
Abstract
Background
Maternal systemic lupus erythematosus (SLE) is at greater risk of pregnancy complications and is associated with increased risk of preterm delivery. However hardly any study has looked at the influence of SLE on the outcomes of preterm infants. This study aimed to explore the influence of SLE on the outcomes of preterm infants.
Methods
In this retrospective cohort study, preterm infants born to mothers with SLE from Shanghai Children’s Medical Center during 2012 to 2021 were enrolled. Infants were excluded if they were died during hospitalization or has major congenital anomalies and neonatal lupus. Exposure was defined as mother diagnosed SLE before or during pregnancy. Maternal SLE group was matched with Non-SLE group by gestational age, birth weight and gender. Clinical data has been extracted from patients’ records and registered. Major morbidities of premature and biochemical parameters in the two groups were compared using multiple logistic regression.
Results
One hundred preterm infants born to 95 mothers with SLE were finally enrolled. The mean (standard deviation) of gestational age and birth weight were 33.09 (7.28) weeks and 1768.50 (423.56) g respectively. There was no significant difference in major morbidities between SLE group and non-SLE group. Compared with non-SLE group, SLE off-spring had significantly lower leukocytes, neutrophiles after birth, neutrophils and platlet in one week (mean difference: -2.825, -2.001, -0.842, -45.469, respectively). Among SLE group, lower birth weight and smaller gestational age were observed in SLE mothers with disease active during pregnancy, kidney involved, blood system involved and not taking Aspirin during pregnancy. In the multivariable logistic regression analysis, exposure to aspirin during pregnancy reduced the risk of very preterm birth and increased the incidence of survive without major morbidities among preterm infants born to SLE mothers.
Conclusion
Born to mothers with SLE may not increase the risk of major premature morbidities, but the hematologic profile of SLE preterm infants may be different from preterm infants born to women without SLE. The outcome of SLE preterm infants is associated with maternal SLE status and may benefit from maternal aspirin administration.
Similar content being viewed by others

Background
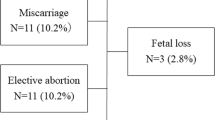
Systemic lupus erythematous (SLE) is an autoimmune disease that involves multiple organs and develops mainly in women of reproductive age. In the last decades, owing to improvements in multidisciplinary perinatal management, SLE was no longer viewed as a contraindication for pregnancy [1]. With the increase of pregnancy in women with SLE, numerous studies have reported that SLE is associated with increased risk of fetal complications including fetal loss, preterm delivery (20.8-28.7%)2,3,4,5, and intrauterine growth retardation.
Such studies have focused on the pregnancy outcomes of SLE [6,7,8,9] while there is only very few observational studies have assessed the outcome in preterm offspring of mothers with SLE [10]. Furthermore, pregnant women with SLE are at greater risk of thrombosis, infection, preeclampsia and multiple drugs would administrate during period of pregancy [11, 12], but hardly any study have looked at the influence of SLE on the outcome of preterm infants.
Understanding the outcomes of preterm infants born to SLE populations can inform clinical care and potentially provide mechanistic insight into such obstetric complication. Accordingly, the primary objective of this study is to assess the impact of SLE on premature newborns by comparing demographic data, prenatal and postnatal characteristics, laboratory data, and morbidities in a cohort of premature infants born to mothers with and without SLE. The secondary objective is to assess the influence of active SLE on preterm birth infants among infants with maternal SLE.
Materials and methods
Study design, setting and participants
This retrospective cohort study was carried out from February 2012 to May 2021 in the Neonatology Department of Shanghai Children’s Medical Center in Shanghai, China. Infants with preterm birth were included in this study. Infants with maternal SLE were identified from the database of medical records in our neonatology department born between February 2012 and May 2021. The exclusion criteria include: death during hospitalization, neonatal lupus and major congenital anomalies. The study participants were followed up until discharge.
Data collection
Data of all preterm participants were collected by trained data abstractor in Shanghai Children’s Medical Center. All SLE mothers in this study delivered in Ren Ji Hospital which located next to our hospital. Ren Ji Hospital is the largest prenatal center of both autoimmune disease and high-risk pregnancy in Shanghai. Almost all pregnant women with SLE in this region will give birth in Renji Hospital. Maternal history were collected by trained data abstractor in Ren Ji Hospital. Site investigators were responsible for data quality control in both hospitals. Data were collected using the same definition in both hospitals.
Exposure
SLE was diagnosed according to the revised criteria for the classification of SLE developed by the American College of Rheumatology [13] The non-SLE group was randomly selected from preterm infants admitted in our center. Non-SLE group were 1:2 matched with SLE group based on gender, birth weight (BW) ± 300 g, gestational age (GA) ± 6 days and date of birth ± 6 months. Infants in non-SLE group with major congenital anomalies, confirmed intrauterine infection, death during hospitalization and born to mother with other autoimmune diseases or malignant disease were excluded. The disease activity of SLE was made an appropriate evaluation based on the SLE Disease Activity Index 2000 (SLEDAI-2 K) [14].
Outcome
The primary outcome was defined as infants who survived without major morbidities. Major morbidities of premature included intraventricular hemorrhage (IVH) (grade ≥ 3) and/or cystic periventricular leukomalacia (PVL), necrotizing enterocolitis (NEC) (stage ≥ 2), sepsis, Retinopathy of prematurity (ROP) (stage ≥ 3), and bronchopulmonary dysplasia (BPD). IVH was defined as greater than or equal to grade 3 according to the Papile criteria [15]. Cystic PVL was defined as the presence of periventricular cysts identified on cranial ultrasonography or magnetic resonance imaging. NEC was defined according to Bell criteria [16, 17]. Sepsis was defined as positive blood or cerebrospinal fluid culture (Exception for specimen contamination) [18]. Retinopathy of prematurity was diagnosed according to the International Classification of Retinopathy of Prematurity [19]. Bronchopulmonary dysplasia was defined as treatment with FiO2 > 0.21 for at least 28 days plus failure of room air challenge test at 36 weeks’ postmenstrual age [20]. Secondary outcome included complete blood count, total bilirubin (TBil) and alanine aminotransferase (ALT).
Definitions of other covariates
Pregnancy-induced hypertension (PIH) was defined as an increase in blood pressure to ≥ 140/90 mmHg on at least two occasions ≥ 6 h apart that arises de novo after the 20th week of pregnancy. Preeclampsia (PE/E) was defined as pregnancy-induced hypertension with proteinuria > 0.3 g/L/d in the absence of a urinary tract infection or the abrupt onset of hypertension and proteinuria after 20 weeks of gestation. Seizures were required for a diagnosis of eclampsia. Gestational diabetes (GDM) was defined as any degree of glucose intolerance with onset or first recognition during pregnancy. HELLP (hemolysis, elevated liver enzymes and low platelet count) syndrome was defined as presence of hemolysis, high levels of lactate dehydrogenase or total bilirubin > 12 mg/L, elevated alanine aminotransferase levels of greater than twofold the upper normal value, and thrombocytopenia < 100*109/L. Small for gestational age (SGA) was defined as infants whose weight was lower than the lower 10% limit of the CI of the Fenton curve. An Apgar score > 7 was defined as normal, while a score ≤ 7 was considered indicative of moderate or severe hypoxia [21].
Statistical analysis
Normally distributed continuous data were expressed as mean and standard deviation (SD) and differences between two groups were tested by independent t-test. Categorical variables were presented with frequency and percentage and using chi-square test to exam the differences among groups.
In order to determine the association of neonatal outcome with maternal SLE in preterm birth, we performed multiple logistic regression analysis after adjustment of 1 min Apgar score and delivery type. Multiple linear regression was also performed in order to determine the association between maternal SLE and biochemical parameters. Log-transformation was conducted if biochemical parameters were not normally distributed before conducting linear regression.
Bi-variate analysis of baseline and neonatal outcome was conducted between active SLE and non-active SLE during pregnancy. In order to further investigate the effect of active SLE during pregnancy on neonatal outcome among infants born to maternal SLE, Multiple logistic regression analysis was conducted after adjustment of potential confounders. Each variable which has p-value < 0.1 was entered into the multivariable logistic regression model to control possible confounders. All tests were two-tailed, and p < 0.05 was considered statistically significant. Statistical analysis was performed using SPSS 22.0 and R 4.1.2.
Ethics statement
This study protocol was reviewed and approved by the Ethics Board of Shanghai Children’s Medical Center, School of Medicine, Shanghai Jiao Tong University (SCMCIRB-K2021016-1). Written informed consent was obtained from all participants’ legal guardian. Approval to obtain clinical data from the database was received from the office of the medical director of the hospital. All patient information was kept confidential.
Results
Clinical characteristics of SLE mothers
One hundred and two preterm infants born to SLE mothers were found from the clinical database. One died during hospitalization, 1 diagnosed with neonatal lupus syndrome were excluded. The remaining 100 preterm infants were born to 95 mothers with SLE. The mean maternal age was 30.63 years with 6.61 years of disease duration. Disease active occurred in 46.3% of pregnancies. Renal manifestation was most common in these mothers (44.2%). During pregnancy, 91 mothers (95.8%) were taking steroids, 67 mothers (70.5%) were taking hydroxychloroquine (HCQ), 16 mothers (16.8%) were taking cytotoxic drugs including azathioprine and cyclosporine, and 75 mothers (78.9%) were taking aspirin. Mean positive antibodies were confirmed in mothers at onset of pregnancy as follows; anti-SSA/Ro antibody (47.9%), anti-SSB/La antibody (10.6%), dsDNA antibodies (57.4%) and antiphospholipid antibodies (aPLs) (5.3%). 57.9% mothers had pregnancy complications. Pregnancy induced hypertension was the most common complication in this cohort (37%). Characteristics of 95 SLE mothers are shown in Table 1.
Major morbidities and biochemical parameters: comparison between SLE group and non-SLE group
According to the matching strategy described previously, 98 infants born to mothers with SLE (SLE group) were matched to 196 preterm infants born to mothers without SLE (non-SLE group). The clinical characteristics of two groups were listed in Table 2.
The intact survival rate was 83.7% in the SLE group, and 75% in the non-SLE group, there was no statistic difference between the two groups. Besides no significant difference was found in the incidence of BPD, PVL, ROP, NEC, Sepsis nor in CHD (congenital heart disease) respectively between the two groups (Table 2).
Neonatal lupus erythematosus presents with 35% hematological abnormalities including anemia, neutropenia or thrombocytopenia and 15–25% asymptomatic elevation of aminotransferases, cholestasis, or hepatomegaly/splenomegaly due to the maternal antibodies exposure [22]. Thus we further compared clinical biochemical parameters between two groups. Compared with non-SLE group, Leukocyte and Neutrophile were significantly lower in SLE group at day 1. After one week, there was no difference in leukocyte between the two groups, but neutrophils in the SLE group was still significantly lower (p = 0.014), and platelet were also significantly lower (p = 0.001) than non-SLE group. No significant differences were observed in Hemoglobin, maximum ALT and TBil (Table 2).
Multivariate logistic regression of relationship between maternal SLE and outcomes of premature infants showed same result when delivery mode and 1 min Apgar score were included as covariates (Tables 3 and 4).
Maternal influence on the outcomes of SLE preterm offspring
Among the 100 SLE preterm offspring, there were 52 males (52%) and 48 females (48%) including 5 pairs of twins. The mean GA of them was 33.09 ± 2.08 weeks, 1% was less than 28 weeks and 24% were between 28 and 32 weeks (Fig. 1). The mean birth weight was 1768.50 ± 423.56 g, 6% were less than 1000 g, 18% were between 1000 and 1500 g (Fig. 2). 36% were SGA.

Gestational age distribution diagram of SLE preterm offspring

Birth weight distribution diagram of SLE preterm offspring
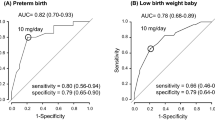
We analyzed the influence of maternal status on SLE offspring which including SLE active, previous manifestations, medications exposure during pregnancy, positive antibodies and pregnancy complications. We found that SLE active during pregnancy, renal and blood system involvement, pregnancy complications, aspirin and HCQ administration were associated with offspring GA and birth weight. There was no difference in birth weight, gestational age and major morbidities between preterm infants of SLE mothers with positive aPLs and those with negative aPLs. (Supplementary Table 1). Univariate analysis displayed that very preterm birth (GA less than 32 weeks) was associated with blood systerm involvement, pregnancy complications and aspirin administration (Supplementary Table 2). In the multivariable logistic regression analysis, exposure to aspirin during pregnancy reduced the risk of very preterm birth (OR = 0.249, p = 0.033) and pregnancy complications were increased the risk of very preterm birth (OR = 3.018, p = 0.043) (Table 5). Univariate analysis displayed that survive without major morbidities was only associated with aspirin administration (p = 0.014, OR = 4.248, 95%CI: 1.343–13.431) (Supplementary Table 3). Multivariable logistic regression analysis also indicated that only aspirin administration during pregnancy were associated with survive without morbidities (p = 0.013) (Table 6).
We further tested whether the association between taking aspirin and survival without major morbidities was mediated by GA. Firstly univariate logistic regression result showed that there was no significant relationship between maternal taking aspirin and survival without major morbidities in very preterm infants. Then we conducted mediation analyses. As shown in Fig. 3, the results of mediation analyses showed that the total effect of maternal taking aspirin on survival without major morbidities was significant (B=-0.226, p < 0.001). Besides, the average causal mediation effects (ACME) between maternal taking aspirin and survival without major morbidities through gestatinal age was − 0.121 (p < 0.001), and the 95% bias-corrected bootstrap confidence interval was − 0.221 to -0.05, which indicated that the indirect effect of maternal taking aspirin on survival without major morbidities was statistically significant. In addition, the direct effect of maternal taking aspirin on survival without major morbidities (ADE=-0.105, p = 0.16) was not significant, indicating that GA mediated the relationship between maternal taking aspirin on survival without major morbidities. Univariate logistic regression analysis showed that taking aspirin was not associated with intact survival rate in the subgroup of very preterm infants (Supplementary Table 4).

Schematic model of gestational age as the mediator between taking aspirin during pregnancy and survival without major morbidities in SLE group
Discussion
In this retrospective cohort study, we found that there was no significant difference of major morbidities between SLE group and non-SLE group. However, SLE preterm offspring showed a hematologic profile that is different from that of non-SLE preterm offspring, with lower leukocyte counts, lower neutrophile and lower platlet.
The intact survival rate was 83.7% and the average GA was 33 weeks in SLE group, only 1% premature infants had a GA less than 28 weeks of which had most morbidities. No significant difference was found in each single morbidity including BPD, PVL, ROP, NEC, and Sepsis between the two groups. Mei-Ying et al. reported that SLE preterm offspring had much higher rate of neonatal infection as compared to preterm babies from women without SLE (47.62% vs. 16.81%)11. In their study the mean GA was 33 weeks plus 4 days which was similar as our study subject, the definition of sepsis in our study was positive blood or cerebrospinal fluid culture while their definition of neonatal infection was covering a wider range. Our definition was more precise, the broad definition may lead to bias. Furthermore, the non-SLE group they enrolled was all other premature infants delivered during the same time period, whereas our study matched the individuals’ GA and weight, excluding the confounding facts of varied GA and weight.
In our study hematological abnormalities were rare in both groups, however significant lower leukocyte, neutrophile and platelets were found in SLE preterm offspring than in non-SLE group. Maria Gariup et al. found that SLE Offspring (mean age 14.9 years) showed an immune profile that is different from relevant health control, with lower leukocyte counts and higher levels of mainly proinflammatory cytokines [23]. Besides their study showed SLE offspring had significantly higher proportions of history of nonallergic autoimmune conditions, and asthma was more frequent in SLE offspring than in health control. A cohort of 719 SLE offspring revealed that instead of rheumatic autoimmune disease, children born to women with SLE had an increased risk of non-rheumatic autoimmune diseases [24]. All these suggested that SLE offspring may have proinflammatory and autoimmune activation. The alteration in immune profile of SLE offspring seems to last for a long duration after birth while the maternal antibodies including Anti-SSA and anti-SSB in the offspring circulation are progressively reduced after birth and diappeared at about 12-month [25]. This phenomenon cannot be simply explained by maternal antibodies directed against auto-antigens in the fetal blood stream. Studies indicate that multiple molecular as well as cellular components originating in pregnant women are transferred to the fetus and program the fetal immune system [26]. SLE pregnancy might modify these signals and may consequently alter immunity in early life and childhood. On the other hand, the previous studies have proven familial risks between rheumatic autoimmune diseases (RAIDs), and SLE was associated with four of five RAIDs [27]. Further studies have highlighted a genetic component in the onset of SLE and other autoimmune diseases that may lead to several different phenotypes even though the genotype is the same [28]. Many of the shared loci were related to immune processes, such as interferon signalling and polymorphisms of STAT genes that may have a wide spectrum of phenotype [28, 29].
The incidence of CHD in this study was much higher than previous reports and with no difference from the non-SLE group. In a large population-based study conducted by Evelyne Yinet et al., reported that in comparison with children from the general population, children born to women with SLE have an increased risk of CHD 5.1% [95% CI, 3.7–7.1] versus 1.9% [95% CI, 1.6–2.2] [30]. One potential reason for these differences in the incidence of CHD is that the GA was significant different between two studies. The mean GA of SLE offspring in their study was 37.7 weeks which was significant different from control children whose mean GA was 38.8 weeks. Epidemiologic study suggests that premature neonates have a more than 2-fold higher risk of cardiovascular abnormalities [31]. CHD is more likely to be associated with prematurity instead of SLE.
In our study the maternal age, SLE disease duration, SLE active, and antibodies characteristics were similar as several studies previously reported in Asia [4, 32,33,34]. The incidence of pregnancy complications in this cohort was significantly higher than other SLE cohorts. The results of our study showed that PIH and preeclampsia are the significant problems in SLE pregnancies with preterm infants. In our study, nearly one-third of SLE mothers were complicated with PIH and preeclampsia, whereas according to previous studies only 3.1–19.2% of the pregnancies in SLE women were affected by such conditions [4, 35]. Several studies have explored that PIH can significantly increase the risk of preterm birth [36], while our subjects are all preterm infants. Yen-Ju Chen et al. has reported that preterm risks increased markedly in participants with both preeclampsia/eclampsia and SLE (OR: 17.5, 95% CI: 12.6_24.1, p < 0.01)32. Therefore, the high incidence of PIH and preeclampsia in our cohort is understandable and we speculate that SLE pregnant women complicated with PIH/PE are more likely to give birth prematurely than those SLE mothers without PIH/PE.
The rate of cesarean section in SLE group was significantly higher than non-SLE group in this study (91.8% vs. 78.5%). Jae-kyoon Hwang et al. reported a slightly lower cesarean section rate by 84.8% in preterm SLE offspring [37]. In SLE women, the general cesarean rate was previously reported to be 30-40%2,38,39,40. In our study, high cesarean section rate could be the confounding factor of SLE, premature birth and high rate of PIH/PE.
Further analysis in this study showed that maternal status including SLE active during pregnancy, renal and blood system involvement and pregnancy complications were associated with smaller offspring GA and lower offspring birth weight. Studies have showed that maternal SLE activity in the last 6–12 months or at conception increased the risk of maternal disease activity (subsequent flare during pregnancy and puerperium) and hypertensive complications, fetal morbidity and mortality [41, 42]. Considering the high risk of active SLE during pregnancy, EULAR (European League Against Rheumatism) recommends that SLE patients plan their pregnancies at least 6 months after achieving remission [42].
Taking aspirin during pregnancy was associated with larger offspring GA and higher offspring birth weight in this study, besides analysis also indicated that aspirin administration during pregnancy would increase the rate of survival without major morbidities. Because of the significant risk of preeclampsia in all lupus pregnancies, especially those with preexisting renal impairment or active lupus, low-dose aspirin is indicated in all women with SLE starting around 12 weeks gestation [43]. There is no study reported the long-term effect of aspirin on offspring outcomes. Here according to the mediation model, GA interaction can explain the effect of aspirin on survival without major morbidities 51.7% which means aspirin reduces morbidities of preterm infants by increasing gestational weeks. Besides, univariate logistic regression analysis showed that in very preterm infants of taking aspirin during pregnancy with survive without major morbidities in among SLE group.
To our knowledge, this was the first retrospective cohort study based on nearly 10 years clinical data of preterm infants born to mothers with SLE. Additionally almost every key influence of the SLE pregnancy on preterm infants was included in this study. Nevertheless, there were several limitations to our study. Firstly, the sample size of this retrospective study is not very large and the actual sample size for preterm morbidities comparison was considerably small, however, the sample size of this study is one of the largest sample sizes of all studies at present. Secondly, in order to control confounding factors, the matching criteria in this study are relatively strict, we can only achieve 1: 2 matching. Finally, the end point of our study was discharge. The long-term outcome is very important for preterm infants. In the future, we may carry out a prospective cohort study of preterm offspring of SLE.
Conclusion
Born to mothers with SLE may not increase the risk of major premature comorbidities, but the hematologic profile of SLE preterm infants may be lower than preterm infants born to women without SLE. The outcome of preterm infants is associated with maternal SLE status and may benefit from maternal aspirin administration.
Data Availability
The original contributions presented in the study are included in the article/supplementary material, futher inquiries can be directed to the corresponding authors.
References
Meyer O. Making pregnancy safer for patients with lupus. Joint, bone, spine: revue du rhumatisme. 2004;71(3):178–182.
Clowse ME, Jamison M, Myers E, James AH. A national study of the complications of lupus in pregnancy. American journal of obstetrics and gynecology. 2008;199(2):127.e121-126. Graziela Carvalheiras, Raquel Faria, Jorge Braga, Fetal outcome in autoimmune diseases. Autoimmunity Reviews 11 (2012) A520–A530.
Normand G, Sens F, Puthet J, Jourde-Chiche N, Lemoine S, Chauveau D, et al. Not only disease activity but also chronic hypertension and overweight are determinants of pregnancy outcomes in patients with systemic lupus erythematosus. Lupus. 2019;28:529–37.
Jiayue WU, Jinghang MA, Chunde BAO. et, al. Pregnancy outcomes among Chinese women with and without systemic lupus erythematosus:a retrospective cohort study. BMJ Open. 2018 Apr13;8(4):e020909.
Ko HS, Ahn HY, Jang DG, Choi SK, Park YG, Park IY, et al. Pregnancy outcomes and appropriate timing of pregnancy in 183 pregnancies in korean patients with SLE. Int J Med Sci. 2011;8:577–83.
Fanouriakis A, Tziolos N, Bertsias G. Et, al. Update οn the diagnosis and management of systemic lupus erythematosus. Ann Rheum Dis. 2021 Jan;80(1):14–25.
Petri M. Pregnancy and systemic Lupus Erythematosus. Best Pract Res Clin Obstet Gynaecol. 2020 Apr;64:24–30.
Moroni G, Ponticelli C. Pregnancy in women with systemic lupus erythematosus (SLE). Eur J Intern Med. 2016 Jul;32:7–12.
Marder W. Update on pregnancy complications in systemic lupus erythematosus. Curr Opin Rheumatol. 2019 Nov;31(6):650–8.
Mei-Ying QUAN, Dan-Hua WANG. Clinical features of preterm infants born to m others with systemic lupus erythem atosus: a retrospective analysis. Chin J Contemp Pediatr. 2013 Dec;15(12):1045–9.
Lazzaroni MG, Dall’Ara F, Fredi M. Et, al. A comprehensive review of the clinical approach to pregnancy and systemic lupus erythematosus. J Autoimmun. 2016 Nov;74:106–17.
Nalli C, Iodice A, Andreoli L, et. The effects of lupus and antiphospholipid antibody syndrome on foetal outcomes. Lupus. 2014 May;23(6):507–17.
Hochberg MC. Updating the American College of Rheumatology revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum. 1997;40(9):1725.
Touma Z, Urowitz MB, Taghavi-Zadeh S, et al. Systemic lupus erythematosus disease activity index 2000. J Rheumatol. 2002;29(2):288–91.
Papile LA, Burstein J, Burstein R, Koffler H. Incidence and evolution of subependymal and intraventricular hemorrhage: a study of infants with birth weights less than 1,500 gm. J Pediatr. 1978;92(4):529–34.
Bell MJ, Ternberg JL, Feigin RD, et al. Neonatal necrotizing enterocolitis: therapeutic decisions based upon clinical staging. Ann Surg. 1978;187(1):1–7.
Walsh MC, Kliegman RM. Necrotizing enterocolitis: treatment based on staging criteria. Pediatr Clin North Am. 1986;33(1):179–201.
Stoll BJ, Hansen N, Fanaroff AA et al. Late-onset sepsis in very low birth weight neonates: the experience of the NICHD Neonatal Research Network. Pediatrics. 2002;110(2, pt 1):285–291.
Gole GA, Ells AL, Katz X, et al. International Committee for the classification of retinopathy of Prematurity. The International classification of retinopathy of Prematurity revisited. Arch Ophthalmol. 2005;123(7):991–9.
Jobe AH, Bancalari E. Bronchopulmonary dysplasia. Am J Respir Crit Care Med. 2001;163(7):1723–9.
Iliodromiti S, Mackay DF, Smith GC, Pell JP, Nelson SM. Apgar score and the risk of cause-specific infant mortality: a population-based cohort study. Lancet (London England). 2014;384(9956):1749–55.
Diaz-Frias J, Badri T, Neonatal. Lupus Erythematosus. 2021 Jun 30.
Gariup M, Lera-Miguel S. Ferrán Torres, et, al. Autoantibodies, elevated cytokines, and neurocognitive abnormalities in offspring of women with systemic lupus erythematosus: comparison with healthy controls. Clin Rheumatol. 2019 Sep;38(9):2529–39.
Julie Couture S, Bernatsky S, Scott, et al. Brief report: risk of Childhood Rheumatic and Nonrheumatic Autoimmune Diseases in Children Born to Women with systemic Lupus Erythematosus. Arthritis Rheumatol. 2018 Nov;70(11):1796–800.
Zuppa AA, Riccardi R, Frezza S. Et, al. Neonatal lupus: follow-up in infants with anti-SSA/Ro antibodies and review of the literature. Autoimmun Rev. 2017 Apr;16(4):427–32.
Jennewein MF, Abu-Raya B, Jiang Y. Transfer of maternal immunity and programming of the newborn immune system. Semin Immunopathol. 2017 Nov;39(6):605–13.
Thomsen H, Li X, Sundquist K, et al. Familial associations for rheumatoid autoimmune diseases. Rheumatol Adv Pract. 2020 Sep;22(2):rkaa048.
Acosta-Herrera M, Kerick M, González-Serna D, et al. Genome-wide meta-analysis reveals shared new loci in systemic seropositive rheumatic diseases. Ann Rheum Dis. 2019;78:311–9.
Acosta-Herrera M, Kerick M, González-Serna D, et al. Genome-wide meta-analysis reveals shared new loci in systemic seropositive rheumatic diseases. Ann Rheum Dis. 2019;78:311–9.
Évelyne Vinet CA, Pineau. Susan Scott, et, al. Increased congenital heart defects in children born to women with systemic lupus erythematosus: results from the offspring of Systemic Lupus Erythematosus Mothers Registry Study. Circulation 2015 Jan 13;131(2):149 – 56.
David M, Axelrod, Valerie Y, Chock V, Mohan Reddy. Management of the Preterm infant with congenital heart disease. Clin Perinatol. 2016 Mar;43(1):157–71.
Chen Y-J, Chang J-C, Lai E-L. Maternal and perinatal outcomes of pregnancies in systemic lupus erythematosus: a nationwide population-based study. Semin Arthritis Rheum. 2020 Jun;50(3):451–7.
Firouzeh Nili L, McLeod. Colleen O’Connell, et, al. Maternal and neonatal outcomes in pregnancies complicated by systemic lupus erythematosus: a population-based study. J Obstet Gynaecol Can. 2013 Apr;35(4):323–8.
Hamijoyo L, Martha JW, Hidayat S. Et, al. Risk factors for poor pregnancy outcome in systemic Lupus Erythematosus Patients. Acta Med Indones. 2019 Apr;51(2):102–9.
Goldenberg RL, Culhane JF, Iams JD. et,al. Epidemiology and causes of preterm birth. Lancet. 2008 Jan5;371(9606):75–84.
Hwang JK, Park HK, Sung YK. Maternal outcomes and follow-up of preterm and term neonates born to mothers with systemic lupus erythematosus. J Matern Fetal Neonatal Med. 2018 Jan;31(1):7–13.
Jakobsen IM, Helmig RB, Stengaard-Pedersen K. Maternal and foetal outcomes in pregnant systemic lupus erythematosus patients: an incident cohort from a stable referral population followed during 1990–2010. Scand J Rheumatol. 2014;43:85.
Bramham K, Hunt BJ, Bewley S, Germain S, Calatayud I, Khamashta MA, et al. Pregnancy outcomes in systemic lupus erythematosus with and without previous nephritis. J Rheumatol. 2011;38:1906–13.
Wallenius M, Salvesen K, Daltveit AK, Skomsvoll JF. Systemic Lupus Erythematosus and Outcomes in First and subsequent births based on data from a National Birth Registry. Arthritis Care and Research. 2014;66(11):1718–24.
Lu Y, Yu Y, Xia W. Pregnancy outcomes in different stages of systemic lupus erythematosus among chinese women-a retrospective cohort study. Ginekol Pol. 2021;92(5):365–70.
Liu J, Zhao Y, Song Y. Pregnancy in women with systemic lupus erythematosus: a retrospective study of 111 pregnancies in chinese women. J Matern Fetal Neonatal Med. 2012 Mar;25(3):261–6.
Andreoli L, Bertsias GK, Agmon-Levin N. Et, al. EULAR recommendations for women’s health and the management of family planning, assisted reproduction, pregnancy and menopause in patients with systemic lupus erythematosus and/or antiphospholipid syndrome. Ann Rheum Dis. 2017 Mar;76(3):476–85.
Amelie M, Schramm MEB, Clowse. Aspirin for prevention of preeclampsia in lupus pregnancy. Autoimmune Dis. 2014;2014:920467.
Acknowledgements
The authors would like to thank Dr. Yanchen Wang for the help in the preliminary statistical analysis.
Funding
This study was supported by Shanghai Municipal Health Commission (Grant No. GWV-10.2-YQ12 to JY W), and Clinical research project of Shanghai Children’s Medical Center (LY-SCMC2020-01).
Author information
Authors and Affiliations
Contributions
XC and WD conceptualized and designed the study, drafted the initial manuscript, and reviewed and revised the manuscript. LY, YH, MJ, JW and JB, JS designed the data collection instruments, collected data, carried out the initial analyses, and reviewed and revised the manuscript. FB conceptualized and designed the study, coordinated and supervised data collection, and critically reviewed the manuscript for important intellectual content. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study protocol was reviewed and approved by the Ethics Board of Shanghai Children’s Medical Center, School of Medicine, Shanghai Jiao Tong University (SCMCIRB-K2021016-1). All methods were performed in accordance with the ethical standards as laid down in the Declaration of Helsinki and its later amendments or comparable ethical standards. Written informed consent was obtained from all participants’ legal guardian.
Consent for publication
Not applicable.
Competing Interests
The authors have no conflicts of interest relevant to this article to disclose.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Chen, X., Di, W., Ye, L. et al. Association of preterm outcome with maternal systemic lupus erythematosus: a retrospective cohort study. Ital J Pediatr 49, 43 (2023). https://doi.org/10.1186/s13052-023-01436-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13052-023-01436-5