
Abstract
Background
Helicopter Emergency Medical Services (HEMS) respond to serious trauma and medical emergencies. Geographical disparity and the regionalisation of trauma systems can complicate accurate HEMS dispatch. We sought to evaluate HEMS dispatch sensitivity in older trauma patients by analysing critical care interventions and conveyance in a well-established trauma system.
Methods
All trauma patients aged ≥65 years that were attended by the Air Ambulance Kent Surrey Sussex over a 6-year period from 1 July 2013 to 30 June 2019 were included. Patient characteristics, critical care interventions and hospital disposition were stratified by dispatch type (immediate, interrogate and crew request).
Results
1321 trauma patients aged ≥65 were included. Median age was 75 years [IQR 69–89]. HEMS dispatch was by immediate (32.0%), interrogation (43.5%) and at the request of ambulance clinicians (24.5%). Older age was associated with a longer dispatch interval and was significantly longer in the crew request category (37 min [34–39]) compared to immediate dispatch (6 min [5–6] (p = .001). Dispatch by crew request was common in patients with falls < 2 m, whereas pedestrian road traffic collisions and falls > 2 m more often resulted in immediate dispatch (p = .001). Immediate dispatch to isolated head injured patients often resulted in pre-hospital emergency anaesthesia (PHEA) (39%). However, over a third of head injured patients attended after dispatch by crew request received PHEA (36%) and a large proportion were triaged to major trauma centres (69%).
Conclusions
Many patients who do not fulfil the criteria for immediate HEMS dispatch need advanced clinical interventions and subsequent tertiary level care at a major trauma centre. Further studies should evaluate if HEMS activation criteria, nuanced by age-dependant triggers for mechanism and physiological parameters, optimise dispatch sensitivity and HEMS utilisation.
Similar content being viewed by others


Introduction
Advances in healthcare have enabled greater independence and activity in older people [1, 2]. This has led to a greater prevalence of older trauma, with 50% of severely injured patients over the age of 65-years recorded on the Trauma Audit and Research Network (TARN) [2, 3]. Inevitably, growing demand is being placed on acute healthcare services. The outcome of older trauma patients is difficult to predict; however, published studies indicate an increased risk of morbidity and mortality, with a mortality rate of 50% in adults aged over 75 years [4].
Helicopter Emergency Medical Services (HEMS) provide enhanced pre-hospital medical care to major trauma victims. HEMS can deliver specialist interventions such as pre-hospital hospital emergency anaesthesia (PHEA). Accurate tasking of HEMS is important to deliver this valuable resource. Accurate HEMS dispatch is critical to the appropriate activation of an enhanced care team to those patients whom may benefit most from advanced critical care interventions [5,6,7]. Various dispatch algorithms enhance sensitivity by coupling mechanism with anatomical and physiological criteria [7]. These have been shown to decrease HEMS activations to 55% of trauma patients, whilst at the same time accurately directing the enhanced care team to higher acuity patients [8].
Emergency medical dispatchers track an established pathway during a 112/999 call to discern traumatic injuries, of which the dispatch triggers are largely validated in the adult trauma population [9] and not specifically adapted to the older trauma subgroup. Clinical observations of traumatically injured older adults may present within parameters equivalent to younger ‘well’ adults [3]. Therefore, injury severity is potentially masked to both the caller and clinician, and subsequently HEMS dispatch is delayed [10].
In the present study, we sought to explore HEMS dispatch accuracy in older trauma patients by analysing HEMS specific interventions and disposition of this subgroup of trauma patients, stratified by dispatch type.
Methods
Study design and setting
We performed a retrospective cohort study of HEMS dispatch to older trauma in the south-east of England between 1 July 2013 to 30 June 2019.
Air Ambulance Kent Surrey Sussex (AAKSS) serves a population of approximately 4.3 million, with a transient population of up-to 11 million. AAKSS attends approximately 1600 patients each year. Two doctor-paramedic teams deploy by helicopter or response car, one of which operates a 24-h day and the other an 18-h day. The HEMS team brings advanced clinical procedures to complement the scope of practice provided by a land based Critical Care Paramedic (CCP), to include: pre-hospital emergency anaesthesia (PHEA), advanced analgesia and sedation, blood product transfusion and surgical intervention (thoracostomy and thoracotomy). The service works alongside the regional ambulance service of South East Coast Ambulance Service (SECAmb).
A CCP and HEMS dispatcher evaluate and task the critical care resources across the region from the Emergency Operations Centre (EOC). The tasking algorithm was devised internally and is previously published [11]. Activations are categorised as: immediate, interrogated or crew request. Immediate dispatch is triggered by pre-determined criteria. Interrogated dispatch is triggered where subsequent clinical information is reviewed, and HEMS dispatch agreed. Both immediate and interrogate dispatches are based on mechanism of injury (MOI), clinical condition of the patient and geographical location. A crew request can be activated by crews on scene (figure 3, suppl. file).
Study population
All older trauma patients (≥65 years) attended by HEMS with suspected traumatic injuries during the study period were included. Exclusion criteria comprised: patients < 65 years and patients presenting with suspected medical aetiology. Inter-facility transfers were excluded due to the unknown interventions delivered prior to HEMS arrival, and mutual aid requests excluded due to a variable, and unaccounted passage of time prior to AAKSS receiving the tasking.
Data collection
An electronic record system (HEMSbase Medic One Systems, Ltd. UK) is used at AAKSS. The following data were retrieved from the electronic patient record: patient identification number, timings (112/999-time, dispatch interval). Patient characteristics (age, gender), mechanism of injury (assault [blunt/penetrating], fall (< 2 m [m], > 2 m), intentional self-harm, road traffic collisions and other (for example, crush injury)), anatomical site of injury (head, neck, thorax, abdomen, upper leg, upper arm), GCS, advanced pre-hospital interventions provided by the HEMS team, drugs administered, patient disposition (pronounced life extinct on scene, or transport to local hospital, Trauma Unit or MTC), and conveyance (carry, ground escort, or ground assist) by transport modality were retrieved.
Advanced pre-hospital interventions comprise those not performed by ground ambulance teams where a CCP is not present: pre-hospital emergency anaesthetic (PHEA), open finger thoracostomy, resuscitative thoracotomy, ultrasound sonography (USS), administration of prothrombin complex concentrate (PCC, beriplex®), insertion of intercostal chest drain (ICD), administration of intravenous (IV) antibiotics and/or antiviral drugs, administration of hypertonic saline 5%, advanced analgesia (fentanyl and ketamine), and pre-hospital transfusion therapy. Transfusion therapy consisted of packed red blood cells (PRBC) and freeze-dried plasma (FDP). PRBCs were available throughout the study period and FDP (Lyoplas) available from 3 April 2015.
Data extraction and eligibility of patients was performed by one of the authors (JG) and any inaccuracies and discrepancies were resolved by a second author (JB). These included miscategorisation of calls with regard to mechanism, and coding of variables.
Ethical considerations
This project met National Institute for Healthcare Research (NIHR, UK) criteria for service evaluation and formal ethical approval was therefore not required. The project was approved by the Research & Development Committee at AAKSS.
Statistical analysis
Descriptive statistics are given as mean [95% CI] or median [IQR]. Patients were stratified into three groups according to age: 65–74, 75–84, 85 and over. Comparisons across groups were made using Chi-square or Kruskal-Wallis tests where appropriate. Where statistical significance was found (set at a p-value < 0.05) Dunn’s post-hoc testing with Bonferroni correction was performed. The study applied Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Guidelines [12], with missing values reported. All statistical analyses were conducted using SPSS 26.0 (IBM).
Results
A total of 6989 patients were attended by AAKSS during the study period (Fig. 1). Of these, 1422 were traumatically injured and aged ≥65. Seventy were excluded because “no injury” was recorded and the injury was of presumed medical aetiology. Seventeen cases were removed due to missing injury data, 13 as they were “mutual aid” requests and 1 as it was an inter-facility transfer. The resulting study population included 1321 patients ≥65 years, with 423 (32.0%) immediate dispatches; 575 (43.5%) interrogated dispatches; and 323 (24.5%) crew requests. During the study period (for all patients), the distribution by dispatch type was; immediate dispatch formed the greatest proportion (40%), followed by interrogate (24%) and crew requests (30%).

Flow chart of study population
Study population characteristics
Males represented 62% (n = 832) of the study population with a median age of 75 years (IQR 69–81). When stratified by age-group, 65–74 year olds represented 49% (n = 675) of the patients attended, 75–84 year olds represented 35% of patients (n = 468), and 14.8% (n = 196) were over 85 years As expected, the dispatch interval from 112/999 call to arrival of the HEMS team on scene was longer for crew requests (37 min [34–39]) compared to immediate (6 min [5–6]) or interrogated dispatch (15 min [13–16], p < .001) (Table 1). This was representative of dispatch for the whole cohort of patients attended by AAKSS during the study period for immediate dispatch (7 min [6–9]), interrogated dispatch (9 min [6–12]) and crew request (36 min [30–41]).
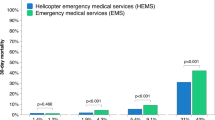
Figure 2 shows that the median age for all three dispatch types was 75 (IQR 69–81). Median patient age increased as dispatch priority decreased (Table 1).

The distribution of the older trauma cohort when age is plotted against dispatch criteria
Mechanism, anatomical injury site and transport modality in relation to dispatch type
When HEMS were dispatched, falls from height (> 2 m) and RTCs were the most frequent mechanism encountered. Overall, frequency distribution of mechanisms for the three dispatch groups were significantly different (p = .001). Direct dispatches were significantly more prevalent in falls > 2 m (p = .006) and when pedestrians were involved in road traffic collisions (RTCs) (p < .001), whereas drivers involved in an RTC were more likely to trigger an interrogated dispatch (p = .001). Falls < 2 m were likely to trigger a dispatch on crew request (p = .001) (Table 1).
Overall, head injuries were the most frequently reported injury (n = 897, 67%) followed by injuries to the thorax (n = 544, 41%, Table 1). Overall there was no significant difference in the frequency distribution of anatomical injury sites (p = .162), however, between dispatch groups, a significant difference in head injuries was observed (p = .001). Post hoc analysis indicated that immediate and crew requests were significantly more prevalent than interrogate (p = .012 and p = .004, respectively). There was no significant difference in the frequency distribution of poly and isolated trauma (p = .358). The majority of patients were transported to hospital (n = 1204, 91%) of which 60% conveyed directly to an MTC (n = 793). The proportion of patients transported to an MTC (69%) was higher after a crew request dispatch than after an immediate or interrogate dispatch (p = .001).
Advanced interventions
Table 2 displays the advanced interventions performed during the study period. PHEA was performed in a greater proportion (n = 86, 26%) of patients attended by crew request compared to immediate dispatch (p = .001) and interrogate dispatch (p = .001). PRBCs and FDP were more often administered in the immediate dispatch group (13 and 12%, respectively) compared to the interrogate group 5% (p = .004) and 4% (p = .004), and the crew request group 3% (p = .002) and 4.3% (p = .032). Advanced analgesia in the form of ketamine was administered similarly across all groups (p = .777), as was hypertonic saline (p = .111).
Isolated head injury
Over a third of all older trauma patients that HEMS attended had a documented isolated head injury (n = 410) and a third of these received PHEA (n = 114, 27%), despite that median presenting GCS of these patients was 14. Patients most often received PHEA following a crew request (35%) especially when the presenting GCS was < 8 (p = .005). Anticoagulant reversal was administered in a similar proportion of patients across each dispatch type (p = .152) (Table 3).
Discussion
In this retrospective cohort analysis on HEMS dispatch to older trauma, we demonstrate that many older trauma patients who do not fulfil the initial criteria for immediate dispatch, need advanced interventions and subsequent tertiary level care at a major trauma centre.
Older trauma represents 20% of all major trauma in the UK [4] and projections suggest that by 2040 one in four people will be aged 65 or over [3]. With the greatest proportion attended aged between the ages of 65–74 years, older trauma represents a significant proportion (20%) of all trauma attended by HEMS, consistent with the current literature [1, 2, 13]. The increasing national trend may be attributed to improved detection and documentation [14], however, the explanation for increasing older trauma seen by HEMS is more likely due to the proportional increase of older people and greater independence, and comprehensive clinical assessment by on-scene clinicians.
HEMS are often associated with major trauma as a result of significant mechanism; however, we report that in an older patient, HEMS are frequently requested after an innocuous mechanism. Falls from < 2 m comprised a significant proportion of the patients attended in our study, which is consistent with both wider literature [3, 15,16,17] and TARN data where falls from standing height contribute significantly to the mechanism of injury [2]. Low impact trauma and specifically low energy falls result in 30% of serious injury in patients > 65 years, compared to 4% in < 65 years; and are 10 times more likely to cause death [15, 18]. Only 33–50% of older trauma patients protect themselves with outstretched arms, compared to 90% of younger adults [4]. This exposes patients to head, neck and thoracic injuries with a high injury severity that is disproportionate to mechanism [14], with associated worse functional outcomes regardless of injury severity [19, 20]. With a heavier weighting on mechanism in our dispatch criteria we could argue it is not suitably adapted to the older trauma patient, hence there are a greater proportion of crew requests than in patients < 65 years.
In our study, the likelihood that HEMS was dispatched on request of a ground crew instead of immediately or after interrogation occurred with a higher frequency with increasing age. As previously noted, serious injury can be masked and clinicians at scene have limited diagnostic tools to aid them in injury identification [18]. The implication of undetected occult injuries, insensitivity of triage tools and clinical decision-making in pre-hospital care is under-triage [18, 21,22,23]. Under-triage is reported to be as high as 58% in patients aged 90 and over [24]. Thus, further exploratory analysis is required on the characterisation of older trauma patients whom are under or over-triaged within trauma networks to feedback into the decision-making of initial clinicians.
Advanced pre-hospital critical care interventions were performed in a high proportion of older trauma activations. We report that even when HEMS was delayed to dispatch, and a passage of time exists whilst the ground ambulance crew assess the patient, a high proportion still required advanced interventions. One such intervention is PHEA, which was increasingly performed when the dispatch category was crew request, irrespective of whether the patient had polytrauma or isolated head injury. It is well documented that older adults with a significant head injury present with a higher functioning GCS compared to younger adults with the same severity of injury, and that GCS is not a good representation of injury severity [25, 26]. This may contribute to under-triage of these patients during the primary dispatch process.
Advanced interventions provided by HEMS are an unparalleled resource and lowering dispatch triggers without robust data would compromise operational models. Dispatch sensitivity may be enhanced by adapting the algorithm to include mechanism adapted to the older trauma patient. For example, we could consider prioritising a 999/112 call advising us of an older person with potential for traumatic injury in combination with a more moderate mechanism. For example, a pedestrian RTC at a speed of >30mph as opposed to 40mph. Novel approaches which review call communication and conversation analysis between the caller or bystander and call taker may allow us to identify unknown criteria missing from reviews of dispatch accuracy. Similarly, live video-transmission from scene may help gauge physiological parameters and expedite dispatch [27].
A marked proportion of older trauma from the crew request dispatch were conveyed to an MTC with the HEMS team by aircraft or land. The regionalisation of trauma services within the study area necessitates targeted critical care resources, and the time-saving nature of expedited transport by helicopter to definitive care itself is advantageous. In combination both HEMS attendance and transport type has shown a significant benefit from ‘low level falls’ in patients with ISS 9 to 15 [7, 28]. The transportation platform, on-scene management and preferred admission to an MTC alone were deemed contributory to survival benefit [29]. A major trauma pre-alert more commonly results in direct transfer to CT in older patients, which conveys earlier detection of injuries [7]. On a HEMS pre-alert a full trauma team will be assembled, this may not be the case when conveyed by a land crew.
Limitations
Inherent limitations are common to our retrospective design. First, we had to rely on the data as provided by the HEMS teams. Although there were some missing data, overall data completeness was good due to the use of our electronic patient record with dedicated data entry fields for all patients. Further, no causal relations could be established due to the retrospective design. Finally, our findings cannot be generalized to non-HEMS dispatch, as we appreciate that HEMS only attends a fraction of elderly patients and confounding by indication has most certainly contributed to the relatively high number of HEMS interventions in our study population. Although considered highly relevant in our study cohort, confounding variables such as co-morbidities, polypharmacy and pre-injury status are not reported. Although it could be inferred that HEMS are tasked to the most critical older trauma patients our study lacks sufficient physiology data and patient follow-up to infer the implication of dispatch accuracy on patient benefit.
Conclusion
Older trauma patients sustain minor injuries warranting HEMS attendance by seemingly innocuous mechanisms, and do not fulfil criteria for immediate HEMS dispatch. However, a high proportion of patients require advanced clinical interventions, such as PHEA, and subsequent tertiary level care at a major trauma centre. Dispatch accuracy may be improved by the addition of physiological parameters to mechanism information. Further studies should evaluate if HEMS activation criteria, nuanced by age-dependant triggers for mechanism and physiological parameters, optimise dispatch sensitivity and HEMS utilisation.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- HEMS:
-
Helicopter Emergency Medical Services
- IQR:
-
Interquartile Range
- RTC:
-
Road Traffic Collision
- PHEA:
-
Pre-hospital Emergency Anaesthesia
- MTC:
-
Major Trauma Centre
- TARN:
-
Trauma Audit and Research Network
- CCP:
-
Critical Care Paramedic
- EOC:
-
Emergency Operations Centre
- MOI:
-
Mechanism of Injury
- PCC:
-
Prothrombin Complex Concentrate
- USS:
-
Ultrasound sonography
- ICD:
-
Intercostal chest drain
- IV:
-
Intravenous
- PRBC:
-
Packed Red Blood Cells
- FDP:
-
Freeze-dried plasma
- NIHR:
-
National Institute for Healthcare Research
- CI:
-
Confidence Interval
- STROBE:
-
Strengthening the Reporting of Observational Studies in Epidemiology Guidelines
- GCS:
-
Glasgow Coma Score
- CT:
-
Computed Tomography
References
Sammy I, Lecky F, Sutton A, Leaviss J, O’Cathain A. Factors affecting mortality in older trauma patients-a systematic review and meta-analysis. Injury. 2016;47(6):1170–83.
Trauma Audit and Research Network - Major Trauma in Older People - 2017 Report. 2018 [cited 2018 Feb 15]. Available from: https://www.tarn.ac.uk/Content.aspx?c=3793.
Kehoe A, Smith JE, Edwards A, Yates D, Lecky F. The changing face of major trauma in the UK. Emerg Med J. 2015;32(12):911–5.
Hendrickson SA, Osei-Kuffour D, Aylwin C, Fertleman M, Hettiaratchy S. ‘Silver’ trauma: predicting mortality in elderly major trauma based on place of injury. Scand J Trauma Resusc Emerg Med. 2015;23(2):A4.
Schellhaaß A, Popp E. Air rescue: current significance and practical issues. Anaesthesist. 2014;63:971–82.
Giannakopoulos G, Bloemers F, Lubbers W. Criteria for cancelling helicopter emergency medical services (HEMS) dispatches. Emerg Med J. 2012;29:582–6.
Andruszkow H, Schweigkofler U, Lefering R, Frey M, Horst K, Pfeifer R, et al. Impact of helicopter emergency medical Service in Traumatized Patients: which patient benefits Most? PLoS One. 2016;11(1):e0146897. https://doi.org/10.1371/journal.pone.0146897.
Hirshon J, Galvagno SM, Comer A. Maryland’s helicopter emergency medical services experience from 2001 to 2011: system improvements and patients’ outcomes. Ann Emerg Med. 2016;67:332–40.
McQueen C, Smyth M, Fisher J, Perkins G. Does the use of dedicated dispatch criteria by emergency medical services optimise appropriate allocation of advanced care resources in cases of high severity trauma? A systematic review. Injury. 2015;46:1197–206.
Grossmann FF, Zumbrunn T, Frauchiger A, Delport K, Bingisser R, Nickel CH. At risk of undertriage? Testing the performance and accuracy of the emergency severity index in older emergency department patients. Ann Emerg Med. 2012;60(3):317–325.e3.
Munro S, Joy M, de Coverley R, Salmon M, Williams J, Lyon R. A novel method of non-clinical dispatch is associated with a higher rate of critical Helicopter Emergency Medical Service intervention. Scand J Trauma Resusc Emerg Med. 2018;26(1):84.
von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet. 2007;370(9596):1453–7.
Acharya K, Schindler A, Heller T. Aging: Demographics, trajectories and health system issues. Health Care People Intellect Dev Disabil Lifesp. 2016;1:423 [cited 2018 Feb 15]; Available from: https://uic.pure.elsevier.com/en/publications/aging-demographics-trajectories-and-health-system-issues.
Lecky F, Woodford M, Edwards A. Trauma scoring systems and databases. Br J Anaesth. 2014;113:286–94.
Hawley C, Sakr M, Scapinello S, Salvo J, Wrenn P. Traumatic brain injuries in older adults—6 years of data for one UK trauma centre: retrospective analysis of prospectively collected data. Emerg Med J. 2017;34(8):509–16.
Beck B, Cameron P, Lowthian J, Fitzgerald M, Judson R, Gabbe BJ. Major trauma in older persons. BJS Open. 2018;2(5):310.
Gardner RC, Dams-O'Connor K, Morrissey MR, Manley GT. Geriatric traumatic brain injury: epidemiology, outcomes, knowledge gaps, and future directions. J Neurotrauma. 2018;35(7):889–906.
Potter D, Kehoe A, Smith JE. The sensitivity of pre-hospital and in-hospital tools for the identification of major trauma patients presenting to a major trauma Centre. J R Nav Med Serv. 2013;99(1):16–9.
McIntyre A, Mehta S, Aubut J, Dijkers M, Teasell RW. Mortality among older adults after a traumatic brain injury: a meta-analysis. Brain Inj. 2013;27(1):31–40.
Dams-O'Connor K, Gibbons LE, Bowen JD, McCurry SM, Larson EB, Crane PK. Risk for late-life re-injury, dementia and death among individuals with traumatic brain injury: a population-based study. J Neurol Neurosurg Psychiatry. 2013;84(2):177–82.
Chang DC, Bass RR, Cornwell EE, MacKenzie EJ. Undertriage of elderly trauma patients to state-designated trauma centers. Arch Surg. 2008;143(8):776–81.
Hsia RY, Wang E, Saynina O, Wise P, Auerbach A. Factors associated with trauma center use for elderly patients with trauma: a statewide analysis, 1999-2008. Arch Surg. 2011;146(5):585–92.
Newgard CD, Nelson MJ, Kampp M, Saha S, Zive D, Schmidt T, et al. Out-of-hospital decision-making and factors influencing the regional distribution of injured patients in a trauma system. J Trauma. 2011;70(6):1345.
Nakamura Y, Daya M, Bulger EM, Schreiber M, Mackersie R, Hsia RY, et al. Evaluating age in the field triage of injured persons. Ann Emerg Med. 2012;60(3):335–45.
Salottolo K, Levy AS, Slone DS, Mains CW, Bar-Or D. The effect of age on Glasgow Coma Scale score in patients with traumatic brain injury. JAMA Surg. 2014;149(7):727–34.
Rau C-S, Wu S-C, Chen Y-C, Chien P-C, Hsieh H-Y, Kuo P-J, et al. Effect of age on glasgow coma scale in patients with moderate and severe traumatic brain injury: an approach with propensity score-matched population. Int J Environ Res Public Health. 2017;14(11):1 [cited 2018 Jun 20]. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5708017/.
ter Avest E, Lambert E, De Coverly R, Tucker H, Griggs J, Wilson MH, et al. Live video footage from scene to aid helicopter emergency medical service dispatch: a feasibility study. Scand J Trauma Resusc Emerg Med. 2019;27(1):55.
Joseph B, Pandit V, Zangbar B, Kulvatunyou N, Hashmi A. Green, D et al. 2014. Superiority of frailty over age in predicting outcomes among geriatric trauma patients: a prospective analysis. JAMA Surg. 2014;149(8):766–72. https://doi.org/10.1001/jamasurg.2014.29.
Voskens FJ, van Rein EA, van der Sluijs R, Houwert RM, Lichtveld RA, Verleisdonk EJ, et al. Accuracy of prehospital triage in selecting severely injured trauma patients. JAMA Surg. 2018;153(4):322–7.
Acknowledgements
We acknowledge the South East Coast Ambulance Service Trust, and associated NHS Hospital Trusts for their ongoing support.
Funding
No funding was received for this study.
Author information
Authors and Affiliations
Consortia
Contributions
All authors were involved in the study design. JB and ETA performed statistical analysis. Data analysis and interpretation was performed by JG, JB, RDC and ETA. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Internal service approval was sought from the Research, Audit and Development Department at KSSAAT. All patient data were collected routinely as standard; therefore, ethics committee approval was not required. Patient identifiable data has been anonymised and stored on electronic devices with technical encryption (Data Protection Act, 1998).
Consent for publication
Not applicable.
Competing interests
JG, ETA, RDC, MN and RL are all employees of Air Ambulance Kent, Surrey and Sussex. JB, JW and MN are employees of South East Coast Ambulance Service NHS Foundation Trust. There were no financial or non-financial conflicts of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
HEMS tasking criteria AAKSS version 2.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Griggs, J.E., Barrett, J.W., ter Avest, E. et al. Helicopter emergency medical service dispatch in older trauma: time to reconsider the trigger?. Scand J Trauma Resusc Emerg Med 29, 62 (2021). https://doi.org/10.1186/s13049-021-00877-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13049-021-00877-3