
Abstract
Background
The cause of adult adenomegalies may be defiant. On the other hand, ectopic thyroid is a rare condition that happens in every 1:100000 to 300,000 of healthy individuals. Here, we present a case report that joins these two clinical rare and defiant challenges.
Clinical case
Forty-seven-year-old woman, with known thyroid nodules for several years. She had no other relevant personal or familiar history. At our appointment she had no complaints. At the physical examination she had a palpable right thyroid nodule (previously known). The routine blood analysis showed normal thyroid function. The routine cervical ultrasonography showed no dimensional progression of the known thyroid nodules and identified a 31x18mm nodule at the left supraclavicular fossa. The patient underwent a cervical, thoracic, and abdominal computed tomography that exhibited no relevant findings, such as abdominal malignancies. The cytology of the nodule showed characteristics that were “compatible with a benign follicular nodule in ectopic thyroid tissue”.
Conclusion
This is a rare case in which we incidentally found a follicular nodule in ectopic thyroid tissue in the left supraclavicular fossa. Given the rarity of the situation, clinical sense is the mainstay of treatment and follow-up.
Similar content being viewed by others

Background
The clinical evaluation of masses in the adult is frequently challenging. The detection of supraclavicular nodules is particularly worrying concerning that around 50% of the cases associate to malignancy. Right supraclavicular nodules are generally due to mediastinal, lung or oesophagus malignancies. Left supraclavicular nodules (when solitary is called Virchow node) are suspicious of abdominal malignancies [1].
On the other hand, ectopic thyroid gland is found in one in every 100,000 to 300,000 of healthy individuals, mainly females, being the most common location the base of the tongue. It has also been described in many other sites, such as sublingual, submandibular region, oesophagus, diaphragm, duodenum, and vagina [2,3,4,5]. It is usually asymptomatic and frequently is not diagnosed and the true incidence is not known; symptoms as obstruction and bleeding may occur according to the location [6, 7]. The cause of ectopic thyroid is not completely understood [6]. Thyroid is the first endocrine gland appearing during the embryonal life. This gland arises at the 3rd week of gestation and descends from caudal to the tongue bud, to the neck and finally to its pretracheal location [7, 8]. It is believed that usually the ectopic thyroid tissue arises from embryologic development, differentiation, and migration anomalies [9].
Here, we present a case report that joins these two clinical rare and defiant challenges.
Case report/case presentation
This is the case of a forty-seven-year-old woman. She was sent to the Endocrinology appointment to follow-up her known thyroid nodules. The patient reported that she had multiple thyroid nodules that were known for many years and that one of the nodules had already been submitted to fine-needle aspiration (follicular adenoma). She did not refer any other relevant personal or familiar history. She had no complaints or recent changes in her health status (namely, she denied weight loss, nausea, loss of appetite or feeling unwell). At the physical examination she had a palpable right thyroid nodule (previously known and described); she had normal blood pressure (127/80 mmHg) and heart rate (77 bpm) and had a normal body mass index.
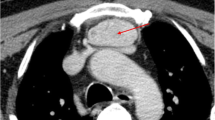
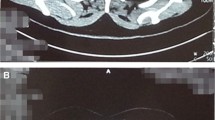
Table 1 displays some laboratory workup that shows thyroid function within the reference range. The routine cervical ultrasonography showed no dimensional progression of the known thyroid nodules; however, this exam identified an unspecific 31x18mm solid nodule at the left supraclavicular fossae (Fig. 1). Due to the concern raised with this mass, we decided to perform an ultrasound guided needle biopsy. The cytology (Fig. 2) showed characteristics that were “compatible with a benign follicular nodule in ectopic thyroid tissue”. Additionally, the patient underwent a cervical, thoracic, and abdominal computed tomography that excluded other possible causes to the incidental finding, such as abdominal malignancies. According to patients’ preference and multidisciplinary team, we agreed on active surveillance.

Ultrasonography showing an unspecific 31x18mm solid nodule at the left supraclavicular fossae

Cytologic evaluation (fine-needle aspiration of the supraclavicular mass). Here we can see numerous macrophages and epithelial cells arranged in sheets or as isolated cells. The nuclei of the epithelial cells are round and hyperchromatic. A- hematoxylin-eosin stain, 200x. B- giemsa stain, 400x. Arrows are showing thick colloid, which was seen focally
Discussion and conclusion
Here we present a case of ectopic thyroid tissue with a follicular nodule, presenting as an incidentally found left supraclavicular mass in a woman with thyroid nodules and no other relevant past or familiar history.
The cause of adult adenomegalies is sometimes straightforward, considering anamnesis and physical examination. However, it may be defiant and is, sometimes, worrisome. When found, the Virchow node must be studied given its strong association with malignancies; for this reason, it is sometimes called sentinel node. It is most frequently a metastasis of an abdominal or thoracic carcinoma, mainly from a gastric carcinoma [1, 4].
On the other hand, ectopic thyroid is a rare condition for which molecular mechanisms are largely unknown; however, there have been studies showing mutations in genes expressed in the developing thyroid [6, 10]. As far as we are concerned, there is only one case reporting ectopic thyroid tissue in the same location; nevertheless, it was associated with seeding from a previous surgical procedure [9].
Given the rarity of the situation, clinical sense is the mainstay of treatment and follow-up. Generally, authors agree that the age and status of the patient, location of the finding, local symptoms and cytology should be considered in the decision [6]. The options can be active surveillance, surgical resection, or suppressive therapy (namely in poor surgical candidates in whom the size is a problem) [6]. In this case, according to patients’ preference, we agreed on active surveillance.
Availability of data and materials
Data sharing is not applicable to this article as no datasets were generated or analysed during the current study.
References
Scully C, Langdon J, Evans J. Marathon of eponyms: 22 Virchow node. Oral Dis. 2012;18(1):107–8.
Feller KU, Mavros A, Gaertner HJ. Ectopic submandibular thyroid tissue with a coexisting active and normally located thyroid gland: case report and review of literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2000;90(5):618–23.
Takahashi T, Ishikura H, Kato H, Tanabe T, Yoshiki T. Ectopic thyroid follicles in the submucosa of the duodenum. Virchows Arch A Pathol Anat Histopathol. 1991;418(6):547–50.
Maini R, Nagalli S. Lymphadenopathy. Treasure Island (FL): StatPearls; 2022.
Salain S, Rodrigues G. Kumar S sublingual thyroid: a case report with literature review the internet. Journal of Surgery. 2007;11:1.
Guerra G, Cinelli M, Mesolella M, Tafuri D, Rocca A, Amato B, et al. Morphological, diagnostic and surgical features of ectopic thyroid gland: a review of literature. Int J Surg. 2014;12(Suppl 1):S3–11.
. S Sahu, P Agarwal, M Husain, M Harsh, N Chauhan, P Sachan Right Supraclavicular Ectopic Thyroid: An Unusual Site Of Presentation The Internet Journal of Surgery 13(1).
Taylor C, Kruskal J, Kane RA. Sonographic detection of synchronous occurrence of benign nodules in orthotopic and ectopic thyroid tissue. J Ultrasound Med. 2006;25(1):137–40.
Ballard DP, Patel P, Schild SD, Ferzli G, Gordin E. Ectopic thyroid presenting as supraclavicular mass: a case report and literature review. Journal of Clinical and Translational Endocrinology: Case Reports. 2018;10(17–20).
Szinnai G. Genetics of normal and abnormal thyroid development in humans. Best Pract Res Clin Endocrinol Metab. 2014;28(2):133–50.
Acknowledgements
Not applicable.
Funding
This work was not funded.
Author information
Authors and Affiliations
Contributions
Marta Borges-Canha followed the patient and wrote the paper. João Sérgio-Neves followed the patient and revised the manuscript. Maria Manuel Silva, Ana Isabel Oliveira, Inês Albuquerque, João Pacheco and Davide Carvalho discussed the clinical case all along the way and revised the manuscript. All authors contributed to the article and approved the submitted version.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Written informed consent was obtained from the patient for publication of this case report.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Borges-Canha, M., Sérgio-Neves, J., Albuquerque, I. et al. Virchow node of an unusual aetiology – the experience of a clinical case. Thyroid Res 15, 10 (2022). https://doi.org/10.1186/s13044-022-00128-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13044-022-00128-2