
Abstract
Objective
To compare colorectal cancer (CRC) incidences in carriers of pathogenic variants of the MMR genes in the PLSD and IMRC cohorts, of which only the former included mandatory colonoscopy surveillance for all participants.
Methods
CRC incidences were calculated in an intervention group comprising a cohort of confirmed carriers of pathogenic or likely pathogenic variants in mismatch repair genes (path_MMR) followed prospectively by the Prospective Lynch Syndrome Database (PLSD). All had colonoscopy surveillance, with polypectomy when polyps were identified. Comparison was made with a retrospective cohort reported by the International Mismatch Repair Consortium (IMRC). This comprised confirmed and inferred path_MMR carriers who were first- or second-degree relatives of Lynch syndrome probands.
Results
In the PLSD, 8,153 subjects had follow-up colonoscopy surveillance for a total of 67,604 years and 578 carriers had CRC diagnosed. Average cumulative incidences of CRC in path_MLH1 carriers at 70 years of age were 52% in males and 41% in females; for path_MSH2 50% and 39%; for path_MSH6 13% and 17% and for path_PMS2 11% and 8%. In contrast, in the IMRC cohort, corresponding cumulative incidences were 40% and 27%; 34% and 23%; 16% and 8% and 7% and 6%. Comparing just the European carriers in the two series gave similar findings. Numbers in the PLSD series did not allow comparisons of carriers from other continents separately. Cumulative incidences at 25 years were < 1% in all retrospective groups.
Conclusions
Prospectively observed CRC incidences (PLSD) in path_MLH1 and path_MSH2 carriers undergoing colonoscopy surveillance and polypectomy were higher than in the retrospective (IMRC) series, and were not reduced in path_MSH6 carriers. These findings were the opposite to those expected. CRC point incidence before 50 years of age was reduced in path_PMS2 carriers subjected to colonoscopy, but not significantly so.
Similar content being viewed by others

Background
In 1995, a study in Finland found that colonoscopy with polypectomy conducted every three to five years was associated with a reduced CRC incidence in Lynch syndrome (LS) when compared to LS patients who did not have colonoscopy [1]. It was stated that ‘The recommended surveillance protocol for HNPCC is based on the hypothesis that the adenoma-carcinoma sequence, which is generally accepted in sporadic colorectal cancer, is also applicable in HNPCC’ [2] and relatives of LS cases were thereafter widely subjected to surveillance with colonoscopy every three years. However, continued occurrence of CRC was noted despite this surveillance and, in response, the recommended interval between colonoscopies was reduced [3, 4]. Despite this change, continuing occurrence of CRC was still observed and in some centres the interval between colonoscopies was therefore reduced further, to one year [5] or even less. Surprisingly, since the initial Finnish report in 1995 that did not control for lead-time bias and was not randomized, there has been no confirmatory study to show that colonoscopy surveillance with polypectomy significantly reduces CRC incidence in LS.
The earliest published reports of LS families [6] suggest that in previous generations, most individuals who developed a first cancer died from that cancer. By contrast, more recently, LS patients diagnosed with a non-colorectal cancer at a young age usually survive and often develop CRC later in life [7]. The extent to which this time-trend (survivor bias) has influenced the outcomes of interventions that aim to prevent occurrence of CRC and improve its prognosis through early detection and treatment, is not known.
No single institution nor country had the resources needed to resolve these issues, leading the European Hereditary Tumour Group in 2012 (www.ehtg.org, that at the time was known as the Mallorca group) to invite pooling of international results of prospective follow-up of LS families in a single shared database, the Prospective Lynch Syndrome Database (PLSD). The goal of PLSD was to describe cancer incidences in all organs in carriers of path_MMR variants who were undergoing follow-up according to the internationally advocated clinical guidelines and to stratify these by age, gene and gender. Once sufficient numbers of carriers and follow-up years were collated, the intention was to use the information obtained to assess whether the results were compatible with current assumptions about carcinogenesis and the expected effects of interventions in LS. This paper reports the results of one such assessment. Because neither randomized trials of colonoscopy versus no-colonoscopy, nor open trials with a non-intervention control arm are likely to be undertaken in LS, a separate goal of PLSD is to produce the information needed to inform development of alternative randomized trials, for example of different surveillance intervals, in the future.
Around the same time as the PLSD was developed, an initiative aiming to compile data on as many LS families as possible for a retrospective segregation analysis was established by the International Mismatch Repair Consortium (IMRC) (https://www.sphinx.org.au/imrc ). Its primary aim was to determine the cumulative CRC incidences in path_MMR carriers by retrospective analysis including family members in former generations who were not subject to the same degree of CRC preventive surveillance with colonoscopy as contemporary patients followed in PLSD [5].
There is limited information on survival following CRC detected during surveillance with colonoscopy in path_MMR carriers, other than reports from the PLSD [8] and the recent IMRC report did not include data on survival [5].
Here, we compare prospective CRC incidences in an updated version of PLSD that includes 8,153 path_MMR carriers aged from 25 to 70 years and subjected to regular follow-up with colonoscopy for a total of 67,604 years with retrospective CRC incidences calculated from path_MMR carriers from 5,255 families collected by the IMRC.
Methods
The PLSD compiles observed cancers in path_MMR carriers from the first prospectively planned and performed colonoscopy. It considers all cancers that occur before or at the same age as the first colonoscopy as prior or prevalent cancers, and from that point onwards it counts new primary cancers as events. Data collection was made from age 25 years at earliest, and cumulative incidence of CRC at age 25 years was set to zero. When CRC was counted as the event, all carriers who already had CRC prior to or at inclusion in the study were excluded, and observation time was right-censored at the first event, last observation or death, whichever came first. These methods have been discussed in detail in a separate report [9]. Lead-time bias was controlled by colonoscopy at inclusion and only scoring CRC after inclusion as an event, but since there is no pre-determined time to right-censoring and no obligatory colonoscopy at right-censoring is required, length-time bias may occur. Although the median observation time was less than 10 years, as it is longer in some patients, time-trend bias may occur. Except for the effects of ascertainment bias, which will affect any study, the annual incidences of CRC reported by PLSD are not subject to any assumptions underlying the calculations: they reflect observed events divided by observation years in each age group. Observation years and events (i.e. CRCs) in each five-year age group were calculated by using MySQL80 ©. Incidence rates (AIR) were calculated in five-year cohorts starting at age 25 as number of events (in this paper CRCs) divided by number of observation years in each age cohort. The corresponding incidence risk (IR) was approximated by IR = AIR × 5 years. Cumulative incidence risk was set to zero at age 25. In previous PLSD reports cumulative incidence, denoted Q, was computed starting at age 25 using the formula Q(age) = Q(age − 1) + [1 − Q(age − 1)] × AIR(age) and the 95% confidence intervals (CIs) were calculated using the Lagrange multiplier test. In this report, we calculated the cumulative incidence risks and the 95% CIs based on Nelson-Aalen estimates with an underlying Poisson distribution as detailed in the supplementary note. As expected, the cumulative incidences calculated by the former and present methods were close to identical, while the Poisson distribution gave slightly different CIs (comparison not shown). There were insufficient numbers to calculate results separately for continents other than Europe.
The IMRC used a segregation analysis to study a retrospective family cohort of first- and second-degree relatives, including 31,944 first-degree relatives and 47,865 second-degree relatives of path_MMR probands in 5,585 families. Most probands were path_MLH1 or path_MSH2 carriers, and the methods were discussed previously. Pedigree data of path_MMR families was sought from clinicians and researchers worldwide between July 11, 2014 and December 31, 2018 [5]. Observation time for all individuals included their lifetime risk of first colorectal cancer from birth to their age at death or last known age at latest update to the cohort in 2018. In summary, standard methods correcting for ascertainment bias and then calculating cumulative incidences of CRC by age, gene and gender were applied. The results were reported by continent. To allow for direct comparison with the PLSD, the results of IMRC segregation analyses for the current study were not right-censored at polypectomy (as had been done in the previously published IMRC report [5]) and consequently the results presented here may differ slightly from those previously published. The overall (global) averages were calculated as a weighted mean of the results from the different continents that were previously reported.
Results
Cumulative incidences at ages 30, 40, 50, 60 and 70 years for male and female carriers by MMR gene are detailed in Table 1. For the PLSD series, numbers of carriers included and follow-up years by country are given in the supplementary Table 1.
Prospective PLSD series under colonoscopy surveillance
In total 8,153 carriers were subject to follow-up with colonoscopy for 67,604 years with mean follow-up time of 8.3 years, including 6,266 carriers followed-up for 53,559 years with mean follow-up time 8.5 years in Europe. Five-hundred and seventy-eight carriers had CRC diagnosed. Average cumulative incidences of CRC (with 95% confidence intervals in parentheses) in path_MLH1, path_MSH2, path_MSH6 and path_PMS2 carriers at 70 years of age were 52 (45-59)%/ 41 (35-48)%, 50 (42-58)%/ 39 (33-46)%, 13 (7-25)%/ 17 (11-26)% and 11 (3-37)%/ 8 (2-29)% in male/female carriers in the total cohort, respectively. For carriers followed-up in Europe, the corresponding cumulative incidences at 70 years were 49 (42-57)% / 41 (35-48)%, 46 (37-57)%/ 39 (31-47) %, 12 (6-24)%/ 15 (9-24)% and 12 (3-40) %/ 3 (1-22)%, respectively.
Retrospective IMRC series
The corresponding average calculated cumulative incidences up to 70 years of age based on all carriers from the IMRC cohort were 40 (34-47)%/ 27 (22-33)%, 34 (28-40)%/ 23 (19-29)%, 16 (12-24)%/ 8 (6-13)% and 7 (6-8)%/ 6 (5-6)%, respectively. The cumulative incidences in families from Europe were 36 (27-48)%/ 22 (15-32)%, 28 (21-38)%/ 17 (11-27)%, 14 (8-24)%/ 6 (3-11)% and 8 (6-10)%/ 5 (4-7)%, respectively. Cumulative incidences at 25 years of ages were < 1.0% in all of the groups considered. Sixty percent of the carriers were right-censored after 1980.
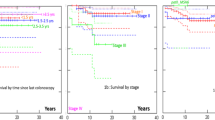
As seen in Table 1 and Fig. 1, the cumulative incidences of CRC in path_MLH1 and path_MSH2 carriers of both genders were significantly higher in the prospective PLSD cohort in which all were subjected to regular colonoscopy surveillance than in the IMRC cohort (95% confidence intervals do not overlap). No significant differences were observed for MSH6, for which fewer patients and events were available in both cohorts (95% confidence intervals of the one series overlap the mean of the other). The point estimates for the mean for path_PMS2 carriers below 50 years of age indicated a lower CRC incidence in the PLSD cohort when compared to the IMRC cohort, but this was not statistically significant.

Cumulative incidences of CRC by genetic variant and gender in PLSD (the prospective series with colonoscopy) and IMRC (the retrospective series) in European path_MLH1, path_MSH2 and path_MSH6 carriers. Broken lines indicate 95% confidence intervals
Discussion
Prospectively observed incidences of CRC in path_MLH1, path_MSH2 and path_MSH6 carriers of both genders in the PLSD cohort, in which all patients were subject to colonoscopy surveillance, were up to twice as high as in the retrospective IMRC series that included carriers who did not all receive regular surveillance colonoscopy.
Consideration of the methodologies used and the associated statistical concepts and confounders is indicated to explore the possibility that the results we obtained might reflect methodological biases, particularly as they were the opposite of what was expected. The PLSD methods have been described previously [9] and the IMRC results were produced using commonly accepted methods, as previously described [5]. Assuming the PLSD mean observation time (8.3 years) to be applicable to IMRC cases right-censored after 1980 (when surveillance with colonoscopy was introduced) as a maximum estimate of the fraction of IMRC cases subjected to colonoscopy, at least 85% of the IMRC observation years would have been completed without colonoscopy. The main finding of the current study would not, anyway, be confounded if a fraction of cases in the IMRC cohort underwent colonoscopy. We recognize that some individuals will have been included in the PLSD as well as the IMRC cohort, but we cannot identify them and their inclusion in both cohorts will not have contributed to the differences in observed CRC incidences. It is possible that CRC was under-reported in the pedigrees obtained by clinical teams, the details of which constituted the primary data source for the IMRC analysis. By contrast, under-reporting of CRC is unlikely in the PLSD cohort whose subjects were under regular surveillance at the contributing centres. It is unlikely that the lower CRC incidences estimated in the IMRC cohort are due to differing frequencies of lower penetrance path_MMR variants or modifying genes in former generations because there have been no known major fluctuations (bottlenecks) in population sizes or structures over the last three generations to cause such changes. As 60% of IMRC cases were right-censored after 1980, possible lower CRC incidence in previous generations (time-trend bias) can not explain the results. However, Lynch syndrome colorectal cancer incidence is associated with lower physical activity [10], and higher body mass index [11]. Temporal changes in such factors could explain some of the observed differences in colorectal cancer incidences between the two cohorts.
In a previous retrospective study, segregation analyses describing cumulative incidences of CRC in French path_MLH1, path_MSH2 and path_MSH6 carriers [12] were not restricted to first and second degree relatives. This helped to avoid simply returning the criteria used to identify families for genetic testing as the results of the study, and to minimize the effects of removing young affected carriers when considering a family to have a hypergeometric distribution of events. Observation time was right-censored at the diagnosis of any cancer in order to avoid survival bias when deaths from other cancers were caused by the same genetic variant. Additional family members were tested and demonstrated to carry the genetic variant in question in order to minimize the confounder of there being additional inherited causes of cancer within the family. Observation time was also right censored if the carrier was subjected to surveillance colonoscopy in order to avoid the confounder of colonoscopy modifying CRC incidence. The point estimates of cumulative CRC incidence at 70 years in that report for both genders combined were 41% for path_MLH1 carriers, 48% for path_MSH2 carriers and 12% for path_MSH6 carriers, very close to the observed incidences in the PLSD series in the current report. The number of cases included was, however, limited and the confidence intervals correspondingly wide – a reason why the PLSD waited for the IMRC results to be available before making a comparison of its prospective data with results of retrospective segregation analyses. While the French report could suggest that the IMRC segregation analyses have underestimated CRC incidence, comparing the current PLSD results with the point estimates in the French series does not demonstrate any reduction in CRC incidence associated with colonoscopy surveillance in the PLSD cohort.
A European multicentre segregation analysis that estimated CRC incidence in path_PMS2 carriers [13] demonstrated an increased incidence in carriers under 50 years of age, similar to the findings reported in the IMRC series. In a subsequent report [14] the same group confirmed that the apparent anticipation observed was a statistical artifact caused by birth cohorts. The PLSD design eliminates such artificial anticipation. The path_PMS2 carriers in the PLSD cohort had lower incidence of CRC before 50 years of age than those reported by the IMRC, but not significantly so. That is, the assumption that colonoscopy reduces CRC incidence may be true for younger adult path_PMS2 carriers. If this finding is confirmed, the recently revised clinical guidelines for path_PMS2 carriers [15] that advocate postponing surveillance compared to other groups with LS would need to be reconsidered. Observations in larger numbers of path_PMS2 carriers are needed to clarify this.
A recent overview of current knowledge on carcinogenetic mechanisms in LS CRCs [16] reported that in addition to the traditional adenoma-carcinoma pathway [2], other carcinogenetic mechanisms also need to be considered. Five hypotheses were described. including 1) adenomas that are overlooked during colonoscopy, 2) fast progression of adenomas to carcinomas [2], 3) CRCs developing without a macroscopically visible adenoma phase 4) over-diagnosis / disappearing cancers [17] and 5) colonoscopy inducing cancer in path_MMR carriers via damage of the colonic epithelium. Hypothesis 1 and 2 cannot explain the results described in this paper as we found higher rates of CRC incidence in those receiving colonoscopy. Although hypothesis 5 is consistent with our results, we have no method to evaluate this. We are left with hypotheses 3 and 4, that CRC may develop directly from MMR deficient crypts without a macroscopically visible precursor and that microsatellite instable crypts, or more advanced cancers, may be invaded by immunocompetent cells leading to their eradication. The latter underlies the principle of neoadjuvant checkpoint inhibitor therapy that has shown marked success in recent trials in MMR deficient CRCs [18, 19] and current studies exploring the feasibility of vaccines to prevent or cure LS cancers [20]. An adult path_MLH1 or path_MSH2 carrier is thought to have > 1000 microsatellite instable crypts in his/her colon [21,22,23,24]. It is known that apparently healthy path_MMR carriers have measurable immune responses against frameshift-induced neo-peptides, suggesting their immune systems can detect and potentially attack microsatellite instable crypts [25]. The probabilities for such crypts persisting, disappearing or developing into infiltrating cancers are not known. The biology of CRC in path_PMS2 carriers may be different from carriers of the pathogenic variants of the other genes [26, 27].
Although the focus of this paper is on CRC incidence, we consider prevention of death due to CRC to be the ultimate goal of surveillance colonoscopy, and the good prognosis of CRC detected in path_MMR carriers who are subjected to colonoscopy every three years or more frequently has been described in previous PLSD reports [8]. This is a strong argument to continue surveillance of path_MMR carriers by colonoscopy. The current paper does not call this into question, but its findings do support a change in the message to be communicated to path_MMR carriers, namely that the purpose of surveillance colonoscopy is not to prevent CRC from occurring but to detect it early. The authors of the current study have previously examined the relationship between colonoscopy interval and CRC incidence, stage at diagnosis, and survival [18, 28,29,30] without finding evidence of lower CRC incidence, less advanced stage or better survival when the interval between colonoscopies is shortened to less than three years.
Lastly, the very low incidence of CRC before 25 years of age that was found in the IMRC cohort indicates that the PLSD methodology of setting CRC incidence to zero at 25 years of age was justified. Indeed, without extensive genetic testing, one cannot exclude the possibility that occurrence of CRC before 25 years of age may, in some cases, have been due to inclusion of unrecognized biallelic path_MMR carriers (i.e. individuals who were affected by constitutional mismatch repair deficiency syndrome) or the presence of pathogenic germline variants in other co-existing CRC predisposition genes [31].
The strength of the current study is that it compares the results of the two largest studies to date on CRC incidences in path_MMR carriers. One weakness is the lack of information on colonoscopy in the IMRC series: contributors to IMRC were asked to provide information on colnosocpy sceeening and polypectomy, however this was not provided for the vast majority of submitted individuals. Another weakness is lack of information on the degree to which follow up for cases included in the PLSD complied with recommendations. The effects of non-compliance would be to diminish the differences between the two series and could not explain the increased CRC incidence in the PLSD series compared to the IMRC series.
Conclusions
We found a higher incidence of CRC in the carriers reported to PLSD, all of whom received colonoscopic surveillance. However, as the details of colonoscopies that will have been undertaken in some of the IMRC cohort are not available, we cannot quantify the magnitude of this effect. Although these findings could reflect differences in the fidelity of recording of CRC in the retrospective and prospective cohorts, the findings could also be explained by the occurrence of carcinogenetic mechanisms in LS CRC that override the preventive effect of colonoscopy [16].
Availability of data and materials
Not applicable.
Abbreviations
- LS:
-
Lynch syndrome
- CRC:
-
colorectal cancer
- Path_MMR :
-
pathogenic or likely pathogenic variant of one of the MLH1, MSH2, MSH6 or PMS2 genes
- Path_MLH1 :
-
pathogenic or likely pathogenic variant of one of the MLH1 gene
- Path_MSH2 :
-
pathogenic or likely pathogenic variant of one of the MLH1 gene
- Path_MSH6 :
-
pathogenic or likely pathogenic variant of one of the MLH1 gene
- Path_PMS2 :
-
pathogenic or likely pathogenic variant of one of the MLH1 gene
- PLSD:
-
The Prospective Lynch Syndrome Database
- IMRC:
-
The International Mismatch Repair Consortium
References
Järvinen HJ, Mecklin JP, Sistonen P. Screening reduces colorectal cancer rate in families with hereditary nonpolyposis colorectal cancer. Gastroenterology. 1995;108(5):1405–11. https://doi.org/10.1016/0016-5085(95)90688-6 PMID: 7729632.
Vasen HF, Nagengast FM, Khan PM. Interval cancers in hereditary non-polyposis colorectal cancer (Lynch syndrome). Lancet. 1995;345(8958):1183–4. https://doi.org/10.1016/s0140-6736(95)91016-6 PMID: 7723574.
Vasen HF, Möslein G, Alonso A, Bernstein I, Bertario L, Blanco I, et al. Guidelines for the clinical management of Lynch syndrome (hereditary non-polyposis cancer). J Med Genet. 2007;44(6):353–62. https://doi.org/10.1136/jmg.2007.048991 Epub 2007 Feb 27. PMID: 17327285; PMCID: PMC2740877.
Vasen HF, Blanco I, Aktan-Collan K, Gopie JP, Alonso A, Aretz S, Bernstein I, Bertario L, Burn J, Capella G, Colas C, Engel C, Frayling IM, Genuardi M, Heinimann K, Hes FJ, Hodgson SV, Karagiannis JA, Lalloo F, Lindblom A, Mecklin JP, Møller P, Myrhoj T, Nagengast FM, Parc Y, Ponz de Leon M, Renkonen-Sinisalo L, Sampson JR, Stormorken A, Sijmons RH, Tejpar S, Thomas HJ, Rahner N, Wijnen JT, Järvinen HJ, Möslein G; Mallorca group. Revised guidelines for the clinical management of Lynch syndrome (HNPCC): recommendations by a group of European experts. Gut. 2013 62(6):812-23. https://doi.org/10.1136/gutjnl-2012-304356. Epub 2013 Feb 13. PMID: 23408351; PMCID: PMC3647358.
International Mismatch Repair Consortium. Variation in the risk of colorectal cancer in families with Lynch syndrome: a retrospective cohort study. Lancet Oncol. 2021;22(7):1014–22. https://doi.org/10.1016/S1470-2045(21)00189-3 Epub 2021 Jun 7. PMID: 34111421.
Douglas JA, Gruber SB, Meister KA, Bonner J, Watson P, Krush AJ, et al. History and molecular genetics of Lynch syndrome in family G: a century later. JAMA. 2005;294(17):2195–202. https://doi.org/10.1001/jama.294.17.2195 PMID: 16264161.
Møller P, Seppälä T, Bernstein I, Holinski-Feder E, Sala P, Evans DG, et al. Incidence of and survival after subsequent cancers in carriers of pathogenic MMR variants with previous cancer: a report from the prospective Lynch syndrome database. Gut. 2017;66(9):1657–64. https://doi.org/10.1136/gutjnl-2016-311403 Epub 2016 Jun 3. PMID: 27261338; PMCID: PMC5561364.
Dominguez-Valentin M, Sampson JR, Seppälä TT, Ten Broeke SW, Plazzer JP, Nakken S, Engel C, Aretz S, Jenkins MA, Sunde L, Bernstein I, Capella G, Balaguer F, Thomas H, Evans DG, Burn J, Greenblatt M, Hovig E, de Vos Tot Nederveen Cappel WH, Sijmons RH, Bertario L, Tibiletti MG, Cavestro GM, Lindblom A, Della Valle A, Lopez-Köstner F, Gluck N, Katz LH, Heinimann K, Vaccaro CA, Büttner R, Görgens H, Holinski-Feder E, Morak M, Holzapfel S, Hüneburg R, Knebel Doeberitz MV, Loeffler M, Rahner N, Schackert HK, Steinke-Lange V, Schmiegel W, Vangala D, Pylvänäinen K, Renkonen-Sinisalo L, Hopper JL, Win AK, Haile RW, Lindor NM, Gallinger S, Le Marchand L, Newcomb PA, Figueiredo JC, Thibodeau SN, Wadt K, Therkildsen C, Okkels H, Ketabi Z, Moreira L, Sánchez A, Serra-Burriel M, Pineda M, Navarro M, Blanco I, Green K, Lalloo F, Crosbie EJ, Hill J, Denton OG, Frayling IM, Rødland EA, Vasen H, Mints M, Neffa F, Esperon P, Alvarez K, Kariv R, Rosner G, Pinero TA, Gonzalez ML, Kalfayan P, Tjandra D, Winship IM, Macrae F, Möslein G, Mecklin JP, Nielsen M, Møller P. Cancer risks by gene, age, and gender in 6350 carriers of pathogenic mismatch repair variants: findings from the Prospective Lynch Syndrome Database. Genet Med. 2020 22(1):15-25. 10.1038/s41436-019-0596-9. Epub 2019 Jul 24. Erratum in: Genet Med. 2020 22(9):1569. PMID: 31337882; PMCID: PMC7371626.
Møller P. The Prospective Lynch Syndrome Database reports enable evidence-based personal precision health care. Hered Cancer Clin Pract. 2020;14(18):6. https://doi.org/10.1186/s13053-020-0138-0 PMID: 32190163; PMCID: PMC7073013.
Dashti SG, Win AK, Hardikar SS, Glombicki SE, Mallenahalli S, Thirumurthi S, et al. Physical activity and the risk of colorectal cancer in Lynch syndrome. Int J Cancer. 2018;143(9):2250–60. https://doi.org/10.1002/ijc.31611 Epub 2018 Aug 7. PMID: 29904935; PMCID: PMC6195467.
Win AK, Dowty JG, English DR, Campbell PT, Young JP, Winship I, Macrae FA, Lipton L, Parry S, Young GP, Buchanan DD, Martínez ME, Jacobs ET, Ahnen DJ, Haile RW, Casey G, Baron JA, Lindor NM, Thibodeau SN, Newcomb PA, Potter JD, Le Marchand L, Gallinger S, Hopper JL, Jenkins MA. Body mass index in early adulthood and colorectal cancer risk for carriers and non-carriers of germline mutations in DNA mismatch repair genes. Br J Cancer. 2011 105(1):162-9. https://doi.org/10.1038/bjc.2011.172. Epub 2011 May 10. PMID: 21559014; PMCID: PMC3137400.
Bonadona V, Bonaïti B, Olschwang S, Grandjouan S, Huiart L, Longy M, et al. French Cancer Genetics Network. Cancer risks associated with germline mutations in MLH1, MSH2, and MSH6 genes in Lynch syndrome. JAMA. 2011;305(22):2304–10. https://doi.org/10.1001/jama.2011.743 PMID: 21642682.
Ten Broeke SW, van der Klift HM, Tops CMJ, Aretz S, Bernstein I, Buchanan DD, de la Chapelle A, Capella G, Clendenning M, Engel C, Gallinger S, Gomez Garcia E, Figueiredo JC, Haile R, Hampel HL, Hopper JL, Hoogerbrugge N, von Knebel Doeberitz M, Le Marchand L, Letteboer TGW, Jenkins MA, Lindblom A, Lindor NM, Mensenkamp AR, Møller P, Newcomb PA, van Os TAM, Pearlman R, Pineda M, Rahner N, Redeker EJW, Olderode-Berends MJW, Rosty C, Schackert HK, Scott R, Senter L, Spruijt L, Steinke-Lange V, Suerink M, Thibodeau S, Vos YJ, Wagner A, Winship I, Hes FJ, Vasen HFA, Wijnen JT, Nielsen M, Win AK. Cancer Risks for PMS2-Associated Lynch Syndrome. J Clin Oncol. 2018 36(29):2961-2968. https://doi.org/10.1200/JCO.2018.78.4777. Epub 2018 Aug 30. Erratum in: J Clin Oncol. 2019 Mar 20;37(9):761. PMID: 30161022; PMCID: PMC6349460.
Ten Broeke SW, Rodríguez-Girondo M, Suerink M, Aretz S, Bernstein I, Capellá G, Engel C, Gomez-Garcia EB, van Hest LP, von Knebel Doeberitz M, Lagerstedt-Robinson K, Letteboer TGW, Moller P, van Os TA, Pineda M, Rahner N, Olderode-Berends MJW, von Salomé J, Schackert HK, Spruijt L, Steinke-Lange V, Wagner A, Tops CMJ, Nielsen M. The Apparent Genetic Anticipation in PMS2-Associated Lynch Syndrome Families Is Explained by Birth-cohort Effect. Cancer Epidemiol Biomarkers Prev 2019 28(6):1010-1014. https://doi.org/10.1158/1055-9965.EPI-18-0576. Epub 2019 Mar 1. PMID: 30824524.
Seppälä TT, Latchford A, Negoi I, Sampaio Soares A, Jimenez-Rodriguez R, Sánchez-Guillén L, et al. European guidelines from the EHTG and ESCP for Lynch syndrome: an updated third edition of the Mallorca guidelines based on gene and gender. Br J Surg. 2021;108(5):484–98. https://doi.org/10.1002/bjs.11902 PMID: 34043773.
Ahadova A, Seppälä TT, Engel C, Gallon R, Burn J, Holinski-Feder E, Steinke-Lange V, Möslein G, Nielsen M, Ten Broeke SW, Laghi L, Dominguez-Valentin M, Capella G, Macrae F, Scott R, Hüneburg R, Nattermann J, Hoffmeister M, Brenner H, Bläker H, von Knebel Doeberitz M, Sampson JR, Vasen H, Mecklin JP, Møller P, Kloor M. The “unnatural” history of colorectal cancer in Lynch syndrome: Lessons from colonoscopy surveillance. Int J Cancer 2021 148(4):800-811. https://doi.org/10.1002/ijc.33224. Epub 2020 Aug 3. PMID: 32683684.
Seppälä TT, Ahadova A, Dominguez-Valentin M, Macrae F, Evans DG, Therkildsen C, et al. Lack of association between screening interval and cancer stage in Lynch syndrome may be accounted for by over-diagnosis; a prospective Lynch syndrome database report. Hered Cancer Clin Pract. 2019;28(17):8. https://doi.org/10.1186/s13053-019-0106-8 PMID: 30858900; PMCID: PMC6394091.
Chalabi M, Fanchi LF, Dijkstra KK, Van den Berg JG, Aalbers AG, Sikorska K, et al. Neoadjuvant immunotherapy leads to pathological responses in MMR-proficient and MMR-deficient early-stage colon cancers. Nat Med. 2020;26(4):566–76. https://doi.org/10.1038/s41591-020-0805-8 Epub 2020 Apr 6. PMID: 32251400.
Versluis JM, Long GV, Blank CU. Learning from clinical trials of neoadjuvant checkpoint blockade. Nat Med 2020;26(4):475-484. https://doi.org/10.1038/s41591-020-0829-0. Epub 2020 Apr 9. PMID: 32273608.
Kloor M, Reuschenbach M, Pauligk C, Karbach J, Rafiyan MR, Al-Batran SE, Tariverdian M, Jäger E, von Knebel Doeberitz M. A Frameshift Peptide Neoantigen-Based Vaccine for Mismatch Repair-Deficient Cancers: A Phase I/IIa Clinical Trial. Clin Cancer Res 2020 26(17):4503-4510. https://doi.org/10.1158/1078-0432.CCR-19-3517. Epub 2020 Jun 15. PMID: 32540851.
Kloor M, Huth C, Voigt AY, Benner A, Schirmacher P, von Knebel Doeberitz M, Bläker H. Prevalence of mismatch repair-deficient crypt foci in Lynch syndrome: a pathological study. Lancet Oncol 2012 13(6):598-606. https://doi.org/10.1016/S1470-2045(12)70109-2. Epub 2012 May 1. PMID: 22552011.
Staffa L, Echterdiek F, Nelius N, Benner A, Werft W, Lahrmann B, Grabe N, Schneider M, Tariverdian M, von Knebel Doeberitz M, Bläker H, Kloor M. Mismatch repair-deficient crypt foci in Lynch syndrome--molecular alterations and association with clinical parameters. PLoS One 2015 10(3):e0121980. https://doi.org/10.1371/journal.pone.0121980. PMID: 25816162; PMCID: PMC4376900.
Pai RK, Dudley B, Karloski E, Brand RE, O’Callaghan N, Rosty C, Buchanan DD, Jenkins MA, Thibodeau SN, French AJ, Lindor NM, Pai RK. DNA mismatch repair protein deficient non-neoplastic colonic crypts: a novel indicator of Lynch syndrome. Mod Pathol. 2018 31(10):1608-1618. https://doi.org/10.1038/s41379-018-0079-6. Epub 2018 Jun 8. PMID: 29884888; PMCID: PMC6396289.
Brand RE, Dudley B, Karloski E, Das R, Fuhrer K, Pai RK, et al. Detection of DNA mismatch repair deficient crypts in random colonoscopic biopsies identifies Lynch syndrome patients. Fam Cancer. 2020;19(2):169–75. https://doi.org/10.1007/s10689-020-00161-w PMID: 31997046.
Schwitalle Y, Kloor M, Eiermann S, Linnebacher M, Kienle P, Knaebel HP, Tariverdian M, Benner A, von Knebel Doeberitz M. Immune response against frameshift-induced neopeptides in HNPCC patients and healthy HNPCC mutation carriers. Gastroenterology. 2008 134(4):988-997. https://doi.org/10.1053/j.gastro.2008.01.015. Epub 2008 Jan 11. PMID: 18395080.
Ten Broeke SW, van Bavel TC, Jansen AML, Gómez-García E, Hes FJ, van Hest LP, Letteboer TGW, Olderode-Berends MJW, Ruano D, Spruijt L, Suerink M, Tops CM, van Eijk R, Morreau H, van Wezel T, Nielsen M. Molecular Background of Colorectal Tumors From Patients With Lynch Syndrome Associated With Germline Variants in PMS2. Gastroenterology. 2018 155(3):844-851. https://doi.org/10.1053/j.gastro.2018.05.020. Epub 2018 Jul 29. PMID: 29758216.
Bajwa-Ten Broeke SW, Ballhausen A, Ahadova A, Suerink M, Bohaumilitzky L, Seidler F, et al. The coding microsatellite mutation profile of PMS2-deficient colorectal cancer. Exp Mol Pathol. 2021;122:104668. https://doi.org/10.1016/j.yexmp.2021.104668 Epub 2021 Jul 22. PMID: 34302852.
Dominguez-Valentin M, Seppälä TT, Sampson JR, Macrae F, Winship I, Evans DG, et al. Survival by colon cancer stage and screening interval in Lynch syndrome: a prospective Lynch syndrome database report. Hered Cancer Clin Pract. 2019;17:28. https://doi.org/10.1186/s13053-019-0127-3 PMID: 31636762; PMCID: PMC6792227.
Seppälä T, Pylvänäinen K, Evans DG, Järvinen H, Renkonen-Sinisalo L, Bernstein I, et al. Colorectal cancer incidence in path_MLH1 carriers subjected to different follow-up protocols: a Prospective Lynch Syndrome Database report. Hered Cancer Clin Pract. 2017;15:18. https://doi.org/10.1186/s13053-017-0078-5 PMID: 29046738; PMCID: PMC5635542.
Engel C, Vasen HF, Seppälä T, Aretz S, Bigirwamungu-Bargeman M, de Boer SY, Bucksch K, Büttner R, Holinski-Feder E, Holzapfel S, Hüneburg R, Jacobs MAJM, Järvinen H, Kloor M, von Knebel Doeberitz M, Koornstra JJ, van Kouwen M, Langers AM, van de Meeberg PC, Morak M, Möslein G, Nagengast FM, Pylvänäinen K, Rahner N, Renkonen-Sinisalo L, Sanduleanu S, Schackert HK, Schmiegel W, Schulmann K, Steinke-Lange V, Strassburg CP, Vecht J, Verhulst ML, de Vos Tot Nederveen Cappel W, Zachariae S, Mecklin JP, Loeffler M; German HNPCC Consortium, the Dutch Lynch Syndrome Collaborative Group, and the Finnish Lynch Syndrome Registry. No Difference in Colorectal Cancer Incidence or Stage at Detection by Colonoscopy Among 3 Countries With Different Lynch Syndrome Surveillance Policies. Gastroenterology. 2018 155(5):1400-1409.e2. https://doi.org/10.1053/j.gastro.2018.07.030. Epub 2018 Jul 29. PMID: 30063918.
Mao R, Krautscheid P, Graham RP, et al. Genetic testing for inherited colorectal cancer and polyposis, 2021 revision: a technical standard of the American College of Medical Genetics and Genomics (ACMG). Genet Med. 2021;23:1807–17.
Acknowledgments
Harsh Sheth contributed with support from Gujarat State Biotechnology Mission grant GSBTM/JD(R&D)/604/2018-2019/7 and clinical oncologists Prof. Suresh h Advani, Dr. Pankaj Shah and Dr. Abhinav Jain. ERN GENTURIS is partly co-funded by the European Union within the framework of the Third Health Programme “ERN-2016 – Framework Partnership Agreement 2017–2021”. Funding bodies had no role in the study design, collection, analysis or interpretation of the data.
Funding
Toni T. Seppälä: Finnish Medical Foundation, Emil Aaltonen Foundation, Cancer Society Finland, Jane and Aatos Erkko Foundation, iCAN Digital Precision Cancer Medicine Flagship, Relander Foundation, Sigrid Juselius Foundation, and Academy of Finland. Jukka-Pekka Mecklin: Cancer Society Finland, Jane and Aatos Erkko Foundation. G Capellá team: funded by the Spanish Ministry of Economy and Competitiveness and co-funded by FEDER funds -a way to build Europe- (grant PID2019-111254RB-I00) and CIBERONC (CB16/12/00234). We thank CERCA Program / Generalitat de Catalunya for institutional support. S Aretz , E Holinski-Feder, and V Steinke-Lange were supported by the European Reference Network on Genetic Tumor Risk Syndromes (ERN GENTURIS) – Project ID No 739547. ERN GENTURIS is partly co-funded by the European Union within the framework of the Third Health Programme “ERN-2016 – Framework Partnership Agreement 2017–2021”. BMRossi team: we thank LA-GETH (Latin America - Grupo de Estudios de Tumores Hereditarios) for the Institutional support. DGE and EJC are supported by the all Manchester NIHR Biomedical Research Centre (IS-BRC-1215-20007). JRS thanks HCRW for its support via Wales Gene Park. MRJ Kohonen-Corish had a grant from Cancer Council NSW grant RG19-01. J Burn contributed with support from Cancer Research U.K. catalyst award: Aspirin for Cancer Prevention AsCaP CRUK A24991. ”. The German Consortium for Familial Intestinal Cancer was supported by grants of the German Cancer Aid. DM Carraro and GT Torrezan: Funded by the National Institute of Science and Technology in Oncogenomics and Therapeutic Innovation (FAPESP 2014/509443-1, CNPq 465682/2014-6 and CAPES - 88887.136405/2017-00). ). We acknowledge funding from the Norwegian Cancer Society, contract 194751-2017.
Author information
Authors and Affiliations
Consortia
Contributions
PLSD results were calculated by PM and SH, IMRC results were calculated by JD and MJ. PM and TTS initially drafted the paper, which was commented by all, after which the above and JS drafted a final version that was approved by all authors.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All contributors to the PLSD and IMRC have declared ethics approval and have obtained consents for participations.
Consent for publication
There is no further need for consent for publication of categorized data.
Competing of interests
L Senter-Jamieson have received speaking/consultant fees from AstraZeneca in the past year. Carmen Guillén-Ponce: registrations for congresses and continuing education courses by Merck, Sanofi and Astra Zeneca. Toni T. Seppälä reports CEO and co-owner of Healthfund Finland and an interview honoraria from Boehringer Ingelheim Finland. All other authors declare no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Møller, P., Seppälä, T., Dowty, J.G. et al. Colorectal cancer incidences in Lynch syndrome: a comparison of results from the prospective lynch syndrome database and the international mismatch repair consortium. Hered Cancer Clin Pract 20, 36 (2022). https://doi.org/10.1186/s13053-022-00241-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13053-022-00241-1