
Abstract
Background
Histological analysis has revealed the need for new treatment techniques for epithelial ovarian cancer. Immune checkpoint inhibitors may be a new therapeutic strategy for ovarian clear cell carcinoma (OCCC). Lymphocyte-activation gene 3 (LAG-3), an immune checkpoint, is a poor prognostic factor and a new therapeutic target for several malignancies. In this study, we demonstrated the correlation between LAG-3 expression and the clinicopathological features of OCCC. We evaluated LAG-3 expression in tumor-infiltrating lymphocytes (TILs) via immunohistochemical analysis using tissue microarrays containing surgically resected specimens from 171 patients with OCCC.
Results
The number of LAG-3-positive cases was 48 (28.1%), whereas the number of LAG-3-negative cases was 123 (71.9%). LAG-3 expression significantly increased in patients with advanced stages (P = 0.036) and recurrence (P = 0.012); however, its expression did not correlate with age (P = 0.613), residual tumor (P = 0.156), or death (P = 0.086). Using the Kaplan − Meier method, LAG-3 expression was found to be correlated with poor overall survival (P = 0.020) and progression-free survival (P = 0.019). Multivariate analysis revealed LAG-3 expression (hazard ratio [HR] = 1.86; 95% confidence interval [CI], 1.00 − 3.44, P = 0.049) and residual tumor (HR = 9.71; 95% CI, 5.13 − 18.52, P < 0.001) as independent prognostic factors.
Conclusion
Our study demonstrated that LAG-3 expression in patients with OCCC may be a useful biomarker for the prognosis of OCCC and could serve as a new therapeutic target.
Similar content being viewed by others


Background
Epithelial ovarian cancer is classified into several histological types based on its morphology. The pathogenesis and clinical features, including cell origin, driver genes, response to treatment, and patient prognosis, differ depending on the histological types; however, a therapeutic strategy based on the histological types has not yet been established. Ovarian clear cell carcinoma (OCCC) is resistant to existing therapies and requires a new effective therapeutic strategy. The use of immune checkpoint inhibitors (ICIs) targeting programmed cell death-1 (PD-1)/programmed death ligand-1 (PD-L1) and cytotoxic T lymphocyte-associated antigen-4 (CTLA-4) is a promising strategy for the treatment of recurrent ovarian cancer and could be more effective for OCCC than for other histological cancer types [1, 2]. Nevertheless, several limitations restrict the treatment of OCCC using ICIs, including the adverse effects of ICIs, especially the co-inhibition of CTLA-4 and PD-1 [1]. The lack of a biomarker for predicting ICI efficacy is another major problem, and data collected from experiments on the immune environment in OCCC have not provided any insights regarding this problem [3]. To overcome these limitations, we focused on a new immune checkpoint molecule.
Lymphocyte-activation gene 3 (LAG-3) is the third immune checkpoint after PD-1/PD-L1 and CTLA-4, and is expressed on the surface of several immune cells, including T cells [4]. T-cell exhaustion is characterized by the overexpression of multiple inhibitory receptors, including PD-1, CTLA-4, and LAG-3 [5]. The upregulation of LAG-3, caused by exposure to persistent inflammatory stimuli, suppresses the proliferation and activation of T cells [6, 7]. T-cell exhaustion is observed in cancers that escape from immune cells [7]. Recently, the co-inhibition of LAG-3 by relatlimab and that of PD-1 by nivolumab revealed a greater antitumor activity than that of nivolumab alone in a randomized phase III study on melanoma [8]. The results of this study also suggested that co-inhibitory LAG-3 and PD-1 are associated with fewer adverse events than co-inhibitory CTLA-4 and PD-1 [8]. Moreover, co-inhibition of LAG-3 and PD-1 enhanced antitumor activity compared with single-ICI in a mouse model of solid tumors, such as melanoma, colon adenocarcinoma, and fibrosarcoma [7]. Co-inhibition of LAG-3 and PD-1 is more effective and safer than traditional ICI therapy.
Matsuzaki et al. [9] observed that tumor-infiltrating lymphocytes (TILs) expressing LAG-3 in ovarian cancer decreased the effector function of PD-1+ CD8+ T cells and restored the effector function under co-inhibition of LAG3 and PD-1 in vitro. However, no studies have demonstrated the effect of LAG-3 expression on the prognosis of patients with OCCC. To the best of our knowledge, this study is the first to determine the relationship between LAG-3-positive TILs and their clinical features as well as the potential of LAG-3 as a new therapeutic target and clinical biomarker of OCCC.
Results
Patients’ characteristics
The patients’ characteristics are depicted in Table 1. The age of the 171 patients ranged from 32 to 80 years; the mean age was 55.3 years. Of the 171 patients, 79 (46.2%) were aged < 55 years and 92 (56.1%) were aged ≥ 55 years. The classification of patients according to the International Federation of Gynecology and Obstetrics (FIGO) staging was variable: 111 patients were in stage I (64.9%), 25 in stage II (14.6%), 31 in stage III (18.1%), and 4 in stage IV (2.3%). A total of 146 patients (85.4%) underwent complete resection, whereas 25 (14.6%) underwent incomplete resection. Adjuvant chemotherapy was administered to 129 (75.4%) patients. The regimens are as follows: paclitaxel and carboplatin were administered to 77 patients, docetaxel and carboplatin to 35, irinotecan and cisplatin to 12, and gemcitabine and carboplatin to 1 patient. Forty-four patients (25.7%) experienced recurrence, whereas 127 (74.3%) did not experience it. Thirty-two patients (18.7%) died, and 139 (81.3%) survived.
Correlation between clinicopathological features and LAG-3 expression
Table 2 presents the correlation between patient characteristics and LAG-3 expression. There were 48 LAG-3-positive cases (28.1%) and 123 (71.9%) LAG-3-negative cases. LAG-3 expression significantly increased in patients with advanced stages, FIGO stages III and IV (P = 0.036), and in cases of cancer recurrence (P = 0.012). However, no correlation was observed between LAG-3 expression and age (P = 0.613), residual tumor (P = 0.156), and death (P = 0.086).
Correlation between patients’ survival and LAG-3 expression
Kaplan − Meier curve analysis (Fig. 1) revealed that poorer overall survival (OS) (P = 0.020) and progression-free survival (PFS) (P = 0.019) were correlated more with LAG-3 expression than with no LAG-3 expression. The univariate and multivariate analyses of PFS with Cox regression analysis were also used to evaluate the correlation (Table 3). The univariate analysis indicated that advanced FIGO stages (stage III and IV; hazard ratio [HR] = 5.37; 95% confidence interval [CI], 2.95 − 9.77, P < 0.001), LAG-3 expression (HR = 2.53; 95% CI, 1.39 − 4.61, P = 0.002), and residual tumor (HR = 11.11; 95% CI, 5.95 − 20.83, P < 0.001) were prognostic factors for PFS. The multivariate analysis regarded LAG-3 expression (HR = 1.86; 95% CI, 1.00 − 3.44, P = 0.049) and residual tumor (HR = 9.71; 95% CI, 5.13 to 18.52, P < 0.001) as independent prognostic factors.

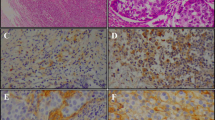
Immunohistochemical expression of the lymphocyte activation gene-3 protein (LAG-3) in ovarian clear cell carcinoma (OCCC). (a, b) LAG-3-negative case: LAG-3 expression was observed in < 20% of the total tumor-infiltrative lymphocytes. (a: H & E, ×40; b: LAG-3, ×40); (c, d) LAG-3-positive case: LAG-3 expression was observed in > 20% of total tumor-infiltrative lymphocytes. (a: H & E, ×40; b: LAG-3, ×40). OCCC cells did not express LAG-3.
Discussion
To the best of our knowledge, this study was the first to investigate the correlation between LAG-3 expression and poor prognosis in OCCC. We demonstrated that LAG-3 expression was observed in higher FIGO stages and was related to poor OS and PFS. LAG-3 expression is notably independent of prognostic factors for PFS. Patients with OCCC for a longer period presented higher expression of LAG-3 than those with OCCC for a shorter period. Conversely, several studies have demonstrated that LAG-3 expression is correlated with a good prognosis [10,11,12,13,14]. This discrepancy can be explained by the immunomodulatory as well as immune exhaustive functions of LAG-3. Soluble LAG-3 separated from the cell surface has been reported to activate dendritic cells [15]. In contrast, the upregulation of LAG-3 is a poor prognostic factor in most malignancies [16,17,18,19,20,21,22,23,24,25]. This result was consistent with the function of LAG-3 in exhausting T cells. Khalique et al. [3] suggested that regulatory T cells were excluded from the vicinity of tumor cells in low-risk patients, indicating that high-risk patients have a more immunosuppressive microenvironment than that in low-risk patients. LAG-3-expressing regulatory T cells exhibited an enhanced immune suppressive function, supporting the hypothesis that the presence of LAG-3 on TILs in patients with cancer leads to poor survival [10]. These results reflect that LAG-3 negatively regulates immune cells secondary to long-term exposure to inflammation [6, 7]. The results of previous studies on various cancers focusing on the relationship between LAG-3 expression analyzed using immunohistochemistry and/or immunofluorescence and patient prognosis are summarized in Table 4 [10,11,12,13,14, 16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35]. These results and review in this study revealed that LAG-3 on TILs is a biomarker for poor prognosis and a potential therapeutic target in advanced/recurrent OCCC.
LAG-3 has an inhibitory pathway, which differs from that of other immune checkpoints, such as PD-1/PD-L1 and CTLA-4. Co-inhibition of PD-1 and CTLA-4 enhances not only antitumor activity but also autoimmune diseases [36], as observed in mice with PD-1 or CTLA-4 deficiencies [37, 38]. Unlike PD-1 and CTLA-4, LAG-3 single deficiency was not a factor of autoimmune disease without an autoimmune background and had less antitumor activity. LAG-3 induces autoimmune diseases and enhances antitumor activity by co-inhibiting PD-1 [9, 39]. Co-inhibition of PD-1 and LAG-3 may cause fewer adverse events than co-inhibition of PD-1 and CTLA-4, which is characterized by single-deficient autoimmune disease. Co-inhibition of PD-1 and CTLA-4 has an antitumor effect in patients with OCCC, but with severe adverse events [1, 2]; however, a randomized phase III study on melanoma revealed that co-inhibition of PD-1 and LAG-3 leads to favorable outcomes [8]. These results indicate that a more suitable target for co-inhibition with PD-1 is LAG-3 rather than CTLA-4. As OCCC with LAG-3 on TILs is advanced and has a poor prognosis, LAG-3 is a promising therapeutic target. Furthermore, ICIs are effective against platinum-resistant cells [1]. Therefore, ICIs via LAG-3 may spread to platinum-resistant ovarian cancer.
This study has two limitations. First, owing to the use of tissue microarray, we were unable to examine the whole tissue, although we analyzed a large number of patients. Second, we analyzed LAG-3, but not its ligands. LAG-3 is currently being developed as a novel therapeutic target; however, it is not clear which ligands should be targeted for cancer therapy. In the future, research on the ligands that contribute to downregulation of immune cells in cancers is warranted.
Conclusions
In summary, LAG-3 expression in patients with OCCC is a useful biomarker for predicting prognosis. This study also revealed that LAG-3 can be a potential therapeutic target and an effective biomarker for predicting therapeutic efficacy in OCCC.
Materials and methods
Patients and samples
A total of 171 patients diagnosed with OCCC underwent surgery at Saitama Medical University International Medical Centre between 2007 and 2016. All study participants provided informed consent (or a formal waiver of consent). Patient data, including age, recurrence/PFS, death/OS, FIGO stage, surgical status (complete resection or incomplete resection), and treatment methods, were reviewed. All samples were collected without neoadjuvant chemotherapy. This study was approved by the Institutional Review Board of the Ethics Committee of the Saitama Medical University International Medical Centre, (IRB number, 16–257) and was performed in accordance with the guidelines of the Helsinki Declaration of 1975, as revised in 1983.
Immunohistochemical staining
The immunohistochemical expression of LAG-3 was analyzed using a tissue microarray (KIN-2, AZUMAYA, Tokyo, Japan). Tissue microarrays consisted of paraffin-embedded tissue blocks constructed by extracting 3-mm cylindrical tissue cores, with appropriate histological findings. All blocks were sliced into Sect. (4 μm thick). After deparaffinization and heat-induced antigen retrieval using 1 mM ethylenediaminetetraacetic acid (pH 9.0), all sections were incubated with 3% hydrogen peroxidase for 10 min to quench the endogenous peroxidase activity. These sections were further incubated with DAKO Blocking Reagent (Protein Block Serum-Free Ready-to-use [Code X0909], DAKO North America Inc., California, USA) at room temperature for 20 min to block nonspecific antigens. LAG-3 antibody (Ab180187, clone EPR4392, diluted 1:1,500; Abcam) was applied as the primary antibody at 4 °C overnight. Secondary antibodies (HISTOFINE Simple Stain MAX-PO MULTI [NICHIREI Code 424,151], Nichirei Biosciences Inc., Tokyo, Japan) were applied at room temperature for 45 min. The antigen/antibody complex formation was performed in 3,3ʹ-diaminobenzidine tetrahydrochloride and hydrogen peroxidase substrate solution for 10 min and counterstained with hematoxylin for 5 s.
Interpretation of immunohistochemical results
Immunohistochemical staining was performed by two researchers (SZ and MiY) who were blinded to the patients’ data. We defined brown staining of > 20% of TILs as positive LAG-3 expression (Fig. 2) [25].

Correlation between the expression of lymphocyte-activation gene 3 (LAG-3) and overall survival (OS)/progression-free survival (PFS). The correlation was obtained using Kaplan − Meier statistical analysis and log-rank test in patients with ovarian clear cell carcinoma (OCCC).
(a) PFS and LAG-3 expression; (b) OS and LAG-3 expression
Statistical analysis
Statistical analysis was performed using SPSS version 25.0 (SPSS Inc., Chicago, IL, USA). We assessed the correlation between the expression of LAG-3 and patient data using Pearson’s chi-square test or Fisher’s exact test. The Kaplan − Meier method was used to estimate survival curves. The log-rank test was used to assess the differences between the groups. The Cox proportional hazards model was used to analyze univariate and multivariate survival. Statistical significance was set at P < 0.05.
Data Availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- CI:
-
confidence interval
- CTLA-4:
-
cytotoxic T lymphocyte-associated antigen-4
- FIGO:
-
International Federation of Gynecology and Obstetrics
- HR:
-
hazard ratio
- ICI:
-
immune checkpoint inhibitor
- LAG-3:
-
lymphocyte activation gene-3
- OS:
-
overall survival
- OCCC:
-
ovarian clear cell carcinoma
- PFS:
-
progression-free survival
- PD-1:
-
programmed cell death-1
- PD-L1:
-
programmed death ligand-1
- TIL:
-
tumor-infiltrating lymphocyte
References
Zamarin D, Burger RA, Sill MW, Powell DJ Jr, Lankes HA, Feldman MD, et al. Randomized phase II trial of nivolumab versus nivolumab and ipilimumab for recurrent or persistent ovarian cancer: an NRG oncology study. J Clin Oncol. 2020;38:1814–23. https://doi.org/10.1200/jco.19.02059.
Lin YC, Wen KC, Sung PL, Chou YT, Liew PL, Chen LY, et al. Complete remission of heavily treated ovarian clear cell carcinoma with ARID1A mutations after pembrolizumab and bevacizumab combination therapy: a case report. J Ovarian Res. 2020;13:143. https://doi.org/10.1186/s13048-020-00751-3.
Khalique S, Nash S, Mansfield D, Wampfler J, Attygale A, Vroobel K, et al. Quantitative assessment and prognostic associations of the immune landscape in ovarian clear cell carcinoma. Cancers (Basel). 2021;13:3854. https://doi.org/10.3390/cancers13153854.
Workman CJ, Vignali DA. Negative regulation of T cell homeostasis by lymphocyte activation gene-3 (CD223). J Immunol. 2005;174:688–95. https://doi.org/10.4049/jimmunol.174.2.688.
Pauken KE, Wherry EJ. Overcoming T cell exhaustion in infection and cancer. Trends Immunol. 2015;36:265–76. https://doi.org/10.1016/j.it.2015.02.008.
Workman CJ, Vignali DA. The CD4-related molecule, LAG-3 (CD223), regulates the expansion of activated T cells. Eur J Immunol. 2003;33:970–9. https://doi.org/10.1002/eji.200323382.
Woo SR, Turnis ME, Goldberg MV, Bankoti J, Selby M, Nirschl CJ, et al. Immune inhibitory molecules LAG-3 and PD-1 synergistically regulate T-cell function to promote tumoral immune escape. Cancer Res. 2012;72:917–27. https://doi.org/10.1158/0008-5472.can-11-1620.
Tawbi HA, Schadendorf D, Lipson EJ, Ascierto PA, Matamala L, Gutiérrez EC, et al. Relatlimab and nivolumab versus nivolumab in untreated advanced melanoma. N Engl J Med. 2022;386:24–34. https://doi.org/10.1056/NEJMoa2109970.
Matsuzaki J, Gnjatic S, Mhawech-Fauceglia P, Beck A, Miller A, Tsuji T, et al. Tumor-infiltrating NY-ESO-1-specific CD8 + T cells are negatively regulated by LAG-3 and PD-1 in human ovarian cancer. Proc Natl Acad Sci U S A. 2010;107:7875–80. https://doi.org/10.1073/pnas.1003345107.
Burugu S, Gao D, Leung S, Chia SK, Nielsen TO. LAG-3 + tumor infiltrating lymphocytes in breast cancer: clinical correlates and association with PD-1/PD-L1 + tumors. Ann Oncol. 2017;28:2977–84. https://doi.org/10.1093/annonc/mdx557.
Hald SM, Rakaee M, Martinez I, Richardsen E, Al-Saad S, Paulsen EE, et al. LAG-3 in non-small-cell lung cancer: expression in primary tumors and metastatic lymph nodes is associated with improved survival. Clin Lung Cancer. 2018;19:249–59e2. https://doi.org/10.1016/j.cllc.2017.12.001.
Fucikova J, Rakova J, Hensler M, Kasikova L, Belicova L, Hladikova K, et al. TIM-3 dictates functional orientation of the immune infiltrate in ovarian cancer. Clin Cancer Res. 2019;25:4820–31. https://doi.org/10.1158/1078-0432.ccr-18-4175.
Gebauer F, Krämer M, Bruns C, Schlößer HA, Thelen M, Lohneis P, et al. Lymphocyte activation gene-3 (LAG3) mRNA and protein expression on tumour infiltrating lymphocytes (TILs) in oesophageal adenocarcinoma. J Cancer Res Clin Oncol. 2020;146:2319–27. https://doi.org/10.1007/s00432-020-03295-7.
Rhyner Agocs G, Assarzadegan N, Kirsch R, Dawson H, Galván JA, Lugli A, et al. LAG-3 expression predicts outcome in stage II colon cancer. J Pers Med. 2021;11:749. https://doi.org/10.3390/jpm11080749.
Demeure CE, Wolfers J, Martin-Garcia N, Gaulard P, Triebel F. T lymphocytes infiltrating various tumour types express the MHC class II ligand lymphocyte activation gene-3 (LAG-3): role of LAG-3/MHC class II interactions in cell-cell contacts. Eur J Cancer. 2001;37:1709–18. https://doi.org/10.1016/s0959-8049(01)00184-8.
Bottai G, Raschioni C, Losurdo A, Di Tommaso L, Tinterri C, Torrisi R, et al. An immune stratification reveals a subset of PD-1/LAG-3 double-positive triple-negative breast cancers. Breast Cancer Res. 2016;18:121. https://doi.org/10.1186/s13058-016-0783-4.
Guo M, Yuan F, Qi F, Sun J, Rao Q, Zhao Z, et al. Expression and clinical significance of LAG-3, FGL1, PD-L1 and CD8(+)T cells in hepatocellular carcinoma using multiplex quantitative analysis. J Transl Med. 2020;18:306. https://doi.org/10.21203/rs.3.rs-19039/v1.
Luo F, Cao J, Lu F, Zeng K, Ma W, Huang Y, et al. Lymphocyte activating gene 3 protein expression in nasopharyngeal carcinoma is correlated with programmed cell death-1 and programmed cell death ligand-1, tumor-infiltrating lymphocytes. Cancer Cell Int. 2021;21:458. https://doi.org/10.1186/s12935-021-02162-w.
Ligon JA, Choi W, Cojocaru G, Fu W, Hsiue EHC, Oke TF, et al. Pathways of immune exclusion in metastatic osteosarcoma are associated with inferior patient outcomes. J Immunother Cancer. 2021;9. https://doi.org/10.1136/jitc-2020-001772.
Datar I, Sanmamed MF, Wang J, Wang J, Henick BS, Choi J, et al. Expression analysis and significance of PD-1, LAG-3, and TIM-3 in human non-small cell lung cancer using spatially resolved and multiparametric single-cell analysis. Clin Cancer Res. 2019;25:4663–73. https://doi.org/10.1158/1078-0432.ccr-18-4142.
Seifert L, Plesca I, Müller L, Sommer U, Heiduk M, von Renesse J, et al. LAG-3-Expressing tumor-infiltrating T cells are associated with reduced disease-free survival in pancreatic cancer. Cancers (Basel). 2021;13. https://doi.org/10.3390/cancers13061297.
Wang H, Mao L, Zhang T, Zhang L, Wu Y, Guo W, et al. Altered expression of TIM-3, LAG-3, IDO, PD-L1, and CTLA-4 during nimotuzumab therapy correlates with responses and prognosis of oral squamous cell carcinoma patients. J Oral Pathol Med. 2019;48:669–76. https://doi.org/10.1111/jop.12883.
Deng WW, Mao L, Yu GT, Bu LL, Ma SR, Liu B, et al. LAG-3 confers poor prognosis and its blockade reshapes antitumor response in head and neck squamous cell carcinoma. Oncoimmunology. 2016;5:e1239005. https://doi.org/10.1080/2162402x.2016.1239005.
Wang W, Chen D, Zhao Y, Zhao T, Wen J, Mao Y, et al. Characterization of LAG-3, CTLA-4, and CD8(+) TIL density and their joint influence on the prognosis of patients with esophageal squamous cell carcinoma. Ann Transl Med. 2019;7:776. https://doi.org/10.21037/atm.2019.11.38.
He Y, Yu H, Rozeboom L, Ellison K, Dziadziuszko R, Suda K, et al. LAG-3 protein expression in non-small cell lung cCancer and its relationship with PD-1/PD-L1 and tumor-infiltratinglymphocytes. J Thorac Oncol. 2017;12:814–23. https://doi.org/10.12659/msm.899909.
Sarradin V, Lusque A, Filleron T, Dalenc F, Franchet C. Immune microenvironment changes induced by neoadjuvant chemotherapy in triple-negative breast cancers: the MIMOSA-1 study. Breast Cancer Res. 2021;23:61. https://doi.org/10.1186/s13058-021-01437-4.
Takeuchi M, Miyoshi H, Nakashima K, Kawamoto K, Yamada K, Yanagida E, et al. Comprehensive immunohistochemical analysis of immune checkpoint molecules in adult T cell leukemia/lymphoma. Ann Hematol. 2020;99:1093–8. https://doi.org/10.1007/s00277-020-03967-x.
Minichsdorfer C, Oberndorfer F, Krall C, Kornek G, Müllauer L, Wagner C, et al. PD-L1 expression on tumor cells is associated with a poor outcome in a cohort of caucasian nasopharyngeal carcinoma patients. Front Oncol. 2019;9:1334. https://doi.org/10.3389/fonc.2019.01334.
Duan J, Xie Y, Qu L, Wang L, Zhou S, Wang Y, et al. A nomogram-based immunoprofile predicts overall survival for previously untreated patients with esophageal squamous cell carcinoma after esophagectomy. J Immunother Cancer. 2018;6:100. https://doi.org/10.1186/s40425-018-0418-7.
Mair MJ, Kiesel B, Feldmann K, Widhalm G, Dieckmann K, Wöhrer A, et al. LAG-3 expression in the inflammatory microenvironment of glioma. J Neurooncol. 2021;152:533–9. https://doi.org/10.1007/s11060-021-03721-x.
Gusak A, Fedorova L, Lepik K, Volkov N, Popova M, Moiseev I, et al. Immunosuppressive microenvironment and efficacy of PD-1 inhibitors in relapsed/refractory classic Hodgkin lymphoma: checkpoint molecules landscape and macrophage populations. Cancers (Basel). 2021;13. https://doi.org/10.3390/cancers13225676.
Shi X, Li CW, Tan LC, Wen S, Liao T, Zhang Y, et al. Immune co-inhibitory receptors PD-1, CTLA-4, TIM-3, LAG-3, and TIGIT in medullary thyroid cancers: a large cohort study. J Clin Endocrinol Metab. 2021;106:120–32. https://doi.org/10.1210/clinem/dgaa701.
Luo C, Xin H, Yin D, Zhao T, Hu Z, Zhou Z, et al. Characterization of immune infiltration in sarcomatoid hepatocellular carcinoma. Aging. 2021;13:15126–38. https://doi.org/10.18632/aging.203076.
Karihtala K, Leivonen SK, Karjalainen-Lindsberg ML, Chan FC, Steidl C, Pellinen T, et al. Checkpoint protein expression in the tumor microenvironment defines the outcome of classical Hodgkin lymphoma patients. Blood Adv. 2021. https://doi.org/10.1182/bloodadvances.2021006189.
Blanc-Durand F, Genestie C, Galende EY, Gouy S, Morice P, Pautier P, et al. Distribution of novel immune-checkpoint targets in ovarian cancer tumor microenvironment: a dynamic landscape. Gynecol Oncol. 2021;160:279–84. https://doi.org/10.1016/j.ygyno.2020.09.045.
Postow MA, Sidlow R, Hellmann MD. Immune-related adverse events associated with immune checkpoint blockade. N Engl J Med. 2018;378:158–68. https://doi.org/10.1183/13993003.congress-2019.pa372.
Nishimura H, Nose M, Hiai H, Minato N, Honjo T. Development of lupus-like autoimmune diseases by disruption of the PD-1 gene encoding an ITIM motif-carrying immunoreceptor. Immunity. 1999;11:141–51. https://doi.org/10.1016/s1074-7613(00)80089-8.
Tivol EA, Borriello F, Schweitzer AN, Lynch WP, Bluestone JA, Sharpe AH. Loss of CTLA-4 leads to massive lymphoproliferation and fatal multiorgan tissue destruction, revealing a critical negative regulatory role of CTLA-4. Immunity. 1995;3:541–7. https://doi.org/10.1016/1074-7613(95)90125-6.
Okazaki T, Okazaki IM, Wang J, Sugiura D, Nakaki F, Yoshida T, et al. PD-1 and LAG-3 inhibitory co-receptors act synergistically to prevent autoimmunity in mice. J Exp Med. 2011;208:395–407. https://doi.org/10.1084/jem.20100466.
Acknowledgements
We are grateful to Editage (www.editage.jp) for editing and proofreading the manuscript.
Funding
This research was supported by The Imai Foundation and Grants-in-Aid for Scientific Research (19K16778) from the Ministry of Education, Culture, Sports, Science, and Technology.
Author information
Authors and Affiliations
Contributions
SZ and MiY designed the study, evaluated immunohistochemical results, and prepared the manuscript. SZ, MiY, SA, and YK performed the statistical analyses. MiY and MM obtained all data. SA performed the immunohistochemical experiments. YK and MaY reviewed the manuscript. MiY and MaY evaluated all tumor specimens histopathologically. YK and MaY supervised this study.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Institutional Review Board of the Ethics Committee of the Saitama Medical University International Medical Centre, (IRB number, 16–257), and was performed in accordance with the guidelines of the Helsinki Declaration of 1975, as revised in 1983. All study participants provided informed consent (or a formal waiver of consent).
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zaitsu, S., Yano, M., Adachi, S. et al. Lymphocyte-activation gene 3 protein expression in tumor-infiltrating lymphocytes is associated with a poor prognosis of ovarian clear cell carcinoma. J Ovarian Res 16, 93 (2023). https://doi.org/10.1186/s13048-023-01179-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13048-023-01179-1