
Abstract
Background
This study aimed to investigate the association between 25-hydroxyvitamin D (25(OH)D) and depression symptoms among adolescents in Kuwait, a country with a high prevalence of vitamin D deficiency.
Methods
A school based cross-sectional study was conducted on randomly selected 704 adolescents in middle schools. Data on depression symptoms were collected using the Children’s Depression Inventory (CDI). Data on covariates were collected from the parents by self-administered questionnaire and from adolescents by face-to-face interview. Blood samples were analyzed in an accredited laboratory; and 25(OH)D was measured using liquid chromatography-tandem mass spectrometry.
Results
Of 704 adolescents, 94 (13.35%; 95%CI:10.35–17.06%) had depression symptom (a score of 19 or more on the CDI). There was no significant difference in the median CDI score between different vitamin D status (p = 0.366). There was also no significant correlation between serum 25(OH)D concentration and CDI score (Spearman’s rank correlation = 0.01; p = 0.825).There was no significant association between 25(OH)D and depression symptoms whether 25(OH)D was fitted as a continuous variable (crude odds ratio (OR) 0 .99 [95%CI: 0.98, 1.01], p = 0.458 and adjusted OR 1.01 [95%CI: 0.99, 1.02], p = 0.233), categorical variable as per acceptable cut-of points (crude analysis p = 0.376 and adjusted analysis p = 0.736), or categorical variable as quartiles (crude analysis p = 0.760 and adjusted analysis p = 0.549).
Conclusion
Vitamin D status does not seem to be associated with depression symptoms among adolescents in our setting. Nevertheless, it is important to have sufficient vitamin D levels during adolescence for several other health benefits.
Similar content being viewed by others

Introduction
The global burden of disease study demonstrated that depression is a major public health problem and is the leading cause of disability worldwide [1]. Depression affects more than 280 million individuals causing great economic burden not only on the affected individuals but also, on their families, communities, employers, and healthcare services [2]. Furthermore, interventions that aim to prevent or improve the outcome of depression have limited success [3] highlighting the need to expand the knowledge on potential risk factors which might influence the risk and the pathogenesis of depression symptoms. The literature suggests that life style factors such as diet [4, 5] and physical activity are related to depression symptoms [6, 7]. Recently, the link between the deficiency in specific nutritional elements such as vitamin D and depression has come under intense debate.
Vitamin D has a well-established role in calcium and phosphorus homeostasis, bone health and various cellular and neuromuscular functions [8]. But recent literature linked low vitamin D levels to several adverse health outcome such as cancer [9], type 2 diabetes [10], multiple sclerosis [11], autism [12], and asthma [13] as well as all-causes mortality [14]. Recently, low vitamin D levels have been linked to the risk [15] and severity [16] of COVID-19. Vitamin D is derived mainly through exposure to sunlight and the link between depression and the lack of sunlight exposure was first noted two thousand years ago [17]. There are several plausible mechanisms in which vitamin D may affect mental health. Vitamin D can cross the blood–brain barrier [18], hence activate the vitamin D receptors (VDR) which are expressed in brain cells along with vitamin D metabolizing enzymes [19,20,21]. Also, vitamin D is involved in signaling cascades and neurobiological pathways [20] which may affect mental health. The active metabolite of vitamin D is thought to modulate the differentiation and maturation of dopaminergic neurons [22] and to affect brain serotonin concentrations [20, 23]. Finally, it is postulated that depression is associated with increased inflammatory markers [24], while vitamin D has been shown to down-regulate inflammatory markers that have been linked to stress and depression [25]. Despite the evidence that vitamin D may play an important function in the human brain, the exact biological mechanisms linking vitamin D to depression are still not fully understood and remain controversial.
Several observational studies have suggested an association between vitamin D deficiency and major depressive disorders in adults (reviewed by Anglin et al. [26] and Ju et al. [27]). The observational nature of these studies means that it is difficult to ascertain the temporal relationship between vitamin D and depression as some individuals with depression may avoid outdoor activities and have poor diet, resulting in reduced sunlight exposure and consequently reduced endogenous vitamin D synthesis, as well as reduced dietary vitamin D intake [28, 29]. Trials on vitamin D supplementation and depression in adults showed controversial results (reviewed by Cheng et al. [30], Gowda et al. [31], Li et al. [32], Spedding et al. [33], Shaffer et al. [34], and Vellekkatt et al. [35]). In children and adolescents, a recent literature review of observational and interventional studies concluded that there might be a positive influence of vitamin D on mental health in children [36]. The reviewed studies were controversial and heterogeneous which preclude making a robust conclusion and the authors highlighted the need for more studies to facilitate comparisons and deepen the observations.
We have previously demonstrated that 81% of schoolchildren in Kuwait were vitamin D deficient [37]. In this study, we aimed to estimate the prevalence of depression symptoms and investigate the association between Serum 25-hydroxyvitamin D (25(OH)D) and depression symptoms among schoolchildren in Kuwait, a country with plenty of sunshine.
Methods
Participants
The study was conducted within a project that aimed to assess vitamin D status in middle schoolchildren (11–16 years) in Kuwait. The details of the project have been described previously [37, 38]. In this project, a nationally representative sample of middle schoolchildren was selected using probability proportional to size sampling method. Trained nurses drew blood samples while trained data collectors gathered data on factors related to lifestyle such as physical activity, sleeping habits, and smoking through face-to-face interviews. Data on socio-demographic factors were collected from the parents of sampled schoolchildren through a self-administered questionnaire.
Another team of researchers at a later time was formulated to interview the schoolchildren and collect data on depression symptoms and its related factors. This was conducted on a subgroup of students (N = 704). Parents provided written informed consent while schoolchildren provided verbal assents before data collection. Both the Ethics Committee at the Health Sciences Centre, Kuwait University (No: DR/EC/2338) and the Ethics Committee at The Ministry of Health in Kuwait (No: 2015/248) approved the study.
Collection of blood samples and laboratory methods
Serum 25-hydroxyvitamin D (25(OH)D) level was measured using liquid chromatography-tandem mass spectrometry (LC–MS/MS), which is the gold standard method to assess vitamin D status [39, 40]. Other biological measurements including complete blood count, Parathyroid Hormone (PTH), vitamin B12, Iron, ferritin, transferrin and transferrin saturation were all measured in an accredited clinical biochemistry laboratory in a teaching hospital under strict quality control. Details of these measurements have been described before [37, 38].
Data collection on depression symptoms
Data on depression symptoms were collected using the Children’s Depression Inventory (CDI) [41], which has been previously translated and adopted in our setting [42]. The CDI is a 27-item self-rated symptom scale instrument, which was originally developed based on Beck’s Depression Inventory (BDI) [43], to screen for depression symptoms in children and adolescents aged 7–17 years. The CDI scores symptoms of depression on five subscales that include negative mood, interpersonal problems, ineffectiveness, anhedonia and negative self-esteem with 27 items scored on a 3-point scale (0: absence of the symptom, 1: moderate symptom, 2: severe symptom). The total CDI score is calculated by summing all items, which ranges between 0 (no depression symptom) and 54 (all depression symptoms exist). Several cut-off scores have been recommended such as “ > 13”, “ > 16” and “ ≥ 19” to indicate elevated depression symptoms in adolescents [44]. It has been suggested that a score of ≥ 19 is an appropriate cut-off point for population-based assessment, with 95% and 96% sensitivity and specificity respectively [45, 46]. Also, several studies have adopted this cut-off score to investigate depression symptoms in community-based studies [47,48,49,50].
Data collection on covariates
Data were collected on socio-economic and lifestyle-related factors using self-administered questionnaire that were sent to the parents. Data on behavioral factors such as physical activity, sedentary lifestyle, sleeping hours during weekdays and weekends were collected by face-to-face interviews with schoolchildren by trained team of data collectors. Data on physical activity were collected by a series of questions that were validated among high school students and showed strong correlation with data objectively measured by accelerometers. The total time spent on physical activity per week was calculated. Similarly, data on sedentary lifestyle were collected using a group of questions about the time spent on watching TV, playing video games, using the internet/computer and setting to read/do homework during weekdays and weekends. Standing height and body weight of the schoolchildren were measured using digital weight and height scale (Detecto®) in a standardized manner by trained data collectors.
Statistical analysis
Using Epidata Entry software, data were double entered into specifically designed database. Then data were transferred to STATA (StataCorp. 2011. Release 14) for data analysis. We used Spearman’s rank correlation to investigate the linear association between CDI score and 25(OH)D level. Vitamin D status was defined according to the Endocrine Society [51] and the Society for Adolescent Health and Medicine [52] as deficiency < 50 nmol/L; insufficiency 50–75 nmol/L; sufficiency ≥ 75 nmol/L. Kruskal–Wallis test was used to investigate the difference in CDI score across different vitamin D status (severe deficiency, deficiency, insufficiency, sufficiency).
The association between 25(OH)D and depression symptoms (CDI score ≥ 19) was assessed using unconditional logistic regression with adjustment for potential confounders. Separate analyses were performed with 25(OH)D fitted as a continuous variable and as a categorical variable. We categorized 25(OH)D using acceptable cutoff points [51] or quartiles. First, crude odds ratios were calculated, then statistically significant variables at 20% level of significant were introduced sequentially to the model while noting the impact of this on the association between 25(OH)D and depression symptoms. There was no difference in conclusion between this analysis and the analysis that was guided by the theory based on the studies that have investigated factors associated with depression symptoms among adolescents and children [53, 54]. As a sensitivity analysis, we used stepwise logistic regression to explore if the conclusion on the association between 25(OH)D and depression symptoms would be different with stepwise variables selection. Furthermore, we used simultaneous quantile regression to assess the association between 25(OH)D (as a continuous and categorical variable) and CDI score as a quantitative outcome using bootstrap to estimate the standard error with 500 replications. Throughout the analysis, all tests were two tailed and factors that showed p < 0.05 were deemed to be statistically significant.
Results
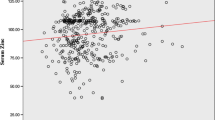
The analysis included 704 schoolchildren of whom 353 (50.14%) were males. The mean (standard deviation: SD) age was 12.25 (0.80) years. Of 704 schoolchildren, 94 (13.35%; 95%CI:10.35–17.06%) had depression symptoms (a score of 19 or more on the CDI). Figure 1 shows the distribution of CDI score in different vitamin D status. There was no significant difference in the median CDI score across different vitamin D status (p = 0.366) or different serum 25(OH)D quartiles (p = 0.540). There was also no significant correlation between serum 25(OH)D concentration and CDI score (Spearman’s rank correlation = 0.01; p = 0.825) or between PTH and CDI score (Spearman’s rank correlation = 0.06; p = 0.145).

Distribution of Children’s Depression Inventory score by vitamin D status among 704 schoolchildren
Table 1 shows the association between socio-demographic factors and depression symptoms (CDI score ≥ 19) in univariable analysis. Only maternal education showed inverse significant association with depression symptoms (p = 0.021). None of the lifestyle factors including the time spent on physical activity (p = 0.461), time spent on sedentary activities (p = 0.714) or body mass index (BMI) categories (p = 0.185) was significantly associated with depression symptoms in univariable analysis (Table 2). However, hours of sleep during weekdays (p = 0.063) and weekends (p = 0.079), and the number of times walking to/from school (p = 0.066) were borderline significantly associated with depression symptoms. Except for PTH, calcium, vitamin B12, anemia, iron, ferritin and folate were all not significantly associated with depression symptoms (Table 3). It is worth noting that the association between PTH and depression symptoms was significant when it was fitted as a continuous variable, but no association was found when PTH was categorized into quartile, tertiles or by the normal value range provided by our laboratory.
Table 4 shows the association between 25(OH)D and depression symptoms before and after adjusting for potential confounders. There was no significant association between 25(OH)D and depression symptoms whether 25(OH)D was fitted as a continuous variable (crude analysis p = 0.458 and adjusted analysis p = 0.233), categorized by acceptable cut-of points (crude analysis p = 0.376 and adjusted analysis p = 0.736), or when categorized as quartiles (crude analysis p = 0.760 and adjusted analysis p = 0.549). To confirm these findings, forward and backward stepwise logistic regression were used, and 25(OH)D was not selected in any model. Similarly, quantile regression showed no association between 25(OH)D and CDI score in any model (data are not shown). Finally, we investigated the interaction between 25(OH)D and BMI categories as some literature suggested [55]. Only the interaction between 25(OH)D quartiles and BMI categories was statistically significant (p = 0.021).
Discussion
This study aimed to estimate the prevalence of depression symptoms among schoolchildren and investigate the association between 25(OH)D and depression symptoms. The prevalence of depression symptoms in schoolchildren was 13.35% and no association was found between 25(OH)D and the CDI depression score. Compared to similar studies that used the CDI and similar cut-off point score, the prevalence of depression symptoms in our setting seems to be lower than that reported from Uganda or Iran (21% and 25.6% respectively) [47, 56], higher than that reported from Cyprus (10.25%)[50], and similar to that reported from Egypt (13.3%) [57].
Our findings suggest that neither vitamin D status nor levels is associated with depression symptoms in adolescents in Middle Eastern settings. Recently, several observational studies have attempted to investigate the link between low vitamin D levels and depression or mental health problems in children and adolescents [58,59,60,61,62,63,64,65,66,67,68,69,70,71] (recently reviewed by Głąbska et al. [36]). Although the review of observational studies supported the notion that vitamin D deficiency is linked to depression or poor mental health, the studies have significant heterogeneity, which precludes meaningful summary of these studies. This included different study populations (healthy children or children with disease conditions such as renal failure, bipolar disorder, or obsessive–compulsive disorder), different methods of measurement of 25(OH)D level, and different measures of the outcome (e.g. Strengths and Difficulties Questionnaire, Beck Depression Inventory, Buss-Perry Aggression Questionnaire, Young Mania Rating Scale, Children’s Depression Rating Scale, and Mood and Feelings Questionnaire). Interventional studies that investigated the impact of vitamin D supplementation on mental health in children and adolescents [72,73,74] (recently reviewed by Głąbska et al. [36]) showed that vitamin D supplementation maybe beneficial for mental health. However, similar to the observational studies, there was a significant heterogeneity in these studies including study population (e.g. children with sickle cell disease or autism spectrum disorder), dosing regimens, and the outcome measurements (e.g. Depression Scale for Children, Child Behavior Checklist, Activity of Daily Living, Screen for Child Anxiety Related Emotional Disorders, Children’s Quality of Life Questionnaire, and Yale-Brown Obsessive Compulsive Scale and Children’s Depression Inventory). The review highlighted the need for more studies to facilitate comparisons and deepen the observations [36]. A recently reported randomized controlled trial (not included in the previous review) on children and adolescents, who were both vitamin D deficient and at least mildly depressed at baseline, showed that vitamin D supplementation has no effect on self-reported depression symptoms although a significant decrease of parent-reported depression symptoms was found [75].
In our study, the lack of association between 25(OH)D and depression symptoms may genuinely reflect the absence of the relationship between vitamin D level and depression symptoms as Mendelian randomization studies did not indicate a causal relationship between 25(OH)D concentrations and depression [76, 77]. However, it could be due to the fact that the majority (80%) of the study participants were vitamin D deficient. The other possible reason is that children with severe depression symptoms might be absent from school. This is plausible because it is postulated that vitamin D is beneficial only among those with clinically significant depression symptoms, but not in healthy participants [78] and that the presumed antidepressant effects of vitamin D may be particularly apparent at more severe stages of depression [61, 75]. Furthermore, we used the CDI, which has been validated previously in our setting. In our data, the reliability of the entire CDI scale was high (Cronbach α 0.839 [95%CI: 0.821, 0.855] and McDonald ω 0.829 [95%CI: 0.811, 0.847]. We also found that the CDI score to be related to students’ academic performance (Fig. 2), which increased our confidence in this psychometric measurement. However, it is not clear if our findings would remain the same if we used another psychometric measurement scale. It is difficult to compare our findings to the previous studies that investigated this issue using the CDI among children and adolescents. One of these studies included children with Cystic fibrosis [58] and found an association between vitamin D and depression symptoms while another study used the CDI as a measure of the outcome and found male (but not female) adolescents with major depressive disorder to have significantly lower bone mineral density as compared to healthy controls after adjusting for body mass and maturity [69]. In another study, authors used the CDI as a measure of the outcome and compared 89 depressed adolescents with 43 controls and found an association between vitamin D level and depression [79]. Finally, the lack of association between 25(OH)D and depression symptoms in our study could be attributed to different VDR genes in our setting or the complex interaction between vitamin D and both the serotonin transporter promotor gene polymorphism and childhood adversity experience [80].

Association between depression symptoms (Children’s Depression Inventory score ≥ 19) and the students’ academic performance
There are several strengths in this study including measuring 25(OH)D using a gold standard method and collecting data from a large sample. The rigorous statistical modeling of 25(OH)D as a continuous or a categorical variable (quartiles or established cut-of points) and using quantile regression to model the CDI score as a continuous, rather than a binary outcome undoubtedly made our conclusion strong and robust. However, we did not collect data on the history of depression in the parents or the siblings, and exposure to early childhood adversity experience (such as abuse, neglect, the loss of a loved one in early life), which are potential risk factors for depression [81]. Also, like other epidemiological studies, we assessed depression symptoms using the CDI without a diagnostic interview. Finally, it is possible that many of the children with severe depression symptoms were absent from school during the study period, which may have attenuated the association.
In conclusion, we have demonstrated that one out of ten schoolchildren in Kuwait has depression symptoms and that 25(OH)D is not associated with having depression symptoms in our setting. It is important to have sufficient vitamin D levels during adolescence for several other health benefits.
Availability of data and materials
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Abbreviations
- 25(OH)D:
-
25-Hydroxyvitamin D
- BMI:
-
Body mass index
- LC–MS/MS:
-
Liquid chromatography-tandem mass spectrometry
- PTH:
-
Parathyroid Hormone
- CDI:
-
Children’s Depression Inventory
- BDI:
-
Beck’s Depression Inventory
References
GBD. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet (London, England). 2016;10053:1545–602.
WHO. Depression: Key fact: World Health Organization 2021 https://www.who.int/news-room/fact-sheets/detail/depression#:~:text=Depression%20is%20a%20common%20mental,affected%20by%20depression%20than%20men.
Kirsch I. Review: benefits of antidepressants over placebo limited except in very severe depression. Evid Based Ment Health. 2010;13(2):49.
Sanchez-Villegas A, Martínez-González MA. Diet, a new target to prevent depression? BMC Med. 2013;11:3.
Jacka FN, O’Neil A, Opie R, Itsiopoulos C, Cotton S, Mohebbi M, et al. A randomised controlled trial of dietary improvement for adults with major depression (the “SMILES” trial). BMC Med. 2017;15(1):23.
Opie RS, Itsiopoulos C, Parletta N, Sanchez-Villegas A, Akbaraly TN, Ruusunen A, et al. Dietary recommendations for the prevention of depression. Nutr Neurosci. 2017;20(3):161–71.
Lopresti AL, Hood SD, Drummond PD. A review of lifestyle factors that contribute to important pathways associated with major depression: diet, sleep and exercise. J Affect Disord. 2013;148(1):12–27.
Mouratidou T, Vicente-Rodriguez G, Gracia-Marco L, Huybrechts I, Sioen I, Widhalm K, et al. Associations of dietary calcium, vitamin D, milk intakes, and 25-hydroxyvitamin D with bone mass in Spanish adolescents: the HELENA study. J Clin Densitometry. 2013;16(1):110–7.
Zhang Y, Fang F, Tang J, Jia L, Feng Y, Xu P, et al. Association between vitamin D supplementation and mortality: systematic review and meta-analysis. BMJ (Clinical research ed). 2019;366: l4673.
Zhang Y, Tan H, Tang J, Li J, Chong W, Hai Y, et al. Effects of Vitamin D Supplementation on prevention of type 2 diabetes in patients with prediabetes: a systematic review and meta-analysis. Diabetes Care. 2020;43(7):1650–8.
Duan S, Lv Z, Fan X, Wang L, Han F, Wang H, et al. Vitamin D status and the risk of multiple sclerosis: a systematic review and meta-analysis. Neurosci Lett. 2014;570:108–13.
Wang Z, Ding R, Wang J. The association between vitamin d status and autism spectrum disorder (ASD): a systematic review and meta-analysis. Nutrients. 2020;13:1.
Jolliffe DA, Greenberg L, Hooper RL, Griffiths CJ, Camargo CA Jr, Kerley CP, et al. Vitamin D supplementation to prevent asthma exacerbations: a systematic review and meta-analysis of individual participant data. Lancet Respir Med. 2017;5(11):881–90.
Garland CF, Kim JJ, Mohr SB, Gorham ED, Grant WB, Giovannucci EL, et al. Meta-analysis of all-cause mortality according to serum 25-hydroxyvitamin D. Am J Public Health. 2014;104(8):e43-50.
Liu N, Sun J, Wang X, Zhang T, Zhao M, Li H. Low vitamin D status is associated with coronavirus disease 2019 outcomes: a systematic review and meta-analysis. Int J Infect Dis. 2021;104:58–64.
Pereira M, Dantas Damascena A, Galvão Azevedo LM, de Almeida Oliveira T, da Mota Santana J. Vitamin D deficiency aggravates COVID-19: systematic review and meta-analysis. Crit Rev Food Sci Nutr. 2020:1–9.
Jordanes. The Origin and Deeds of the Goths. Princeton, NJ, USA.: Princeton University Press: http://people.ucalgary.ca/~vandersp/Courses/texts/jordgeti.html. Accessed 8 Apr 2014.
Farhangi MA, Mesgari-Abbasi M, Nameni G, Hajiluian G, Shahabi P. The effects of vitamin D administration on brain inflammatory markers in high fat diet induced obese rats. BMC Neurosci. 2017;18(1):81.
Eyles DW, Smith S, Kinobe R, Hewison M, McGrath JJ. Distribution of the vitamin D receptor and 1 alpha-hydroxylase in human brain. J Chem Neuroanat. 2005;29(1):21–30.
Eyles DW, Burne TH, McGrath JJ. Vitamin D, effects on brain development, adult brain function and the links between low levels of vitamin D and neuropsychiatric disease. Front Neuroendocrinol. 2013;34(1):47–64.
Stumpf WE. Drugs in the brain–cellular imaging with receptor microscopic autoradiography. Prog Histochem Cytochem. 2012;47(1):1–26.
Cui X, Pertile R, Liu P, Eyles DW. Vitamin D regulates tyrosine hydroxylase expression: N-cadherin a possible mediator. Neuroscience. 2015;304:90–100.
Garcion E, Wion-Barbot N, Montero-Menei CN, Berger F, Wion D. New clues about vitamin D functions in the nervous system. Trends Endocrinol Metab. 2002;13(3):100–5.
Humble MB. Vitamin D, light and mental health. J Photochem Photobiol B. 2010;101(2):142–9.
McCann JC, Ames BN. Is there convincing biological or behavioral evidence linking vitamin D deficiency to brain dysfunction? FASEB J. 2008;22(4):982–1001.
Anglin RE, Samaan Z, Walter SD, McDonald SD. Vitamin D deficiency and depression in adults: systematic review and meta-analysis. Br J Psychiatry. 2013;202:100–7.
Ju SY, Lee YJ, Jeong SN. Serum 25-hydroxyvitamin D levels and the risk of depression: a systematic review and meta-analysis. J Nutr Health Aging. 2013;17(5):447–55.
Bertone-Johnson ER. Vitamin D and the occurrence of depression: causal association or circumstantial evidence? Nutr Rev. 2009;67(8):481–92.
Penckofer S, Kouba J, Byrn M, Estwing FC. Vitamin D and depression: where is all the sunshine? Issues Ment Health Nurs. 2010;31(6):385–93.
Cheng YC, Huang YC, Huang WL. The effect of vitamin D supplement on negative emotions: A systematic review and meta-analysis. Depress Anxiety. 2020;37(6):549–64.
Gowda U, Mutowo MP, Smith BJ, Wluka AE, Renzaho AM. Vitamin D supplementation to reduce depression in adults: meta-analysis of randomized controlled trials. Nutrition (Burbank, Los Angeles County, Calif). 2015;31(3):421–9.
Li G, Mbuagbaw L, Samaan Z, Falavigna M, Zhang S, Adachi JD, et al. Efficacy of vitamin D supplementation in depression in adults: a systematic review. J Clin Endocrinol Metab. 2014;99(3):757–67.
Spedding S. Vitamin D and depression: a systematic review and meta-analysis comparing studies with and without biological flaws. Nutrients. 2014;6(4):1501–18.
Shaffer JA, Edmondson D, Wasson LT, Falzon L, Homma K, Ezeokoli N, et al. Vitamin D supplementation for depressive symptoms: a systematic review and meta-analysis of randomized controlled trials. Psychosom Med. 2014;76(3):190–6.
Vellekkatt F, Menon V. Efficacy of vitamin D supplementation in major depression: A meta-analysis of randomized controlled trials. J Postgrad Med. 2019;65(2):74–80.
Głąbska D, Kołota A, Lachowicz K, Skolmowska D, Stachoń M, Guzek D. The influence of vitamin D intake and status on mental health in children: a systematic review. Nutrients. 2021;13:3.
Al-Taiar A, Rahman A, Al-Sabah R, Shaban L, Al-Harbi A. Vitamin D status among adolescents in Kuwait: a cross-sectional study. BMJ Open. 2018;8(7): e021401.
Al-Taiar A, Rahman A, Al-Sabah R, Shaban L, AlBaloul AH, Banaee S, et al. Vitamin D levels in relation to low back pain during adolescence. Br J Nutr. 2020;123(11):1302–11.
Yetley EA, Pfeiffer CM, Schleicher RL, Phinney KW, Lacher DA, Christakos S, et al. NHANES monitoring of serum 25-hydroxyvitamin D: a roundtable summary. J Nutr. 2010;140(11):2030s-s2045.
de la Hunty A, Wallace AM, Gibson S, Viljakainen H, Lamberg-Allardt C, Ashwell M. UK Food Standards Agency Workshop Consensus Report: the choice of method for measuring 25-hydroxyvitamin D to estimate vitamin D status for the UK National Diet and Nutrition Survey. Br J Nutr. 2010;104(4):612–9.
Kovacs M. The Children’s Depression, Inventory (CDI). Psychopharmacol Bull. 1985;21(4):995–8.
Al-Balhan EM. The Children’s Depression Inventory as a reliable measure for post-Iraqi invasion Kuwaiti youth. Soc Behav Personal Int J. 2006;34(4):351–66.
Beck A, Beamesderfer A. Assessment of depression: The depression inventory. IPPRO-M, editor. Oxford,England: Karger; 1974.
Timbremont B, Braet C, Dreessen L. Assessing depression in youth: relation between the Children’s Depression Inventory and a structured interview. J Clin Child Adolesc Psychol. 2004;33(1):149–57.
Figueras Masip A, Amador-Campos JA, Gómez-Benito J, del Barrio GV. Psychometric properties of the Children’s Depression Inventory in community and clinical sample. Spanish J Psychol. 2010;13(2):990–9.
Smucker MR, Craighead WE, Craighead LW, Green BJ. Normative and reliability data for the Children’s Depression Inventory. J Abnorm Child Psychol. 1986;14(1):25–39.
Nalugya-Sserunjogi J, Rukundo GZ, Ovuga E, Kiwuwa SM, Musisi S, Nakimuli-Mpungu E. Prevalence and factors associated with depression symptoms among school-going adolescents in Central Uganda. Child Adolesc Psychiatry Ment Health. 2016;10:39.
Hong X, Li J, Liang Y, Wang Z, Xu F. Investigation on overweight, obesity and depression among middle school students in Nanjing. Chin Ment Health J. 2008;22:744–8.
Niu X, Zhao H. Association between self-assessed somatotypes and depression among children and adolescents aged 9–17 years. Chin J Sch Health. 2015;36:1334–7.
Sokratis S, Christos Ζ, Despo P, Maria K. Prevalence of depressive symptoms among schoolchildren in Cyprus: a cross-sectional descriptive correlational study. Child Adolesc Psychiatry Ment Health. 2017;11:7.
Holick MF, Binkley NC, Bischoff-Ferrari HA, Gordon CM, Hanley DA, Heaney RP, et al. Evaluation, treatment, and prevention of vitamin D deficiency: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2011;96(7):1911–30.
SfAHaM. Society for Adolescent Health and Medicine-Recommended vitamin D intake and management of low vitamin D status in adolescents: a position statement of the society for adolescent health and medicine. The Journal of adolescent health : official publication of the Society for Adolescent Medicine. 2013;52(6):801–3.
Elovainio M, Pulkki-Råback L, Hakulinen C, Ferrie JE, Jokela M, Hintsanen M, et al. Childhood and adolescence risk factors and development of depressive symptoms: the 32-year prospective Young Finns follow-up study. J Epidemiol Community Health. 2015;69(11):1109–17.
Saluja G, Iachan R, Scheidt PC, Overpeck MD, Sun W, Giedd JN. Prevalence of and risk factors for depressive symptoms among young adolescents. Arch Pediatr Adolesc Med. 2004;158(8):760–5.
Milaneschi Y, Simmons WK, van Rossum EFC, Penninx BWJH. Depression and obesity: evidence of shared biological mechanisms. Mol Psychiatry. 2019;24(1):18–33.
Sajjadi H, Mohaqeqi Kamal SH, Rafiey H, Vameghi M, Forouzan AS, Rezaei M. A systematic review of the prevalence and risk factors of depression among iranian adolescents. Glob J Health Sci. 2013;5(3):16–27.
El-Missiry A, Soltan M, Hadi MA, Sabry W. Screening for depression in a sample of Egyptian secondary school female students. J Affect Disord. 2012;136(1–2):e61–8.
Smith BA, Cogswell A, Garcia G. Vitamin D and depressive symptoms in children with cystic fibrosis. Psychosomatics. 2014;55(1):76–81.
Tolppanen AM, Sayers A, Fraser WD, Lewis G, Zammit S, Lawlor DA. The association of 25-hydroxyvitamin D3 and D2 with behavioural problems in childhood. PLoS ONE. 2012;7(7): e40097.
Husmann C, Frank M, Schmidt B, Jöckel KH, Antel J, Reissner V, et al. Low 25(OH)-vitamin D concentrations are associated with emotional and behavioral problems in German children and adolescents. PLoS ONE. 2017;12(8): e0183091.
Schäfer TK, Herrmann-Lingen C, Meyer T. Association of circulating 25-hydroxyvitamin D with mental well-being in a population-based, nationally representative sample of German adolescents. Qual Life Res. 2016;25(12):3077–86.
Robinson SL, Marín C, Oliveros H, Mora-Plazas M, Lozoff B, Villamor E. Vitamin D Deficiency in Middle Childhood Is Related to Behavior Problems in Adolescence. J Nutr. 2020;150(1):140–8.
Han B, Zhu FX, Yu HF, Liu S, Zhou JL. Low serum levels of vitamin D are associated with anxiety in children and adolescents with dialysis. Sci Rep. 2018;8(1):5956.
Petrov B, Aldoori A, James C, Yang K, Algorta GP, Lee A, et al. Bipolar disorder in youth is associated with increased levels of vitamin D-binding protein. Transl Psychiatry. 2018;8(1):61.
Yazici KU, Percinel Yazici I, Ustundag B. Vitamin D levels in children and adolescents with obsessive compulsive disorder. Nord J Psychiatry. 2018;72(3):173–8.
Esnafoğlu E, Yaman E. Vitamin B12, folic acid, homocysteine and vitamin D levels in children and adolescents with obsessive compulsive disorder. Psychiatry Res. 2017;254:232–7.
MacDonald K, Godziuk K, Yap J, LaFrance R, Ansarian M, Haqq A, et al. Vitamin D status, cardiometabolic, liver, and mental health status in obese youth attending a pediatric weight management center. J Pediatr Gastroenterol Nutr. 2017;65(4):462–6.
Ataie-Jafari A, Qorbani M, Heshmat R, Ardalan G, Motlagh ME, Asayesh H, et al. The association of vitamin D deficiency with psychiatric distress and violence behaviors in Iranian adolescents: the CASPIAN-III study. J Diabetes Metab Disord. 2015;14:62.
Fazeli PK, Mendes N, Russell M, Herzog DB, Klibanski A, Misra M. Bone density characteristics and major depressive disorder in adolescents. Psychosom Med. 2013;75(2):117–23.
Gracious BL, Finucane TL, Friedman-Campbell M, Messing S, Parkhurst MN. Vitamin D deficiency and psychotic features in mentally ill adolescents: a cross-sectional study. BMC Psychiatry. 2012;12:38.
Mousa A, Naderpoor N, de Courten MPJ, de Courten B. Vitamin D and symptoms of depression in overweight or obese adults: A cross-sectional study and randomized placebo-controlled trial. J Steroid Biochem Mol Biol. 2018;177:200–8.
Bahrami A, Mazloum SR, Maghsoudi S, Soleimani D, Khayyatzadeh SS, Arekhi S, et al. High Dose Vitamin D supplementation is associated with a reduction in depression score among adolescent girls: a nine-week follow-up study. J Diet Suppl. 2018;15(2):173–82.
Dougherty KA, Schall JI, Bertolaso C, Smith-Whitley K, Stallings VA. Vitamin D supplementation improves health-related quality of life and physical performance in children with sickle cell disease and in healthy children. J Pediatr Health Care. 2020;34(5):424–34.
Grung B, Sandvik AM, Hjelle K, Dahl L, Frøyland L, Nygård I, et al. Linking vitamin D status, executive functioning and self-perceived mental health in adolescents through multivariate analysis: a randomized double-blind placebo control trial. Scand J Psychol. 2017;58(2):123–30.
Libuda L, Timmesfeld N, Antel J, Hirtz R, Bauer J, Führer D, et al. Effect of vitamin D deficiency on depressive symptoms in child and adolescent psychiatric patients: results of a randomized controlled trial. Eur J Nutr. 2020;59(8):3415–24.
Libuda L, Laabs BH, Ludwig C, Bühlmeier J, Antel J, Hinney A, et al. Vitamin D and the risk of depression: a causal relationship? findings from a mendelian randomization study. Nutrients. 2019;11:5.
Michaëlsson K, Melhus H, Larsson SC. Serum 25-Hydroxyvitamin D concentrations and major depression: a mendelian randomization study. Nutrients. 2018;10:12.
Yalamanchili V, Gallagher JC. Treatment with hormone therapy and calcitriol did not affect depression in older postmenopausal women: no interaction with estrogen and vitamin D receptor genotype polymorphisms. Menopause. 2012;19(6):697–703.
Esnafoglu E, Ozturan DD. The relationship of severity of depression with homocysteine, folate, vitamin B12, and vitamin D levels in children and adolescents. Child Adolesc Ment Health. 2020;25(4):249–55.
Bonk S, Hertel J, Zacharias HU, Terock J, Janowitz D, Homuth G, et al. Vitamin D moderates the interaction between 5-HTTLPR and childhood abuse in depressive disorders. Sci Rep. 2020;10(1):22394.
Bonin L, Brent D, Solomon D. Patient education: Depression in children and adolescents (Beyond the Basics) 2021 https://www.uptodate.com/contents/depression-in-children-and-adolescents-beyond-the-basics.
WHO. Haemoglobin concentrations for the diagnosis of anaemia and assessment of severity. Vitamin and Mineral Nutrition Information System. Geneva; 2011.
Acknowledgements
We would like to thank Ms Nadien Rushdi for the coordination of data collection. We would like also to thank schoolchildren and their parents.
Funding
Part of the data presented in this article were collected in the project no. WF 02/13 which was funded by Kuwait University, Research Sector.
Author information
Authors and Affiliations
Contributions
RA-S and AA-T both supervised data collection, analyzed the data, and drafted the manuscript. LS, ANA, RSA, PKD contributed to the data interpretation and revised the manuscript with significant intellectual input. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The Ethics Committee at the Health Sciences Centre, Kuwait University (No: DR/EC/2338) and the Ethics Committee at The Ministry of Health in Kuwait (No: 2015/248) both approved the study. Parents provided written informed consent while schoolchildren provided verbal assents before data collection.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Al-Sabah, R., Al-Taiar, A., Shaban, L. et al. Vitamin D level in relation to depression symptoms during adolescence. Child Adolesc Psychiatry Ment Health 16, 53 (2022). https://doi.org/10.1186/s13034-022-00489-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13034-022-00489-4