
Abstract
Objective
The objectives of this study were to: (i) review and provide a narrative synthesis of three-dimensional (3D) foot surface scanning methodological and statistical analysis protocols, and (ii) develop a set of recommendations for standardising the reporting of 3D foot scanning approaches.
Methods
A systematic search of the SCOPUS, ProQuest, and Web of Science databases were conducted to identify papers reporting 3D foot scanning protocols and analysis techniques. To be included, studies were required to be published in English, have more than ten participants, and involve the use of static 3D surface scans of the foot. Papers were excluded if they reported two-dimensional footprints only, 3D scans that did not include the medial arch, dynamic scans, or derived foot data from a full body scan.
Results
The search yielded 78 relevant studies from 17 different countries. The available evidence showed a large variation in scanning protocols. The subcategories displaying the most variation included scanner specifications (model, type, accuracy, resolution, capture duration), scanning conditions (markers, weightbearing, number of scans), foot measurements and definitions used, and statistical analysis approaches. A 16-item checklist was developed to improve the consistency of reporting of future 3D scanning studies.
Conclusion
3D foot scanning methodological and statistical analysis protocol consistency and reporting has been lacking in the literature to date. Improved reporting of the included subcategories could assist in data pooling and facilitate collaboration between researchers. As a result, larger sample sizes and diversification of population groups could be obtained to vastly improve the quantification of foot shape and inform the development of orthotic and footwear interventions and products.
Similar content being viewed by others


Background
Human foot morphology is highly variable and is influenced by a broad array of factors, including age [1], sex [2], ethnicity [3], body mass [4], genetic disorders [5], and musculoskeletal foot conditions such as hallux valgus [6, 7] and osteoarthritis [8]. Foot shape impacts many aspects of an individual's life, including standing balance, movement during walking, sporting performance, predisposition to lower limb injury, and footwear fit [9]. Sub-optimal footwear fit has a significant impact on an individuals comfort, risk of foot pathology development, and falls risk [10].
The impact of variation in foot shape and on footwear fit are significant barriers that consumers, clinicians, and industry face. With the use of three-dimensional (3D) scanning technology, detailed information about the foot can be obtained and analysed to quantify foot shape [11]. This detailed foot shape data can provide researchers with a greater understanding of foot shape across population groups to improve footwear design and fit. Obtaining optimal footwear fit has been increasingly difficult with the continued rise of online purchasing. Currently, there are hundreds of footwear brands on the market, and they do not follow a standardised sizing system [12, 13]. For example, length measurement differences (in the same US size) of 0.5 cm can be observed when comparing a Nike and Adidas running shoe [12]. Difficulties in obtaining correct footwear fit have resulted in higher return rates from online orders due to fit uncertainty, resulting in a negative client experience and increased cost for the company [12, 14]. Additionally, the higher return rates has a significant environmental and economic impact [15].
Although 3D surface scanning has been used to measure foot shape since the mid-1990s [16], only recently has statistical shape modelling using sophisticated morphometric and multivariate statistical analysis techniques been used to identify discrete foot types from 3D shape data [17]. These techniques allow foot shape to be separated from overall object size by using rich 3D data to identify characteristics that are unable to be measured using predetermined 2D measurements [18]. The ability to differentiate foot shape according to sex, age, ethnicity, and pathology has practical applications for footwear design from a structural and functional perspective.
Capturing a 3D model of the foot has been achieved through a variety of methods since its inception. The type of 3D scanning systems have been varied, ranging from the use of stereophotogrammetry (which uses multiple photographs taken from different angles) to structured light (patterns projected on the object) and laser scanning systems (laser/s are repeatedly projected onto a surface while the camera/s and computer system acquires the 3D data) [19]. Early scanning equipment involved using a projector paired with a charged coupled device to capture 3D foot shape [16]. In addition to these methods, smart phone cameras, digitisers, RealSense depth cameras (Microsoft® Kinect; Microsoft, Redmond, WA, USA), and adjustable height pins (Amfit® system, Amfit Inc, Vancouver, WA, USA) have been used to generate 3D foot data [20,21,22]. Recent studies primarily employ laser scanning technology; however, a wide range of laser scanners are currently available. As a result of the large variety of 3D scanning systems, potential differences in scanner specifications, scanning condition protocols, foot measurements, and statistical analysis techniques may exist between studies. To help overcome some of these issues, 3D surface scanning standards have been created by the International Organisation for Standardisation (ISO) [23] and the Institute of Electrical and Electronics Engineers (IEEE) [24], with the first ISO standard being released in 2015. However, currently it is unclear if these standards have been adopted in the literature.
To the best of our knowledge, with the exception of a broad overview of 3D foot scanning published in 2010 [25], and recent reviews specifically focused on smartphone apps [26] and comparing 3D scanning to traditional methods for fabricating orthoses [27], no studies have consolidated and reviewed the literature pertaining to 3D foot scanning methods in detail. Therefore, the objectives of this paper are to: (i) review and provide a detailed narrative synthesis of 3D foot surface scanning methodological and statistical analysis protocols, and (ii) construct a methodological checklist to help homogenise the reporting of 3D scanning and statistical analysis protocols for future studies.
Methods
This scoping review was conducted and reported in accordance with the Joanna Briggs Institute methodology for scoping reviews [28] and the PRISMA extension for scoping reviews [29].
Search strategy
Three electronic databases were searched. An initial limited search of SCOPUS, ProQuest, and Web of Science were undertaken by two independent reviewers (JJA, HBM) to identify key studies for the topic. A reviewer (JJA) and research librarian (NP) identified key text words contained in the titles and abstracts of key studies and these were used to develop a full search strategy for SCOPUS, ProQuest, and Web of Science. Key search terms were grouped into three main concepts and adapted to each database: (i) 3D foot scanning, (ii) shape modelling/analysis/morphology, and (iii) foot/feet. Concept synonyms were searched under ‘topic’ which included title, abstract, and key words. Results from within each concept were combined with ‘OR’ and between concepts were combined with ‘AND’. The search strategy is provided in Supplementary file 1. Manual citation tracking and reference checking of included studies were performed. Grey literature such as conference proceedings were screened for additional studies. Only studies published in the English language were included. Studies published from inception to March 28th, 2022, were included. Titles and abstracts were screened by two independent reviewers (JJA and HBM) for assessment against the inclusion/exclusion criteria for the review. Any disagreements on eligibility were resolved at a consensus meeting by a third independent reviewer (SEM).
Inclusion / exclusion criteria
To be included, papers needed to report studies that employed static 3D surface scanning of the foot. Studies with participants of any age, sex, geographical location, musculoskeletal pathology, or health setting were included. Papers were excluded if the studies used two-dimensional footprints only, 3D scans that did not include the medial arch, dynamic/sequential scans to infer foot movement, derived foot data from a full body scan, or diagnostic imaging techniques that may be used to create 3D models of the foot (such as x-ray, magnetic resonance imaging or computed tomography). Single case studies, studies involving 10 or fewer participants, non-English full text or conference proceedings/abstracts with less than four text pages were excluded due to a lack of detail provided, as were papers which described a scanning technique but provided no data on foot shape, and thesis dissertations. Foot dimensions measured were included if used in two or more studies.
Study selection and data extraction
Study selection and data extraction were performed independently by two reviewers (JJA and HBM). Any disagreements on study eligibility were discussed between reviewers (JJA and HBM) and resolved at a consensus meeting by a third independent reviewer (SEM). A custom generated data extraction template was created in Covidence (Covidence, Melbourne, Australia). The following individual study data were extracted from included studies: general study information (title, author, database / journal, country, and primary objective), 3D scanner characteristics (name, type, accuracy, and capture duration), study methods (e.g., sample size), 3D scanner methodology (e.g., calibration, data collection, 3D foot measures), scanner reliability (intra- and inter-rater), participant demographics (participant subgroup, age, sex, weight, height, body mass index [BMI], co-morbidities, shoe size, and ethnicity), processing techniques (meshing, smoothing, cropping, scaling, and software used), broad study design, statistical analysis approach, inclusion/exclusion criteria, and main outcomes. All 3D foot measures were cross checked using the IEEE and ISO definitions.
Results
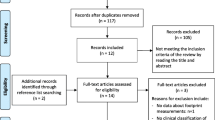
A flowchart of included studies is shown in Fig. 1. The initial search yielded 1,635 articles; from which 224 duplicates were removed. A further 1,180 articles were excluded in the title and abstract screening with an additional 153 excluded after the full text screening. A final 78 studies were deemed to meet the inclusion criteria.

Flowchart of included studies
Characteristics of included studies
The included studies originated from 17 different countries: China (n = 41) [4, 11, 30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68], Japan (n = 6) [16, 44, 69,70,71,72], Germany (n = 4) [13, 73,74,75], Romania (n = 3) [8, 76, 77], South Korea (n = 3) [78,79,80], Spain (n = 3) [22, 81, 82], United States (n = 3) [83,84,85], Italy (n = 3) [20, 21, 86], India (n = 2) [5, 87], Malaysia (n = 2) [3, 88], New Zealand (n = 2) [35, 62], Australia (n = 2) [89, 90], Belgium (n = 2) [18, 91], United Kingdom (n = 2) [92, 93], Canada (n = 1) [94], Iran (n = 1) [9], Russia (n = 1) [47], Slovenia (n = 1) [95], and Sweden (n = 1) [75]. Several study designs were utilised in the literature, these included: 51 comparisons of mean differences between groups [3, 5, 8, 9, 22, 30,31,32,33,34,35, 38,39,40,41, 43,44,45, 47,48,49,50, 52,53,54,55,56,57,58,59,60,61,62, 66, 68, 70, 72, 75,76,77,78, 80, 83, 85,86,87,88,89, 93,94,95], 20 cluster/principal component analyses [5, 11, 13, 16, 18, 31, 32, 38, 42, 51, 58, 63, 64, 68, 73, 79, 82, 85, 87, 90], 14 reliability studies [20,21,22, 34, 37, 39, 48, 49, 53, 75, 78, 88, 90, 91], 10 validation studies [20, 21, 39, 40, 46, 48, 53, 65, 78, 81], one correlation study [33], one comparison of distributions between groups [92], one regression analysis [87], and 11 repeated measures studies were reported, which were grouped into three subcategories; seven studies reported the effect of different loading conditions [4, 22, 36, 39, 74, 84, 90], three reported changes before/after exercise [62, 69, 71], and one reported different alignment methods [67]. Thirty-one studies reported participant inclusion criteria [4, 5, 9, 11, 13, 16, 32, 34, 36, 40, 43, 47, 50, 52, 56, 58, 61, 69, 71, 73, 74, 78, 79, 81, 83, 84, 87, 89, 91, 92, 94] and 30 studies reported exclusion criteria [4, 5, 9, 22, 32,33,34,35,36, 40,41,42, 46, 47, 52, 61, 67, 69, 71, 73,74,75,76, 78, 84, 89,90,91,92, 94].
Sample size ranged from 11 to 1,200,847, with 57 studies including healthy young adults [3, 4, 8, 11, 13, 16, 18, 20, 21, 30,31,32,33,34,35,36,37,38,39,40, 42,43,44,45,46, 48,49,50, 54,55,56, 59,60,61, 63,64,65,66,67,68,69,70,71, 74, 77, 78, 80,81,82,83,84, 87, 88, 90, 91, 93, 94]. Other groups included: older adults (> 65 years) (n = 18) [8, 9, 34, 38, 45, 56, 61, 70, 72, 74, 77, 82,83,84, 87, 91, 93, 94], children/adolescents (< 18 years) (n = 11) [5, 13, 37, 38, 41, 52, 56, 75, 80, 89, 92], participants with medical conditions (n = 7) (such as Down syndrome [89], diabetes [8, 34, 87], arthritis [8, 94], and cerebral palsy [5]), sports people (n = 8) (such as football (soccer) players [73], American football players [85], road cyclists [22], collegiate runners [69, 71], recreational runners [35, 62], and amateur sprinters [50]), non-habitual exercisers [50], pregnant women [4], and habitually barefoot or shod participants [35, 47]. Additionally, five studies included controls in their sample [8, 73, 87, 89, 93], while other studies did not provide specific participant characteristics [51, 58, 79, 86].
All but six studies [21, 53, 57, 65, 73, 79] reported participant sex. Fifty-three studies reported mean age (ranging from 8 to 75 years) [3, 4, 8, 9, 11, 13, 16, 18, 22, 30,31,32,33,34,35,36, 38, 40, 43,44,45,46, 48, 50, 51, 54,55,56, 58, 59, 61,62,63,64, 67,68,69,70,71,72, 74, 75, 77, 82,83,84, 86,87,88,89,90, 93, 94], and 51 reported age standard deviation [3, 4, 8, 9, 11, 13, 16, 18, 22, 30,31,32,33,34,35,36, 38, 40, 43,44,45,46, 48, 50, 51, 54,55,56, 58, 59, 61,62,63,64, 68,69,70,71,72, 74, 75, 77, 82,83,84, 86,87,88,89,90, 94]. Fifty-four studies reported minimum age (ranging from 2 to 69 years), maximum age (ranging from 7 to 87 years), and age range (2 to 87 years) [3,4,5, 9, 11, 16, 18, 20, 21, 30,31,32,33,34, 36,37,38,39,40,41,42, 46, 48,49,50, 52, 54, 55, 59, 60, 63,64,65,66,67,68, 70, 72, 74, 75, 77, 78, 80,81,82,83,84, 88,89,90,91,92,93,94]. Fifty-three studies reported mean height (ranging from 100.9 to 187.8 cm) and 52 reported height standard deviation [3, 4, 8, 9, 11, 16, 18, 22, 30,31,32, 35, 36, 38, 39, 41,42,43,44,45,46,47,48,49,50,51,52, 54,55,56, 58, 59, 61,62,63,64, 68,69,70,71,72, 74, 75, 84,85,86,87,88,89,90,91, 93, 94]. Fifty-four studies reported mean weight (ranging from 15.7 to 111.8 kg) and 53 reported weight standard deviation [3, 4, 8, 9, 11, 16, 18, 22, 30,31,32,33, 35, 36, 38, 39, 41,42,43,44,45,46,47,48,49,50,51,52, 54,55,56, 58, 59, 61,62,63,64, 68,69,70,71,72, 74, 75, 84,85,86,87,88,89,90,91, 93, 94]. Twenty-four studies reported BMI mean (ranging from 15.2 to 32.9 kg/m2), and 23 reported standard deviation [18, 20, 21, 34, 35, 41, 43,44,45, 47, 50, 52, 54, 55, 61, 68, 70,71,72, 74, 75, 89, 93, 94]. Twenty-three studies reported participant ethnicity/cultural background [3, 4, 11, 13, 31,32,33, 35, 40,41,42, 44, 55, 59,60,61, 63, 64, 68, 76, 77, 80, 88].
Scanning conditions
Sixty-seven of the included studies performed 3D surface scanning of participants in bipedal stance (half bodyweight) [3, 4, 9, 11, 13, 16, 18, 20,21,22, 30,31,32,33,34,35,36,37, 39,40,41,42,43,44,45, 47, 48, 50,51,52,53,54, 56,57,58,59, 61,62,63,64,65,66,67,68,69,70,71,72,73,74,75, 78,79,80,81,82, 84,85,86, 88,89,90,91,92,93,94,95], 11 studies with partial/semi weightbearing (seated/standing) [22, 43, 52, 59, 70,71,72, 83, 84, 86, 90], six studies in unipedal stance (full bodyweight) [18, 57, 59, 75, 84, 90], five studies in non-weightbearing (prone/supine) [4, 30, 34, 46, 57], and two studies with external bodyweight [36, 57]. Nine studies did not report the weightbearing condition [5, 8, 38, 49, 55, 60, 76, 77, 87]. Thirty-nine studies reported performing scans bilaterally [3, 5, 9, 11, 13, 18, 20,21,22, 30, 31, 33, 37, 40, 43, 44, 50, 52, 53, 55, 56, 58, 59, 61, 62, 65, 69, 70, 72, 73, 76, 77, 79, 86,87,88, 91, 92, 95] and 32 reported unilateral scanning [4, 16, 32, 34, 35, 39, 41, 42, 45,46,47,48,49, 51, 63, 64, 66,67,68, 71, 74, 75, 78, 80,81,82,83,84,85, 89, 90, 93]. Seventeen studies provided a justification if unilateral scanning was performed (random, dominant, left, right, most painful) [16, 34, 45, 63, 64, 67, 68, 74, 75, 81, 82, 84, 85, 89, 90, 93, 94]. Thirty studies analysed the right foot only [4, 9, 16, 32, 35, 39, 41,42,43,44,45, 47,48,49, 51, 63, 64, 68,69,70,71, 78, 80,81,82,83,84, 89, 92, 93], 30 analysed both feet [3, 5, 8, 11, 13, 18, 21, 22, 31, 33, 37, 40, 50, 52, 53, 55, 56, 58, 59, 61, 65, 72, 73, 75,76,77, 86,87,88, 91], and three analysed the left foot only [67, 85, 90]. Forty studies reported scanning the foot in a barefoot condition [3, 9, 16, 20,21,22, 30, 32,33,34, 36, 39, 40, 43,44,45, 47, 48, 52,53,54,55, 59, 64,65,66,67,68,69,70,71,72, 74, 81, 83, 84, 86, 92, 94, 95], while one study reported the use of socks/hosiery [46]. Twenty-eight studies reported the number of scans per foot (ranging from two to 15 scans) [4, 16, 18, 21, 22, 33, 34, 36, 39, 50, 52,53,54,55, 63, 64, 66, 68, 69, 71, 72, 75, 78, 86, 88, 90,91,92]. Thirty-three studies reported the use of scanning markers [3, 13, 16, 32,33,34, 39, 40, 42, 44, 48, 50, 51, 54, 55, 59, 61, 63, 64, 67,68,69, 71, 72, 77, 80,81,82,83,84, 86, 88, 91] and 12 used markerless scanning [20, 30, 46, 47, 52, 53, 75, 79, 92,93,94,95]. Thirty studies reported the number of markers used in their scanning process, which included a range of one to 14 markers [3, 16, 32,33,34, 39, 40, 42, 44, 48, 50, 51, 54, 55, 59, 61, 63, 64, 67,68,69, 71, 72, 80,81,82,83,84, 86, 91]. Except for four studies [22, 34, 46, 92], static platform scanners were used. Fifty-nine studies captured at or above malleolar level [3, 8, 11, 16, 18, 22, 30,31,32,33,34, 37,38,39,40,41,42, 44, 46,47,48,49,50, 53,54,55,56,57,58,59, 61, 62, 64, 66,67,68,69, 72,73,74,75,76,77, 79, 81,82,83,84,85,86,87,88,89,90,91,92,93,94,95], six studies captured the plantar surface only [4, 20, 21, 52, 65, 78], and thirteen studies did not report the depth of scan [5, 9, 13, 35, 36, 43, 45, 51, 60, 63, 70, 71, 80].
Scanner specifications
Seventy-two of the included studies reported the 3D scanner model. Twenty-five studies used the INFOOT USB scanning system (IFU-S-01, I-Ware Laboratory Co., Ltd, Japan) [3, 8, 33, 40, 41, 44, 50, 54,55,56, 58, 61, 63, 64, 68, 76, 77, 80,81,82, 85, 87,88,89, 91], seven used the YETI foot scanner (Vorum Research Corporation, Canada) [38, 48, 51, 59, 66, 67, 73], four used the Microsoft® Kinect [11, 20, 21, 53], four used the 3D easy-foot-scan (OrthoBaltic, Kaunas, Lithuania) [35, 36, 47, 62], three used the FSN-2100 (Dream GP Inc., Osaka, Japan) [43, 45, 70], two used the FotoScan 3D scanner (Precision 3D Limited, United Kingdom) [89, 94], two used the FootIn3D (Elinvision, Lithuania) [18, 90], and 25 studies reported using other scanner models not used in any other study included in this review [4, 9, 13, 16, 22, 30, 34, 37, 39, 42, 46, 49, 52, 69, 71, 72, 74, 75, 78, 79, 83, 86, 92, 93, 95]. Sixty-one studies reported the scanner type. Forty-two studies stated the use of a laser scanner [3,4,5, 9, 18, 33, 36, 38, 40, 43,44,45, 47, 48, 50,51,52, 54,55,56,57,58,59, 61, 63,64,65, 67, 68, 70, 72, 73, 79,80,81,82, 84, 85, 87, 89, 91, 93], eight studies stated the use of a structured/projected light scanner [16, 34, 37, 74, 75, 78, 89, 92], 11 studies stated other scanner types (RGB-depth camera, smartphone [LiDAR], and author own custom devices) [11, 20,21,22, 30, 32, 39, 41, 42, 46, 86], and 18 studies did not state a scanner type [8, 13, 31, 35, 49, 53, 60, 62, 66, 69, 71, 76, 77, 83, 88, 90, 94, 95]. Forty-five studies reported scanner accuracy, with a range of < 0.2 to 3.4 mm [3,4,5, 9, 11, 16, 18, 21, 30, 31, 33,34,35, 37, 40, 44, 46, 47, 49,50,51,52,53,54,55, 58, 59, 62,63,64, 68, 69, 71, 73,74,75, 78, 83, 84, 86, 89, 90, 92,93,94]. Thirty-two studies reported scanner resolution [4, 13, 16, 18, 21, 30, 33,34,35,36,37, 40, 43, 46,47,48, 51, 56, 58, 59, 70, 72,73,74,75, 78, 82,83,84,85, 88, 90, 92]. Thirty-four studies reported scanner capture duration (ranging from 0.1 to 30 s) [3, 4, 16, 18, 21, 30, 32, 34, 37, 39, 40, 42,43,44,45,46,47, 49, 50, 52,53,54, 59, 63, 64, 68, 70, 72, 78, 84, 90,91,92, 95]. Eleven studies performed independent testing for scanner accuracy [21, 39, 49, 53, 59, 69, 71, 75, 78, 86, 91].
Scanner reliability and calibration methods
Twenty-seven studies reported 3D scanner intra-rater (test–retest) reliability [20,21,22, 30,31,32,33,34, 37, 39, 40, 46, 49, 53, 59, 69, 71, 73, 75, 78, 82, 86, 88, 90,91,92,93]. Two studies reported scanner inter-rater reliability [90, 93]. Fourteen studies reported scanner calibration methods [22, 30, 33, 37, 39, 49, 57, 59, 78, 83, 84, 86, 89, 93].
Foot dimensions measured
A wide range of foot measures to quantify foot shape were reported within the included studies (see Fig. 2). Sixty-five studies measured foot length [3,4,5, 8, 9, 11, 13, 20,21,22, 30,31,32,33,34,35,36,37,38, 40,41,42,43,44, 46,47,48,49,50, 53, 55,56,57,58,59,60,61,62,63,64, 66,67,68,69,70,71,72,73,74,75,76,77, 79,80,81,82, 84, 85, 87,88,89, 91, 93,94,95], 64 studies measured ball width/breadth [3,4,5, 9, 11, 13, 20,21,22, 30,31,32,33,34,35, 37, 39,40,41,42,43,44, 46,47,48,49,50, 53, 55,56,57,58,59,60,61,62,63,64, 66,67,68,69,70,71,72,73,74,75,76,77, 79, 81,82,83,84,85,86,87,88,89, 91, 93,94,95], 51 studies measured ball girth [3, 5, 11, 22, 30,31,32,33, 37, 38, 40,41,42,43,44, 47,48,49, 53, 55,56,57, 59, 61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77, 79, 82,83,84,85,86,87,88,89, 91, 93], 51 studies measured instep height [4, 8, 13, 20, 21, 30,31,32,33,34, 38, 40,41,42,43,44, 47,48,49,50, 54, 55, 57,58,59, 61,62,63,64, 67,68,69,70,71,72,73,74,75, 78,79,80,81,82,83,84, 89, 91, 93,94,95], 43 studies measured heel width [8, 9, 13, 30,31,32,33, 40,41,42,43,44, 46,47,48, 55, 57,58,59, 61, 63, 64, 66,67,68,69, 71,72,73,74,75,76, 79, 81, 83,84,85,86, 89, 91, 93, 95], 43 studies measured length to first metatarsal head (medial arch length) [13, 21, 30,31,32,33,34, 40,41,42,43,44, 47, 48, 50, 54,55,56,57, 59, 61,62,63,64, 67,68,69,70,71, 73,74,75,76, 79, 80, 83,84,85,86, 88, 89, 91, 93], 38 studies measured instep girth [8, 22, 30,31,32,33,34, 37, 38, 40,41,42,43,44, 47,48,49,50, 55, 56, 61,62,63,64, 66,67,68, 72, 75,76,77, 79, 82, 84, 86, 87, 89, 91], 27 studies measured length to fifth metatarsal head (lateral arch length) [13, 32, 33, 40, 41, 43, 44, 47, 50, 55, 56, 61, 63, 64, 68,69,70,71, 73,74,75, 79, 84, 88, 89, 91, 93], 20 studies measured first toe angle [33, 35, 39,40,41, 43, 44, 47, 50, 61, 63, 64, 69,70,71,72, 74,75,76, 91], 20 studies measured malleolus/sphyrion height [8, 30,31,32, 41, 42, 44, 46, 48, 49, 55, 57, 59, 61, 73, 76, 81, 83, 84, 91], 19 studies measured toe height [8, 13, 32, 33, 41, 42, 57, 61, 63, 64, 68, 72, 73, 76, 81,82,83,84, 89], 17 studies measured fifth toe angle [33, 39, 40, 43, 44, 50, 61, 63, 64, 69,70,71,72, 74,75,76, 91], 13 studies measured instep width [21, 30, 31, 48, 56, 58, 59, 67, 78, 79, 83,84,85], 13 studies measured ball height [33, 37, 39, 40, 42, 50, 55, 61, 73,74,75, 91, 93], 13 studies measured navicular height (sitting/standing) [34, 41, 42, 50, 55, 61, 63, 69, 71, 72, 76, 80, 91], 12 studies measured short heel girth [5, 30, 32, 37, 41, 44, 48, 55, 67, 76, 82, 87], eight studies measured ankle girth [30, 32, 42, 48, 49, 73, 79, 87], six studies measured heel angle (frontal plane) [69, 71, 73, 76, 91, 94], six studies measured ball angle [32, 74, 75, 79, 83, 84], five studies measured long heel girth [30, 34, 48, 67, 86], three studies measured flare angle [11, 58, 85], and two studies measured toe length [50, 84]. Figure 3 shows the most commonly reported foot dimensions.

Frequency of reported 3D foot scan dimensions from the included papers

The most frequently reported 3D foot scan dimensions from the included papers. A: foot length (FL), B: ball width, C: ball girth, D: instep height, E: heel width, F: length to first metatarsal head, G: instep girth
IEEE and ISO reporting
Thirteen studies cited the ISO standards [33, 35, 39, 47, 49, 50, 57, 63, 64, 68, 80, 82, 88]. No studies cited the IEEE whitepaper standards.
Processing techniques and software used
Nineteen studies reported the processing techniques used. Sixteen studies used meshing [11, 16, 18, 20, 37, 39, 49, 52, 65, 79, 82, 88, 90, 92, 94, 95], 11 studies used smoothing [20, 35,36,37, 42, 47, 58, 78, 85, 92, 94], six studies used scaling [18, 44, 46, 79, 82, 90], and four studies used cropping [18, 79, 85, 93].
Statistical analysis techniques
Forty-three studies reported analysing mean differences (i.e., t-tests or ANOVAs) [3,4,5, 8, 9, 11, 22, 32,33,34,35,36, 39,40,41, 43,44,45, 47, 48, 50, 52, 54,55,56, 59,60,61,62, 68,69,70,71,72, 75, 76, 80, 83, 86, 87, 89, 91, 93], 24 studies reported analysing associations (i.e., Pearson’s r, Spearman’s rho, or intraclass correlation coefficients) [5, 9, 11, 16, 20, 22, 32,33,34, 40, 41, 43, 45, 49, 51, 52, 55, 58, 75, 78, 80, 84, 87, 91], and 20 studies reported performing cluster analysis (i.e., principal components analysis [PCA] or k-means) [11, 13, 16, 18, 20, 31, 32, 38, 42, 51, 56, 58, 63, 64, 68, 73, 78, 85, 87, 90].
Discussion
The purpose of this scoping review was to provide a description of the methodological and statistical analysis protocols used in 3D surface scanning of the foot. Overall, the included literature highlights large variability of methods used in 3D foot scanning. We identified four key areas that showed variability and paucity of reporting between 3D scanning methods, these included the wide range of scanners used (model, type, specifications), scanner condition protocols (weightbearing condition, markers used, number of scans, unilateral/bilateral, barefoot/socks), statistical analysis techniques, and foot measures used. Additionally, the literature included a broad range of participants (height, weight, age, sex, sport, medical condition); however, studies were heavily skewed to include healthy young adults of Chinese heritage. The predominance of young adults from Chinese heritage may be due to most studies being conducted in China and using a convenience sample. Furthermore, the included studies lacked data on pathological foot shapes (hallux valgus and osteoarthritis). This underlines the need for a consistent approach in reporting methods for future 3D surface scanning research.
The available evidence incorporated several 3D scanning models and associated scanning types to collect 3D foot shape data. The most common type of scanning system was laser scanning, with the INFOOT USB scanning system (IFU-S-01, I-Ware Laboratory Co., Ltd, Japan) being the most frequently used (see Fig. 4). However, a large proportion of studies did not report the scanning type or scanner model. Authors may have not considered this detail to be of high importance to the methods or aims of the study. Additionally, another reason may have been due to the scanner being the authors’ own custom design. A likely explanation for the variability of model selection is scanner cost with several studies using low-cost scanners such as smartphone cameras [22] and the Microsoft Kinect motion sensor [53]. Across studies, 3D scanner price ranged from approximately $200USD for a depth sensor (Microsoft® Kinect) to $20,000USD for the INFOOT USB scanning system, with the latter potentially not being economically viable for many researchers. The reporting of scanner accuracy, resolution, and capture duration were also highly variable between studies. For example, scanner accuracy, resolution, and capture duration were only reported in 39 (50%), 25 (32%), and 28 (35%) studies, respectively. Additionally, resolution was reported in several different ways, these included width x height (pixels), megapixels (width x height divided by 1 million), or total point clouds at intervals per cross section of foot length (mm) [48, 56, 84]. The variability in capture duration reporting was evident between studies. Capture duration is an important specification to include in the scanner selection process as shape data distortion can be minimised with faster capture speeds [96]. Currently, it is difficult for current and future researchers to select the best suited scanner model as there is a lack of consistency and clarity in reporting of these specifications.

The INFOOT USB scanning system (IFU-S-01, I-Ware Laboratory Co., Ltd, Japan), the most frequently reported 3D scanner from the included papers
Scanner reliability was scarcely reported, with only 21 of the 78 (26%) studies performing test–retest reliability and 13 (17%) reporting scanner calibration methods. This may be problematic as potential technical error of measurement of the observer conducting the scan could occur, and may not be identified without reliability and scanner calibration being performed prior to data collection [88]. Similarly, there was considerable variation in the number of foot scans performed per participant. Two studies examined reliability and validity of the INFOOT 3D scanner using three repeat scans per participant [91, 97]. This showed very good to excellent reliability for most measurements and a strong correlation between the scanner and both x-ray and clinical measurements [91].
Variability in weightbearing condition definitions were evident among the included studies. The description for semi/partial weightbearing and non-weightbearing were inconsistent. The IEEE define non-weightbearing as “the foot is in the air when measured not supporting any bodyweight” [24]. Several studies reported the participant in a non-weightbearing condition; however, the described position involved the participant resting their foot on the 3D scanner (in a seated or reclined position). This inconsistency would result in some weight transfer through the foot, with authors reporting this weight being up to 1% of the participant bodyweight [84]. As a result, this positioning cannot truly be classified as non-weightbearing and instead represents a partial/semi weightbearing condition. Additionally, the term ‘minimal weightbearing’ has been used by authors to describe the semi/partial weightbearing condition [90]. Since length, width, and arch height have been shown to vary in different weightbearing conditions [57] and the largest inter and intra operator foot shape differences occur in semi/partial bodyweight scans [90], it is important to have accurate descriptions of the participant scanning condition. Furthermore, there is no current definition for the external body weight condition or a specific protocol of how to collect external body weight scans. For example, authors calibrated external weight (using iron bars) and placed into vest pockets [36], while others used pressure sensors under toughened glass [57]. The IEEE definitions for weightbearing postures are shown in Fig. 5.

Diagrammatic representations of the most frequently reported 3D foot scanning postures from the included papers. A: half-weightbearing (bipedal), B: fully weightbearing (unipedal), C: non-weightbearing, D: partial weightbearing (seated), E: partial weightbearing, seated, inclined plane
The types of marker placement (manual and virtual/automatic) were inconsistent between studies. Both methods have their limitations. The manual method is time consuming and relies on an experienced investigator to accurately palpate anatomical landmarks. Automatic marker placement is faster, although there may be errors during software estimation of landmark positions [75, 98]. There was also considerable variability in the number of markers used. Some studies simply used two manual markers to identify the first and fifth metatarsal heads, then used software to estimate the other landmarks (virtual and manual) [50]. Conversely, other authors used up to 14 manual markers to identify anatomical landmarks critical for shoe fitting [81]. The use of unilateral and bilateral scanning was comparable within the included studies, with 50% and 41% of studies using bilateral and unilateral scanning, respectively. Several studies found differences between the left and right foot. The differences largely involved arch height, which was theorised to be related to foot dominance [50, 70]. These findings indicate that unilateral scanning has the potential to miss key foot shape information involving the midfoot/arch area. Furthermore, this may be more apparent in populations with unilateral foot pathology (e.g., hallux and osteoarthritis).
While all studies included in this review used 3D scanning technology and several authors applied PCA to determine foot shape, most studies performed PCA by extracting simple 1D or 2D measures (e.g., length, width, and girth measurements) from the 3D foot scan [13, 42]. This is commonly performed by predetermining the measures from all participants prior to obtaining the 3D scan, then comparing the measurement variations across the range of foot scans. This technique reduces the ability to utilise the rich shape data provided by 3D scan [99], resulting in the acquisition of incomplete foot shape data and attempting to infer 3D characteristics of the foot from 1D or 2D measurements. A more sophisticated approach was reported by Stanković et al, who collected 3D point cloud data from the scans and performed PCA by aligning mesh vertices to determine shape differences [18]. This means that the shape information that cannot be inferred from 1D or 2D measures are included to achieve a more accurate representation of the variability in foot morphology regardless of foot size (see Fig. 6).

The use of principal components analysis of 3D point cloud data to identify shape differences between females and males. Image adapted from Stankovic et al. (J Foot Ankle Res 2018;11:8)
Twenty-two scanning measures were identified that satisfied our inclusion criteria of being reported in at least two studies. There was high variability in foot measure descriptor terminology and definitions across the included studies. This resulted in multiple descriptors being used for the same foot measurement. For example, ball width (a term used by the IEEE) has been described within the included studies as ‘ball breadth’, ‘forefoot width/breadth’, ‘linear width’, ‘ball section width/breadth’, ‘metatarsophalangeal joint width’, ‘stick width’, and ‘diagonal width’, and several descriptors have been used to identify foot length from the posterior aspect of the heel to the first metatarsal head, including ‘instep length’, ‘arch length’, ‘heel-to-ball-length’, ‘ball of foot length’, ‘medial ball reach’, and ‘medial arch length’. We also found that definitions of the same foot measure varied depending on the scanner model and definition of the foot axis used. The ISO has created standards for 3D body scanning; however, foot length and width are the only included foot measures [23]. Additionally, only 13 (17%) of the included studies cited the use of these standards. The IEEE whitepaper [24] has collated several key descriptors and definitions based on various 3D scanner models to improve reporting consistency; however, no studies in this review cited the use of this resource. Furthermore, the IEEE whitepaper does not currently include a definition for ‘heel (frontal plane) angle’ and ‘navicular height’ and therefore no collective definition for these measures currently exists.
This review has several strengths. Firstly, we conducted a rigorous search strategy with the assistance of a research librarian (NP) to ensure optimum coverage of the available literature. Secondly, two independent reviewers were involved in the title and abstract screening and data extraction, with any conflicts being resolved by a third reviewer. Thirdly, we followed the Joanna Briggs Institute methodology for scoping reviews and used a standardised template for the extraction, analysis, and presentation of results [100]. However, the findings of this review should be interpreted in the context of the following key limitations. First, we did not include non-English publications in this review. Second, despite there being international standards, a wide range of foot measurement descriptors and definitions were used, so comparisons between studies were difficult. The difficulty in comparing foot descriptors and definitions was largely due to the limitations of the available literature. Third, due to limiting the included studies to ten participants, there could have been techniques missed from the excluded papers involving less than ten participants. Finally, a quality assessment of individual studies was not performed. However, this is considered optional when undertaking a scoping review and would not have been feasible considering the variability of study designs included.
Recommendations
This review highlights the need for consistent reporting of 3D foot scanning protocols. There were inconsistencies in reporting of several key areas which were highlighted between studies, these included reporting of the equipment used (type, model, scanner specifications), scanning conditions (markers, weightbearing, number of scans, unilateral versus bilateral), and definitions and descriptions of scanner measurements. Additionally, the statistical analysis approaches used throughout the literature are highly variable with many studies utilising techniques that may not optimise the shape analysis capabilities of 3D scanning technology. Although international standards (ISO and IEEE) exist, they were not widely adopted in the included studies. Based on the findings of this review, we have developed a consistent reporting method (CRITIC 16 item checklist - Consistent ReportIng Three-dimensIonal sCanning) for the identified areas above to help improve protocol transparency and reporting consistency between studies (see Table 1). The accurate reporting and improved protocol transparency has implications for holding researchers accountable for collecting reliable, repeatable, and accurate data to enhance industry products, which has never been more important in the 3D scanning space due to the increasing accessibility of 3D scanning technology.
Conclusions
The paper provides an overview of 3D foot scanning methodological and statistical analysis protocols. It can be concluded that inadequate reporting and lack of consistency in 3D foot scanning methodological and statistical analysis protocols exists. Despite the availability of international standards for 3D foot scanning, few studies utilised this resource and consequently there is a lack of homogeneity between scanning protocols. Additionally, the need for utilisation of optimal statistical analysis techniques of a diverse population group to quantify foot shape is needed. The improved consistency of 3D foot scanning methodologies and utilisation of more sophisticated statistical analysis techniques could enhance data pooling and collaboration between researchers. As a result, larger sample sizes, diversification of population groups, and simultaneous data collection could be obtained to enhance the quantification of foot shape and facilitate the development of improved orthotic and footwear products.
Availability of data and materials
Data sharing not applicable to this article as no data-sets were generated or analysed during the current study.
References
Ansuategui Echeita J, Hijmans JM, Smits S, Van der Woude LH, Postema K. Age-related differences in women’s foot shape. Maturitas. 2016;94:64–9.
Krauss I, Grau S, Mauch M, Maiwald C, Horstmann T. Sex-related differences in foot shape. Ergonomics. 2008;51(11):1693–709.
Shariff SM, Merican AF, Shariff AA: Foot morphological between ethnic groups. In: Anthropometry, Apparel Sizing and Design 2019; 317–330.
Chiou WK, Chiu HT, Chao AS, Wang MH, Chen YL. The influence of body mass on foot dimensions during pregnancy. Appl Ergon. 2015;Part A:212–7.
Kumar DS, Gautham G, Sadiq M, Das BN, Krishna KMJ. Characteristics of Foot Dimensions of Children with Cerebral Palsy and Standardizing Orthosis Size - Through an Anthropometric Pilot Study. Anthropol. 2015;20(3):727–34.
O’Connor K, Bragdon G, Baumhauer JF. Sexual dimorphism of the foot and ankle. Orthop Clin North Am. 2006;37(4):569–74.
Mickle KJ, Munro BJ, Lord SR, Menz HB, Steele JR. Foot shape of older people: implications for shoe design. Footwear Sci. 2010;2(3):131–9.
Mihai A, Dragomir A, DriŞCu M, Berijan G. Comparative Study on the Assessment of Anthropometric Parameters Defining the 3D Shape of Diabetic and Arthritic Foot. Revista de Pielarie Incaltaminte. 2009;9(1):23–31.
Jalali A, Azadinia F, Jalali M, Saeedi H, Shahabi S, Rajabi Moghadam A. Evaluating shoe fit in older adults using a 3D scanner: a cross-sectional observational study. Footwear Sci. 2020;12(3):161–71.
Menz HB, Bonanno DR. Footwear comfort: a systematic search and narrative synthesis of the literature. J Foot Ankle Res. 2021;14(1):63.
Luximon A, Jiang LY, Luximon Y. Sizing and grading methods with consideration of footwear styles. Int J Ind Ergon. 2020;78:102960.
Singh SA, Mohammad Abdulla G, Borar S, Arora S.: Footwear Size Recommendation System. 2018 arXiv:1806.11423v1 [pre-print].
Krauss I, Valiant G, Horstmann T, Grau S. Comparison of Female Foot Morphology and Last Design in Athletic FootwearAre Men’s Lasts Appropriate for Women? Res Sports Med. 2010;18(2):140–56.
Gustafsson E, Jonsson P, Holmström J. Reducing retail supply chain costs of product returns using digital product fitting. Int J Phys Distrib. 2021;51(8):877–96.
Stöcker B, Baier D, Brand BM. New insights in online fashion retail returns from a customers’ perspective and their dynamics. J Bus Econ. 2021;91(8):1149–87.
Kouchi M, Tsutsumi E. Relation between the medial axis of the foot outline and 3-d foot shape. Ergonomics. 1996;39(6):853–61.
Mitteroecker P, Gunz P. Advances in Geometric Morphometrics. Evol Biol. 2009;36(2):235–47.
Stanković K, Booth BG, Danckaers F, Burg F, Vermaelen P, Duerinck S, Sijbers J, Huysmans T: Three-dimensional quantitative analysis of healthy foot shape: A proof of concept study. J Foot Ankle Res 2018; 11(1).
Rajulu SC, B.: 3D Surface Scanning. In: The Science of Footwear. Taylor & Francis Group; 2012.
Rogati G, Leardini A, Ortolani M, Caravaggi P. Semi-automatic measurements of foot morphological parameters from 3D plantar foot scans. J Foot Ankle Res. 2021;14:18.
Rogati G, Leardini A, Ortolani M, Caravaggi P. Validation of a novel Kinect-based device for 3D scanning of the foot plantar surface in weight-bearing. J Foot Ankle Res. 2019;12:46.
San Emeterio C, Menéndez H, Guillén-Rogel P, Marín PJ: The reliability of a smartphone application in measuring the foot structure of cyclists during sitting and standing. Footwear Sci 2021.
ISO: ISO7250–1 Basic human body measurements for technological design Part 1: Body measurement definitions and landmarks; 2017.
Kouchi MB, A; McDonald, C; Jurca, A; Dessery, Y; Armitage, Z; Schwartz, L; Martirosyan, V; Dubey; S.: 3DBP Foot Measurements Terminology; 2021.
Telfer S, Woodburn J. The use of 3D surface scanning for the measurement and assessment of the human foot. J Foot Ankle Res. 2010;3:19.
Kabir MA, Rahman SS, Islam MM, Ahmed S, Laird C. Mobile Apps for Foot Measurement in Pedorthic Practice: Scoping Review. JMIR Mhealth Uhealth. 2021;9(3):e24202.
Farhan M, Wang JZ, Bray P, Burns J, Cheng TL. Comparison of 3D scanning versus traditional methods of capturing foot and ankle morphology for the fabrication of orthoses: a systematic review. J Foot Ankle Res. 2021;14:2.
Aromataris E MZE (ed.): JBI Manual for Evidence Synthesis: JBI; 2020.
Andrea C, Tricco EL, Zarin Wasifa, et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann Intern Med. 2018;169(7):467–73.
Wu G, Li D, Hu P, Zhong Y, Pan N. Automatic foot scanning and measurement based on multiple RGB-depth cameras. Text Res J. 2018;88(2):167–81.
Wu G, Li D, Hu P, Zhong Y, Pan N. Foot shape prediction using elliptical Fourier analysis. Text Res J. 2018;88(9):1026–37.
Hong Y, Wang L, Xu DQ, Li JX. Gender differences in foot shape: A study of Chinese young adults. Sports Biomech. 2011;10(2):85–97.
Lee YC. Stature estimation using foot dimensions via 3D scanning in Taiwanese male adults. Sci Justice. 2021;61(6):669–77.
Zhang L, Kit-lun Y, Pui-ling L, Yip J, Sun-pui N. Foot deformation analysis with different load-bearing conditions to enhance diabetic footwear designs. PLoS One. 2022;17(3):e0264233.
Shu Y, Mei Q, Fernandez J, Li Z, Feng N, Gu Y. Foot morphological difference between habitually shod and unshod runners. PLoS One. 2015;10(7):e0131385.
Cen X, Xu D, Baker JS, Gu Y: Effect of additional body weight on arch index and dynamic plantar pressure distribution during walking and gait termination. PeerJ 2020; 2020(4).
Yuan M, Li X, Xu J, Jia C, Li X. 3D foot scanning using multiple RealSense cameras. Multimed Tools Appl. 2021;80(15):22773–93.
Zhu JJ, Wang XX, Ma SD, Fan JF, Song S, Ma X, Ai DN, Song H, Jiang YR, Wang YT, et al. Unbiased groupwise registration for shape prediction of foot scans. Med Biol Eng Comput. 2019;57(9):1985–98.
Wan FKW, Yick KL, Yu WWM. Validation of a 3D foot scanning system for evaluation of forefoot shape with elevated heels. Measurement. 2017;99:134–44.
Hsieh MC, Zhu A, Lee YC: Stature estimation from various three-dimensional anthropometric foot measurements of Taiwanese female population. Leg Med 2022; 54.
Ran S, Liu H, Yan S, Li R, Badurova J, Yang L. Comparison of foot morphology between chinese and mongolian children. Leather Footwear J. 2020;20(2):97–108.
Xu MM, Li JX, Hong YL, Wang L. Foot type Classification for Chinease Children and Adolescents. Kinesiology. 2019;51(1):127–32.
Zhao XG, Hue F, Yu JB, Zhou ZX. Is obesity associated with foot structure and the strength of muscles that move the ankle in adult men? J Mens Health. 2022;18(3):57.
Lee YC, Kouchi M, Mochimaru M, Wang MJ. Comparing 3D foot shape models between taiwanese and japanese females. J Hum Ergol (Tokyo). 2015;44(1):11–20.
Zhao XG, Gu YD, Yu JB, Ma Y, Zhou ZX. The Influence of Gender, Age, and Body Mass Index on Arch Height and Arch Stiffness. Foot Ankle Surg. 2020;59(2):298–302.
Hu K, Zhong Y, Wu G. Reconstruction of 3D foot model from video captured using smartphone camera. J Fiber Bioeng Inform. 2015;8(3):493–500.
Liang ZQ, Yao M, Popik S, Chen FF. Analysis of Foot Morphology in Habitually Barefoot Group. J Biomimetics Biomater Biomed Eng. 2019;41:1–9.
Witana CP, Xiong SP, Zhao JH, Goonetilleke RS. Foot measurements from three-dimensional scans: A comparison and evaluation of different methods. Int J Ind Ergon. 2006;36(9):789–807.
Tu HH. Foot volume estimation formula in healthy adults. Int J Ind Ergon. 2014;44(1):92–8.
Chen LH, Chang CC, Wang MJ, Tsao LX. Comparison of foot shape between recreational sprinters and non-habitual exercisers using 3D scanning data. Int J Ind Ergon. 2018;68:337–43.
Rodrigo AS, Goonetilleke RS, Ieee: A Turning Function Based Approach for Foot Outline Classification. In: IEEE International Conference on Industrial Engineering and Engineering Management (IEEM 2009): Dec 08–11 2009; Hong Kong, Peoples R China 2009; 861–864.
Wang J, Tang L, Tang J, Chen J, Gong X, Qin L, Huang J, Deng Y, Liu X, Huang W, et al. The typically developing pediatric foot — The data of the 1744 children in China. Foot Ankle Surg. 2022;28(3):347–53.
Wang M. Xin’an W, Fan Z, Zhang S, Chen P, Liu Z: A 3D foot shape feature parameter measurement algorithm based on Kinect2. EURASIP J Image Video Process. 2018;2018(1):1–12.
Lee YC, Lin G, Wang MJJ: Evaluating arch dimension difference by using 3-D foot scanning data. In: Ergonomics in Asia: Development, Opportunities, and Challenges - Selected Papers of the 2nd East Asian Ergonomics Federation Symposium, 2011: 2012; 2012: 223–226.
Lee YC, Lin G, Wang MJJ: Evaluating gender differences in foot dimensions. In: Ergonomics for All: Celebrating PPCOE's 20 Years of Excellence - Selected Papers of the Pan-Pacific Conference on Ergonomics, 2010: 2011; 2011: 9–13.
Luximon A, Goonetilleke RS: Foot size and foot shape of children, adults and elderly. In: DHM and Posturography 2019: 295–319.
Liu GZ, Wang BX, Shi H, Luo XZ: Development and application of 3-D foot-shape measurement system under different loads. In: Conference on Smart Sensor, Phenomena, Technology, Networks, and Systems: Mar 10–12 2008; San Diego, CA; 2008.
Luximon A, Zhang YF, Luximon Y, Xiao M. Sizing and grading for wearable products. Comput Aided Des. 2012;44(1):77–84.
Xiong SP, Goonetilleke RS, Zhao JH, Li WY, Witana CP. Foot deformations under different load-bearing conditions and their relationships to stature and body weight. Anthropol Sci. 2009;117(2):77–88.
Zhang F, Zhao J, Zhao C, Wu G, Ding W, Wang H: Foot anthropometric data for young chinese population. In: Adv Intell Syst Comput. vol. 777; 2019: 183–189.
Luximon A, Luximon Y, Wong DWC, Zhang M: The geriatric 3D foot shape. In: Advances in Applied Digital Human Modeling 2010; 176–185.
Mei QC, Gu YD, Sun D, Fernandez J. How foot morphology changes influence shoe comfort and plantar pressure before and after long distance running? Acta Bioeng Biomech. 2018;20(2):179–86.
Lee YC, Chao WY, Wang MJ: Foot shape classification using 3D scanning data. In: 2012 Southeast Asian Network of Ergonomics Societies Conference: Ergonomics Innovations Leveraging User Experience and Sustainability, SEANES 2012: 2012; 2012.
Lee YC, Chao WY, Wang MJ: Developing a New Foot Shape and Size System for Taiwanese Females. In: 19th International Conference on Industrial Engineering and Engineering Management: Oct 27–29 2012; Changsha, Peoples R China 2012; 959–968.
Liu B, Shangguan N, Lin JY, Jiang KY: Individual foot shape modeling from 2D dimensions based on template and FFD. In: Global Design to Gain a Competitive Edge: An Holistic and Collaborative Design Approach Based on Computational Tools: 2008; 2008: 437–445.
Yan LW, Fang LX, Goonetilleke RS: Dimensional Tolerances Related to Feet and Their Use in Computer-aided Shoe Last Design. In: 3rd International Symposium of Textile Bioengineering and Informatics: May 28–30 2010; Coll Textiles, Shanghai, Peoples R China 2010; 891–895.
Goonetilleke RS, Witana CP, Zhao JH, Xiong SP: The Pluses and Minuses of Obtaining Measurements from Digital Scans. In: 2nd International Conference on Digital Human Modeling held at the HCI International 2009: Jul 19–24 2009; San Diego, CA; 2009: 681-+.
Lee YC, Wang MJ. Taiwanese adult foot shape classification using 3D scanning data. Ergonomics. 2015;58(3):513–23.
Fukano M, Iso S. Changes in foot shape after long-distance running. J Funct Morphol Kinesiol. 2016;1(1):30–8.
Zhao XG, Tsujimoto T, Kim B, Katayama Y, Tanaka K. Characteristics of foot morphology and their relationship to gender, age, body mass index and bilateral asymmetry in Japanese adults. J Back Musculoskelet Rehabil. 2017;30(3):527–35.
Fukano M, Inami T, Nakagawa K, Narita T, Iso S. Foot posture alteration and recovery following a full marathon run. Euro J Sport Sci. 2018;18(10):1338–45.
Saghazadeh M, Kitano N, Okura T. Gender differences of foot characteristics in older Japanese adults using a 3D foot scanner. J Foot Ankle Res. 2015;8:29.
Grimmer R, Eskofier B, Schlarb H, Hornegger J. Comparison and classification of 3D objects surface point clouds on the example of feet. Mach Vis Appl. 2011;22(2):235–43.
Grau S, Barisch-Fritz B. Improvement of safety shoe fit - evaluation of dynamic foot structure. Footwear Sci. 2018;10(3):179–87.
Barisch-Fritz B, Schmeltzpfenning T, Plank C, Grau S. Foot deformation during walking: differences between static and dynamic 3D foot morphology in developing feet. Ergonomics. 2014;57(6):921–33.
Pantazi M, Vasilescu AM, Mihai A, GurĂU D. Statistical-mathematical processing of anthropometric foot parameters and establishing simple and multiple correlations. Part 1: statistical analysis of foot size parameters. Revista de Pielarie Incaltaminte. 2017;17(4):199–208.
Sarghie B, Mihai A, Costea M, Rezuş E: Comparative Anthropometric Study Regarding the Foot of Elderly Female Population. In: Procedia Eng 2017; 2017: 182–186.
Chun S, Kong S, Mun KR, Kim J: A foot-arch parameter measurement system using a Rgb-D camera. Sens 2017; 17(8).
Baek SY, Lee K. Statistical foot-shape analysis for mass-customisation of footwear. Int J Comput Aided Eng Technol. 2016;8(1–2):80–98.
Park KN, Koh EK, Jung DY. The influence of age and gender on normalized foot arch height of Korean children and adolescents: a cross-sectional study. Footwear Sci. 2021;14(2):104–11.
García-Hernández J, Heras S, Juan A, Paredes R, Nácher B, Alemany S, Alcántara E, González JC: The MORFO3D foot database. In: Lecture Notes in Computer Science 2005; 2005: 658–665.
Alcacer A, Epifanio I, Ibanez MV, Simo A, Ballester A. A data-driven classification of 3D foot types by archetypal shapes based on landmarks. Plos One. 2020;15:1-e0228016.
Luo GM, Houston VL, Mussman M, Garbarini M, Beattie AC, Thongpop C. Comparison of Male and Female Foot Shape. J Am Podiatr Med Assoc. 2009;99(5):383–90.
Houston VL, Luo GM, Mason CP, Mussman M, Garbarini M, Beattie AC. Changes in male foot shape and size with weightbearing. J Am Podiatr Med Assoc. 2006;96(4):330–43.
Park G, Kent R. Foot shape analysis of professional American Football players. Footwear Sci. 2020;12(3):153–9.
Preatoni E, Rodano R, Squadrone R, Cazzola D, Mazzola M, Moroni G, Andreoni G, Pedotti A. Characterization of foot morphology through 3D optical measures. SAE Tec Pap. 2008;1(1):585–9.
Priyadharshini R, Saraswathy G, Gopalakrishna G, Das BN, Viswanathan V: Standardization of foot sizes of patients with diabetic foot ulcer through anthropometric survey. In: Proceedings of the 34th IULTCS Congress: Science and Technology for Sustainability of Leather: 2017; 2017: 202–210.
Rijal OBM, Hamzah MFM, Sankaraiah S, Noor NM. A three dimensional foot fourier descriptors model. ARPN J Eng Appl Sci. 2018;13(13):4042–56.
Hassan NM, Buldt AK, Shields N, Landorf KB, Menz HB, Munteanu SE. Differences in foot dimensions between children and adolescents with and without Down syndrome. Disabil and Rehabil. 2022;44(15):3959–66.
Schuster RW, Cresswell A, Kelly L. Reliability and quality of statistical shape and deformation models constructed from optical foot scans. J Biomech. 2021;115:110137.
De Mits S, Coorevits P, De Clercq D, Elewaut D, Woodburn J, Roosen P. Reliability and validity of the Infoot 3D foot digitizer for normal healthy adults. Footwear Sci. 2010;2(2):65–75.
Varga M, Price C, Morrison SC. Three-dimensional foot shape analysis in children: a pilot analysis using three-dimensional shape descriptors. J Foot Ankle Res. 2020;13(1):6.
Price C, Nester C. Foot dimensions and morphology in healthy weight, overweight and obese males. Clin Biomech. 2016;37:125–30.
Lewinson RT. R, Killick A, Wannop JW, Wiley JP, Lun VMY, Patel C, LaMothe JM, Stefanyshyn DJ: Foot structure and knee joint kinetics during walking with and without wedged footwear insoles. J Biomech. 2018;73:192.
Jurca A, Žabkar J, Džeroski S. Analysis of 1.2 million foot scans from North America, Europe and Asia. Sci Rep. 2019;9:19155.
Saunders C, Chang J: 3D Shape Capture of Human Feet and Shoe Lasts. In: The Science of Footwear. Edited by Goonetilleke RS: Taylor & Francis Group; 2012.
De Mits S, Coorevits P, De Clercq D, Elewaut D, Woodburn J, Roosen P. Reliability and Validity of the INFOOT Three-dimensional Foot Digitizer for Patients with Rheumatoid Arthritis. J Am Podiatr Med Assoc. 2011;101(3):198–207.
Gill SS, E; McDonald, C; Klepser, A; Dabolina, I.: Landmarking for product development whitepaper: The Institute of Electrical and Electronics Engineers, Inc; 2022.
Thelwell M, Bullas A, Kühnapfel A, Hart J, Ahnert P, Wheat J, Loeffler M, Scholz M, Choppin S. Modelling of human torso shape variation inferred by geometric morphometrics. PLoS ONE. 2022;17(3):e0265255.
Pollock D, Peters MDJ, Khalil H, McInerney P, Alexander L, Tricco AC, Evans C, de Moraes EB, Godfrey CM, Pieper D, et al. Recommendations for the extraction, analysis, and presentation of results in scoping reviews. JBI Evid Synth. 2022;20:1–14.
Acknowledgements
At the time this review was conducted, HBM was a National Health and Medical Research Council Senior Research Fellow (ID: 1135995). AKB and DRB are currently Deputy Editor and Associate Editor, respectively of J Foot Ankle Res. It is journal policy to remove editors from the peer review processes for papers they have co-authored.
Funding
JJA is recipient of a La Trobe – Sheffield Hallam PhD scholarship. At the time this work was conducted, HBM was recipient of a National Health and Medical Research Fellowship (ID 1135995).
Author information
Authors and Affiliations
Contributions
HBM and JJA conceived the idea and obtained funding for the study. JJA and HBM designed the study protocol with input from SEM, DBB, AKB, NP, SC and AB. JJA drafted the manuscript with input from HBM, SEM, DBB, AKB, SC, and AB. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
None to declare.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Allan, J.J., Munteanu, S.E., Bonanno, D.R. et al. Methodological and statistical approaches for the assessment of foot shape using three-dimensional foot scanning: a scoping review. J Foot Ankle Res 16, 24 (2023). https://doi.org/10.1186/s13047-023-00617-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13047-023-00617-z