
Abstract
Background
Growth hormone (GH) has a strong positive influence on bone, stimulating both bone elongation and increase in size. The aim of the study was to compare the effect of two different GH dosages on final height and bone geometry in two groups of GH-deficient children.
Methods
We evaluated 121 children (86 m, 35f). Group 1 (77 patients) treated with GH at a mean dose of 0.16 mg/kg/week and group 2 (44 patients) at 0.3 mg/kg/week. Bone geometry was evaluated at final height from a digitalized X-ray of the left hand considering the following parameters: metacarpal index (MI), cross-sectional area (CSA), cortical area (CA) and medullary area (MA).
Results
At baseline, group 2 was shorter than group 1 (−1.54 vs −1.01 SDS; p < 0.005), while at final height there was no difference. Height gain was significantly greater in group 2 than in group 1 (1.62 vs 1.13 SDS; p < 0.001). Bone geometry: MI was significantly greater in group 2 (0.62 vs 0.55; p < 0.001) as well as CA (46.87 vs 42.69 cm2; p < 0.005), while MA was significantly lower in group 2 (8.48 vs 11.65 cm2; p < 0.002).
Conclusion
Higher GH doses elicit a significantly greater statural gain and a greater bone cortical area.
Similar content being viewed by others

Background
Growth hormone (GH) exerts a strong positive influence on bone by stimulating both bone elongation and increase in size. It enhances the accrual of trabecular [1] and cortical bone [2] up to the attainment of peak bone mass in young adults [3]. GH stimulates longitudinal bone growth and therefore statural growth, acting mainly on the resting zone chondrocytes and inducing local IGF-I production, which stimulates the clonal expansion of proliferating chondrocytes in an autocrine/paracrine manner [4]. In addition, GH increases bone size by IGF-I mediated subperiosteal bone growth [5–9]. We already showed in a previous paper [10] that higher GH doses result in a greater height gain with a trend toward larger bones at final height, leading eventually to improved bone strength. In this study, we wanted to confirm our previous findings by examining a larger group of patients, similarly treated with two different GH dosages.
Methods
This is a confirmatory study on the effect of two different doses of GH on final height and bone geometry in a large group of GH deficient children. The study was performed in a University clinic and in a Regional Hospital. Final height was measured in both centres by a wall-mounted stadiometer and bone geometry was evaluated on the X-ray obtained for evaluation of bone age. The study protocol followed the ethical principles outlined by the Helsinki Declaration. Adequate information about the protocol supported the decision-making by the parents.
Subjects
A total of 121 children (86 M and 35 F) affected by isolated idiopathic GH-deficiency (GHD), who reached their final height, were selected for the study. The diagnosis of GHD was based on auxological criteria and a GH peak < 10 μg/l after at least 2 consecutive conventional pharmacological tests. All children had a normal pituitary on MRI, and were not affected by any cardiovascular, respiratory, renal, rheumatic diseases or by any other endocrine disorders. Seventy seven children (57 M, 20 F) age 9.9 ± 3.6 were treated in Pavia with a weekly rGH dosage of 0.16 mg/Kg for a mean period of 6.07 ± 3.2 years (group 1) while forty four children (29 M, 15 F), age 10.3 ± 3.1 were treated in Bolzano with a weekly rGH dosage of 0.3 mg/Kg for a mean period of 5.8 ± 2.7 years (group 2).
The male/female ratio in the two groups was not different (0.66 vs 0.74; NS). They were all regularly followed-up until final height (bone age >15 years in girls and >17 years in boys according to the method of Greulich and Pyle [11]. Height and BMI were converted to standard deviation score (SDS) according to the Italian Standards [12]. However, in order to also take the patient’s genetic potential for growth into account, height was expressed as parentally adjusted height-SDS, i.e. the difference between height-SDS for chronological age and target height–SDS (average height of both parents plus 6.55 cm for boys and minus 6.55 cm for girls). The difference between the parentally adjusted height-SDS on attainment of adult stature and the one before starting treatment was defined as relative height gain. The auxological features of the patients are reported in Table 1 (raw data) and Table 2 (parentally adjusted).
Bone geometry
We used the digitalised X-rays (Dicom files) taken for the assessment of bone age, for the evaluation of bone geometry. The following parameters were evaluated at the level of the 2nd metacarpal bone at its narrowest site, as previously described: outer (D) and inner (d) diameter, metacarpal index (MI = D-d/D: mm), which is a relative measure of the thickness of the 2nd metacarpal cortical bone, total cross sectional area (TCSA: mm2), cortical area (CA: mm2) and medullary endocortical area (MA: mm2). TCSA, CA and MA are not directly measured with this technique, but calculated assuming that the bone is cylindrical. Bone strength was calculated at the metacarpus: it is dependent upon the material property of the metacarpal bones (which cannot be directly measured in vivo) and the cross-sectional moment of inertia which is a function of the fourth power of the cortical ring. By assuming a constant material property, a Bending Breaking Resistance Index (BBRI-1) can be calculated as follows: outer diameter (D) to the fourth power minus inner diameter (d) to the fourth power divided by D [D4-d4/D]. Furthermore, considering that due to anatomical irregularities, the outer and the inner circumferences are not exactly homogenenous, we tried to overcome this problem by calculating the bone strength using the corresponding areas instead of the diameters (BBRI-2), according to the formula: (CSA2-MA2)/√CSA).
Statistical analysis
The data were normally distributed and are reported as mean ± SD. Student’s paired and unpaired t-test were used to verify differences within and between groups, after adjusting for height and sex. Simple correlations were used to investigate the association between the different parameters. A P value of less than 0.05 indicated statistical significance. The SAS Enterprise Guide 4.3statistical software (SAS Institute Inc. Cary, NC, 27513, USA) was used for these analyses.
Results
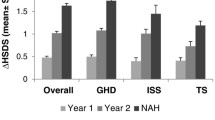
Auxology: parentally-adjusted height-SDS was significantly higher in group 1 at the beginning of treatment than in group 2 (−1.01 ± 0.83 vs −1.54 ± 1.14; p < 0.005), while no difference between the 2 groups (0.11 ± 0.94 vs 0.15 ± 1.0;NS) was observed at the end of treatment. Group 1 (−1.01 ± 0.83 vs 0.11 ± 0.94; p < 0.01) and group 2 (−1.54 ± 1.14 vs 0.15 ± 1.0; p < 0.001) significantly improved their parentally-adjusted height-SDS, but height gain was significantly higher in group 2 than in group 1 (1.13 ± 0.70 vs 1.62 ± 0.69; p < 0.001) (see Table 2).
Bone geometry: at final height, group 2 showed a greater MI (0.55 ± 0.07 vs 0.62 ± 0.07; p < 0.001), a greater CA (42.69 ± 8.39 vs 46.87 ± 9.39 mm2; p < 0.005) but a significantly lower MA (11.65 ± 4.65 vs 8.48 ± 3.87 mm2; p < 0.002). There was no difference in total cross sectional area (see Table 3 and Fig. 1). BBRI-1 (556.11 ± 167.69 vs 584.66 ± 177.30 mm3; NS), BBRI-2 (389.78 ± 116.57 vs 406.64 ± 123.32 mm3; NS).

Bone geometry in the two groups
Correlations
CA was positively correlated with final height (r 0.40, p < 0.001), height gain (r 0.22, p < 0.05), final BMI, CSA (r 0.92, p < 0.0001) and BBRI. MI was positively correlated with BMI at baseline (r 0.38, p < 0.0005) and at final height (r 0.39, p < 0.0005) and negatively with MA (r −0.82, p < 0.001) and CSA (r −0.24, p < 0.05). MA was negatively correlated with BMI at baseline (r −0.29, p < 0.01) and at final height (r −0.28, p < 0.01) and positively with final height (r 0.31, p < 0.005) and BBRI (r 0.57, p < 0.001).
Discussion
The major outcome of this study is the confirmation that higher doses of GH elicit a significantly greater statural gain and improvement of the bone geometry. The greater height gain achieved by the children receiving the higher GH dosage is in agreement with previous reports [10, 13–15], emphasizing the advantage of using higher GH doses. Although 0.3 mg/Kg/week is a slightly higher dose than that usually employed in isolated GHD, it is in agreement with the recommendations of the GH Research society [16].
Statural growth is mainly the result of bone elongation under the influence of GH which, moreover, also stimulates the width growth of the bones leading to an increased size. In this study we were able to confirm the positive influence of GH on bone, since the group of children treated more intensively accrued more cortical bone compared to the other group. This finding is also supported by the positive correlations found between cortical area and final height, height gain, cross sectional area and BMI, which are all GH-dependent parameters.
In agreement with our findings, a previous study on adults with growth hormone (GH) deficiency, also showed the strong positive effect of GH treatment on cortical bone, which was exerted by stimulating both periosteal and endosteal bone apposition.
Furthermore, we found a smaller medullary area in group 2 at final height (p < 0.002), suggesting that higher dose of GH could induce a clearer effect on the endosteal side (the smaller the area, the clearer the effect) than on the periosteal side of the bone.
MI and CA were therefore significantly higher in group 2 (higher dose GH), strengthening the advantage of using the higher GH dose. However, these geometrical advantages, possibly due to the low number of subjects, were not sufficient to produce a significant improvement in BBRI, although a trend was observed.
One cannot exclude the possibility that another possible explanation for all these geometrical remarks might be that the children in group 2 were significantly shorter at baseline and so, presumably, they also had smaller bones. In this case, the CSA might prove to be increased more efficiently under higher GH dose. Unfortunately, we were not able to calculate the relative gain in the different parameters of bone geometry in the two groups since in many patients the X-rays taken at the beginning of the treatment with GH were not available. Another possible explanation might have been an overrepresentation of females in group 2, since females are known to have a greater endocortical acquisition during puberty. The male/female ratio in the two groups was however not different and differences in sex and height have been taken into account in statistical analysis.
In our study we did not measure for technical reasons bone mineral density at the lumbar spine, which is an important marker of peak bone mass, however, bone geometry measured at metacarpal level is strongly related with bone status in other sites [17–19].
One limit of this paper is the fact that the diagnosis of GHD was based on a level of GH after pharmacological stimulation of less than 10 μg/l while now, in Italy, a value of 8 μg/l is considered as more appropriate. This might have allowed the inclusion of some short normal children, according to the new criteria.
Conclusion
We confirm the beneficial effects of larger doses of growth hormone on both height gain and bone accretion.
The study protocol followed the ethical principles outlined by the Helsinki Declaration. Adequate information about the protocol supported the decision-making by the parents.
References
Brixen K, Hansen TB, Hauge E, Vahl N, Jorgensen JO, Christiansen JS, et al. Growth hormone treatment in adults with adult-onset growth hormone deficiency increases iliac crest trabecular bone turnover: a 1-year, double-blind, randomized, placebo-controlled study. J Bone Miner Res. 2000;15(2):293–300. doi:10.1359/jbmr.2000.15.2.293.
Ueland T, Bollerslev J, Flyvbjerg A, Hansen TB, Vahl N, Mosekilde L. Effects of 12 months of GH treatment on cortical and trabecular bone content of IGFs and OPG in adults with acquired GH deficiency: a double-blind, randomized, placebo-controlled study. J Clin Endocrinol Metab. 2002;87(6):2760–3. doi:10.1210/jcem.87.6.8549.
Baroncelli GI, Bertelloni S, Sodini F, Saggese G. Longitudinal changes of lumbar bone mineral density (BMD) in patients with GH deficiency after discontinuation of treatment at final height; timing and peak values for lumbar BMD. Clin Endocrinol (Oxf). 2004;60(2):175–84.
Isaksson OG, Lindahl A, Nilsson A, Isgaard J. Mechanism of the stimulatory effect of growth hormone on longitudinal bone growth. Endocr Rev. 1987;8(4):426–38. doi:10.1210/edrv-8-4-426.
Ohlsson C, Bengtsson BA, Isaksson OG, Andreassen TT, Slootweg MC. Growth hormone and bone. Endocr Rev. 1998;19(1):55–79. doi:10.1210/edrv.19.1.0324.
Walenkamp MJ, Wit JM. Genetic disorders in the GH IGF-I axis in mouse and man. Eur J Endocrinol. 2007;157 Suppl 1:S15–26. doi:10.1530/EJE-07-0148.
Yakar S, Courtland HW, Clemmons D. IGF-1 and bone: New discoveries from mouse models. J Bone Miner Res. 2010;25(12):2543–52. doi:10.1002/jbmr.234.
Mohan S, Baylink DJ. Role of growth hormone/insulin-like growth factor axis. In: Glowacki J, Rosen CJ, Bilezikian JP, editors. The aging skeleton. San Diego: Academic; 1999. p. 209–19.
Olson LE, Ohlsson C, Mohan S. The role of GH/IGF-I-mediated mechanisms in sex differences in cortical bone size in mice. Calcif Tissue Int. 2011;88(1):1–8. doi:10.1007/s00223-010-9436-2.
Radetti G, D’Addato G, Gatti D, Bozzola M, Adami S. Influence of two different GH dosage regimens on final height, bone geometry and bone strength in GH-deficient children. Eur J Endocrinol. 2006;154(3):479–82. doi:10.1530/eje.1.02113.
Greulich WW, Pyle SI. Radiographic Atlas of Skeletal Development of the hand and wrist. 1959.
Cacciari E, Milani S, Balsamo A, Spada E, Bona G, Cavallo L, et al. Italian cross-sectional growth charts for height, weight and BMI (2 to 20 yr). J Endocrinol Invest. 2006;29(7):581–93. doi:10.1007/BF03344156.
Radetti G, Buzi F, Paganini C, Pilotta A, Felappi B. Treatment of GH-deficient children with two different GH doses: effect on final height and cost-benefit implications. Eur J Endocrinol. 2003;148(5):515–8.
Wit JM, Rekers-Mombarg LT, Cutler GB, Crowe B, Beck TJ, Roberts K, et al. Growth hormone (GH) treatment to final height in children with idiopathic short stature: evidence for a dose effect. J Pediatr. 2005;146(1):45–53. doi:10.1016/j.jpeds.2004.08.055.
Coelho R, Brook CG, Preece MA, Stanhope RG, Dattani MT, Hindmarsh PC. A randomised study of two doses of biosynthetic human growth hormone on final height of pubertal children with growth hormone deficiency. Horm Res. 2008;70(2):85–8. doi:10.1159/000139149.
Growth Hormone Research S. Consensus guidelines for the diagnosis and treatment of growth hormone (GH) deficiency in childhood and adolescence: summary statement of the GH Research Society. GH Research Society. J Clin Endocrinol Metab. 2000;85(11):3990–3. doi:10.1210/jcem.85.11.6984.
Wilczek ML, Kalvesten J, Algulin J, Beiki O, Brismar TB. Digital X-ray radiogrammetry of hand or wrist radiographs can predict hip fracture risk--a study in 5,420 women and 2,837 men. Eur Radiol. 2013;23(5):1383–91. doi:10.1007/s00330-012-2706-9.
Forsblad-d’Elia H, Carlsten H. Bone mineral density by digital X-ray radiogrammetry is strongly decreased and associated with joint destruction in long-standing rheumatoid arthritis: a cross-sectional study. BMC Musculoskelet Disord. 2011;12:242. doi:10.1186/1471-2474-12-242.
Adami S, Zamberlan N, Gatti D, Zanfisi C, Braga V, Broggini M, et al. Computed radiographic absorptiometry and morphometry in the assessment of postmenopausal bone loss. Osteoporos Int. 1996;6(1):8–13.
Financial support
There is no financial support for this study.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
FL have been involved in drafting the manuscript have made substantial contributions to acquisition of data, analysis and interpretation of data. MB have made substantial contributions to conception and design and acquisition of data and revising the manuscript critically for important intellectual content. SL have made substantial contributions to acquisition of data and interpretation of data. GF have been involved in drafting the manuscript and revising it critically for important intellectual content. GR conceived of the study, participated in its design and coordination and helped to draft the manuscript, he revised it critically and have given final approval of the version to be published.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Lupi, F., Bozzola, M., Longhi, S. et al. The effect of two different GH dosages on final height and bone geometry. Ital J Pediatr 42, 5 (2016). https://doi.org/10.1186/s13052-016-0212-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13052-016-0212-4