
Abstract
Background
Threatening and hostile interpretation biases are seen as causal and maintaining mechanisms of childhood anxiety and aggression, respectively. However, it is unclear whether these interpretation biases are specific to distinct problems or whether they are general psychopathological phenomena. The specificity versus pervasiveness of interpretation biases could also differ depending on mental health status. Therefore, in the current study, we investigated whether social anxiety and callous-unemotional (CU) traits were uniquely related to threatening and hostile interpretation biases, respectively, in both a community and a clinical sample of adolescents.
Methods
A total of 161 adolescents between 10 to 15 years of age participated. The community sample consisted of 88 participants and the clinical sample consisted of 73 inpatients with a variety of psychological disorders. Social anxiety and CU-traits were assessed with self-report questionnaires. The Ambiguous Social Scenario Task was used to measure both threatening and hostile interpretations in response to written vignettes.
Results
Results showed that social anxiety was uniquely related to more threatening interpretations, while CU-traits were uniquely related to more hostile interpretations. These relationships were replicated for the community sample. For the clinical sample, only the link between social anxiety and threatening interpretations was significant. Explorative analyses showed that adolescents with externalizing disorders scored higher on hostile interpretations than adolescents with internalizing disorders.
Conclusions
Overall, these results support the content-specificity of threatening interpretation biases in social anxiety and of hostile interpretation biases in CU-traits. Better understanding the roles of interpretation biases in different psychopathologies might open avenues for tailored prevention and intervention paradigms.
Similar content being viewed by others


Many theories stress the role of interpretation biases, i.e. systematic distortions in the interpretation of environmental cues, in problematic behavior and psychopathology throughout childhood and adolescence [1,2,3]. Negative, threatening interpretations have mostly been linked to internalizing problems, such as depression and anxiety (for review, see [4,5,6]), whereas hostile interpretations have mostly been linked to externalizing problems, such as aggression and conduct problems (for review, see [7,8,9]). However, some studies found that children with elevated anxiety levels also show hostile interpretations [10, 11], and that aggressive children also show threatening interpretations [12]. These seemingly contrasting findings raise the question of whether interpretation biases are specific to particular problems or disorders (i.e. content-specificity hypothesis; [13, 14]), or whether they are general and a commonality between anxiety and aggression [15,16,17]. The specificity versus generalizability of interpretation biases could also depend on an individual’s mental health status and the presence of psychopathology [5]. To better understand the occurrences of interpretation biases and their role in the development of psychopathology, it is necessary to investigate their link to both internalizing and externalizing problems in samples with varying levels of psychopathology. Therefore, the present study investigates whether threatening and hostile interpretation biases of identical social situations are specific to self-reported social anxiety and callous-unemotional (CU) traits in a clinical and a community sample of children.
Social anxiety and CU-traits are relevant concepts in internalizing and externalizing problems, respectively, and they are common in community samples [18, 19]. Social anxiety is characterized by high fear in and the avoidance of social situations in which devaluation by others is possible [20]. CU-traits are characterized by the lack of guilt and remorse, flat affect and disinterest in important activities such as school and social relationships [21, 22]. Increased levels of social anxiety and CU-traits are seen as normative during adolescence [23,24,25]. However, social anxiety disorder typically develops during adolescence [26], which increases the risk on comorbid depression, other anxiety disorders and substance abuse [20]. Furthermore, CU-traits in adolescence are related to severe, persistent aggressive behavior, as well as a higher risk on the development of antisocial personality disorder and psychopathy later in life [27]. Causal and maintaining mechanisms of social anxiety and aggressive behavior are threatening [3, 28, 29] and hostile interpretation biases [1, 7, 8, 30, 31], respectively. Yet, there are some open questions regarding the link between interpretation biases and both social anxiety and CU-traits in adolescence.
The content-specificity of threatening interpretation bias has generally been supported for social anxiety (for reviews, see [4, 5]). For instance, while children with higher levels of social anxiety interpret social scenarios as the most threatening, children with higher levels of separation anxiety interpret separation scenarios as the most threatening ([32, 33]; for contrasting findings, see [34]). Furthermore, in both clinical and community samples the strength of threatening interpretation bias has been found to increase as the severity of social anxiety increases [33, 35,36,37,38,39]. However, only a few studies compared clinical to subclinical or non-clinical samples (for research that did so, see 33, 39). As a consequence, a meta-analysis concluded that the content-specificity of interpretation biases in childhood anxiety could be supported for different samples separately, but not across different samples [5]. To further support the content-specificity of interpretation biases, not only different samples but also different interpretations should be compared.
Research on interpretation biases in CU-traits examined different interpretation biases but the findings are inconsistent. Hostile interpretation bias has been found to be higher [40] or lower [41] as a function of CU-traits in community samples. Other studies did not find any link between CU-traits and hostile interpretation bias, neither in community nor in clinical samples [42, 43]. Threatening interpretation bias has been found to be increased in delinquent adolescents with higher levels of CU-traits [44]. Given the high comorbidity of internalizing and externalizing problems [45], controlling for both sort of problems might help to disentangle the relationships between CU-traits and interpretation biases.
The assessment of threatening and hostile interpretation biases together has shown support for content-specific interpretation biases in relation to social anxiety and CU-traits, respectively. The Ambiguous Social Scenario Task (ASST) is a newly developed task that measures both threatening and hostile interpretations in response to the same situations [46]. In a clinical sample of adolescent inpatients, self-reported social anxiety was uniquely related to threatening interpretations, and CU-traits were uniquely related to hostile interpretations [47]. By investigating whether these relationships express themselves similarly in different samples, the role of interpretation biases in different problems might be better understood.
The goal of the current study was to examine whether threatening and hostile interpretation biases are specific to social anxiety and CU-traits, respectively, in both a clinical and a community sample of adolescents. In line with the content-specificity of interpretation biases, we expected that higher levels of social anxiety were related to more threatening interpretations (e.g. [33]), and that higher levels of CU-traits were related to more hostile interpretations [47]. General, pervasive interpretation biases would be supported when social anxiety would be related to more hostile interpretations and when CU-traits were related to more threatening interpretations. We expected that the clinical sample, compared to the community sample, would score higher on both interpretation biases (as has already been shown for threatening interpretations; [33]), but we did not expect that the link between social anxiety, CU-traits and interpretation biases would differ between samples.
Method
Participants
For the current study, an existing clinical sample (fully described in 47) was matched to a newly recruited community sample. The existing clinical sample consisted of 401 participants (253 girls) between 10 and 20 years of age (M = 14.66, SD = 1.94). The three most common primary diagnoses based on the 10th version of the International Classification of Diseases (ICD-10) were major depressive disorder (F32.-; n = 33; 45%), mixed disorder of conduct and emotion (F92.-; n = 25; 34%), and other emotional disorders (F93.-; n = 5; 9%). The newly recruited community sample consisted of 116 children and adolescents (76 girls) between 7 and 15 years of age (M = 11.09, SD = 1.93).
We randomly matched the number of boys and girls per age from the clinical sample with the number of boys and girls per age of the community sample by using the function sample of the R base package [48]. Since number of boys and girls was not always equally represented, the size and gender distribution differed for the two newly created samples. That is, the clinical sample consisted of 73 participants (44 girls) and the community sample consisted of 88 participants (58 girls). Both samples were between 10 and 15 years of age with a mean age of 12 years. The sample characteristics are shown in Table 1.
Measurements
Ambiguous Social Scenario Task (ASST—youth version; [46])
The ASST—youth version assesses hostile, threatening and neutral interpretations of ambiguous social situations. Participants have to indicate for 10 social scenarios how likely a threatening, a hostile and a neutral interpretation would come to their minds. An example situation is ‘You asked a question in a WhatsApp group. After a while you see that everyone read your message but no one responded.' The three interpretations given read 1) ‘Probably they find my question stupid and annoying.’ (threatening), 2) ‘People are lazy. I won’t answer their questions anymore, either.’ (hostile) and 3) ‘Probably everyone is busy and doesn’t have time to answer.’ (neutral). Answers are given for each interpretation on a visual analogue scale ranging from 0% (‘very unlikely’) to 100% (‘very likely’). For the analyses, mean scores for each interpretation category are used. The current internal consistencies were good for threatening interpretations (clinical sample: α = 0.83, community sample: α = 0.80), and acceptable for both hostile (clinical sample: α = 0.75, community sample: α = 0.71) and neutral interpretations (clinical sample: α = 0.73, community sample: α = 0.74).
Spence children’s anxiety scale (SCAS-D; [49])
The SCAS-D measures self-reported anxiety using six subscales that assess symptoms of social anxiety, panic disorder, agoraphobia, generalized anxiety disorder, obsessive–compulsive disorder, separation anxiety disorder, and specific phobia. Participants answer 38 items, such as ‘I feel afraid that I will make a fool of myself in front of people.‘ (social anxiety subscale), on a 4-point Likert scale ranging from 0 (‘never’) to 3 (‘always’). The social anxiety subscale consists of 6 items. For girls and boys, scores higher than 9 and 7, respectively, are considered as clinically-relevant (based on the cutoff scores published online; https://www.scaswebsite.com). The social anxiety subscale had an excellent internal consistency in the current study (clinical sample: α = 0.88, community sample: α = 0.77).
Inventory of callous-unemotional traits (ICU; [50])
The ICU assesses callous-unemotional (CU) traits in terms of three subscales, namely callousness (e.g., ‘I do not care who I hurt to get what I want’), uncaring (e.g., ‘I care about how well I do at school’, reversed score) and unemotional (e.g., ‘I do not show my emotions to others’). Participants rate 24 items on a 4-point Likert scale ranging from 0 (‘not at all true’) to 3 (‘definitely true’). Scores higher than 30 and 35 indicate at-risk for girls and boys, respectively (based on the cutoff scores published online; https://faculty.lsu.edu/pfricklab/icu.php). In the current study, the total ICU score had an acceptable internal consistency in the clinical sample (α = 0.74) and a slightly lower internal consistency in the community sample (α = 0.67). The internal consistencies of both the callousness and the uncaring subscales were in a similar range (clinical sample: α = 0.67 and 72, community sample: α = 0.57 and 60). However, the internal consistency of the unemotional subscale was low (clinical sample: α = 0.25, community sample: α = 0.27).
Procedure
The community sample was recruited in German elementary and high schools. The schools distributed information about the study among parents. When parents indicated their interest in letting their children participate, they received a digital information letter and were asked for digital consent. After agreeing to their child’s participation, a link to the questionnaires was sent. Information letter, informed consent and questionnaires were provided by using the Qualtrics online platform [51]. It was stressed that children should fill in the questionnaires on their own by using a computer and by sitting in a quiet environment. Filling in the questionnaires took about 20 min. Participation was rewarded with a 5€ voucher. The ethical committee of the Faculty of Social Sciences had no formal objection to the study (ECSW-2020-154).
Data from the clinical sample were gathered as part of the diagnostic routine of an inpatient clinic within a predefined period of 6 months (for details see [47]). Informed consent was obtained from the patients’ legal guardians. The adolescents were verbally informed about the study and were given the possibility to refrain from participation. The whole diagnostic routine took approximately 1 h. The clinical sample did not receive a compensation for their participation. The local medical-ethical committee approved the use of the data (No.: 4359–12).
Statistical approach
The main research questions, whether threatening and hostile interpretation biases are content-specific to social anxiety and CU-traits, respectively, and whether these links differ between a clinical and a community sample were examined by using multivariate multiple regression followed-up by univariate multiple regression. The relationships between all variables of interest were furthermore investigated by performing Pearson’s correlations and t-tests.
The freely available software R (version 4.0.3; [48]) and RStudio (RStudio 2022.02.3; [52]) were used for data preparation and analyses. The function lm of the stats package (version 4.0.3; [48]) was used to conduct both multivariate and univariate multiple regression. For multivariate multiple regression, both threatening and hostile interpretations were entered as outcome. Social anxiety, CU-traits, sample, as well as the two-way interactions between social anxiety and sample and between CU-traits and sample were entered as predictors. Univariate regression analyses were used to further interpret the results with only one interpretation bias at a time as outcome. Continuous predictors were standardized to align their scales. The correlations between all measurement were computed per sample by using the function corr.test of the package psych (version 2.0.12; [53]). Holm adjustment was used to control for multiple testing. The differences between the samples were further examined by performing t-tests using the function t.test of the stats package (version 4.0.3; [48]).
Transparency statement
The current study has been pre-registered on osf.io (https://osf.io/jermg). Different to what was pre-registered, we used multivariate regression instead of the pre-registered Structural Equation Model (SEM). For SEM, a minimum of 300 participants is generally recommended [54]. Unfortunately, we did not achieve this sample size since the corona pandemic hindered our data collection resulting in time constraints. With a final sample size of 161 participants, five predictors and p = 0.05, we had an excellent power (1 − ß = 0.98) to detect effects of medium size (f2 = 0.15) with regression analyses. Therefore, we decided to analyze our principal research question with multivariate regression.
Results
The role of social anxiety, CU-traits and sample on both interpretation biases
Multivariate multiple regression analysis indicated significant main effects for both CU-traits, V = 0.08, F(2, 150) = 6.03, p = 0.003, and social anxiety, V = 0.15, F(2, 150) = 13.37, p < 0.001, on threatening and hostile interpretations together. The effect of sample was not significant. This indicates that both CU-traits and social anxiety play a role on interpretation biases. Next, we inspected the results of the univariate regression analyses for hostile and threatening interpretations separately.
The role of social anxiety, CU-traits and sample on threatening interpretations
The univariate multiple regression for threatening interpretations was significant F(5, 151) = 21.33, p < 0.001 with the predictors explaining 39.46% of the variance, 95% bootstrapped CI [30.60, 51.63]. A significant main effect of sample was found (β = 0.15, p = 0.02). A follow-up t-test showed that the clinical sample scored higher on both social anxiety, t(159) = -3.92, p < 0.001, and threatening interpretations than the community sample, t(159) = -4.04, p < 0.001 (see Table 1). Furthermore, a significant main effect for social anxiety on threatening interpretations was found (β = 0.60, p < 0.001). Pearson’s correlations indicated that higher levels of social anxiety were related to more threatening interpretations in both the clinical (r = 0.64) and the community sample (r = 0.44, both p’s < 0.001; see Table 2).
The role of social anxiety, CU-traits and sample on hostile interpretations
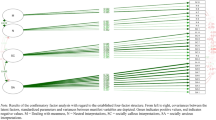
The univariate model for hostile interpretations was significant F(5, 151) = 4.42, p < 0.001 with the predictors explaining 9.87% of the variance, 95% bootstrapped CI [5.22, 20.42]. A significant interaction effect for social anxiety and sample on hostile interpretations was found (β = − 0.31, p = 0.03). Higher levels of social anxiety were related to more hostile interpretations in the community sample, but they were related to less hostile interpretations in the clinical sample (see Fig. 1). The correlations between social anxiety and hostile interpretations for each sample separately were not significant, though (see Table 2).

Significant interaction effect between social anxiety and sample on hostile interpretation bias
Furthermore, the results showed a significant main effect for CU-traits on hostile interpretations (β = 0.36, p < 0.001). For consistency, we also conducted t-tests for sample differences and Pearson’s correlation for each sample separately. Neither CU-traits nor hostile interpretations differed between the samples (both p’s > 0.05, see Table 1). Only for the community sample, a significant positive correlation between CU-traits and hostile interpretations was found (r = 0.37, p < 0.01). In the clinical sample, the relationship was positive but not significant (r = 0.22, p = 0.46; see Table 2).
Exploring internalizing and externalizing diagnoses to differentiate interpretation biases
Given the unexpected finding that hostile interpretations were not related to CU-traits in the clinical sample, we explored whether grouping participants into externalizing and internalizing disorders would relate to hostile and threatening interpretation biases, respectively. The externalizing group consisted of 33 patients (10 girls). Most of them had a subtype of conduct disorders as main diagnosis (F90.1, F91.2, F92.0 and F92.8); Other diagnoses were addiction and attachment disorders (F12.2, F94.1 and F94.2). The internalizing group consisted of 39 patients (33 girls) including the main diagnoses depressive disorder (F32.,-), somatization disorder (F45.0) and other childhood emotional disorder (F93.8). One patient with the diagnosis atypical anorexia nervosa (F50.1) was not classified as internalizing or externalizing.
A 2 (externalizing disorders, internalizing disorders) group × 3 (hostile, threatening, neutral) interpretation repeated measures ANOVA on strength of interpretation yielded a significant main effect of interpretation, F(1.82, 127.7) = 13.2, p < 0.001, as well as a significant interaction effect for group and content of interpretation, F(1.82, 127.7) = 12.9, p < 0.001, on strength of interpretation bias. Follow-up t-tests for the interaction effect showed that threatening interpretations were higher in the internalizing group t(70) = − 3.23, p < 0.01, whereas hostile interpretations were higher in the externalizing group, t(70) = 2.15, p < 0.05. Furthermore, social anxiety was higher in the internalizing group, t(70) = − 5.29, p < 0.001, while CU-traits did not differ per group (p > 0.05).
Exploring the relationships between interpretation biases
Pearson’s correlations indicated a significant positive correlation between threatening interpretations and hostile interpretations for the community sample (r = 0.51, p < 0.001). This correlation was not significant for the clinical sample (p > 0.05). This indicates that adolescents in the community sample who interpreted ambiguous situations as threatening were more likely to also interpret them as hostile.
Discussion
The current study examined whether threatening and hostile interpretations of the same ambiguous social situations were specific to social anxiety and callous-unemotional (CU) traits, respectively, and whether these relationships differed between a community and a clinical sample of adolescents. Across both samples, social anxiety was uniquely related to threatening interpretations, and CU-traits were uniquely related to hostile interpretations. Both of these relationships hold true for the community sample. However, the relationship between CU-traits and hostile interpretations was not significant for the clinical sample separately. Only adolescents with externalizing disorders scored higher on hostile interpretations. Despite these sample differences, the results overall support the content-specificity of threatening and hostile interpretation biases to social anxiety and CU-traits, respectively.
In line with our hypotheses, we found that adolescents with higher levels of social anxiety made more threatening interpretations of ambiguous situations in both the clinical and the community sample. This finding is in line with other studies that found positive associations between social anxiety and threatening interpretation biases in samples with varying levels of anxiety (e.g. [32, 33, 37, 38]). In both samples threatening interpretations increased as a function of social anxiety, and they were distinct from CU-traits. This suggests that the content-specificity hypothesis applies equally to community and clinical samples, and that threatening interpretations express themselves similarly—if not the same—in subclinical and clinical social anxiety. The only difference between the two samples was quantitative rather than qualitative. Stronger threatening interpretations in adolescents with more severe social anxiety might be explained by a stronger activation of schemas related to danger and one’s own inability to cope [3, 29, 55], as well as by more frequent negative self-statements (e.g. [3, 37]). In addition to that, the link between social anxiety and threatening interpretations is in line with many theories and recent classification systems that cluster mood-related cognitions, affect, physiology and behavior together [20, 56, 57]. Together, these results underline threatening interpretations as underlying mechanism of fear in social situations and the avoidance thereof.
Across both samples, adolescents with higher levels of CU-traits showed more hostile interpretations of ambiguous social situations. Furthermore, CU-traits were not related to threatening interpretations. This finding supports the content-specificity of hostile interpretation bias in CU-traits. However, when testing the samples separately, no significant link between CU-traits and hostile interpretations was found for the clinical sample. Only adolescents with externalizing disorders, as compared to adolescents with internalizing disorders, showed higher levels of hostile interpretation bias. This suggests that CU-traits and their cognitive correlates express themselves differently in community and clinical samples. In line with this explanation, previous research identified some variants of CU-traits which differ in terms of their comorbid problems and physiological reactivities [58, 59]. It is possible that these variants also differ in their cognitive mechanisms and interpretation biases. In line with this idea, the internal reliabilities of the self-reported Inventory of Callous-Unemotional traits (ICU) were low ranging from poor to acceptable. Thus, CU-traits were not a very reliable concept in the current study. In addition to that, the explained variance for the regression model on hostile interpretations was small. In a larger clinical sample, of which the current clinical sample was randomly extracted, we did find a significant link between CU-traits and hostile interpretation bias [47]. Together, this might suggest that the link between CU-traits and hostile interpretation bias is weak, if it exists at all, and that larger sample sizes are necessary to control for the heterogeneity of CU-traits.
Some unexpected findings need to be discussed. First, adolescents of the community sample that interpreted ambiguous social situations as more threatening also interpreted them as more hostile. More research found internalizing and externalizing cognitions to correlate with each other [46, 57, 60, 61]. In response to another person’s ambiguous behavior, it might be healthy to engage in both self-doubt (e.g. s/he doesn’t like me) and other-blame (e.g. s/he is a jerk). In the clinical sample, the different interpretation biases did not significantly relate to each other. This might indicate that with a higher degree of symptomatology, interpretation biases are specific rather than general. Another explanation for the lack of significance might be the smaller sample size of the clinical sample. However, the correlation coefficient was very small (r = 0.05). Therefore, this explanation remains speculative. Second, there was an interaction between social anxiety and sample on hostile interpretations. In the community sample, hostile interpretations appeared to increase as social anxiety increased, whereas in the clinical sample, hostile interpretations appeared to decrease as social anxiety increased. This suggests that healthy adolescents with higher levels of social anxiety sometimes react callously to handle ambiguous situations (similar to the link between anxiety and aggression; [15, 16, 62]), whereas adolescents with mental health problems and higher social anxiety react fearful. Post-hoc correlations between hostile interpretations and social anxiety did not reach significance, though, neither for the community sample, nor for the clinical sample.
Despite several strengths, the current study also has some limitations. Strengths include the comparison of a community and a clinical sample, which allowed us to examine the generalizability of interpretation biases across subclinical and clinical symptomatology. Furthermore, a simultaneous assessment of different interpretations in the same situation is crucial to disentangle (content-specific) interpretation biases. Yet, the current study is only one of a few studies that made use of such a combined approach. Alas, the data were partly collected during the COVID-19 pandemic, which considerably complicated the data collection. Since home schooling and often changing COVID measures were already intense for many teachers, parents and children, little room was left for the participation in research. This led to a smaller sample size for the community sample than anticipated. Although we had enough statistical power to answer our main research questions, the power for exploratory analyses in subsamples was restricted. Future research should examine the role of moderating variables on the link between symptoms and biases with higher sample sizes. Theory-wise it would be interesting for future research to also include measurements on (observable) behavior, such as avoidance and aggression, to investigate how different symptoms and interpretations relate to it.
Conclusions
The current study offers further support for the content-specificity of interpretation biases in social anxiety and partly in CU-traits. By investigating whether interpretation biases are unique to specific symptoms in different samples, the underlying mechanisms of different psychopathologies can be better understood. On the long-term, this knowledge could bear crucial information for the development of tailored versus general prevention and intervention paradigms.
Availability of data and materials
The datasets used and analyzed during the current study, as well as part of the materials can be requested from the first author upon reasonable request.
References
Crick NR, Dodge KA. A review and reformulation of social information-processing mechanisms in children’s social adjustment. Psychol Bull. 1994;115:74–101. https://doi.org/10.1037/0033-2909.115.1.74
Dodge KA. Social-cognitive mechanisms in the development of conduct disorder and depression. Annu Rev Psychol. 1993;44(1):559–84. https://doi.org/10.1146/annurev.ps.44.020193.003015
Kendall PC. Toward a cognitive-behavioral model of child psychopathology and a critique of related interventions. J Abnorm Child Psychol. 1985;13(3):357–72. https://doi.org/10.1007/BF00912722
Stuijfzand S, Creswell C, Field AP, Pearcey S, Dodd H. Research Review: Is anxiety associated with negative interpretations of ambiguity in children and adolescents? A systematic review and meta-analysis. J Child Psychol Psychiatry Allied Discip. 2018;59(11):1127–42. https://doi.org/10.1111/jcpp.12822
Subar AR, Humphrey K, Rozenman M. Is interpretation bias for threat content specific to youth anxiety symptoms/diagnoses? A systematic review and meta-analysis. Eur Child Adolesc Psychiatry. 2021. https://doi.org/10.1007/s00787-021-01740-7.
Platt B, Waters AM, Schulte-Koerne G, Engelmann L, Salemink E. A review of cognitive biases in youth depression: attention, interpretation and memory. Cogn Emot. 2017;31(3):462–83. https://doi.org/10.1080/02699931.2015.1127215.
Martinelli A, Ackermann K, Bernhard A, Freitag CM, Schwenck C. Hostile attribution bias and aggression in children and adolescents: a systematic literature review on the influence of aggression subtype and gender. Aggress Violent Behav. 2018;39(January):25–32. https://doi.org/10.1016/j.avb.2018.01.005
Verhoef REJ, Alsem SC, Verhulp EE, De Castro BO. Hostile intent attribution and aggressive behavior in children revisited: a meta-analysis. Child Dev. 2019;90(5):e525–47. https://doi.org/10.1111/cdev.13255
De Castro BO, Veerman JW, Koops W, Bosch JD, Monshouwer HJ. Hostile attribution of intent and aggressive behavior: a meta-analysis. Child Dev. 2002;73(3):916–34. https://doi.org/10.1111/1467-8624.00447
Bell-Dolan DJ. Social cue interpretation of anxious children. J Clin Child Psychol. 1995;24(1):2–10. https://doi.org/10.1207/s15374424jccp2401_1
Reid SC, Salmon K, Lovibond PF. Cognitive biases in childhood anxiety, depression, and aggression: are they pervasive or specific? Cognit Ther Res. 2006;30(5):531–49. https://doi.org/10.1007/s10608-006-9077-y.
Barrett PM, Rapee RM, Dadds MM, Ryan SM. Family enhancement of cognitive style in anxious and aggressive children. J Abnorm Child Psychol. 1996;24(2):187–203. https://doi.org/10.1007/BF01441484
Beck AT. Cognitive therapy and the emotional disorders. New York: International University Press; 1976.
Beck AT, Haigh EAP. Advances in cognitive theory and therapy: the generic cognitive model. Annu Rev Clin Psychol. 2014;10:1–24. https://doi.org/10.1146/annurev-clinpsy-032813-153734
Andrews LA, Brothers SL, Sauvé JS, Nangle DW, Erdley CA, Hord MK. Fight and flight: examining putative links between social anxiety and youth aggression. Aggress Violent Behav. 2019;48(August):94–103. https://doi.org/10.1016/j.avb.2019.08.005
Kunimatsu MM, Marsee MA. Examining the presence of anxiety in aggressive individuals: the illuminating role of fight-or-flight mechanisms. Child Youth Care Forum. 2012;41(3):247–58. https://doi.org/10.1007/s10566-012-9178-6
Bubier JL, Drabick DAG. Co-occurring anxiety and disruptive behavior disorders: the roles of anxious symptoms, reactive aggression, and shared risk processes. Clin Psychol Rev. 2009;29(7):658–69. https://doi.org/10.1016/j.cpr.2009.08.005
Hare RD, Neumann CS. Psychopathy as a clinical and empirical construct. Annu Rev Clin Psychol. 2008;4(1):217–46. https://doi.org/10.1146/annurev.clinpsy.3.022806.091452
Spence SH, Rapee RM. The etiology of social anxiety disorder: an evidence-based model. Behav Res Ther. 2016;86:50–67. https://doi.org/10.1016/j.brat.2016.06.007.
American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 5th ed. Washington, DC: Author; 2013.
Frick PJ, Ray JV, Thornton LC, Kahn RE. Annual research review: a developmental psychopathology approach to understanding callous-unemotional traits in children and adolescents with serious conduct problems. J Child Psychol Psychiatry. 2014;55(6):532–48. https://doi.org/10.1111/jcpp.12152
Frick PJ, Ray JV, Thornton LC, Kahn RE. Can callous-unemotional traits enhance the understanding, diagnosis, and treatment of serious conduct problems in children and adolescents? A comprehensive review. Psychol Bull. 2014;140(1):1–57. https://doi.org/10.1037/a0033076
Beesdo-Baum K, Knappe S, Fehm L, Höfler M, Lieb R, Hofmann SG, et al. The natural course of social anxiety disorder among adolescents and young adults. Acta Psychiatr Scand. 2012;126(6):411–25. https://doi.org/10.1111/j.1600-0447.2012.01886.x.
Essau CA, Sasagawa S, Frick PJ. Callous-unemotional traits in a community sample of adolescents. Assessment. 2006;13(4):454–69. https://doi.org/10.1177/1073191106287354
Lynam DR, Charnigo R, Mofitt TE, Raine A, Loeber R, Stouthamer-Loeber M. The stability of psychopathy across adolescence. Dev Psychopathol. 2009;21(4):1133–53. https://doi.org/10.1017/S0954579409990083
Beesdo-Baum K, Knappe S. Developmental epidemiology of anxiety disorders. Child Adolesc Psychiatr Clin N Am. 2012;21(3):457–78. https://doi.org/10.1016/j.chc.2012.05.001
MacMahon RJ, Witkiewitz K, Kotler JS, Group TCPPR. Predictive validity of callous-unemotional traits measured in early adolescence with respect to multiple antisocial outcomes. J Abnorm Psychol. 2010;119(4):752–63. https://doi.org/10.1037/a0020796
Muris P, Field AP. Distorted cognition and pathological anxiety in children and adolescents. Cogn Emot. 2008;22(3):395–421. https://doi.org/10.1080/02699930701843450
Daleiden EL, Vasey MW. An information-processing perspective on childhood anxiety. Clin Psychol Rev. 1997;17(4):407–29. https://doi.org/10.1016/s0272-7358(97)00010-x
Crick NR, Dodge KA. Social information-processing mechanisms in reactive and proactive aggression. Child Dev. 1996;67(3):993–1002. https://doi.org/10.1111/j.1467-8624.1996.tb01778.x.
Lemerise EA, Arsenio WF. An integrated model of emotion processes and cognition in social information processing. Child Dev. 2000;71(1):107–18. https://doi.org/10.1111/1467-8624.00124
Mobach L, Rinck M, Becker ES, Hudson JL, Klein AM. Content-specific interpretation bias in children with varying levels of anxiety: the role of gender and age. Child Psychiatry Hum Dev. 2019;50(5):803–14. https://doi.org/10.1007/s10578-019-00883-8.
Klein AM, Rapee RM, Hudson JL, Morris TM, Schneider SC, Schniering CA, et al. Content-specific interpretation biases in clinically anxious children. Behav Res Ther. 2019;121(July):103452. https://doi.org/10.1016/j.brat.2019.103452.
Creswell C, Murray L, Cooper P. Interpretation and expectation in childhood anxiety disorders: age effects and social specificity. J Abnorm Child Psychol. 2014;42(3):453–65. https://doi.org/10.1007/s10802-013-9795-z
Giannini M, Loscalzo Y. Social anxiety and adolescence: Interpretation bias in an Italian Sample. Scand J Psychol. 2016;57(1):65–72. https://doi.org/10.1111/sjop.12263.
Yu M, Westenberg PM, Li W, Wang J, Miers AC. Cultural evidence for interpretation bias as a feature of social anxiety in Chinese adolescents. Anxiety Stress Coping. 2019;32(4):376–86. https://doi.org/10.1080/10615806.2019.1598556.
Miers AC, Blöte AW, Bögels SM, Westenberg PM. Interpretation bias and social anxiety in adolescents. J Anxiety Disord. 2008;22(8):1462–71. https://doi.org/10.1016/j.janxdis.2008.02.010
Higa CK, Daleiden EL. Social anxiety and cognitive biases in non-referred children: the interaction of self-focused attention and threat interpretation biases. J Anxiety Disord. 2008;22(3):441–52. https://doi.org/10.1016/j.janxdis.2007.05.005
Loscalzo Y, Giannini M, Miers AC. Social anxiety and interpretation bias: examining clinical and subclinical components in adolescents. Child Adolesc Ment Health. 2018;23(3):169–76. https://doi.org/10.1111/camh.12221.
Kokkinos CM, Voulgaridou I. Relational victimization, callous-unemotional traits, and hostile attribution bias among preadolescents. J Sch Violence. 2018;17(1):111–22. https://doi.org/10.1080/15388220.2016.1222500.
Frick PJ, Cornell AH, Bodin SD, Dane HE, Barry CT, Loney BR. Callous-unemotional traits and developmental pathways to severe conduct problems. Dev Psychol. 2003;39(2):246–60. https://doi.org/10.1037//0012-1649.39.2.246
Hartmann D, Ueno K, Schwenck C. Attributional and attentional bias in children with conduct problems and callous-unemotional traits: a case–control study. Child Adolesc Psychiatry Ment Health. 2020;14(1):9. https://doi.org/10.1186/s13034-020-00315-9.
Helseth SA, Waschbusch DA, King S, Willoughby MT. Aggression in children with conduct problems and callous-unemotional traits: social information processing and response to peer provocation. J Abnorm Child Psychol. 2015;43(8):1503–14. https://doi.org/10.1007/s10802-015-0027-6
Cima M, Vancleef LMG, Lobbestael J, Meesters C, Korebrits A. Don’t you dare look at me, or else: Negative and aggressive interpretation bias, callous unemotional traits and type of aggression. J Child Adolesc Behav. 2014;2(2):1–9. https://doi.org/10.4172/2375-4494.1000128
Achenbach TM, Ivanova MY, Rescorla LA, Turner LV, Althoff RR. Internalizing/externalizing problems: review and recommendations for clinical and research applications. J Am Acad Child Adolesc Psychiatry. 2016;55(8):647–56. https://doi.org/10.1016/j.jaac.2016.05.012.
Dapprich AL, Lange W-G, Cima M, Becker ES. A validation of an ambiguous social scenario task for socially anxious and socially callous interpretations. Cognit Ther Res. 2022. https://doi.org/10.1007/s10608-021-10283-9.
Dapprich AL, Derks LM, Holtmann M, Lange W-G, Legenbauer T, Becker ES. Hostile and threatening interpretation biases in adolescent inpatients are specific to callous-unemotional traits and social anxiety. submitted.
R Core Team. R: A language and environment for statistical computing [Internet]. Vienna, Austria: R Organisation for Statistical Computing; 2022. https://www.r-project.org/
Spence SH. A measure of anxiety symptoms among children. Behav Res Ther. 1998;36(5):545–66. https://doi.org/10.1016/s0005-7967(98)00034-5
Frick PJ. Inventory of callous-unemotional traits. 2004.
Qualtrics. Provo, Utah, USA; 2020.
RStudio Team. RStudio: integrated development environment for R [Internet]. Boston, MA: RStudio, Inc.; 2022. http://www.rstudio.com/
Revelle W. psych: procedures for personality and psychological research [Internet]. Evanston, Illinois: Northwestern University; 2020. https://cran.r-project.org/package=psych
Tabachnik BG, Fidell LS. Using multivariate statistics. 6th ed. Boston, MA: Pearson; 2013.
Beck AT, Emery G, Greenberg RL. Anxiety disorders and phobias: a cognitive perspective. New York: Basic Books; 1985.
Chorpita BF, Albano AM, Barlow DH. The structure of negative emotions in a clinical sample of children and adolescents. J Abnorm Psychol. 1998;107(1):74–85. https://doi.org/10.1037/0021-843X.107.1.74.
Schniering CA, Rapee RM. The relationship between automatic thoughts and negative emotions in children and adolescents: a test of the cognitive content-specificity hypothesis. J Abnorm Psychol. 2004;113(3):464–70. https://doi.org/10.1037/0021-843X.113.3.464
Cecil CAM, McCrory EJ, Barker ED, Guiney J, Viding E. Characterising youth with callous–unemotional traits and concurrent anxiety: evidence for a high-risk clinical group. Eur Child Adolesc Psychiatry. 2018;27(7):885–98. https://doi.org/10.1007/s00787-017-1086-8.
Fanti KA, Kyranides MN, Petridou M, Demetriou CA, Georgiou G. Neurophysiological markers associated with heterogeneity in conduct problems, callous unemotional traits, and anxiety: comparing children to young adults. Dev Psychol. 2018;54(9):1634–49. https://doi.org/10.1037/dev0000505.
Leung PWL, Wong MMT. Can cognitive distortions differentiate between internalising and externalising problems? J Child Psychol Psychiatry Allied Discip. 1998;39(2):263–9. https://doi.org/10.1017/S0021963097001868
Leung PWL, Poon MWL. Dysfunctional schemas and cognitive distortions in psychopathology: a test of the specificity hypothesis. J Child Psychol Psychiatry Allied Discip. 2001;42(6):755–65. https://doi.org/10.1111/1469-7610.00772
Granic I. The role of anxiety in the development, maintenance, and treatment of childhood aggression. Dev Psychopathol. 2014;26:1515–30. https://doi.org/10.1017/S0954579414001175
Acknowledgements
We kindly thank all adolescents who participated in the current study. Furthermore, we are grateful to the LWL-University Hospital, and in particular to Luisa Lüken, for this collaboration.
Funding
The study was funded by department of Clinical Psychology and the Behavioral Science Institute of Radboud University. These institutions did not play a role in the design of the study, or in the collection and analysis of the data. They were also not involved in the interpretation of the results, or in writing of the manuscript.
Author information
Authors and Affiliations
Contributions
All authors designed the study. The data collection for the clinical samples was supervised by LD and TL. The data collection for the community sample was supervised by AD. AD analyzed the data and wrote a first draft of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The current study was carried out in accordance with the principles of the Declaration of Helsinki. Approval of using the data for the current study was granted by the local medical-ethical committee of the LWL-University Hospital Hamm (No.: 4359-12), as well as by the ethical committee of the Faculty of Social Sciences (ECSW-2020-154). Before the start of the study, informed consent was obtained from the legal guardians of the participants. Verbal informed consent was obtained from the participants.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Dapprich, A.L., Becker, E.S., Derks, L.M. et al. Specific interpretation biases as a function of social anxiety and callous-unemotional traits in a community and a clinical adolescent sample. Child Adolesc Psychiatry Ment Health 17, 46 (2023). https://doi.org/10.1186/s13034-023-00585-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13034-023-00585-z