
Abstract
Background
Combined simultaneous arginine clonidine stimulation (CSACS) test represents a more appropriate stimulus to detect Ghrelin, for it does not affect glucose metabolism.
Methods
Fifty prepubertal children with dwarfism were recruited and further classified into normal growth hormone (NGH) and growth hormone deficiency (GHD) group with growth hormone (GH) peak cut-off value of 10 μg/l. In both groups, GH and Ghrelin serum levels were determined after the GH provocation test at 30, 60, and 120 min and the height standard deviation score (SDS) for bone age was measured six months later.
Results
The participants were classified into NGH (n = 24) and GHD group (n = 26). A decrease in the circulating Ghrelin levels prior to the GH peak was observed in the NGH children, whereas both GH and Ghrelin levels demonstrated a rise in the GHD children. Ghrelin level in GHD group was higher compared with NGH group and the GH peak in GHD group is lower than NGH group. The 6 months CSACS treatment could increase the height SDS in both groups.
Conclusion
Although analogous changes were not detected in GHD group, the inverse correlation between GH and Ghrelin in NGH indicates a negative feedback lying between GH and Ghrelin.
Similar content being viewed by others

Background
Dwarfism can be defined as a standing height more than two standard deviations below the average or below the 3rd percentile (for sex and age) [1,2,3]. Achondroplasia and growth hormone deficiency (GHD) are responsible for the majority of children dwarfism cases. Excluding other serious diseases, the diagnosis of GHD is usually confirmed by a growth hormone (GH) provocation test where different GH secretagogues (insulin, clonidine, glucagon, arginine, and L-dopa) can be chosen to detect GH peak [4, 5]. In order to improve the discrimination, consecutive tests are suggested. It is worth noting that the further consecutive tests can be affected by down-regulated hypothalamic/pituitary axis which makes the diagnosis of GHD a clinical challenge [6].
Ghrelin is a 28 amino-residue peptide hormone produced by ghrelinergic cells in the gastrointestinal tract which is initially considered to have growth hormone-releasing function and can act as the endogenous ligand of the growth hormone secretagogue receptor type 1α. Due to the strong association with glucose metabolism, the utility of glucagon or insulin for GH provocation may be unsuitable to detect Ghrelin.
Clonidine, as an α-adrenergic agonist to be used as an anti-hypertensive drug, does not affect glucose metabolism and could not only inhibit somatostatin to stimulate the release of GH but also increase the secretion of growth hormone releasing hormone. Arginine can inhibit the release of somatostatin. Thus, the combined arginine and clonidine test could represent a more appropriate stimulus to detect Ghrelin. Some research is performed to optimize the sensitivity and specificity of the combined arginine and clonidine test, the detection time course is shortened [7, 8] and the sequential way of administration is changed into simultaneous delivery [9, 10], which show the similar or even better diagnostic accuracy.
In this study, combined simultaneous arginine clonidine stimulation (CSACS) and treatment in children with dwarfism are performed and dynamic Ghrelin and GH serum levels are monitored.
Methods
Subjects
Fifty children (27 boys and 23 girls, age between 8 to 12 years) with dwarfism or restricted growth were recruited in this studied from March 2016 to March 2018 in Jiangdu People’s Hospital of Yangzhou. Before entering the study, the children were given a thorough physical examination, biochemical test (renal, liver, and thyroid function), and neurological examination, without serious chronic disease, intrauterine growth retardation, or unremarkable personal medical history. The growth charts were used to calculate standard deviation score (SDS) as previously reported [11, 12]. All the study procedure was approved by the Ethics Committee of the Jiangdu People’s Hospital of Yangzhou and informed written consents were got from guardians of all participants.
Combined simultaneous arginine clonidine stimulation
CSACS test was performed as previously reported [10]. After overnight fast, an intravenous catheter was administrated in the antecubital vein to infuse Arginine (arginine hydrochloride, 10% solution, Sigma, St. Louis, MO, USA) at a dose of 0.5 g/kg (maximum 30 g, over 30 min) and clonidine (Catapresan, Boehringer, Germany) was administrated orally at a dose of 0.15 mg/m2. Blood pressure was strictly monitored during the whole procedure and blood samples were drawn at baseline, 30, 60, and 120 min after the arginine infusion.
GH reserve or the peak GH response was defined biochemically by the peak serum concentration after CSACS. Serum GH level was determined by immunoradiometric assay (IRMA) (Auto Delfia, Wallac Turku, Finland) and the lower detection limit was 0.01 μg/l. The cut-off value was set at 10 μg/l to classify the dwarfism participants into GHD group and the normal growth hormone (NGH) group.
Ghrelin and IGF-1 assay
A commercially available radioimmunoassay kit (Phoenix Pharmaceuticals, Inc. Belmont, CA, USA) was used to measure the serum level of Ghrelin which used a rabbit polyclonal antibody against octanoylated human Ghrelin and a 125I-labeled Ghrelin tracer. Insulin-like growth factor 1 (IGF-1) levels were determined by a fully automated, two-site chemiluminescent immunoassay (Nichols Advantage®, Nichols Institute Diagnostics).
The height standard deviation score
The effect of CSACS on growth was confirmed by comparison of height standard deviation score (SDS) which showed the number of standard deviations below or above the mean value of the height [13].
Statistical analyses
A t-test was used to assess the differences between GHD and NGH group. Paired samples t-test was used to calculate the changes in different time intervals compared with baseline during CSACS.
Results
Combined simultaneous arginine clonidine stimulation increase GHD serum ghrelin level
50 children diagnosed as dwarfism were further classified into two groups according to cut-off value (peak GH, 10 μg/l): the GHD group (n = 26) and the NGH group (n = 24). The relevant clinical and biochemical characteristics of the participants were shown in Table 1 and the two groups showed no differences in sex, age, body weight, height, and the baseline Ghrelin levels. When compared with NGH group, GHD group showed decreased serum levels of GH peak (Fig. 1a, p < 0.01) and IGF-1 (Fig. 1b, p < 0.05).

Serum levels of GH peak (a) and IGF-1 (b) were analyzed in the NGH and GHD groups. Data were shown as mean ± sd, p < 0.05*, p < 0.01**
After the CSACS test, participants with GHD demonstrated an increase in serum Ghrelin level at 30, 60, and 120 min compared to baseline, while circulating Ghrelin in the NGH group was lower than baseline. When compared with NGH group, Ghrelin levels in the GHD group were significantly higher at 30 (p < 0.05), 60 (p < 0.01), and 120 min (p < 0.01) post the CSACS test (Fig. 2).

Serum levels of Ghrelin during combined simultaneous arginine clonidine stimulation test were evaluated in the NGH and GHD groups. Data were shown as mean ± sd, p < 0.05*, p < 0.01** when GHD group compared with NGH group
The mean Ghrelin and GH fluctuations within NGH and GHD groups were demonstrated in Fig. 3. Ghrelin levels at GHD group increased after 30, 60, and 120 min of the CSACS, while decreased in NGH group. GH levels decreased at 30 min and significantly increased at 60 and 120 min compared to baseline in the GHD group (Fig. 3a), while in the NGH participants, increased GH could be observed at 30 and 60 min compared with the previous time interval and then GH secretion decreased a little (Fig. 3b). GH level was higher in the NGH group at 30, 60, and 120 min compared with the GHD group. It was worth noting that the serum levels of Ghrelin and GH in GHD group showed a clear correlation.

Serum Ghrelin and GH values during combined simultaneous arginine clonidine stimulation test were evaluated in the NGH (a) and GHD (b) groups. Data were shown as mean ± sd
Arginine and clonidine treatment could accelerate the height SDS for bone age
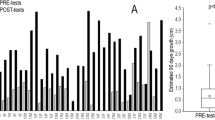
The 6 months CSACS treatment could increase the height SDS for bone age in both NGH and GHD groups which could be used as a measure of growth prognosis. The decreasing negative scores after the stimulation test indicated that the growth acceleration of children in NGH and GHD groups were gradually increased and got closer to the average height (Fig. 4).

Change in height standard deviation score (SDS) for bone age between NGH and GHD groups after 6 months arginine and clonidine treatment
Discussion
Dynamic detection shows that CSACS can induce different Ghrelin and GH responses pattern in the GHD and NGH groups. Compared with the NGH participants, Ghrelin levels in the GHD group are higher at 30, 60, and 120 min after CSACS test, while the GH peak in GHD group is lower than NGH group. Circulating Ghrelin and GH show an inverse correlation prior to the GH peak in NGH group; while in the GHD group, an increase in serum GH levels is followed by the accelerating circulating Ghrelin. The dynamic change pattern of Ghrelin and GH in the GHD and NGH groups are difficult to interpret for these subjects involved may have different genetic traits [14, 15] and the participants sample recruited is relative small [16, 17]. The results of the present study need to be confirmed in future larger clinical trials and more detailed genetic information should be considered.
Although Ghrelin is not the principal stimulator of GH synthesis and secretion, it has a marked growth hormone-stimulating activity which can link gastrointestinal-pituitary axis and bind with the growth hormone secretagogue receptor to stimulate IP3 signal transduction pathway to promote GH release [18]. While in our research, the rise in circulating GH is positively correlated with Ghrelin in GHD group and negatively correlated with Ghrelin in NGH group prior to the GH peak, which indicates that Ghrelin might be inhibited by the secretion of GH provoked by CSACS and a feedback loop between GH and Ghrelin may exist.
Height growth results from the proliferation of chondrocyte and the hypertrophy of the growth plates which can mainly attribute to GH stimulation [19, 20]. IGF-1, also called somatomedin C, is a primary mediator of the effects of GH, which plays a vital role in childhood growth and adults anabolic process. Mecasermin, a synthetic analog of IGF-1, is designed to treat growth failure. Because IGF-1 secretion can maintain a constant daily level and GH level shows large diurnal fluctuation, IGF-1 was considered as surrogate measures of GH secretion [21, 22], which turns out not sensitive enough to diagnose GHD [23, 24]. Our study demonstrates some positive relationship between GH and IGF-1 in both NGH and GHD groups.
Conclusions
In conclusion, our findings indicate that CSACS can not only be used to provoke GH secretion but also increase the height SDS for bone age in both NGH and GHD groups. The dynamic Ghrelin and GH secretion detection indicates some negative regulation or feedback mechanism lying between GH and Ghrelin. CSACS could be used as a height acceleration option, further investigations are needed to confirm the results and better decipher the relationship between Ghrelin and GH and the underlying mechanisms.
CSACS may be used to dynamically detect Ghrelin and GH and to accelerate the growth of children with dwarfism.
Abbreviations
- CSACS:
-
Combined simultaneous arginine clonidine stimulation
- GH:
-
Growth hormone
- GHD:
-
Growth hormone deficiency
- NGH:
-
Normal growth hormone
- SDS:
-
Standard deviation score
References
Vorontsova MV, Nagaeva EV, Naygovzina NB. Economic and social aspects of pituitary dwarfism treatment with recombinant growth hormone. Problemy E̊ndokrinologii. 2017;63:82–91.
Lin S, Li C, Li C, Zhang X. Growth hormone receptor mutations related to individual dwarfism. Int J Mol Sci. 2018;19:1433.
Frasier SD. Short stature in children. Pediatr Rev. 2008;3:171–9.
V G GB, C B NP, S DG AB, F G IT, M M EG. Acylated ghrelin as a provocative test for the diagnosis of GH deficiency in adults. Eur J Endocrinol. 2013;168:23–30.
Murray RD, Peacey SR, Rahim A, Toogood AA, Thorner MO, Shalet SM. The diagnosis of growth hormone deficiency (GHD) in successfully treated acromegalic patients. Clin Endocrinol. 2010;54:37–44.
Wu KH, Tsai FJ, Peng CT. Growth hormone (GH) deficiency in patients with beta-thalassemia major and the efficacy of recombinant GH treatment. Ann Hematol. 2003;82:637.
Strich D. Can the Clonidine Stimulation Test for Growth Hormone Deficiency be Shortened?
Al KR, Moisan L, Bui H. The shortened combined clonidine and arginine test for growth hormone deficiency is practical and specific: a diagnostic accuracy study. Journal of Pediatric Endocrinology & Metabolism Jpem. 2016;29:305–10.
Liang JT. Impact of body mass index on peak growth hormone response to combined stimulation test with arginine and clonidine. Journal of Applied Clinical Pediatrics. 2012;27:1582–4.
Bhat N, Dulmovits E, Lane A, Messina C, Wilson T. Combined simultaneous arginine clonidine stimulation test: timing of peak growth hormone (GH) concentration and correlation with clinical indices of GH status. Growth Hormone & Igf Research Official Journal of the Growth Hormone Research Society & the International Igf Research Society. 2018;40:28.
RJ K, CL O, SS G, LM G-S, KM F ZM, R W LRC, AF R, CL J. CDC growth charts for the United States: methods and development. Vital Health Stat. 2000;2002(246):1–190.
Kuczmarski R, Ogden C, Guo S, Kuczmarski R, Grummerstrawn L, Flegal K, Guo S, Mei R. Grummerstrawn L. In: CDC growth charts; 2000.
Satoh M. Bone age: assessment methods and clinical applications. Clin Pediatr Endocrinol. 2015;24:143–52.
Maghnie M, Pennati MC, Civardi E, Di IN, Aimaretti G, Foschini ML, Corneli G, Tinelli C, Ghigo E, Lorini R. GH response to ghrelin in subjects with congenital GH deficiency: evidence that ghrelin action requires hypothalamic-pituitary connections. Eur J Endocrinol. 2007;156:449–54.
Aguiar-Oliveira MH, Aho S, Crp O, Campos VC, Oliveira-Neto LA, Salvatori R. MECHANISMS IN ENDOCRINOLOGY: the multiple facets of GHRH/GH/IGF-I axis: lessons from lifetime, untreated, isolated GH deficiency due to a GHRH receptor gene mutation. Eur J Endocrinol. 2017;177:R85.
Stylianou C, Galli-Tsinopoulou A, Grammatikopoulou MG, Koliakos G, Varlamis G. Ghrelin and growth hormone serum levels during the clonidine test in children with short stature and variable growth hormone status. Hormones. 2011;10:39.
Nass RM, Gaylinn BD, Rogol AD, Thorner MO. Ghrelin and growth hormone: story in reverse. Proc Natl Acad Sci U S A. 2010;107:8501–2.
Khatib N, Gaidhane S, Gaidhane AM, Khatib M, Simkhada P, Gode D, Zahiruddin QS. Ghrelin: ghrelin as a regulatory peptide in growth hormone secretion. Journal of Clinical & Diagnostic Research Jcdr. 2014;8:13–7.
Choi WJ, Yang S, Im JH, Lee YI, Shin JH. The relationship between insulin-like growth factor binding Protein-3 promoter polymorphism and growth; 2006.
Obara-Moszyńska M, Kedzia A, Korman E, Niedziela M. Usefulness of growth hormone (GH) stimulation tests and IGF-I concentration measurement in GH deficiency diagnosis. J Pediatr Endocrinol Metab. 2008;21:569–79.
Boschetti M, Teti C, Albertelli M, Minuto F, Ferone D. Adult GH deficiency - the value of IGF-I estimation. Reviews in Endocrinology & Metabolism. 2013.
Firth SM, Baxter RC. Cellular actions of the insulin-like growth factor binding proteins. Endocr Rev. 2002;23:824–54.
Whatmore AJ, Hall CM, Jones J, Westwood M, Clayton PE. Ghrelin concentrations in healthy children and adolescents. Clin Endocrinol. 2010;59:649–54.
Jarkovská Z, Rosická M, Marek J, Hána V, Weiss V, Justová V, Lacinová Z, Haluzík M, Krsek M. Plasma levels of total and active ghrelin in acromegaly and growth hormone deficiency. Physiol Res. 2006;55:175.
Acknowledgements
Not applicable.
Funding
This study was supported by Zhenjiang Science and Technology Plan (Social Development) Project (SH2015036).
Availability of data and materials
All data generated or analyzed during this study are included in this published article.
Author information
Authors and Affiliations
Contributions
GZ, RD performed the experiments, analyzed and interpreted the data. RD wrote the manuscript. Both authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All participants have given informed and written consent. This study was approved by the ethics committee of Jiangdu People’s Hospital of Yangzhou, and followed the ethical guidelines laid down in the 1975 Declaration of Helsinki.
Consent for publication
All participants have given consent for publication.
Written informed consent was obtained from the participant for publication of their individual details in this manuscript. The consent form is held by the authors’ institution and is available for review by the Editor-in-Chief.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Zhou, G., Du, R. Dynamic Ghrelin and GH serum levels during combined simultaneous arginine clonidine stimulation test in children with dwarfism. Ital J Pediatr 45, 17 (2019). https://doi.org/10.1186/s13052-019-0610-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13052-019-0610-5