
Abstract
Background
Childhood obesity has become a huge challenge to childhood health, and there is a lack of understanding about the relationship between dietary inflammatory index (DII) and childhood obesity. The main objective of this study was to analyze the potential link between DII and obesity among children and adolescents residing in the United States.
Methods
A cross-sectional analysis was performed using data obtained from the National Health and Nutrition Examination Survey between 2009 and 2018. In total, 12,454 participants were included in the analysis. DII was calculated based on dietary data from the first day of the 24-hour dietary recall. Logistic regression was used to analyze the association between DII and obesity, as well as central obesity defined by the waist-to-height ratio of 0.5 or higher or waist circumference ≥ 90th percentile for age and sex.
Results
The mean dietary inflammation index was 2.05 (SE = 0.02), with higher levels in children than in adolescents (P = 0.01). According to our findings, the prevalence of central obesity was higher among adolescents (38.0%) than among children (31.4%). The adolescents in the third quartile of DII have a higher risk of overweight/obesity (OR = 1.46, 95% CI: 1.24–1.71) after adjusting for age, sex, and race. This positive association remained significant even after physical activity was added to the model. Concerning central obesity, the adolescents in the highest quartile of DII have a higher risk, independent of demographic characteristics and physical activity. However, no significant association was observed among children.
Conclusions
The dietary inflammation index was positively associated with overweight/obesity and central obesity among adolescents in the United States after adjusting for confounding factors. These findings highlight the importance of promoting anti-inflammatory diets in adolescents to prevent obesity and its associated complications.
Similar content being viewed by others

Introduction
Childhood obesity is a major global, public health challenge, with implications for childhood hypertension, abnormal lipid metabolism, and abnormal glucose metabolism. It is also associated with the risk of developing chronic diseases such as coronary heart disease, cerebrovascular disease, and cancer in adulthood [1,2,3,4]. Although the mechanisms are not yet clear, there have been many valuable findings. In recent years, the concept of unhealthy obesity has been proposed in academia [5, 6]. It suggests that excessive accumulation of body fat, especially visceral fat, leads to adiposopathy, which is a significant cause of metabolic complications. Research has shown that the presence of adipose tissue dysfunction in obese individuals can lead to a state of inflammation in the body [7]. Studies indicate that inflammation may play a significant role in the development of metabolic disorders, cardiovascular diseases, and obesity-associated tumors [8, 9]. This is attributed to excess adipose tissue in obese individuals, which leads to increased production of cytokines and leptin while reducing anti-inflammatory immune cells [10, 11].
The Dietary Inflammation Index (DII) is a tool that assesses the inflammatory impact of a specific diet and has been associated with various chronic conditions [12,13,14,15,16]. This index incorporates a comprehensive assessment of the pro- and anti-inflammatory components of food, including macronutrients, minerals, vitamins, flavonoids, and specialty food constituents [13]. Currently, the DII is a standard tool used to assess diets internationally and across cultures.
Recently, there has been a surge in research on the correlation between DII and obesity. However, there is conflicting evidence regarding the findings of these studies. Certain studies have established a positive correlation between DII score and obesity in adults, indicating a higher likelihood of obesity with the consumption of pro-inflammatory foods. Nevertheless, other studies have yielded contradictory results [17, 18], while few studies have stated no significant relationships [19]. Limited studies conducted on DII and childhood obesity are often confined to a single age group and may not necessarily represent a larger population. Previous studies indicate conflicting results regarding the correlation between DII and obesity in children. A study conducted on 8–9 year–old children showed no significant association between DII, total body mass, and central obesity but showed a negative association with adipokine levels [20]. Another study of children aged 5–9 years discovered a positive association between DII and obesity [21]. In Iranian adolescents, a positive correlation between DII and body fat content has been reported [22], whereas a Brazilian study on 12–17-year-olds found an association between DII and overweight and abdominal obesity [23]. This is the largest study of its kind to date that analyzes data from a representative sample of American children and adolescents to investigate the potential link between DII and obesity.
Methods
Study design and Population
The analytical data utilized in this study were obtained from NHANES, specifically from the years 2009 to 2018. NHANES employs a complex, stratified, multistage probability sampling procedure to collect health and nutritional data. The data is gathered from a representative sample of the civilian, noninstitutionalized US population. The NHANES process involves a combination of a home interview and a physical examination, which includes a face-to-face 24-hour dietary recall interview conducted at a mobile examination center (MEC). Additionally, a second 24-hour dietary recall is administered via telephone 3 to 10 days later. The NHANES is an ongoing series of cross-sectional surveys that employ a multistage probability sampling method and oversample certain population segments [18]. Publicly available data from approximately 10,000 participants are released for each annual cycle [18]. Mobile clinics and home visits were used to conduct physical examinations, collect biological samples, and interview participants. The NCHS Research Ethics Review Committee approved the survey protocol and written informed consent was obtained from all participants. For detailed information on the NHANES design and procedures, please refer to previous studies [19, 24].
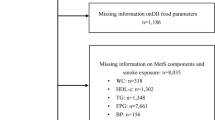
From 2009 to 2018, a total of 12,957 individuals participated in the MEC for the five-year cycles. Among them, 503 individuals did not complete the dietary survey, resulting in a total of 12,454 individuals included in the study. Age, gender, race, socioeconomic status, physical activity, energy intake, dietary components, and anthropometric measurements are some of the parameters that can be extracted from the NHANES database for the study participants.
Adiposity measures
We used standard procedures and equipment to measure height, weight, and waist circumference [25]. BMI was calculated as weight in kilograms divided by height in meters squared. Further, We defined underweight, normal weight, overweight/obesity, obesity, and severe obesity according to age- and sex-specific percentile cutoffs acquired from CDC growth charts [26]. Underweight was defined as a BMI below the 15th percentile. Normal weight was defined as a BMI between the 15th and 85th percentile. Obesity was defined as BMI for age- and sex-specific categories at the 95th percentile or higher. Overweight/obesity was defined as a BMI at or above the age- and sex-specific 85th percentile of the 2000 CDC growth charts. Severe obesity was defined as a BMI at or above the age- and sex-specific 120% of the 95th percentile of the CDC growth charts published in 2000. According to NHANES III data, central obesity was defined as a waist circumference equal to or greater than the sex and age-specific 90th percentile, or a waist-to-height ratio of 0.5 or higher [27].
Dietary inflammatory index
The development and validation of the DII have been thoroughly documented in other publication [28]. DII was calculated using dietary data collected during 24 h on day 1 [14, 29, 30]. This included information on the type and amount of food and drinks consumed during the preceding 24 h (midnight to midnight), which were collected by MEC. Subsequently, the data were used to approximate the intake of energy, nutrients, and food components from foods and beverages, as validated by the Working Group on Nutritional Methods [31, 32] and explained in another report [13].
The DII, which consists of 28 dietary components, was calculated based on the protocol provided by Shivappa et al. [28]. This index aims to evaluate the level of systemic inflammation by using six important inflammation markers (IL-1β, IL-6, IL-4, IL-10, TNF-α, and CRP). In this study, a score of “+1” was assigned if a dietary component increased the levels of CRP, TNF-α, IL-1β, and IL-6 or reduced the levels of IL-4 and IL-10. Conversely, a score of “-1” was assigned if a dietary component decreased the levels of CRP, TNF-α, IL-1β, and IL-6 or increased the levels of IL-4 and IL-10. Each individual food parameter was then multiplied by its respective effect score derived from the literature review. The sum of all food parameter-specific DII scores yielded the overall DII score for each participant, calculated as DII = b1 * n1 + b2 * n2…b28 * n28. Here, “b” refers to the literature-derived inflammatory effect score for each food parameter, and “n” refers to the food parameter-specific percentiles obtained from the dietary data derived from the FFQ (food frequency questionnaire). The pooled DII represents the pro-inflammatory or anti-inflammatory potential of an individual’s daily diet. Additionally, we employ imputation methods to infer missing food parameters [28].
To account for the total energy intake, the E-DII was calculated for every 1000 calories of food consumed, necessitating the use of an energy-standardized version of the global database.
Covariates
The NHANES used several covariates to adjust for individual characteristics, including age, sex, race, ethnicity, BMI, physical activity, and poverty-income ratio. The CDC website provides detailed information on the measurement procedures. Physical activity data adhered to the World Health Organization guidelines [33]. According to the 2018 Physical Activity Guidelines Advisory Committee scientific report [34, 35], participants who reported less than 10 min of moderate-to-vigorous physical activity per week were labeled as inactive.
Statistical analyses
The study conducted descriptive analyses on the entire sample and further stratified the data by age group, specifically children between 6 and 10 years old and adolescents between 11 and 19 years old. Results were presented as weighted means or percentages with standard errors. The main exposure variable was the estimated intake of DII. Multiple logistic regression was performed to investigate the relationship between DII and weight-related measures (overweight/obesity, obesity, and central obesity). Odds ratios were calculated and sorted into quartiles, allowing for comparisons across different DII percentiles. Combined dietary sample weights were used during statistical analyses performed using SAS version 9.4, or SAS-callable SUDAAN to account for non-response and sampling design. All statistical tests were conducted using a two-sided approach, and statistical significance was defined as P < 0.05.
Results
Table 1 illustrates the sample size and baseline characteristics of the US children and adolescents who participated in the 2009–2018 NHANES. Children aged 6–11 represented 55.7% of the total sample, whereas adolescents aged 12–19 represented 44.3%. Interestingly, there was an almost equal distribution between the sexes, with 49.1% girls and 50.9% boys. Furthermore, no significant differences in race or poverty income ratios were observed between the children and adolescents (Table 1).
Table 1 shows that the average DII was 2.05 (SE = 0.02), which was significantly higher in the children compared with adolescents (P = 0.01). Energy intake was significantly higher in adolescents than in children (P < 0.0001). Furthermore, Table 2 indicates that central obesity diagnosed using the WtHR was observed more frequently in adolescents than in children (38.0% vs. 31.4%). In contrast, there was no significant difference in the percentage of overweight/obesity between the two groups (40.7% vs. 40.3%). Additionally, the prevalence of severe obesity was slightly higher in adolescents (9.5%) than in children (8.3%) (Table 2).
Table 3 reveals the correlation between estimated weight gain and overweight/obesity in children and adolescents. Among adolescents, the adjusted odds ratio of overweight/obesity in DII quartile three was 1.46 (95% CI: 1.24–1.71) compared to the lowest quartile, and the adjusted OR values remained significant (1.42 (95% CI: 1.21–1.67)(P < 0.0001)) after adjusting for age, sex, and race (Table 3, Model 2). The positive correlation remained significant when physical activity was added to the model to adjust for potential false positives (Table 3, Model 3). However, no significant association was observed in overweight or obese children (Table 3).
Table 4 discloses that after adjusting for various confounding variables, the positive correlation between DII and obesity among adolescents was more pronounced and increased with increasing DII quartiles compared with overweight or obesity in the same age group. Conversely, no such correlation was observed among children after making the same adjustments.
In adolescents, DII had a positive correlation with central obesity, as measured by WC. Those in the highest quartile of DII had an increased likelihood of central obesity compared with those in the lowest quartile, even after adjusting for demographic characteristics and physical activity (adjusted OR = 1.56, 95%CI:1.27–1.93, P < 0.0001), as shown in Table 5, Model 3. This correlation remained significant when central obesity was defined as WtHR ≥ 0.5 (adjusted OR = 1.52, 95%CI:1.29–1.80, P < 0.0001), as displayed in Table 6, Model 3. However, we did not observe any noteworthy associations among children. In addition, there was no sex difference in the relationship between DII and obesity in children or adolescents (Table 7).
Discussion
Our study utilized NHANES 2009–2018 data and revealed that a higher DII was linked to increased odds of being overweight and/or obese. In addition, we observed a positive correlation between the DII score and central obesity in adolescents, even after adjusting for age, sex, and race. However, we did not find a significant association between DII and obesity in children in the US. Our findings are consistent with those of previous studies on childhood and adolescent obesity [20, 21, 36]. Although the exact reasons for the difference in the association between DII and obesity in children and adolescents remain uncertain, factors such as changes in hormone levels during puberty and the duration of obesity may play a significant role [37, 38]. Furthermore, the specific reasons for the association between the third quartile of DII and higher odds ratio in adolescents are still unclear and require further research. It also suggests that there is a non-linear relationship between DII and obesity in adolescents.
However, the precise biological mechanisms underlying the relationship between DII and obesity are not fully elucidated. Previous studies established a clear link between diet and inflammation [39,40,41]. Insulin resistance plays a significant role in the development of obesity. Inflammation can disrupt insulin signaling pathways, resulting in insulin resistance [42]. It is hypothesized that the inflammatory components of a high DII score may contribute to insulin resistance, thereby promoting weight gain and obesity. The composition and diversity of the gut microbiota have been implicated in obesity [43]. A pro-inflammatory diet may cause changes in the composition of gut bacteria, leading to an imbalance between beneficial and harmful bacteria. This imbalance, known as dysbiosis, can affect energy metabolism, inflammation, and fat storage, potentially contributing to weight gain and obesity [44]. Inflammatory factors can also influence the function of adipose tissue, including the secretion of adipokines and lipid metabolism [45]. A pro-inflammatory diet may disrupt the normal functioning of adipose tissue, leading to increased fat accumulation and obesity. Additionally, dietary patterns are also important risk factors leading to obesity.
The exact mechanism through which diet induces inflammation remains incompletely understood. Inflammation is significantly influenced by one’s dietary choices. While certain food items have the potential to trigger inflammation, others may aid in its reduction. The consumption of processed foods, refined carbs, sugary drinks, and unhealthy fats can contribute to the development of chronic inflammation. These particular food choices are capable of activating the immune system, thereby initiating an inflammatory response [46]. Conversely, a diet abundant in whole foods such as fruits, vegetables, whole grains, lean proteins, and healthy fats can effectively mitigate inflammation. Scientific investigations have demonstrated that adherence to the Mediterranean diet, as well as diets incorporating ample amounts of fruits, vegetables, and omega-3 fatty acids, correlates with diminished inflammation levels [47]. Implementing a low-inflammation or anti-inflammatory diet may serve as a valuable therapeutic approach in addressing obesity and its associated complications.
Inflammation is associated with various diseases, including obesity and metabolic syndromes [48, 49]. Despite the implementation of numerous measures to combat obesity, its prevalence in children and adolescents remains high which represents a major challenge for society. Therefore, it is essential to understand the relationship between DII and obesity in children and adolescents to develop dietary interventions for effectively tackling this issue. Based on our results, it appears that lowering DII in the diet may be an effective means of mitigating obesity risk, particularly in adolescents. Inflammation is a significant factor in the development of various health issues associated with obesity, such as metabolic syndrome, cardiovascular disease, and cancer (50–51). Managing dietary inflammation is critical for preventing health problems in obese children and adolescents.
The current study had several significant strengths. First, it utilized a nationally representative sample of children and adolescents in the United States, which enabled a broader reach to the general population. This sample size also allowed comprehensive anthropometric measurements and demographic data to be collected, thereby increasing the validity of the results. Moreover, collecting NHANES data on all days of each year reduced the likelihood of errors resulting from day-specific information bias, further increasing the robustness of the data and the outcome validity [52]. Additionally, employing a thorough dietary recall to determine the DII score ensured the accuracy and comprehensiveness of the dietary inflammatory potential assessment. Ultimately, this study presents valuable insights into the relationship between DII and obesity in children and adolescents, offering support for initiatives and policies that aim to mitigate childhood obesity.
The limitation of the study was the application of imputation methods to infer missing food parameters. A sensitivity analysis conducted on the imputed values yielded findings similar to those of the main analysis. Additionally, there was a lack of relevant data on Tanner stage and metabolic profile among our study participants. Despite these limitations, this study provides important insights into the relationship between DII scores and obesity in children and adolescents. However, further research is needed to confirm our findings. Additionally, future studies should consider including a more comprehensive dietary assessment tool to accurately capture the habitual diets of individuals. Furthermore, it should accumulate all relevant food parameters required to calculate the DII score. However, the DII calculated using the same number of food parameters as our study was evaluated in the NHANES, with C-reactive protein as the outcome [53]. Furthermore, because our study was cross-sectional, causality could not be directly inferred. Hence, future studies with larger sample sizes and multiple dietary assessments are required to provide further insights into the underlying mechanisms and validate our findings.
Conclusions
Our findings indicate a possible link between DII scores and overweight/obesity, obesity, and central obesity in adolescents. These results support the hypothesis that inflammation triggered by dietary habits may play a role in the development of obesity in adolescents. Nonetheless, additional investigations are necessary to verify and expand our findings, as well as to probe the underlying biological mechanisms. Overall, these findings emphasize the critical role of a nutritious diet in the prevention and control of obesity in adolescents.
Data availability
The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding author.
Abbreviations
- WC:
-
Waist circumference
- WtHR:
-
Waist-to-height ratio
- NHANES:
-
National Health and Nutrition Examination Survey
- DII:
-
Dietary Inflammation Index
- MEC:
-
Mobile examination center
- BMI:
-
Body mass index
References
Ogden CL, Carroll MD, Kit BK, Flegal KM. Prevalence of childhood and adult obesity in the United States, 2011–2012. JAMA. 2014;311(8):806–14. https://doi.org/10.1001/jama.2014.732.
Weihrauch-Blüher S, Schwarz P, Klusmann JH. Childhood obesity: increased risk for cardiometabolic disease and cancer in adulthood. Metabolism. 2019;92:147–52. https://doi.org/10.1016/j.metabol.2018.12.001. Epub 2018 Dec 5.
Llewellyn A, Simmonds M, Owen CG, Woolacott N. Childhood obesity as a predictor of morbidity in adulthood: a systematic review and meta-analysis. Obes Rev. 2016;17(1):56–67. https://doi.org/10.1111/obr.12316. Epub 2015 Oct 6.
Bendor CD, Bardugo A, Pinhas-Hamiel O, Afek A, Twig G. Cardiovascular morbidity, diabetes and cancer risk among children and adolescents with severe obesity. Cardiovasc Diabetol. 2020;19(1):79. https://doi.org/10.1186/s12933-020-01052-1.
Lorenzo AD, Soldati L, Sarlo F, Calvani M, Lorenzo ND. Laura Di Renzo. New obesity classification criteria as a tool for bariatric surgery indication. World J Gastroenterol. 2016;22(2):681–703. https://doi.org/10.3748/wjg.v22.i2.681.
Carla Iacobini G, Pugliese CB, Fantauzzi M, Federici. Stefano Menini. Metabolically healthy versus metabolically unhealthy obesity. Metabolism. 2019;92:51–60. https://doi.org/10.1016/j.metabol.2018.11.009.
Angelica Artasensi A, Mazzolari A, Pedretti G, Vistoli. Laura Fumagalli Molecules. 2023;28(7):3094. https://doi.org/10.3390/molecules28073094.
Kolb R, Sutterwala FS, Zhang W. Obesity and cancer: inflammation bridges the two. Curr Opin Pharmacol. 2016;29:77–89. https://doi.org/10.1016/j.coph.2016.07.005. Epub 2016 Jul 16.
Saltiel AR, Olefsky JM. Inflammatory mechanisms linking obesity and metabolic disease. J Clin Invest. 2017;127(1):1–4. https://doi.org/10.1172/JCI92035.
Amin MN, Hussain MS, Sarwar MS, Rahman Moghal MM, Das A, Hossain MZ, Chowdhury JA, Millat MS, Islam MS. How the association between obesity and inflammation may lead to insulin resistance and cancer. Diabetes Metab Syndr 2019 Mar-Apr;13(2):1213–24. doi: 10.1016/j.dsx.2019.01.041. Epub 2019 Jan 29.
María C-R, Rueda-Medina B. Emilio González-Jiménez, Jorge Enrique Correa-Bautista, Robinson Ramírez-Vélez, Jacqueline Schmidt-RioValle. Dietary inflammatory index, bone health and body composition in a population of young adults: a cross-sectional study. Int J Food Sci Nutr. 2018;69(8):1013–9. https://doi.org/10.1080/09637486.2018.1446915.
Philip P, Cavicchia SE, Steck TG, Hurley JR, Hussey Y, Ma IS, Ockene. James R Hébert. A new dietary inflammatory index predicts interval changes in serum high-sensitivity C-reactive protein. J Nutr. 2009;139(12):2365–72. https://doi.org/10.3945/jn.109.114025.
Shivappa N, Steck SE, Hurley TG, Hussey JR, Hébert JR. Designing and developing a literature-derived, population-based dietary inflammatory index. Public Health Nutr. 2014;17(8):1689–96. https://doi.org/10.1017/S1368980013002115.
Mazidi M, Shivappa N, Wirth MD, Hebert JR, Mikhailidis DP, Kengne AP, Banach M. Dietary inflammatory index and cardiometabolic risk in US adults. Atherosclerosis. 2018;276:23–7. https://doi.org/10.1016/j.atherosclerosis.2018.02.020.
Hariharan R, Odjidja EN, Scott D, Shivappa N, Hébert JR, Hodge A, de Courten B. The dietary inflammatory index, obesity, type 2 diabetes, and cardiovascular risk factors and diseases. Obes Rev. 2022;23(1):e13349. https://doi.org/10.1111/obr.13349.
Shakya PR, Melaku YA, Shivappa N, Hébert JR, Adams RJ, Page AJ, Gill TK. Dietary inflammatory index (DII®) and the risk of depression symptoms in adults. Clin Nutr. 2021;40(5):3631–42. https://doi.org/10.1016/j.clnu.2020.12.031.
Sokol A, Wirth MD, Manczuk M, Shivappa N, Zatonska K, Hurley TG, Hébert JR. Association between the dietary inflammatory index, waist-to-hip ratio and metabolic syndrome. Nutr Res. 2016;36(11):1298–303. https://doi.org/10.1016/j.nutres.2016.04.004.
Mohsen Mazidi ED, Michos M, Banach. The association of telomere length and serum 25-hydroxyvitamin D levels in US adults: the National Health and Nutrition Examination Survey. Arch Med Sci. 2017;13(1):61–5. https://doi.org/10.5114/aoms.2017.64714.
Marielle F, Engberink 1, Stephan JL, Bakker EJ, Brink, Marleen A, van Baak, Frank JA, van Rooij A, Hofman, Jacqueline CM, Witteman, Johanna M, Geleijnse. Dietary acid load and risk of hypertension: the Rotterdam Study. Am J Clin Nutr. 2012;95(6):1438–44. https://doi.org/10.3945/ajcn.111.022343.
Lara Gomes Suhett HHM, Hermsdorff N, Shivappa JR, Hébert. Juliana Farias de Novaes. The dietary inflammatory index is associated with anti- and pro-inflammatory adipokines in Brazilian schoolchildren. Eur J Nutr. 2021;60(5):2841–2849. https://doi.org/10.1007/s00394-021-02500-8.
Pilar Navarro N, Shivappa JR, Hébert J, Mehegan CM, Murrin, Cecily C, Kelleher, Catherine MP, Lifeways Cross-Generation Cohort Study. Predictors of the dietary inflammatory index in children and associations with childhood weight status: a longitudinal analysis in the lifeways cross-generation Cohort Study. Clin Nutr. 2020;39(7):2169–79. https://doi.org/10.1016/j.clnu.2019.09.004.
Gholamalizadeh M, Ahmadzadeh M, BourBour F, Vahid F, Ajami M, Majidi N, Hajipour A, Doaei S, Kalantari N, Alizadeh A, Jarrahi AM. Associations between the dietary inflammatory index with obesity and body fat in male adolescents. BMC Endocr Disord. 2022;22(1):115. https://doi.org/10.1186/s12902-022-01001-x.
Luana Senna Blaudt. Taís De Souza Lopes, Amanda De Moura Souza, Edna Massae Yokoo, Camilla Medeiros Macedo Da Rocha, Rosangela Alves Pereira. Association between dietary inflammatory index and anthropometric indicators of adiposity in Brazilian adolescents. Pediatr Obes. 2023;18(5):e13011. https://doi.org/10.1111/ijpo.13011.
Drai CK-PJ, Oujaa M, Schlienger J-L, Chantal Simon. Plasma fatty acid composition is associated with the metabolic syndrome and low-grade inflammation in overweight adolescents. Am J Clin Nutr. 2005;82(6):1178–84. https://doi.org/10.1093/ajcn/82.6.1178.
Centers for Disease Control and Prevention. National Health and Nutrition Examination Survey (NHANES): MEC Laboratory Procedures Manual. Published January 2013. Accessed August 8., 2017. https://wwwn.cdc.gov/nchs/data/nhanes/2013-2014/manuals/2013_mec_laboratory_procedures_manual.pdf.
Craig M, Hales CD, Fryar MD, Carroll DS, Freedman, Cynthia L, Ogden. Trends in obesity and severe obesity prevalence in US youth and adults by sex and age, 2007–2008 to 2015–2016. JAMA. 2018;319(16):1723–5. https://doi.org/10.1001/jama.2018.3060.
Bo Xi J, Mi M, Zhao T, Zhang C, Jia J, Li T, Zeng, Lyn M, Steffen; Public Health Youth Collaborative and Innovative Study Group of Shandong University. Trends in abdominal obesity among U.S. children and adolescents. Pediatrics. 2014;134(2):e334–9. https://doi.org/10.1542/peds.2014-0970.
Nitin Shivappa SE, Steck TG, Hurley JR, Hussey. James R Hébert. Designing and developing a literature-derived, population-based dietary inflammatory index. Public Health Nutr. 2014;17(8):1689–96. https://doi.org/10.1017/S1368980013002115.
Zuheng Liu H, Liu Q, Deng C, Sun W, He W, Zheng R, Tang W, Li Q, Xie. Association between Dietary Inflammatory Index and Heart failure: results from NHANES (1999–2018). Front Cardiovasc Med. 2021;8:702489. https://doi.org/10.3389/fcvm.2021.702489.
Liu N, Feng Y, Luo X, Ma X, Ma F. Association between Dietary Inflammatory Index and Sex hormone binding globulin and sex hormone in U.S. adult females. Front Public Health. 2022;10:802945. https://doi.org/10.3389/fpubh.2022.802945.
Plan and operation of the Third National Health and Nutrition Examination Survey., 1988-94. Series 1: programs and collection procedures. Vital Health Stat 1. 1994;(32):1-407.
Hyattsville MD. US Department of Health and Human Services. Centers: Public Health Service; 1994.
National Center for Health Statistics. National Health and Nutrition Examination Survey: 2013–2014 Data Documentation, Codebook, and Frequencies. Physical Activity (PAQ_H). Centers for Disease Control and Prevention website. Published October 2015. Updated March 2017. Accessed August 5., 2017. https://wwwn.cdc.gov/Nchs/Nhanes/2013-2014/PAQ_H.htm.
Overwyk KJ, Zhao L, Zhang Z, Wiltz JL, Dunford EK, Cogswell ME. Trends in blood pressure and usual dietary sodium intake among children and adolescents, National Health and Nutrition Examination Survey 2003 to 2016. Hypertension. 2019;74:260–6.
2018 Physical Activity Guidelines Advisory Committee. 2018 Physical Activity Guidelines Advisory Committee Scientific Report US Department of Health and Human Services; 2018. https://health.gov/sites/default/files/2019-09/PAG_Advisory_Committee_Report.pdf.
Shu Y, Wu X, Wang J, Ma X, Li H, Xiang Y. Associations of Dietary Inflammatory Index with prediabetes and insulin resistance. Front Endocrinol (Lausanne). 2022;13:820932. https://doi.org/10.3389/fendo.2022.820932.
Yi Q, Li X, He Y, Xia W, Shao J, Ye Z, Song P. Associations of dietary inflammatory index with metabolic syndrome and its components: a systematic review and meta-analysis. Public Health Nutr. 2021;24(16):5463–70. https://doi.org/10.1017/S1368980021000288.
Varghese M, Griffin C, Singer K. The role of sex and sex hormones in regulating obesity-Induced inflammation. Adv Exp Med Biol. 2017;1043:65–86. https://doi.org/10.1007/978-3-319-70178-3_5.
Horst RT, Inge CL, van den Munckhof K, Schraa R, Aguirre-Gamboa M, Jaeger, Sanne P, Smeekens, et al. Sex-specific regulation of inflammation and metabolic syndrome in obesity. Arterioscler Thromb Vasc Biol. 2020;40(7):1787–800. https://doi.org/10.1161/ATVBAHA.120.314508.
Bordoni A, Danesi F, Dardevet D, Dupont D, Fernandez AS, Gille D, Nunes Dos Santos C, Pinto P, Re R, Rémond D, Shahar DR, Vergères G. Dairy products and inflammation: a review of the clinical evidence. Crit Rev Food Sci Nutr. 2017;57(12):2497–525. https://doi.org/10.1080/10408398.2014.967385.
Christ A, Lauterbach M, Latz E. Western Diet and the Immune System: an inflammatory connection. Immunity. 2019;51(5):794–811. https://doi.org/10.1016/j.immuni.2019.09.020.
Amin Gasmi S, Noor A, Menzel A, Doşa L, Pivina. Geir Bjørklund. Obesity and insulin resistance: associations with chronic inflammation, genetic and epigenetic factors. Curr Med Chem. 2021;28(4):800–26. https://doi.org/10.2174/0929867327666200824112056.
Torsten PM, Scheithauer E, Rampanelli M, Nieuwdorp BA, Vallance C, Bruce Verchere, Daniël H, van Raalte. Hilde Herrema. Gut microbiota as a trigger for metabolic inflammation in obesity and type 2 diabetes. Front Immunol. 2020;11:571731. https://doi.org/10.3389/fimmu.2020.571731.
Ashley Beam E, Clinger LH. Effect of Diet and Dietary Components on the composition of the gut microbiota. Nutrients. 2021;13(8):2795. https://doi.org/10.3390/nu13082795.
Tatsuo Kawai MV, Autieri R. Adipose tissue inflammation and metabolic dysfunction in obesity. Am J Physiol Cell Physiol. 2021;320(3):C375–91. https://doi.org/10.1152/ajpcell.00379.2020.
Malesza IJ, Malesza M, Walkowiak J, Mussin N, Walkowiak D, Aringazina R, Bartkowiak-Wieczorek J, Mądry E. High-Fat, Western-Style Diet, systemic inflammation, and gut microbiota: a narrative review. Cells. 2021;10(11):3164. https://doi.org/10.3390/cells10113164.
Dong Y, Zhu H, Chen L, Huang Y, Christen W, Cook NR, Copeland T, Mora S, Buring JE, Lee IM, Costenbader KH, Manson JE. Effects of vitamin D3 and Marine Omega-3 fatty acids supplementation on biomarkers of systemic inflammation: 4-Year findings from the VITAL randomized trial. Nutrients. 2022;14(24):5307. https://doi.org/10.3390/nu14245307.
Myette-Côté É, Durrer C, Neudorf H, Bammert TD, Botezelli JD, Johnson JD, DeSouza CA, Little JP. The effect of a short-term low-carbohydrate, high-fat diet with or without postmeal walks on glycemic control and inflammation in type 2 diabetes: a randomized trial. Am J Physiol Regul Integr Comp Physiol. 2018;315(6):R1210–9. https://doi.org/10.1152/ajpregu.00240.2018.
Battineni G, Sagaro GG, Chintalapudi N, Amenta F, Tomassoni D, Tayebati SK. Impact of obesity-Induced inflammation on Cardiovascular diseases (CVD). Int J Mol Sci. 2021;22(9):4798. https://doi.org/10.3390/ijms22094798.
Uzma Zafar S, Khaliq HU, Ahmad S, Manzoor, Khalid P, Lone. Metabolic syndrome: an update on diagnostic criteria, pathogenesis, and genetic links. Horm (Athens). 2018;17(3):299–313. https://doi.org/10.1007/s42000-018-0051-3.
Kristian Leisegang R, Henkel A, Agarwal. Obesity and metabolic syndrome associated with systemic inflammation and the impact on the male reproductive system. Am J Reprod Immunol. 2019;82(5):e13178. https://doi.org/10.1111/aji.13178.
Janet A, Tooze D, Midthune KW, Dodd, Laurence S, Freedman, Susan M, Krebs-Smith AF, Subar PM, Guenther, Raymond J, Carroll V, Kipnis. A new statistical method for estimating the usual intake of episodically consumed foods with application to their distribution. J Am Diet Assoc. 2006;106(10):1575–87. https://doi.org/10.1016/j.jada.2006.07.003.
Nitin Shivappa MD, Wirth TG, Hurley, James R, Hébert. Association between the dietary inflammatory index (DII) and telomere length and C-reactive protein from the National Health and Nutrition Examination Survey-1999-2002. Mol Nutr Food Res. 2017;61(4). https://doi.org/10.1002/mnfr.201600630.
Acknowledgements
Thanks to Zhang Jing (Shanghai Tongren Hospital) for his work on the NHANES database. His outstanding work, nhanesR package and webpage, makes it easier for us to explore NHANES database.
Funding
The study was supported by Guangdong Basic and Applied Basic Research Foundation (2020A1515010184).
Author information
Authors and Affiliations
Contributions
HB, YW, and LZ conceived and designed the study. HP collected data. HB wrote the paper. All authors contributed to the article and approved the submitted version.
Corresponding authors
Ethics declarations
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Ethics approval and consent to participate
The NCHS Research Ethics Review Committee approved the survey protocol and written informed consent was obtained from all participants. All methods were carried out in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Consent for publication
Not applicable.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zhang, L., Peng, H., Wang, Y. et al. Association of dietary inflammatory index with obesity among children and adolescents in the United States NHANES cohort: a population-based study. Ital J Pediatr 50, 14 (2024). https://doi.org/10.1186/s13052-024-01586-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13052-024-01586-0