
Abstract
Congenital hearing loss is the most frequent birth defect. The American Academy of Pediatrics and the Joint Committee on Infant Hearing established quality of care process indicators for Universal Newborn Hearing Screening starting from 1999. In a previous systematic review of Universal Newborn Hearing Screening studies we highlighted substantial variability in program design and in reported performance data. In order to overcome these heterogeneous findings we think it is necessary to optimize the implementation of Universal Newborn Hearing Screening programs with an appropriate application of the planning, executing, and monitoring, verifications and reporting phases. For this reason we propose a conceptual framework that logically integrates these three phases and, consequently, a tool (a check-list) for their rationalization and standardization.
Our paper intends to stimulate debate on how to ameliorate the routine application of high quality Universal Newborn Hearing Screening programs. The conceptual framework is proposed to optimize, rationalise and standardise their implementation. The checklist is intended to allow an inter-program comparison by removing heterogeneity in processes description and assessment.
Similar content being viewed by others


Background
Sensorineural hearing loss is one of the most frequently occurring permanent congenital defects at birth with a prevalence of 0.1–0.3 % for newborns [1–4] (2–5 % in presence of audiological risk factors) [5]. Its late diagnosis could negative influence language, learning and speech development with lifelong consequences [6–11]. Universal Neonatal Hearing Screening (UNHS) programs were developed in several countries to identify the majority of newborns with hearing impairment. UNHS programs adopt, as screening tests, otoacoustic emissions (OAEs) and/or automated auditory brainstem response (aABR) testing. Those who are positive at tests are referred to full audiological diagnosis. Audiological or medical/surgical management, educational and (re)habilitation methods, and child and family support are available strategies for subjects with confirmed hearing loss [12]. Recognised benefits of UNHS are better language outcomes at school age and improved long-term language development [13, 14].
Since the 1999, process and outcome performance indicators and benchmarks were established for Early Hearing Detection and Intervention (EHDI) programs (i.e., identification before 3 months of age and intervention by 6 months of age) [15] to evaluate progress and determine consistency and stability [16, 17]. In 2007 the JCIH recommended timely and accurate monitoring of relevant quality measures, based on its reviewed performance indicators and benchmarks, as an essential practice for inter-program comparison and continuous quality improvement [17].
With the aim to verify whether literature reporting experiences on hospital-based UNHS programs include sufficient information to allow inter-program comparisons according to the already available indicators/benchmarks defined by the AAP and JCIH, we performed a systematic review [18]. We found that not all studies reported all the data necessary for calculating the complete proposed set of quality indicators, and that when comparing available data on indicators with corresponding benchmarks, the full achievement of all the recommended targets is an open challenge. We also found substantial heterogeneity in terms of extent of hearing loss (hearing threshold, uni- vs. bilateral hearing loss), criteria for identification of neonates at higher risk of hearing loss, screening tests used, personnel performing the tests, testing environment.
In order to overcome these heterogeneous findings we think it is necessary to optimize the implementation of Universal Newborn Hearing Screening programs with an appropriate application of the planning, executing, and monitoring, verifications and reporting phases. For this reason we propose a conceptual framework that logically integrates these three phases and, consequently, a tool (a check-list) for their rationalization and standardization.
Discussion - The conceptual framework for rationalized and standardized UNHS programs
The framework is structured on several phases (see also Fig. 1 and Fig. 2):

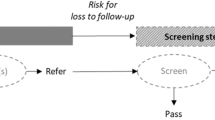
A framework for managing a UNHS program – general view. The framework is composed by three phases: a planning phase based on indications from guidelines and recommendations, specificities of the local context, benchmarks, reports from verification phase; an executing phase where the protocol is applied and where data are generated, managed and aggregated for monitoring; a monitoring, reporting and verifying phase where the indicators are compared with benchmarks and a report is generated. The Unified Modeling Language™ (UML®) notation is adopted for representation purposes: black filled circle represents the initial state and rounded circle the ending state; the rounded square indicates an action and the diamond a gateway where the process can take different roots upon a specified conditions; the arrowed line depicts the flow and the stylized sand-glass a time event (specifically adopted for a waiting time); the sharp-cornered square is used for objects/data/information

A framework for managing a UNHS program – detailed description. A detailed description of the conceptual framework is provided. In the central lane a description of the executing phase is reported recurring to the UML® notation: in addition to the specifications in Fig. 1, the folded square is used for noting. The key elements of the planning phase are reported on the top of the Figure and the proposed indicators on the bottom. In both cases their impact on the UNHS process is represented recurring to vertical lines ending on a specific point in the executing phase
-
1)
A planning phase based on indications from guidelines and recommendations, specificities of the local context, benchmarks, reports from verification phase. The Deliver the protocol Action is activated, apart from the first instance, if the benchmarks are not achieved, if guidelines/recommendations are updated, or if the context specificities change. The output of this phase is the protocol for UNHS execution.
-
2)
An executing phase where the protocol is applied and where data should be generated and managed for monitoring. The outputs of this phase are the raw data for process monitoring.
-
3)
A monitoring, reporting and verifying phase where the Monitor action is activated periodically or upon request to aggregate data and build performance indicators. The verification is made comparing indicators with benchmarks and a report is generated with an analysis of reasons for possible deviations which can push for a redefinition of the protocol and/or for a re-organization of its execution. Reports can be used also for disseminating purposes.
A more detailed description of the single phases follows in the following sections (note that the EXECUTING UNHS PROGRAM phase is out of the scope of our work and will not be discussed further).
Planning UNHS program
In order to deliver a protocol it necessary to define the target and the processes.
Definition of the target
Two elements are of importance: the definition of hearing loss and the identification of criteria used to define newborns at higher risk of hearing loss. Hearing threshold and uni- vs. bilateral have an impact in the number of neonates going through testing and evaluations, the number of infants admitted to therapy, the rate of newborns with hearing loss with early diagnosis and treatment, the number of neonates that could erroneously be evaluated as with no hearing deficits. These two parameters are fundamental for inter-program comparison. Several classifications of Hearing Loss have been formulated [19–21] which brings in the definition of the levels of severity (see Additional file 1). It is therefore necessary to make the choice explicit also for their impact on the typology of treatment/rehabilitation. We have previously observed that, in the lack of standardization, several thresholds have been applied in UNHS programs (26 to 40 dB HL).(6) Newborns with risk factors for neonatal hearing loss have about a 10 fold probability for hearing deficits with respect to the overall population [1, 2]. Criteria for higher audiological risk have been defined by several subjects (JCIH [17], the US National Institutes for Health - NIH [22], ASHA [23]) or are chosen directly by program coordinators (e.g., Clemens et al. [24]).
The audiological risk criteria are relevant for that: specific audiological risk may require a specific screening protocol; the timing and number of hearing re-evaluation (surveillance) for infants at risk should be customized and individualized depending on the relative likelihood of a subsequent delayed onset hearing loss.
Definition of the processes
Activities, detailed actions, decision nodes, workflows, roles, environmental conditions have to be identified and specified. More specifically key issues are reported. The typology and the number of tests, and the healthcare setting in which performing the examinations (before or after the discharge) – The program needs to be well balanced for sensitivity, specificity, coverage of the population and costs per subject identified. E.g., Kennedy et al. [25] reported to have changed their protocol using unilateral failure on aABR, rather than bilateral failure on Transient Evoked OAEs (TEOAEs) testing, as the second step; this change was associated with a reduction in the screen-failure rate from 2.4 % (95 % CI 2.2–2.6) to 1.3 % (1.1–1.5) of babies screened. The presence of specific protocol for neonates at higher risk (e.g., aABR for NICU staying in NICUs for more than 5 days instead of TEOAEs) [17] - Such neonates, in fact, are at risk of having neural hearing loss (auditory neuropathy/auditory dyssynchrony) which is not detectable with TEOAEs. The set of examinations for the full audiological evaluation – E.g., the one recommended by the JCIH [17]. The tasks to be performed to increase the percentage of enrolment and to reduce the lost to follow up (neonates referred to further examinations that do not show at the planned appointments) - With reference to the former, it has to be noted that specific actions should be done for an appropriate communication with families creating the conditions for an informed consent. With reference to the latter, a survey conducted in USA [26] shows that only 62 % of all newborns who need a diagnostic evaluation actually did it and, out of them, only 52 % by the age of 3 months (as recommended by the JCIH). The lost to follow-up at all stages of the EHDI process continues to be a serious concern also for the World Health Organization (WHO) [27] that states the importance, for its success, of monitoring and implementing all the phases of the screening (responsibilities, training, information campaign, procedures of quality assurance). The surveillance program for early identification of infants and children with late onset (especially in presence of high risk factors) – It is recommended to perform regular surveillance of developmental milestones, auditory skills, parental concerns, and middle-ear status to for all infants, together with an objective standardized screening of global development, at 9, 18, and 24 to 30 months of age or at any time if the health care professional or family has concern [17]. The cooperation among all the involved operators, services and institutions - The identification of the key roles is an essential step for an appropriate management of the entire process and for monitoring purposes.
Monitoring, verifying and reporting
Monitoring
In our systematic review [18] the AAP [16] and JCIH [17] performance indicators focused on early diagnosis of neonates with hearing loss have been presented in detail and grouped in three areas:
-
1)
Universality– completeness of universality in both recruitment and follow-up phases;
-
2)
Timely detection– specification of follow-up deadlines for identification and intervention, and determination of the observed prevalence;
-
3)
Overreferral – Efficient use of highly specialized care.
Verification of program performance
For each reported indicator a reference benchmark has been identified [18] which represent a consensus of expert opinion in the field of newborn hearing screening and intervention, and are the minimal requirements that should be attained by high quality EHDI programs. Frequent measures of quality permit prompt recognition and correction of any unstable component of the EHDI process. The JCIH recommends timely and accurate monitoring of relevant quality measures for inter-program comparison and continuous quality improvement [17].
Reporting of process indicators
This is the output of the Monitor, Verify and Report Activity and it is used to make process results explicit and, as previously reported, as the basis for possible re-planning and/or reorganization.
The proposed framework has been used as a conceptual guidance for building a checklist (Additional file 2) intended to support UNHS program coordinators in the planning, monitoring, reporting and verification.
Conclusions
As reported in the 2007 JCIH Position Statement [17], regular measurement of performance and routine monitoring of indicators are recommended for inter-programme comparison and continuous quality improvement. With the aim of achieving high quality UNHS programs by achieving AAP and JCIH quality benchmarks, our work proposes a conceptual framework and a checklist. The former is a way to optimize, rationalise and standardise the implementation of UNHS programs by considering all the relevant phases: Planning, executing, and monitoring, verifying and reporting. The latter allows an inter-program comparison by removing heterogeneity in processes description and assessment.
The paper is a contribution toward a standardisation in reporting UNHS experiences which may favour the emerging of best practises.
Abbreviations
- aABR:
-
Automatic auditory brainstem response
- AAP:
-
American Academy of Pediatrics
- EHDI:
-
Early hearing detection and intervention
- JCIH:
-
Joint Committee on infant hearing
- NICU:
-
Neonatal intensive care unit
- OAEs:
-
Evoked otoacoustic emissions
- TEOAEs:
-
Transiently evoked OAEs
- UNHS:
-
Universal Newborn Hearing Screening
References
BarskyFirkser L, Sun S. Universal Newborn Hearing Screenings: a three-year experience. Pediatrics. 1997;99(6):e4. doi:10.1542/peds.99.6.e4.
Mehl AL, Thomson V. The colorado newborn hearing screening project, 1992–1999: on the threshold of effective population- based universal newborn hearing screening. Pediatrics. 2002;109(1):8. doi:10.1542/peds.109.1.e7.
Vartiainen E, Kemppinen P, Karjalainen S. Prevalence and etiology of bilateral sensorineural hearing impairment in a finnish childhood population. Int J Pediatr Otorhinolaryngol. 1997;41(2):175–85.
US Center for Diseases Control and Prevention. Summary of 2009 National CDC EHDI Data2009
Norton SJ, Gorga MP, Widen JE, Folsom RC, Sininger Y, Cone-Wesson B, et al. Identification of neonatal hearing impairment: a multicenter investigation. Ear Hear. 2000;21(5):348–56. doi:10.1097/00003446-200010000-00003.
Rach GH, Zielhuis GA, van den Broek P. The influence of chronic persistent otitis media with effusion on language development of 2- to 4-year-olds. Int J Pediatr Otorhinolaryngol. 1988;15(3):253–61.
Moeller MP OM, Eccarius M. Receptive language skills. In: MJ O, editor. Language and learning skills of hearing-impaired children: ASHA Monograph 23. Rockville, MD: ASHA; 1986.
Allen TE. Patterns of academic achievement among hearing impaired students: 1974 and. Deaf children in America. 1983;1986:161–206.
Davis A, Hind S. The impact of hearing impairment: a global health problem. Int J Pediatr Otorhinolaryngol. 1999;49 Suppl 1:S51–4.
van Eldik TT. Behavior problems with deaf Dutch boys. Am Ann Deaf. 1994;139(4):394–9.
Vostanis P, Hayes M, Du Feu M, Warren J. Detection of behavioural and emotional problems in deaf children and adolescents: comparison of two rating scales. Child Care Health Dev. 1997;23(3):233–46.
Patel H, Feldman M. Universal newborn hearing screening. Paediatr Child Health. 2011;16(5):301–10.
Nelson HD, Bougatsos C, Nygren P. Universal newborn hearing screening: systematic review to update the 2001 US preventive services task force recommendation. Pediatrics. 2008;122(1):e266–76. doi:10.1542/peds.2007-1422.
Wolff R, Hommerich J, Riemsma R, Antes G, Lange S, Kleijnen J. Hearing screening in newborns: systematic review of accuracy, effectiveness, and effects of interventions after screening. Arch Dis Child. 2010;95(2):130–5. doi:10.1136/adc.2008.151092.
NIH. Consensus development conference statement - early identification of hearing impairment in infants and young-children - 1–3 March 1993. Int J Pediatr Otorhinolaryngol. 1993;27(3):215–27.
American Academy of Pediatrics Task Force on Newborn and Infant Hearing. Newborn and infant hearing loss: Detection and intervention. Pediatrics. 1999;103(2):527–30.
Busa J, Harrison J, Chappell J, Yoshinaga-Itano C, Grimes A, Brookhouser PE, et al. Year 2007 position statement: Principles and guidelines for early hearing detection and intervention programs. Pediatrics. 2007;120(4):898–921. doi:10.1542/peds.2007-2333.
Mincarone P, Leo CG, Sabina S, Costantini D, Cozzolino F, Wong JB, et al. Evaluating reporting and process quality of publications on UNHS: a systematic review of programmes. BMC Pediatr. 2015;15(1):86. doi:10.1186/s12887-015-0404-x.
Bureau International d’Audiophonologie. BIAP Recommendation 02/1 bis. 1996. http://www.biap.org/index.php?option=com_content&view=article&id=5%3Arecommandation-biap-021-bis&catid=65%3Act-2-classification-des-surdites&Itemid=19&lang=en. Accessed 11/07/2014.
World Health Organization. Primary Ear And Hearing Care Training Resource. Advanced Level., Geneva. 2006. http://www.who.int/pbd/deafness/activities/hearing_care/advanced.pdf. Accessed 11/07/2014.
Clark JG. Uses and abuses of hearing loss classification. Asha. 1981;23(7):493–500.
National Institutes of Health. Summary of the National Institutes of Health consensus: early identification of hearing impairment in infants and young children. Am J Otol. 1994;15(2):130–1.
American Speech-Language-Hearing Association. Guidelines for the identification of hearing impairment in at risk infants age birth to 6 months. Asha. 1988;30(4):61–4.
Clemens CJ, Davis SA, Bailey AR. The false-positive in universal newborn hearing screening. Pediatrics. 2000;106(1):5. doi:10.1542/peds.106.1.e7.
Kennedy C, Kimm L, Thornton R, Davis A. False positives in universal neonatal screening for permanent childhood hearing impairment. Lancet. 2000;356(9245):1903–4. doi:10.1016/s0140-6736(00)03267-0.
Shulman S, Besculides M, Saltzman A, Ireys H, White KR, Forsman I. Evaluation of the Universal Newborn Hearing Screening and Intervention Program. Pediatrics. 2010;126:S19–27. doi:10.1542/peds.2010-0354F.
World Health Organization. Newborn and infant hearing screening - Current issues and guiding principles for action: outcome of a who informal consultation held at WHO headquarters, Geneva, Switzerland. WHO. November 2009. http://www.who.int/blindness/publications/Newborn_and_Infant_Hearing_Screening_Report.pdf.
Acknowledgements
Our work has been complemented by the contribution of Roberto Guarino (National Research Council, Institute of Clinical Physiology) who collaborated in representing the framework of the screening processes.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interest
The authors declare that they have no competing interests.
Authors’ contributions
All the authors participated in the systematic review upon which the present manuscript is based (see reference [18]). CGL and PM equally contributed to the work. They designed the work (the conceptual framework and the checklist), drafted the manuscript (with the contribution of SS for UML description and representation), approved the final version of the manuscript. SS, GL and JBW contributed to the conception of the work, critically revised the manuscript for important intellectual content and gave their final approval to the version to be published. All the authors agree to be accountable for all the aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Additional files
Additional file 1:
The need of an explanation: what is the target Hearing Loss for UNHS?. (PDF 82 kb)
Additional file 2:
Check list for the quality of Universal Newborn Hearing Screening programs. (DOC 94 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Leo, C.G., Mincarone, P., Sabina, S. et al. A conceptual framework for rationalized and standardized Universal Newborn Hearing Screening (UNHS) programs. Ital J Pediatr 42, 15 (2016). https://doi.org/10.1186/s13052-016-0223-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13052-016-0223-1