
Predicted mortality risks and SMRs calculated by the APACHE IV scores are not directly comparable in patients admitted from the ED if hospitals differ in their policy to stabilize patients in the ED before ICU admission.
Availability of data and materials
Data are available from the corresponding author upon reasonable request.
Change history
11 May 2022
A Correction to this paper has been published: https://doi.org/10.1186/s13054-022-04008-x
Abbreviations
- APACHE:
-
Acute Physiology and Chronic Health Evaluation
- AUROC:
-
Area Under the Receiving Operating Characteristics
- ED:
-
Emergency Department
- ICU:
-
Intensive Care Unit
- IQR:
-
Interquartile Range
- LOS:
-
Length of Stay
- NEED:
-
The Netherlands Emergency department Evaluation Database
- NICE:
-
National Intensive Care Evaluation
- SD:
-
Standard deviation
- SMR:
-
Standardized Mortality Ratio
References
Zimmerman JE, Kramer AA, McNair DS, Malila FM. Acute Physiology and Chronic Health Evaluation (APACHE) IV: hospital mortality assessment for today’s critically ill patients. Crit Care Med. 2006;34(5):1297–310.
Bouch DC, Thompson JP. Severity scoring systems in the critically ill. Continu Educ Anaesthesia Crit Care Pain. 2008;8(5):181–5.
Knaus WA, Wagner DP, Draper EA, Zimmerman JE, Bergner M, Bastos PG, et al. The APACHE III prognostic system: risk prediction of hospital mortality for critically III hospitalized adults. Chest. 1991;100(6):1619–36.
Buist M, Bernard S, Nguyen TV, Moore G, Anderson J. Association between clinically abnormal observations and subsequent in-hospital mortality: a prospective study. Resuscitation. 2004;62(2):137–41.
Considine J, Jones D, Bellomo R. Emergency department rapid response systems: the case for a standardized approach to deteriorating patients. Eur J Emerg Med. 2013;20(6):375–81.
Flabouris A, Hart GK, George C. Outcomes of patients admitted to tertiary intensive care units after interhospital transfer: comparison with patients admitted from emergency departments. Crit Care Resusc. 2008;10(2):97–105.
Simpson H, Clancy M, Goldfrad C, Rowan K. Admissions to intensive care units from emergency departments: a descriptive study. Emerg Med J. 2005;22(6):423–8.
Dragsted L, Jörgensen J, Jensen N-H, Bönsing E, Jacobsen E, Knaus WA, et al. Interhospital comparisons of patient outcome from intensive care: importance of lead-time bias. Crit Care Med. 1989;17(5):418–22.
Tunnell R, Millar B, Smith G. The effect of lead time bias on severity of illness scoring, mortality prediction and standardised mortality ratio in intensive care—a pilot study. Anaesthesia. 1998;53(11):1045–53.
van de Klundert N, Holman R, Dongelmans DA, de Keizer NF. Data resource profile: the Dutch National Intensive Care Evaluation (NICE) registry of admissions to adult intensive care units. Int J Epidemiol. 2015;44(6):1850-h.
Arts D, de Keizer N, Scheffer G-J, de Jonge E. Quality of data collected for severity of illness scores in the Dutch National Intensive Care Evaluation (NICE) registry. Intensive Care Med. 2002;28(5):656–9.
Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a severity of disease classification system. Crit Care Med. 1985;13(10):818–29.
Koetsier A, Peek N, De Keizer N. Identifying types and causes of errors in mortality data in a clinical registry using multiple information systems. Quality of Life through Quality of Informations. Amsterdam: IOS Press; 2012. p. 771–5.
Candel BG, Duijzer R, Gaakeer MI, Ter Avest E, Sir Ö, Lameijer H, et al. The association between vital signs and clinical outcomes in emergency department patients of different age categories. Emerg Med J. 2022.
Zeserson E, Goodgame B, Hess JD, Schultz K, Hoon C, Lamb K, et al. Correlation of venous blood gas and pulse oximetry with arterial blood gas in the undifferentiated critically ill patient. J Intensive Care Med. 2018;33(3):176–81.
Rivers E, Nguyen B, Havstad S, Ressler J, Muzzin A, Knoblich B, et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med. 2001;345(19):1368–77.
Pappachan JV, Millar B, Bennett ED, Smith GB. Comparison of outcome from intensive care admission after adjustment for case mix by the APACHE III prognostic system. Chest. 1999;115(3):802–10.
Gunnerson KJ, Bassin BS, Havey RA, Haas NL, Sozener CB, Medlin RP, et al. Association of an emergency department–based intensive care unit with survival and inpatient intensive care unit admissions. JAMA Network Open 2019;2(7):e197584-e.
Acknowledgements
Not applicable.
Funding
No funding.
Author information
Authors and Affiliations
Contributions
BC, EDJ and BDG devised and designed the study. BC, NDK, and FT collected data and analyzed data. BC, EDJ and BDG wrote the manuscript. HL, WT and BDG are founders of the NEED, collected data and edited the manuscript. EDJ, NDK, FT and WR edited the manuscript. BdG takes full responsibility for the study. All authors have read and approved the manuscript.
Corresponding author
Ethics declarations
Ethical approval and consent to participate
The medical ethical committee of Máxima MC reviewed the research proposal and concluded that the anonymized data were not subject to the Dutch Research on Humans Subjects Act (in Dutch “WMO”) and waived the need for informed consent (registration number N20.117).
Consent or publication
Not applicable.
Competing interests
All authors declare no conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original online version of this article was revised: the authors identified an error in the author name Fabian Termorshuizen. The family name contained an error.
Supplementary Information
Additional file 1
. A table with variables is shown including the variables that are extracted from the NICE (Intensive Care database) and the NEED (The Emergency Department database) to calculate the Acute Physiology Score, as part of the Acute Physiology and Chronic Health Evaluation (APACHE)-IV.
Additional file 2
. This file describes how points are given for each physiological parameter to calculate the Acute Physiology Score as part of the Acute Physiology and Chronic Health Evaluation (APACHE)-IV.
Additional file 3
. Patient characteristics of excluded patients who could not be linked with the Netherlands Emergency department Database (N = 323).
Additional file 4
. Additional patient characteristics including triage categories, top five presenting complaints, top seven reasons for admission to the ED, diagnostics in the ED and fluid administration.
Additional file 5
. Calibration plots for both the ICU APACHE-IV score and the ED APACHE-IV score
Additional file 6
. The change in predicted mortality for individual patients is presented if the ED Acute Physiology and Chronic Health Evaluation (APACHE)-IV is compared to the ICU APACHE-IV score.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visithttp://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Candel, B.G.J., Raven, W., Lameijer, H. et al. The effect of treatment and clinical course during Emergency Department stay on severity scoring and predicted mortality risk in Intensive Care patients. Crit Care 26, 112 (2022). https://doi.org/10.1186/s13054-022-03986-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13054-022-03986-2