
Abstract
Introduction
This study reports the evaluation of the short-term effects of the Strengthening Families Program (SFP 10–14), adapted as Famílias Fortes (Strong Families) in Brazil, on preventing adolescent drug use and improving parenting behaviors.
Methods
A two-arm, parallel cluster randomized controlled trial was conducted in 60 Social Assistance Reference Centers (SARC) from 12 Brazilian municipalities. In each city, the SARC were randomly assigned to the intervention or control group. A total of 805 families participated in the study, each contributing data from one parent or legal guardian and one adolescent totaling 1,610 participants. Data collection occurred before intervention implementation and 6 months after baseline collection. Data were analyzed using multilevel mixed-effects modeling with repeated measures in two different paradigms: Intention to Treat (ITT) and Per protocol (PP). The study was registered in the Brazilian Ministry of Health Register of Clinical Trials (REBEC), under protocol no. RBR-5hz9g6z.
Results
Considering the ITT paradigm, the program reduced the chance of parents and legal guardians being classified as negligent by 60% (95%CI 0.21; 0.78), increased the use of nonviolent discipline by caregivers (Coef 0.33, 95%CI 0.01; 0.64) and decreased the chance of adults exposing adolescents to their drunken episodes by 80% (95%CI 0.06; 0.54). No program effects were observed on outcomes related to adolescent drug use. Similar results were found for the PP paradigm.
Conclusion
The positive effects on family outcomes suggest preventive potential of the program among the Brazilian population. Long-term evaluations are necessary to verify if the program can also achieve the drug use reduction goals not observed in the short term.
Similar content being viewed by others

Introduction
Alcohol and other drug use during adolescence are important markers for the global burden of disease in adulthood [1], and are among the leading causes of disability-adjusted life years lost among youth [2]. According to the 2019 PeNSE (Brazilian National School Health Survey), 22.6% of Brazilian students from 13 to 17 years of age had experimented with cigarettes, while 63.3% had experimented with alcohol [3]. Additionally, 13.0% of these students had used an illicit drug at some point in their lives, with recent marijuana use (30 days prior to the survey) reported by 5.3% [3]. Public policies aimed at reducing drug use [4] is essential in Brazil, especially considering that one in every five Brazilian adolescents reported getting drunk before age 13 [3].
Family-based drug use prevention programs have been implemented worldwide to decrease risk factors and increase protection for early alcohol and other drugs use [5]. These programs focus on developing and strengthening parenting skills, which act as mediators in reducing drug use by children and adolescents, and have shown the highest degree of evidence of effectiveness among interventions [6].
Strengthening Families Program (SFP) is an intervention aimed at preventing adolescent drug use and other behavioral problems by promoting parenting skills and strengthening the family bond [7]. According to its logic model [8], short-term effects on parenting skills, adolescents’ social and personal skills, and family bonds would lead to long-term outcomes, such as reduced drug use, conduct disorders, school dropout, and criminal activities. The program’s syllabus is grounded on the following social and psychological theories: (1) Family Systems Theory [9], which addresses the importance of individuation and autonomy in family relations for development of better mental health; (2) Social Learning Theory [10], which suggests that behavior can be modeled by observing other individuals’ behavior; (3) Kumpfer’s Resilience Theory [11], which emphasizes the importance of goals and purpose in life for resilience development; and (4) Reinforcement and Punishment Theory, which suggests that positive reinforcement by parents and legal guardians can increase desired behaviors, and punishment or neglect can increase undesired behaviors [12].
SFP for children and adolescents aged 10 to 14 years (SFP10-14) has undergone several effectiveness evaluations in Europe, Latin America, and the United States. Regarding the program’s primary outcomes, consistent positive effects were reported by studies conducted primarily in the United States, which showed late initiation and reduced frequency of alcohol and other drugs use [13,14,15,16]. Conversely, some European and Latin American studies found null effects on drug use prevention [17,18,19,20].
Regarding family outcomes, North American and Latin American studies have shown improvement in family cohesion and supervision [21]; increased display of affection towards the child, father’s communication and involvement with the child, family functionality, supervision of norm compliance (1); decreased aggressive behavior in family interactions [22]; resilience, involvement, family conflicts, positive parenting [23] and reduced violent parenting practices [24], despite contradictory effects for adolescent “problem-solving skills” and “parent-youth hostility” [25].
Considering the mostly positive SFP evidence found in other countries, its version developed by Oxford Brookes University, United Kingdom [26], was adapted to the Brazilian context where it was renamed Famílias Fortes and implemented in “Social Assistance Reference Centers” (SARC). Between 2013 and 2015, the program underwent cultural adaptation to the Brazilian population attending SARC in six sub-districts of Distrito Federal [27, 28]. The main goal was to maintain the core components in each lesson while adapting language, slang and situations described. Some examples of the changes introduced were the replacement of “rugby” and “basketball” with “football” to better align with the Brazilian context. Additionally, certain written activities were modified to oral formats to accommodate participants with limited literacy skills while preserving the program’s integrity [28].
From 2013 to 2019, the program was implemented by the Ministry of Health and monitored via evaluation with a “pre-experimental” design [29]. In 2019, the program began to be implemented as a public policy under the responsibility of the Ministry of Women, Family and Human Rights (MMFDH) by means of a public call for municipalities. MMFDH considered it essential to assess the program based on a gold standard study of effectiveness to guide decision-makers on whether to maintain its diffusion or make adaptations to this public policy. As the effects of interventions may not be replicated in different cultures [30], conducting randomized controlled trials (RCT) is essential to evaluate the effectiveness of the Famílias Fortes program in Brazil.
This study investigates whether the Famílias Fortes program, in the short term, is effective in preventing lifetime drug use and increasing risk perception by adolescents and in improving parenting behaviors that mediate adolescent drug use prevention (such as family skills, reduced family violence, and reduced parental exposure to drug use), measured along a 6-month follow-up.
Method
Effectiveness of the Famílias Fortes program was evaluated by a two-arm cluster randomized controlled trial (RCT) conducted in 60 Social Assistance Reference Centers (SARC) and similar municipal services, hereafter referred to globally as “social services,” from 12Footnote 1 municipalities designated by the Federal Government. These SARC are public centers responsible for delivering social programs, benefits and projects to low-income families and individuals in the community, including registering and monitoring the families benefited by Bolsa Família, a a social welfare program provided by the government to extremely low-income families. The existing SARCs were randomized in each city between intervention and control groups. Each SARC invited 15 families to participate in the study from the list of attended families and considering the inclusion criteria (have at least one child/adolescent between 10 and 14 years old; adult and teenagers living in the same house; availability to attend the 7 program meetings; live up to 1 km away from the social centers) and exclusion criteria (families with very high needs or challenges such as drug addiction and family breakdown). If the SARCs had more than 15 families interested, the first to volunteer were included in the study.
The families (made up of parents or legal guardians and child/adolescent) in the intervention group attended the Famílias Fortes program for seven weeks in person, while those from the control group were put on a waiting list to participate in the program after the end of the study. Data collection occurred at two time points: before the intervention (November/December 2021), and 6 months after implementation (May/June 2022).
Families answered self-completed, anonymous, virtual questionnaires via Android smartphone app or Internet link provided by the researchers. Parent and adolescent data were integrated through linkage considering the family confidential code. For any family code typing errors, the Levenshtein algorithm was used to pair the subjects, as described in previous studies [31, 32].
Intervention
The Famílias Fortes program (PFF-BR 10–14) is the Brazilian adaptation of the Strengthening Families Programme (SFP-UK 10–14), developed in the United Kingdom by the Oxford Brookes University [26]. PFF-BR 10–14 consists of seven consecutive weekly 2-hour in-person meetings. Caregivers and children meet separately in the first hour and spend the second hour together in family activities. All meetings include debates, games, and interactive activities and a snack is offered at the end. Some sessions have the support of videos depicting situations of daily family life. The themes of these meetings are: (1) support goals and dreams; (2) admire family members; (3) family moments; (4) understanding family values; (5) strengthen family communication; (6) family and pressure from friends; and (7) putting it all together. Highly structured, the program is guided by the instructor, caregiver, and youth manual, all available at https://www.gov.br/mdh/pt-br/navegue-por-temas/familia/familias-fortes-1.
The professionals who delivered the program (called implementers) were typically SARC employees, such as psychologists and social workers, who had been previously serving the participating families and had undergone specific training for program implementation. Program methodology training for implementers was supervised and monitored by the MMFDH team. It was conducted online via a digital platform developed specifically for distance learning courses, the training was configured as a 25-hour course divided into 3 modules: (1) Introduction and theoretical grounds of the Famílias Fortes; (2) Training to conduct the Famílias Fortes meetings, and (3) Practices for the follow-up and closing of the Famílias Fortes.
Importantly, the program’s cultural adaptation was carried out in 2014 and 2015 by the Federal University of Brasilia [27]. In this process, European everyday examples were replaced by activities typical to Brazilian everyday life. The branding, vocabulary, and presentation format of some activities were also adapted without changes in content and core elements. Evaluations of this culturally adapted version [33, 34] concluded that the program was sufficiently attractive, culturally relevant, with acceptable goals, and compatible with the needs of Brazilian families in vulnerable contexts (the target audience of the SARC).
Instruments and measures
Adolescents and caregivers each answered a self-completed, virtual, anonymous questionnaire via an Android smartphone app or Internet link made available by the researchers during data collection, without any participation of the implementers. The two questionnaires, one for parents/guardians and the other for adolescents, were built based on international instruments developed for evaluating the Strengthening Families Program (SFP 10–14) [35] in combination with instruments previously employed in effect evaluation studies of drug use prevention programs in Brazil [36, 37]. Such instruments were extracted from questionnaires widely used in several national and international studies on drugs such as the World Health Organization questionnaire used by the Brazilian Center for Drug Information (CEBRID) [38] and that used by the Substance Abuse and Mental Health Services Administration [39].
In this study, parental outcomes (family violence, parenting styles, and children’s exposure to parental drug use) and adolescent outcomes (perceived drug risk and lifetime drug use) were assessed both at baseline and at 6-month follow-up.
Parental outcomes
Family violence was assessed using the WorldSAFE Core Questionnaire scale [40] translated and validated into Brazilian Portuguese [41]. Questionnaire questions are grouped into 5 subscales: Nonviolent Discipline, Moderate Verbal Discipline, Severe Verbal Discipline, Moderate Physical Discipline, and Severe Physical Discipline. The instrument asks how often caregivers have used specific disciplinary tactics, with responses rated on a 3-point scale: never, 1–2 times, and ≥ 3 times in the previous three months. The Moderate Verbal Discipline and Severe Verbal Discipline subscales were grouped together and its corresponding score ranged from 0 to 16, in which the higher the value the higher the degree of verbal discipline imposed. The Moderate Physical Discipline and Severe Physical Discipline subscales were also grouped together and the score ranged from 0 to 24, in which the higher the value the greater the degree of physical discipline effected. Nonviolent Discipline score ranged from 0 to 10, and the higher the value, the greater the degree of nonviolent discipline employed.
Parenting styles were evaluated by the Scale of Parental Demands and Responsiveness [42], translated and validated into Portuguese [43]. Each instrument item (six items composing the demanding dimension; and ten items the responsive dimension) is assessed by a 3-point Likert scale, where values closer to three indicate greater perceived demand and responsiveness (ranging from 0 to 12 and 0 to 20, respectively). Parenting style dimensions were established using the median split procedure following the methodology proposed by previous studies [42,43,44]. Caregivers who scored at or above the median for demandingness or responsiveness were classified as high in demandingness or responsiveness, whereas caregivers with scores at or below the median were classified as low in demandingness or responsiveness. Parenting styles were organized into four categories combining these two factors: authoritative (scoring high on demandingness or responsiveness), authoritarian (scoring high on demandingness and low on responsiveness), indulgent (scoring low on demandingness and high on responsiveness), and negligent (scoring low on demandingness and responsiveness). Prior psychometric evaluation of the scale in a sample of Brazilian adolescents showed good fit: χ2 = 1518.249, p < 0.001, RMSEA = 0.050, CFI = 0.940, TLI = 0.929, WRMR = 2.377 [45].
Child exposure to parental drug use was measured by means of a block of questions that assessed the degree to which caregivers exposed their child to drug use (alcohol, cigarette, marijuana, and cocaine), such as “Do you get drunk near your child?,” and similarly to social drinking, smoking and use of illegal drugs, whose response options could be “never, sometimes, and always.”
Adolescent outcomes
Adolescent drug use was assessed as lifetime drug use (alcohol, cigarette, marijuana, inhalants, and binge drinking) and risk perception (alcohol, cigarette, and marijuana) measured by questions drawn from the CEBRID [38] and SAMHSA [39] questionnaires. Lifetime drug use (yes X no) was assessed through questions such as “Have you ever tried any alcoholic beverages?” Perceived risk was measured by one question for each drug with Likert-type response options ranging from no risk to high risk, such as “How risky is it for someone your age to smoke cigarettes once or twice?”
Covariates included age, gender, race, and socioeconomic status (SES) of the caregivers and adolescents. SES was assessed using the Brazilian Association of Research Enterprises (ABEP) scale [46], which considers the schooling of the head of the household and goods and services used by the household. ABEP score ranged from 1 to 100 points, with categories ranging from highest to lowest according to the cut-off points established in literature: high (45–100), medium [29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44], medium-low [17,18,19,20,21,22,23,24,25,26,27,28] and low (0–16) [46].
Data analysis
Program effectiveness analysis was performed according to two paradigms: Intention to Treat (ITT) and Per Protocol (PP). The ITT model considered all families who participated in the study regardless of number of meetings attended and whether or not they answered the questionnaire at follow-up. The PP model, in turn, considered only those families who had participated in at least five program sessions or more and who answered the baseline and 6-month follow-up questionnaires, aiming to ensure program evaluation among people who joined it, similar to another study [21]. Attending at least five sections was considered the protocol for MMFDH dissemination and not an arbitrary decision of the researchers.
Considering the longitudinal hierarchical structure of the data, a multilevel mixed-effects modeling with repeated measures approach was adopted. Changes in intervention outcomes use over time was evaluated by three-level mixed-effects models (level 1: repeated time observations nested within the subject; level 2: subject clustered within SARC; level 3: SARC). Models were calculated using SARC and subjects as a random effect, and explanatory variables (experimental group, time of assessment, the interaction between group and time), controlling variables (gender, age, SES), and study outcomes as fixed effects. Unadjusted estimations were obtained when considering the effect of only one independent (predictor) variable and adjusted estimations were controlled for covariates (sex, age, and socioeconomic status). Standard errors allow for intragroup correlation, that is, the observations are independent across groups (clusters) but not necessarily within groups. All models were fitted with STATA 17 program generalized linear mixed models (GLMM).
Mixed-effects models are powerful tools for analyzing cluster randomized trials that handle two sources of non-independence: the clustered observations and the repeated measures within each subject over time [47]. Additionally, mixed-effects models deal with missing data using maximum-likelihood estimation analyzing all available outcome data, regardless of whether an individual has complete data, making these models consistent with an ITT analysis [48]. In our sample, we assumed the missing data mechanism as missing at random (MAR), that is, when the probability of missing data on a variable is related to other variables measured in the model rather than the variable with missing values itself. Missing data stemmed mostly from failure to answer the follow-up assessment questionnaire and not because single items remained unanswered or due to dropping out. Mixed model for repeated measures under MAR assumption produces valid and unbiased estimations and additional methods for handling missing data, such as multiple imputation, are generally unecessary [47]. For attrition analysis, we compared families whose data from the two time-points had been matched with families who answered only the baseline questionnaire.
Results
Participants’ characteristics
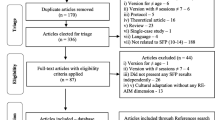
Data were collected from 805 families at baseline, 371 in the intervention group and 434 in the control group (Fig. 1). At the 6-month follow-up, 12.4% of participants were lost over time, thus valid data were collected from 705 families, 324 in the intervention group and 381 in the control group. Of the 324 families in the intervention group, 89% received five or more intervention lessons, that is, they attended at least five of the seven program meetings.

Flowchart of the randomized controlled trial of the Famílias Fortes program
The sample of adolescents consisted of 51.5% girls with a mean age of 12.6 years and mainly from the lower social status (73.5%). Caregivers were mainly adult females (91.8%) with a mean age of 39.5 (± 8.11). At baseline, the drug most used by adolescents was alcohol (13.3%) and marijuana was the substance with the highest perceived risk (75.3%). Most parents/guardians reported not exposing their children to alcohol and other drugs. Authoritative (38.3%) was the most prevalent parenting style, followed by negligent (29.1%). As for family violence, the control group showed higher scores for nonviolent discipline (3.3 ± 1.6 and 3.1 ± 1.6, respectively) and more total violence compared with the intervention group (25.5 ± 2.6 and 24.8 ± 3.7, respectively) (Table 1).
Table 2 summarizes the descriptive data for the study variables of interest (drug use, risk of drug use, parental drug use exposure, parenting styles, and family violence) concerning the control and intervention groups. Lifetime drug use increased over time in both groups. Regarding risk of drug use, the perception of high risk increased between the two time-points for the three drugs (alcohol, cigarettes, and marijuana) and for both groups. As for parenting styles, both groups showed an increase in the percentage of the authoritative style between the two time-points, whereas the intervention group had a reduction in the negligent style. Both groups presented descriptive differences between the time points for family violence scores. For example, we observed a statistically significant difference in the nonviolent discipline score of 0.30 in the control group and 0.45 in the intervention group.
Intervention effect
Regarding the program’s impact, the statistically significant outcomes, as indicated by the Intention to Treat and Per Protocol models (Table 3), encompassed the following factors: child exposure to parental drunkenness, parenting styles, and nonviolent discipline. Caregivers who participated in the program reduced their child’s exposure to episodes of drunkenness by 88% in the ITT analysis (95%CI 0.04; 0.41) and by 79% in the PP analysis (95%CI -0.30; 0.52) compared with the control group. Results from the multinomial regression showed an effect of the intervention in modifying parenting styles, indicating a 60% lower odds of caregivers being negligent (versus authoritative) in the intervention group compared with the control group in the two models assessed (ORITT = 0.40, 95%CI 0.21; 0.78 and ORpp = 0.39, 95%CI 0.19; 0.79). As for nonviolent discipline, caregivers who participated in the program reported increasing this practice by 0.32 (95%CI 0.01; 0.63) and 0.35 (95%CI 0.01; 0.70) points compared with the control group, considering the ITT and the PP models, respectively. The program failed to be effective in reducing lifetime use of any of the drugs surveyed, perceived risk of drug use among adolescents, child exposure to alcohol, tobacco, and illicit drug use, and caregivers physical and verbal violent disciplinary actions.
Attrition
Attrition was not differential by intervention condition. When comparing families who were lost at the 6-month follow-up and those who could be located, the attrition analysis showed no statistically significant difference for most sociodemographic variables and the surveyed outcomes measured at baseline. Regarding sociodemographic variables, families lost at the 6-month follow-up were slightly younger (12.2%) compared with those who completed the follow-up questionnaire (12.7%). As for outcomes, inhalant use at baseline was more common among families who did not complete the questionnaire at follow-up (12.6%) compared with those who did (6.9%). A statistically significant difference was observed in parenting styles: lost families reported that their caregivers were more forgiving (29%) and less negligent (11%) compared with followed families (14.3% and 31.8%, respectively). Further details of these analyses are shown in Table 4.
Discussion
Since a 6-month follow-up period may be insufficient to identify changes in drug use patterns among 12-year-olds, we directed our study toward examining the mediators of program effects. Famílias Fortes showed reduced negligent parenting style, increased nonviolent disciplinary practices, and decreased adolescent exposure to episodes of parental drunkenness. The program showed no short-term effect on the prevalence of lifetime alcohol and other drugs use or even increased perceived risk of these substances among adolescents. These findings are similar for the PP and ITT paradigms.
Our most robust finding showed a significant decrease in negligent parenting style in the group attending the Famílias Fortes program compared with the control group. Negligent parenting is characterized by low rates of demandingness and responsiveness in parental practices [49], i.e., parents offer low reception and emotional support to their children, in addition to low monitoring and supervision of daily activities and behaviors, such as knowing where and with whom their child is [43]. The scientific literature consensually affirms that responsive and demanding parenting practices are predictors of healthier adolescent development. Studies have shown that these parenting skills are associated with drug use prevention [45] and that children of negligent parents are at higher risk for early involvement with these substances [50]. Previous evaluations on the effect of SFP on family outcomes have also reported results similar to ours, although we could not find any articles that examined parental outcomes using the same variables (parenting styles). A US study developed in public schools found an effect of the program on improving family supervision six months after the intervention [3]. A quasi-experimental study on the Colombian adaptation of the program showed an increase in parenting skills such as expressions of affection, communication, supervision, and parental involvement in the lives of children at 12 and 18 months of follow-up [51]. Another quasi-experimental study, conducted in Chile during SFP dissemination, showed a reduction in coercive and permissive parenting practices such as yelling, insults, and lack of control when their children misbehave [24].
Famílias Fortes has also been shown to be effective in increasing nonviolent discipline education practices, with participating caregivers reporting increasing discipline strategies involving positive parenting practices. When children misbehave, caregivers explain why the child’s behavior is inappropriate and use non-aggressive parenting techniques like grounding, giving them something else to do, or even forbidding them to do something they like without any violent action [40]. Some program activities teach these techniques to parents and legal guardians by encouraging nonviolent educational strategies in response to inappropriate behavior, for example, when a child refuses to take a bath the consequence should be a reduction in video game time, not a spanking. Nonviolent discipline is a predictor of healthier youth development and less involvement in risky behaviors [52]. Similarly, a previous study evaluating the effect of SFP in the United States found that the program decreased aggressive and hostile behaviors in family interactions [22]. In another US study, the SFP applied in schools reduced adolescents’ hostility in family conflicts, but not the parents’ [25]. However, even though the program expanded the use of nonviolent educational practices, it failed to be effective in reducing verbal and physical violence. Such null fundings may be explained by the fact that the program activities put more emphasis on skills that should be acquired and not on those that need to be erased. Perhaps this is why the program was effective in increasing nonviolent discipline, but not in decreasing violent parental practices. In this regard, revisions should be made to the manual to insert clear messages of non-violence as an educational practice.
Famílias Fortes also showed an effect on caregivers’ drinking behavior, as they became less intoxicated in the presence of their children. Child exposure to increased parental drinking levels and a liberal attitude toward alcohol use are considered risk behaviors for alcohol use [53] and binge drinking [54] in adolescents. A Brazilian study observed a threefold increase in the odds of adolescent early alcohol consumption compared with those who had no experience with alcohol in the family [55].
Conversely, we observed no effect of the program in reducing the prevalence of lifetime drug use or in increasing risk perception about these substances. However, two aspects must be considered when analyzing these null findings: (1) this study evaluates short-term effects of the program (6-month follow-up after baseline collection); (2) we are dealing with adolescents who started the study with a mean age of 12.6 years and, 6 months later, were turning 13. Thus, two hypotheses should be considered. The first, and more robust, stems from the program’s logic model which understands the reduction in drug use as a distal outcome arising from changes in parenting styles, taken as proximal outcomes [14, 33]. Previous studies on program effect have shown a more consistent reduction in alcohol and drug use prevalence and initiation, with more significant results after 6 months of follow-up. A US study [14] followed students from 6th to 12th grade and showed a universal prevention shield effect. No significant difference between controls and intervention on drug use was observed at 6-month and 1-year follow-up; however at 2-, 3-, and 4-year follow-ups, the control group was more susceptible to initiation of illicit substance use [13]. A second hypothesis is that since Brazilian adolescents start consuming alcohol on average around 13.5 years old [38], our sample showed low prevalence of consumption of all substances. As such, age need to advance so adolescents can draw on the developed skills when the opportunity for experimentation arises. Consequently, new program evaluations with at least 12-month follow-up is required to effectively verify if any positive effect on drug use can occur.
Importantly, in European countries who implemented the same program as ours, it has failed to reproduce the same strong effects as the US version of reducing illicit drug use initiation by almost 50% in a 6-year follow-up [14], showing mostly null effects on all substance use outcomes. In Poland [19] and the UK [20], the program was not effective in reducing drug use at up to 2 years of follow-up; and in Sweden [18], at up to 4 years of follow-up. In contrast, a 50% reduction in the prevalence of cigarette experimentation was identified in Germany 18 months after program implementation [15]. In Spain, the program showed a reduction trend in drug use progression; however, the study had methodological limitations, as it did not use a gold standard for effectiveness evaluation [17].
Other hypotheses for this lack of effectiveness among adolescents include the implementers’ inability to carry out activities aimed at adolescents since these require more training than delivering sessions to adults, or even that the activities designed for adolescents might not be effective in reducing consumption since the program targets a very wide age range (adolescents from 10 to 14 years old). An activity designed for a 10-year-old might not engage a 14-year-old and vice versa. Another point to consider is the superficial or poorly conducted discussion about alcohol and other drugs in adolescent workshops, which, although present, may not have been sufficient or well conducted. Finally, even after a few years of follow-up, we may find that the program is not effective in reducing alcohol and drug use among adolescents, as identified in Europe.
As for study limitations, we highlight that 12% of the families were lost during the 6-month follow-up and, additionally, 23.3% of the families in the intervention group did not participate in all program meetings. However, this is a low sample loss compared with another Brazilian study with a sample loss of 38% [56], and other SFP studies, where attrition rates ranged from 21% [21] to 44% [25] after 6 months. Regarding the difficulty in maintaining participant adherence throughout the intervention, in Spain only 65.38% regularly attended the main program sessions, a much lower family participation than in our study [17]. But the sessions were held in places of easy access to families and by known SARC professionals [21]. Another limitation was assessment performed by self-reported scales rather than observations of family interactions as in Semeniuk et al. [25], which may generate information bias. However, most SFP studies have conducted assessments using self-completed questionnaires due to lower costs and less need for rater training [56]. Our findings cannot be generalized to the Brazilian population. Importantly, this is the only study in Latin America that evaluated SFP by RCTs, a gold standard study design for intervention evaluation [57]. Moreover, the findings need to be interpreted with caution as the effect sizes found are small and confidence intervals for some of the estimations are quite large.
In conclusion, the Brazilian version of the SFP 10–14 program showed effectiveness in enhancing parenting skills and nonviolent educational practices, as well as reducing parental drinking behavior near their children. These family-level positive results demonstrate the program’s preventive and health-promoting potential, since evidence about the influence of family behaviors on adolescent development is conclusive. Future studies should conducted a long-term evaluation of the program effects to see if changes in family outcomes achieve the preventive results for adolescent drug use, as well as investigate why the program failed to modify other outcomes predicted in its logic model.
At this stage, the researchers suggest that the program be continued, given its positive effects on family outcomes and its importance for Brazilian public policies related to family environment, drugs and violence, but in conjunction with further studies aimed at improving it. Potential issues regarding day and time of implementation (weekdays and working hours are not the best moment for meetings), lack of good physical structure and human resources for program delivery, the broad age of adolescents involved (10 to 14 years old), and literacy of vulnerable parents should be considered in a new cultural adapted version.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Notes
Barueri/SP, Campina Grande/PB, Cascavel/CE, Carapicuíba/SP, Eusebio/CE, Fortaleza/CE, Ingá/PB, Nova Iguaçu/RJ, Pacatuba/CE, São Gonçalo do Amarante/CE, São José dos Campos/SP, Sinop/MT. Seven municipalities are located in the Northeast, Brazil’s poorest region. Among those, five are small cities, with populations ranging from 17,600 to 94,000 inhabitants and HDI ranging from 0.592 to 0.788. One of these municipalities is medium-sized with a population of 402,000 inhabitants and an HDI of 0.720, while the other is a major city with 2.6 million inhabitants and an HDI of 0.754.
The other five municipalities are located in the southern and central-western regions of the country, are more urban, and have populations ranging from 146,000 to 823,000 inhabitants, with HDI ranging from 0.749 to 0.807.
References
Degenhardt L, Stockings E, Patton G, Hall WD, Lynskey M. The increasing global health priority of substance use in young people. Lancet Psychiatry. 2016;3:251–64. https://doi.org/10.1016/S2215-0366(15)00508-8.
Gore FM, Bloem PJ, Patton GC, Ferguson J, Joseph V, Coffey C, et al. Global burden of disease in young people aged 10–24 years: a systematic analysis. Lancet. 2011;377:2093–102. https://doi.org/10.1016/S0140-6736(11)60512-6.
Instituto Brasileiro de Geografia e Estatística - IBGE [Internet]. Pesquisa Nacional de Saúde do Escolar PeNSE 2019, Manual de Instrução. Brasília;2019. https://biblioteca.ibge.gov.br/biblioteca-catalogo.html?id=55618&view=detalhes
Hall WD, Patton G, Stockings E, Weier M, Lynskey M, Morley KI, et al. Why young people’s substance use matters for global health. Lancet Psychiatry. 2016;3:265–79. https://doi.org/10.1016/S2215-0366(16)00013-4.
Ladis BA, Macgowan M, Thomlison B, Fava NM, Huang H, Trucco EM, et al. Parent-focused preventive interventions for Youth Substance Use and Problem behaviors: a systematic review. Res Social Work Pract. 2019;29:420–42. https://doi.org/10.1177/1049731517753686.
United Nations Office on Drugs and Crime - UNODC [Internet]. International Standards on Drug Use Prevention - Second updated edition. United Nations Office on Drugs and Crime and the World Health Organization. 2018. Available from: from http://www.unodc.org/documents/prevention/standards_180412.pdf.
Kumpfer KL, Magalhães C. Strengthening families program: an evidence-based family intervention for parents of high-risk children and adolescents. J Child Adolesc Subst Abuse. 2018;27:174–9. https://doi.org/10.1080/1067828X.2018.1443048.
EPISCenter [Internet]. The Evidence based Prevention and Intervention Center, Logic Model Created by the Evidence-based Prevention & Intervention Support Center. Penn State University. 2021. http://episcenter.psu.edu/sites/default/files/13-06-10%2520Full%2520SFP%252010-14%2520Logic%25%0A20Model.pdf.
Bowen M. Alcoholism as viewed through family systems theory and family psychotherapy. Ann N Y Acad Sci. 1974;233:115–22. https://doi.org/10.1111/j.1749-6632.1974.tb40288.x.
Bandura A. Social Cognitive Theory: an agentic perspective. Annu Rev Psychol. 2001;52:1–26. https://doi.org/10.1146/annurev.psych.52.1.1.
Kumpfer KL, Olds DL, Alexander JF, Zucker RA, Gary LE. Family Etiology of Youth. Drug abuse prevention through family interventions 1999, 177, 42-77 https://archives.nida.nih.gov/sites/default/files/042-077_Kumpfer.pdf.
Forgatch MS, Kjøbli J. Parent management training—oregon model: adapting intervention with Rigorous Research. Fam Process. 2016;55:500–13. https://doi.org/10.1111/famp.12224.
Spoth R, Redmond C, Shin C, Azevedo K. Brief family intervention effects on adolescent substance initiation: school-level growth curve analyses 6 years following baseline. J Consult Clin Psychol. 2004;72:535–42. https://doi.org/10.1037/0022-006X.72.3.535.
Spoth R, Guyll M, Shin C. Universal Intervention as a Protective Shield against exposure to Substance Use: long-term outcomes and Public Health significance. Am J Public Health. 2009;99:2026–33. https://doi.org/10.2105/AJPH.2007.133298.
Baldus C, Thomsen M, Sack P-M, Bröning S, Arnaud N, Daubmann A, et al. Evaluation of a German version of the strengthening families Programme 10–14: a randomised controlled trial. Eur J Public Health. 2016;26:953–9. https://doi.org/10.1093/eurpub/ckw082.
Gorman DM. The decline effect in evaluations of the impact of the strengthening families Program for Youth 10–14 (SFP 10–14) on adolescent substance use. Child Youth Serv Rev. 2017;81:29–39. https://doi.org/10.1016/j.childyouth.2017.07.009.
Carballo JL, García-rodríguez O, FAMILY-BASED DRUG, USE PREVENTIOn - THE FAMILIAS QUE FUNCIONAN PROGRAM. PSYCHOLOGY IN SPAIN 2010 14(1), 1–7. https://www.psychologyinspain.com/content/full/2010/14001.pdf.
Skarstrand E, Sundell K, Andreasson S. Evaluation of a Swedish version of the strengthening families Programme. Eur J Public Health. 2014;24:578–84. https://doi.org/10.1093/eurpub/ckt146.
Foxcroft DR, Callen H, Davies EL, Okulicz-Kozaryn K. Effectiveness of the strengthening families programme 10–14 in Poland: cluster randomized controlled trial. Eur J Public Health 2016:ckw195. https://doi.org/10.1093/eurpub/ckw195.
Segrott J, Gillespie D, Lau M, Holliday J, Murphy S, Foxcroft D, et al. Effectiveness of the Strengthening Families Programme in the UK at preventing substance misuse in 10–14 year-olds: a pragmatic randomised controlled trial. BMJ Open. 2022;12:e049647. https://doi.org/10.1136/bmjopen-2021-049647.
Riesch SK, Brown RL, Anderson LS, Wang K, Canty-Mitchell J, Johnson DL. Strengthening families Program (10–14): effects on the Family Environment. West J Nurs Res. 2012;34:340–76. https://doi.org/10.1177/0193945911399108.
Spoth RL, Redmond C, Shin C. Reducing adolescents’ aggressive and hostile behaviors: Randomized Trial effects of a brief family intervention 4 years past baseline. Arch Pediatr Adolesc Med. 2000;154:1248. https://doi.org/10.1001/archpedi.154.12.1248.
Sánchez-Prieto L, Orte C, Ballester L, Amer J. Can better parenting be achieved through short prevention programs? The challenge of universal prevention through strengthening families Program 11–14. Child Family Social Work. 2020;25:515–25. https://doi.org/10.1111/cfs.12717.
Corea VML, Zubarew GT, Valenzuela MMT, Salas PF. Evaluación Del programa Familias fuertes: amor y límites en familias con adolescentes de 10 a 14 años. Rev Méd Chile. 2012;140:726–31. https://doi.org/10.4067/S0034-98872012000600005.
Semeniuk Y, Brown RL, Riesch SK, Zywicki M, Hopper J, Henriques JB. The strengthening families Program 10–14: influence on parent and youth problem-solving skill: parent youth problem solving. J Psychiatr Ment Health Nurs. 2009;17:392–402. https://doi.org/10.1111/j.1365-2850.2009.01534.x.
Allen D, Coombes L, Foxcroft DR. Cultural accommodation of the Strengthening Families Programme 10–14: UK Phase I study. Health Educ Res. 2006;22:547–60. https://doi.org/10.1093/her/cyl122.
Murta SG, De Almeida Nobre-Sandoval L, De Souza Pedralho M, Tavares TNG, Ramos CEPL, Allen D, et al. Needs assessment for cultural adaptation of strengthening families program (SFP 10-14-UK) in Brazil. Psicol Refl Crít. 2018;31:25. https://doi.org/10.1186/s41155-018-0105-0.
Rocha VPS, Aló CM, Damasceno MRV, Borges JM, Pedralho M, Seidl J, Morais CA. De SFP a PFF: adaptação de um programa de prevenção ao uso de drogas para famílias brasileiras no contexto da saúde e do serviço social. In. Prevenção ao uso de drogas: implantação e avaliação de programas no Brasil (pp. 203–221). 2018, Ministério da Saúde. https://www.researchgate.net/publication/329403844_De_SFP_a_PFF_Adaptacao_de_um_Programa_de_Prevencao_ao_Uso_de_Drogas_para_Familias_Brasileiras_no_Contexto_da_Saude_e_do_Servico_Social.
Murta SG, Vinha LGDA, Nobre-Sandoval LDA, Miranda AAV, Menezes JCLD, Rocha VPS. Feasibility of the strengthening families program for Brazilian families: a mixed method study. Psic: Teor E Pesq. 2020;36. https://doi.org/10.1590/0102.3772e36nspe16. e36nspe16.
Resnicow K, Soler R, Braithwaite RL, Ahluwalia JS, Butler J. Cultural sensitivity in substance use prevention. J Community Psychol. 2000;28:271–90. https://onlinelibrary.wiley.com/doi/10.1002/(SICI)1520-6629(200005)28:3%3C271::AID-JCOP4%3E3.0.CO;2-I.
Sanchez ZM, Valente JY, Galvão PP, Gubert FA, Melo MHS, Caetano SC, et al. A cluster randomized controlled trial evaluating the effectiveness of the school-based drug prevention program #Tamojunto2.0. Addiction. 2021;116:1580–92. https://doi.org/10.1111/add.15358.
Valente JY, Cogo-Moreira H, Sanchez ZM. Applying a pattern-centered Approach to assess the Effect of a School-Based Drug Use Prevention Program in Brazil: a Cluster Randomized Controlled Trial. J Prim Prevent. 2022;43:529–48. https://doi.org/10.1007/s10935-022-00681-4.
Murta SG, De Almeida Nobre-Sandoval L, Rocha VPS, Miranda AAV, Duailibe KD, Farias DA, et al. Social Validity of the Strengthening Families Program in Northeastern Brazil: the voices of parents, adolescents, and facilitators. Prev Sci. 2021;22:658–69. https://doi.org/10.1007/s11121-020-01173-9.
Murta SG, Vinha LGDA, Nobre-Sandoval LDA, Rocha VPS, Duailibe KD, Gomes MDSM, et al. Exploring the short-term effects of the strengthening families program on Brazilian adolescents: a pre-experimental study. Drugs: Educ Prev Policy. 2021;28:267–77. https://doi.org/10.1080/09687637.2020.1769030.
Molgaard V, Spoth R. The strengthening families Program for Young adolescents: overview and outcomes. Residential Treat Child Youth. 2001;18:15–29. https://doi.org/10.1300/J007v18n03_03.
Sanchez ZM, Valente JY, Sanudo A, Pereira APD, Cruz JI, Schneider D, et al. The #Tamojunto Drug Prevention Program in Brazilian schools: a Randomized Controlled Trial. Prev Sci. 2017;18:772–82. https://doi.org/10.1007/s11121-017-0770-8.
Galvão PPDO, Valente JY, Millon JN, Melo MHS, Caetano SC, Cogo-Moreira H, et al. Validation of a Tool to evaluate drug Prevention Programs among students. Front Psychol. 2021;12:678091. https://doi.org/10.3389/fpsyg.2021.678091.
Carlini EA, Noto A, Sanchez ZM, Carlini CA, Locatelli D, Abeid L, Amato T, Opaley E, Tondowski C, Moura Y. (2010). VI Levantamento nacional sobre o consumo de drogas psicotrópicas entre estudantes do ensino fundamental e médio das redes pública e privada de ensino nas 27 capitais brasileiras. (1st ed.). Universidade Federal de São Paulo 2010. https://www.mds.gov.br/webarquivos/obid/publica%C3%A7%C3%B5es/VI%20Levantamento%20Nacional%20sobre%20o%20Consumo%20de%20Drogas%20Psicotr%C3%B3picas%20entre%20Estudantes%20do%20Ensino%20Fundamental%20e%20M%C3%A9dio%20das%20Redes%20P%C3%BAblica%20e%20Privada%20de%20Ensino%20nas%2027%20Capitais%20Brasileiras.pdf.
Substance Abuse and Mental Health Services Administration– SAMHSA [Internet]. National Minority AIDS Initiative (MAI). Substance Abuse/HIV Prevention Initiative Youth Questionnaire. In National Minority Substance Abuse, HIV and Hepatitis Prevention Initiatives Tool. USA, 2006. https://www.samhsa.gov/sites/default/files/maimrt-new-youth-questionnaire.pdf.
Sadowski LS, Hunter WM, Bangdiwala SI, Muñoz SR. The world studies of abuse in the family environment (WorldSAFE): a model of a multi-national study of family violence. Injury Control Saf Promotion. 2004;11:81–90. https://doi.org/10.1080/15660970412331292306.
Bordin IA, Paula CS. Brazilian brief version of the Questionnaire WorldSAFE. Brasil, 2013.
Lamborn SD, Mounts NS, Steinberg L, Dornbusch SM. Patterns of competence and Adjustment among adolescents from authoritative, authoritarian, indulgent, and neglectful families. Child Dev. 1991;62:1049. https://doi.org/10.2307/1131151.
Costa FTD, Teixeira MAP, Gomes WB. Responsividade E exigência: duas escalas para avaliar estilos parentais. Psicol Reflex Crit. 2000;13:465–73. https://doi.org/10.1590/S0102-79722000000300014.
Calafat A, García F, Juan M, Becoña E, Fernández-Hermida JR. Which parenting style is more protective against adolescent substance use? Evidence within the European context. Drug Alcohol Depend. 2014;138:185–92. https://doi.org/10.1016/j.drugalcdep.2014.02.705.
Valente JY, Cogo-Moreira H, Sanchez ZM. Evaluating the effects of parenting styles dimensions on adolescent drug use: secondary analysis of #Tamojunto randomized controlled trial. Eur Child Adolesc Psychiatry. 2020;29:979–87. https://doi.org/10.1007/s00787-019-01410-9.
Associação Brasileira de empresas de pesquisa - ABEP. [Internet]. Critério Brasil 2019. In ABEP - Associação Brasileira Econômica de Pesquisa (pp. 1–6). São Paulo. 2019. http://www.abep.org/criterio-brasil.
Detry MA, Ma Y. Analyzing repeated measurements using mixed models. JAMA. 2016;315:407. https://doi.org/10.1001/jama.2015.19394.
Carpenter JR, Kenward MG. Missing data in randomised controlled trials: a practical guide. Birmingham: Health Technology Assessment Methodology Programme; 2007. https://researchonline.lshtm.ac.uk/id/eprint/4018500.
Maccoby EE. The role of parents in the socialization of children: an historical overview. Dev Psychol. 1992;28:1006–17. https://doi.org/10.1037/0012-1649.28.6.1006.
Valente JY, Cogo-Moreira H, Sanchez ZM. Predicting latent classes of drug use among adolescents through parental alcohol use and parental style: a longitudinal study. Soc Psychiatry Psychiatr Epidemiol. 2019;54:455–67. https://doi.org/10.1007/s00127-018-1645-4.
Castaño Pérez G, Salas C, Buitrago C. Evaluation of the Prevention Program: strong families: love and limits in Colombia. Int J Ment Health Addict. 2020;18:459–70. https://doi.org/10.1007/s11469-019-00218-7.
Cuartas J, McCoy DC, Rey-Guerra C, Britto PR, Beatriz E, Salhi C. Early childhood exposure to non-violent discipline and physical and psychological aggression in low- and middle-income countries: National, regional, and global prevalence estimates. Child Abuse Negl. 2019;92:93–105. https://doi.org/10.1016/j.chiabu.2019.03.021.
Bowden JA, Delfabbro P, Room R, Miller CL, Wilson C. Levels of parental drinking in the Presence of children: an exploration of attitudinal correlates. Alcohol Alcohol. 2022;57:460–9. https://doi.org/10.1093/alcalc/agab071.
Conegundes LSO, Valente JY, Martins CB, Andreoni S, Sanchez ZM. Binge drinking and frequent or heavy drinking among adolescents: prevalence and associated factors. Jornal De Pediatria. 2020;96:193–201. https://doi.org/10.1016/j.jped.2018.08.005.
Willhelm AR, Cabral JCC, Steiger JO, Silva JFFD, Ugarte LM, Almeida RMMD. Consumo De Álcool na Adolescência E Relação com Uso Excessivo De Bebidas Alcóolicas dos Pais: Estudantes De Quatro Escolas De Porto Alegre. Psico. 2015;46:208. https://doi.org/10.15448/1980-8623.2015.2.18129.
Pinheiro-Carozzo NP, Murta SG, Vinha LGDA, Da Silva IM, Fontaine AMGV. Beyond effectiveness of the strengthening families Program (10–14): a scoping RE-AIM-based review. Psicol Refl Crít. 2021;34:16. https://doi.org/10.1186/s41155-021-00182-z.
Mejía A, Bertello L, Gil J, Griffith J, López AI, Moreno M, et al. Evaluation of Family Skills Training Programs to Prevent Alcohol and Drug Use: a critical review of the Field in Latin America. Int J Ment Health Addict. 2020;18:482–99. https://doi.org/10.1007/s11469-019-00060-x.
Acknowledgements
All SARCs and families who participated in this study.
Funding
This study was supported by the Ministry of Women, Family and Human Rights (MMFDH) through grant no. TED 02/2020.
Author information
Authors and Affiliations
Contributions
Dr Zila Sanchez conceptualized, and designed the study, and was responsible for the grant acquisition and wrote the final version of the manuscript. Dr Juliana Valente and Dr Hugo-Cogo conducted and interpreted the data analyses. Dr Patricia Galvao and Dr Juliana Valente drafted the initial manuscript. Dr Lidiane Reboucas, Dr. Fabiane Gurbert and MSc. Miguel Henrique Santos reviewed and revised the manuscript. Dra Sheila and Dra Marcia Melo were co-responsible for study design, instrument development and critical review. All authors approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was registered in the Brazilian Ministry of Health Register of Clinical Trials (REBEC), under protocol no. RBR-5hz9g6z (https://ensaiosclinicos.gov.br/rg/RBR-5hz9g6z).
Consent for publication
Authors declare that they have no conflict of interest.
Competing interests
The authors declare no competing interests.
Informed consent
All procedures in the study followed the institutional norms and ethical standards of the Brazilian national research committee, and the 1964 Declaration of Helsinki and further amendments. Parents and legal guardians completed Informed Consent Forms and adolescents completed Informed Assent Forms stating their agreement in participating in the study.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Sanchez, Z.M., Valente, J.Y., Gubert, F.A. et al. Short-term effects of the strengthening families Program (SFP 10–14) in Brazil: a cluster randomized controlled trial. Child Adolesc Psychiatry Ment Health 18, 64 (2024). https://doi.org/10.1186/s13034-024-00748-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13034-024-00748-6